

Abstract
Study Design:
Retrospective database analysis.
Objective:
The impact of the 2008-2009 economic downtown on elective lumbar spine surgery is unknown. Our objective was to investigate the effect of the economic downturn on the overall trends of elective lumbar spine surgery in the United States.
Methods:
The Nationwide Inpatient Sample (NIS) was used in conjunction with US Census and macroeconomic data to determine historical trends. The economic downturn was defined as 2008 to 2009. Codes from the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), were used in order to identify appropriate procedures. Confidence intervals were determined using subgroup analysis techniques.
Results:
From 2003 to 2012, there was a 19.8% and 26.1% decrease in the number of lumbar discectomies and laminectomies, respectively. Over the same time period, there was a 56.4% increase in the number of lumbar spinal fusions. The trend of elective lumbar spine surgeries per 100 000 persons in the US population remained consistent from 2008 to 2009. The number of procedures decreased by 4.5% from 2010 to 2011, 7.6% from 2011 to 2012, and 3.1% from 2012 to 2013. The R 2 value between the number of surgeries and the S&P 500 Index was statistically significant (P ≤ .05).
Conclusions:
The economic downturn did not affect elective lumbar fusions, which increased in total from 2003 to 2013. The relationship between the S&P 500 Index and surgical trends suggests that during recessions, individuals may utilize other means, such as insurance, to cover procedural costs and reduce out-of-pocket expenditures, accounting for no impact of the economic downturn on surgical trends. These findings can assist multiple stakeholders in better understanding the interconnectedness of macroeconomics, policy, and elective lumbar spine surgery trends.
Keywords: Nationwide Inpatient Sample, national trends, lumbar spine surgery, lumbar discectomy, lumbar laminectomy, lumbar spinal fusion, economic recession, macroeconomic factors
Introduction
Elective lumbar spine surgeries including discectomies, laminectomies, and fusions are common procedures in the United States. Previous studies have demonstrated the increasing trend in elective lumbar spine surgery in the United States in the 1980s, 1990s, and early to mid-2000s.1–4 However, unlike previous periods studied, the late 2000s witnessed an economic downturn unlike any since the Great Depression. The same time period also involved reimbursement and policy-related changes. For example, the early 2010s led to the passage of a new health care law, Affordable Care Act (ACA), which aimed at improving health care delivery by reducing costs, focusing on patient outcomes, and improving efficiency.5–8 Analyzing national trends from 2003 to 2013 will yield valuable information, as prior research of this time frame has only addressed state-level trends and impacts of insurance changes but not national implications.9,10
Researchers have called for surgeons to be more involved in health care policy debates and decision making throughout the implementation process of new outcome-based payment and care systems.11,12 In order for physicians to successfully participate in these discussions, a deep understanding of what drives trends in surgery, outside of clinical decision making, is important. Research by Weinstein and colleagues showed that lumbar spine surgery trends are not correlated with the per capita supply of spine surgeons.3 Deyo et al suggest that the increasing trend of complex lumbar spine surgery from 2003 to 2007 may be driven by the introduction of new surgical devices and the opinions of spine surgery thought leaders.4 Kurtz et al have reported on the relationship between total joint replacement and macroeconomic factors including the economic downturn of 2008.13 However, to our knowledge, no studies thus far have evaluated the role of macroeconomic factors on rates of lumbar spine surgery.
Our objective was to analyze the national trends of elective lumbar spine surgery in the United States from 2003 to 2013 with a focus on the effects of macroeconomic conditions. Our goal was to address the following questions: (1) Was the trend of elective lumbar spine surgery affected by the economic downturn of 2008 to 2009? (2) How is the trend of elective lumbar spine surgery correlated with major macroeconomic indicators in the United States? (3) What are the trends of elective lumbar spine surgeries from 2003 to 2013?
Materials and Methods
Surgical Procedure Data Source
The Nationwide Inpatient Sample (NIS) was used in this study. Each year of NIS data contains more than 7 million data entries, which represents a 20% sample of discharges from hospitals throughout the United States. Developed for the Healthcare Cost and Utilization Project and through a federal-state-industry partnership sponsored by the Agency for Healthcare Research and Quality, the NIS is the largest publicly available and nationally representative all-payer health care database in the United States.14
Each year of NIS data coincides with a trend weight file that allows for national estimates to be extrapolated from the 20% sample. The Agency for Healthcare Research and Quality suggests using available data from 1993 onwards when conducting longitudinal analyses due to its stable sampling design and reoptimization of trend weights starting in that year. Our study period is from 2003 to 2012, making NIS data usage appropriate.
Population Measurements
The size of the total US population for each year was determined using intercensal estimates from the US Census Bureau.15 The size of the employed population in the United States for each year was determined using labor force statistics from the US Department of Labor, Bureau of Labor Statistics.16
Macroeconomic Measurements
National Health Expenditure data was acquired from the National Health Expenditure Accounts at the Centers for Medicare and Medicaid Services.17 Gross domestic product (GDP) was attained from the US Department of Commerce, Bureau of Economic Analysis.18 The Standard and Poor’s (S&P) 500 Index over the relevant study years was downloaded from Yahoo! Finance.19
Surgical Inclusion Criteria
Using NIS data, the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), codes 722.10 (lumbar disc herniation), 724.02 (lumbar stenosis), 738.4 (acquired spondylolisthesis), and 722.52 (degeneration of lumbar or lumbosacral intervertebral disc) were applied to identify common lumbar spine conditions. If a patient record included more than one of the aforementioned ICD-9-CM diagnoses codes, only one episode was recorded.
Following the initial diagnosis step above, separate queries were then conducted for lumbar discectomy, laminectomy, and spinal fusion, respectively, using ICD-9-CM procedure codes. The ICD-9-CM procedure codes used in the queries were 80.51 (lumbar discectomy), 03.09 (lumbar laminectomy), and 81.06, 81.07, and 81.08 (lumbar spinal fusion).
Trend and Statistical Analysis
Stata/SE, version 14.0 for Mac, was used for the NIS data cleaning and analysis. The total number of elective lumbar spine surgeries performed each year from 2003 to 2013 was calculated using the NIS by summing the yearly totals of lumbar discectomy, laminectomy, and spinal fusion procedures.
NIS data was used to calculate population subgroups as a function of age, sex, and census region. This allowed for confidence interval calculations for both the number of procedures and percentage reimbursed by each payer type.
Using US Census Bureau data for each year and NIS data, the number of elective lumbar spine surgeries per 100 000 persons in the United States was calculated. The same analysis was done using Bureau of Labor Statistics data to determine the number of elective lumbar spine surgeries performed per 100 000 employed persons in the United States. US Census Bureau data was also used to look at the trend of subset of the population 65 years of age and older.
The trend of elective lumbar spine surgeries from 2003 to 2013 was regressed against the National Health Expenditure, GDP, and the stock market (S&P 500 Index) using linear regression.
Results
The incidence of elective lumbar spine surgeries was not affected by the economic downturn from 2008 to 2009 relative to the total US population (Figure 1). In the midst of the economic downturn in 2008, there were 189 657 lumbar discectomies (95% confidence interval [CI]: 174 761 to 204 553), 96 749 lumbar laminectomies (95% CI: 93 426 to 100 073), and 172 411 lumbar spinal fusions (95% CI: 160 117 to 184 704; Table 1). In 2012, there were 176 330 lumbar discectomies (95% CI: 164 459 to 188 201), 82 550 lumbar laminectomies (95% CI: 80 012 to 85 087), and 180 770 lumbar spinal fusions (95% CI: 169 951 to 191 589; Table 1).
Figure 1.
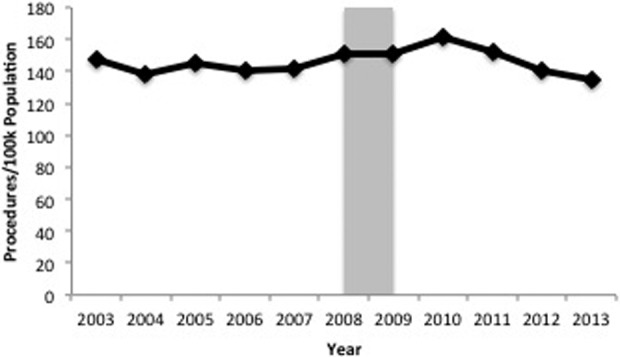
The incidence of elective lumbar spine surgery relative to the population saw no effect from the economic downturn from 2008 to 2009. A significant decrease in the trend occurred from 2010 to 2013. The years of the economic downturn are highlighted in light gray.
Table 1.
Elective Lumbar Spine Procedure Trenda.
| Procedure | 2004 | 2008 | 2012 |
|---|---|---|---|
| Lumbar discectomy | 182 312 (167 165-197 459) | 189 657 (174 761-204 553) | 176 330 (164 459-188 201) |
| Lumbar laminectomy | 99 199 (95 024-103 374) | 96 749 (93 426-100 073) | 82 550 (80 012-85 087) |
| Lumbar spinal fusion | 121 224 (111 892-130 556) | 172 411 (160 117-184 704) | 180 770 (169 951-191 589) |
aThe number of elective lumbar procedures in 2004, 2008, and 2012 are shown above, with the 95% confidence interval in parentheses.
From 2003 to 2013, lumbar discectomies showed a decreasing trend and, in total, declined by 19.8% (Figure 2). Similarly, lumbar laminectomies demonstrated a decreasing trend and diminished by 26.1% over the same time period (Figure 2). In contrast, lumbar spinal fusions increased between 2003 and 2013 by 56.4% over the relevant time frame (Figure 2). The total rate of all elective lumbar spine surgery dropped from 148 per 100 000 in the population in 2003 to 135 per 100 000 in the population in 2013.
Figure 2.
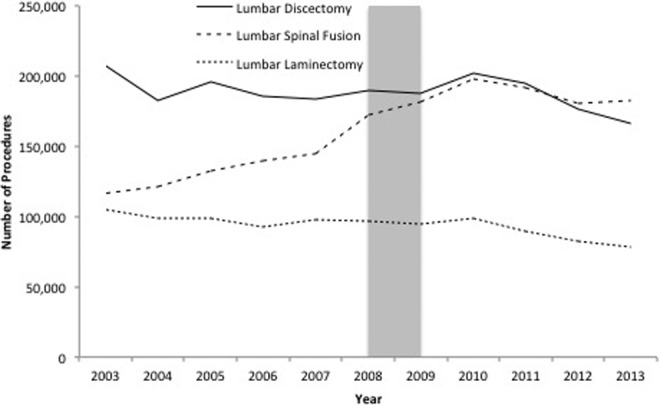
Lumbar discectomy and laminectomy showed a decreasing trend from 2003 to 2013. Lumbar spinal fusion showed an increasing trend over the same time frame. The economic downturn did not affect the rate of any of the 3 surgeries. The years of the economic downturn are highlighted in light gray.
The number of lumbar laminectomies declined from 2010 to 2011, 2011 to 2012, and 2012 to 2013 by 9.5%, 7.5%, and 5.7%, respectively. The quantity of lumbar discectomies also contracted from 2010 to 2011, 2011 to 2012, and 2012 to 2013 by 3.2%, 9.6%, and 6.0%, respectively. In contrast, the number of lumbar spinal fusions decreased by 3.2% from 2010 to 2011 and by 5.5% from 2011 to 2012 but increased by 0.9% from 2012 to 2013.
When all 3 elective lumbar spine surgeries were combined, the incidence of elective lumbar spine surgery increased from 2008 to 2009 and from 2009 to 2010 by 1.0% and 7.4%, respectively. However, the number of elective lumbar spine surgery dropped from 2010 to 2011, 2011 to 2012, and 2012 to 2013 by 4.5, 7.6%, and 3.1%, respectively.
In 2012, Medicare reimbursed 32.8% of lumbar discectomies (95% CI: 29.8% to 35.8%), 54.1% of lumbar laminectomies (95% CI: 48.5% to 59.6%), and 41.4% of lumbar spinal fusions (95% CI: 37.2% to 45.5%; Table 2). In contrast, private insurance reimbursed 48.2% of lumbar discectomies (95% CI: 42.5% to 53.9%), 34.2% of lumbar laminectomies (95% CI: 30.9% to 37.5%), and 42.6% of lumbar spinal fusions (95% CI: 37.4% to 47.7%; Table 2).
Table 2.
Primary Reimbursement Source of Elective Lumbar Spine Procedures in 2012a.
| Procedure | Medicare | Medicaid | Private Insurance | Other |
|---|---|---|---|---|
| Lumbar discectomy | 32.8% (29.8% to 35.8%) | 6.3% (5.5% to 7.1%) | 48.2% (42.5% to 53.9%) | 12.7% (11.0% to 14.5%) |
| Lumbar laminectomy | 54.1% (48.5% to 59.6%) | 4.1% (3.6% to 4.6%) | 34.2% (30.9% to 37.5%) | 7.6% (6.7% to 8.5%) |
| Lumbar spinal fusion | 41.4% (37.2% to 45.5%) | 5.2% (4.5% to 6.0%) | 42.6% (37.4% to 47.7%) | 10.8% (9.5% to 12.2%) |
aEach value is the percentage of the procedure reimbursed by that given payer method, with the 95% confidence interval in parentheses.
Macroeconomic Conditions on Elective Lumbar Spine Surgery Trends
From 2008 to 2009, there was an increase in the total number of elective spine surgeries performed in the United States. In 2008 and 2009, there were 458 817 and 463 340 elective lumbar spine surgeries completed, respectively. However, relative to the US population, there was no noticeable effect (Figure 1). From 2008 to 2009, the incidence of elective lumbar spine surgeries relative to the employed population increased by 4.9% (Figure 3).
Figure 3.
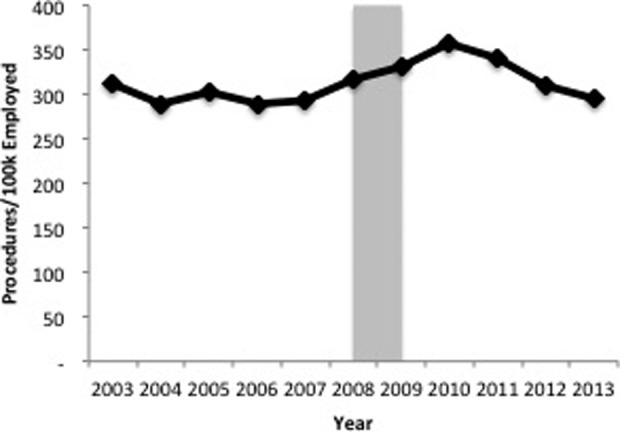
The elective lumbar spine surgery trend continued upwards with a growth of 4.9% during the economic downturn from 2008 to 2009. The years of the economic downturn are highlighted in light gray.
During the economic downturn from 2008 to 2009, lumbar discectomies and laminectomies had negative growth rates of 1.3% and 2.2%, respectively. Lumbar laminectomies had a negative growth rate the year prior to the economic downturn (2007) of 1.3%, while lumbar discectomies had a positive growth rate of 3.1%. Lumbar spinal fusion witnessed a positive growth rate of 5.2% during the economic downturn.
The percentage of elective lumbar spine surgeries paid for by private payers decreased by 5.6% from 2008 to 2009 and had an overall downward trend from 2003 to 2013. In 2003, 49.9% of all elective lumbar spine surgeries performed were reimbursed by a private payer (Figure 4). By 2013, 41.6% of the total number of elective lumbar spine surgeries was covered by a private payer (Figure 4). Conversely, the number of persons in the population age 65 years or older steadily increased over the study years from 2003 to 2012 (Figure 5).
Figure 4.
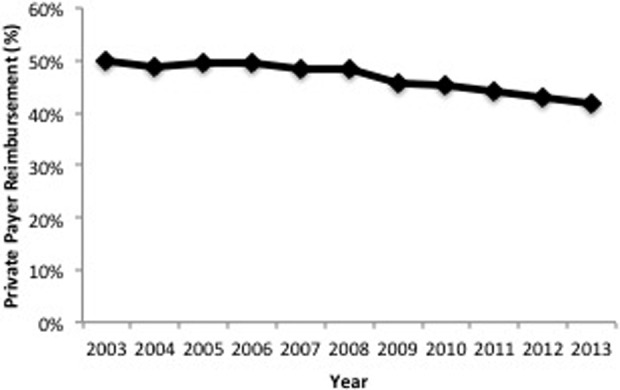
The percentage of elective lumbar spine surgeries reimbursed by a private payer decreased over the study period from 2003 to 2013. The years of the economic downturn are highlighted in light gray.
Figure 5.
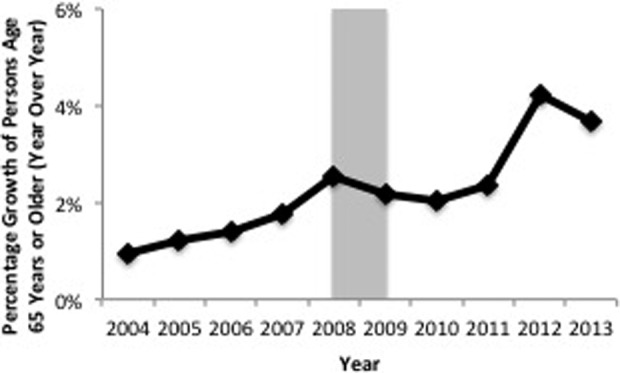
The growth rate of persons age 65 years or older increased over the study years. In 2013, there was a 3.7% growth in persons age 65 years or older in the US population. The years of the economic downturn are highlighted in light gray.
The correlation, as denoted by the coefficient of determination (R 2), between National Health Expenditure, GDP, and total elective lumbar spine procedures relative to the population was not statistically significant (Table 3). However, the correlation between the S&P 500 Index and national elective lumbar surgical trends from 2003 to 2013 was statistically significant (P ≤ .05) with an R 2 of 0.37 (Table 3).
Table 3.
Results of Elective Lumbar Spine Surgery Trend Regressed Against Key Macroeconomic Factors.
| Macroeconomic Factor | R 2 | P |
|---|---|---|
| National health expenditure | .0112 | .76 |
| Gross domestic product | .0011 | .92 |
| Standard & Poor’s (S&P) 500 Index | .37 | .05* |
*P ≤ .05.
Discussion
The recent economic downturn from 2008 to 2009, the worst since the Great Depression, affected many lives. Our objective was to quantify the effect of this event on the trends of elective lumbar spine surgery. The economic downturn from 2008 to 2009 did not affect the incidence of elective lumbar spine surgeries in the United States even though unemployment increased, GDP contracted, and the real estate market collapsed. Typically, it is assumed that economic downturns affect individuals’ decisions to move forward with elective procedures, including elective lumbar spine surgeries. It is assumed as economic conditions worsen, individuals tend to save money in lieu of spending to stimulate economic growth. Yet our work suggests that such a significant decrease did not occur in lumbar spine surgical trends during and immediately after the Great Recession. This appears consistent with other studies analyzing trends in lumbar spine surgery in Western health care systems during our years of interest. While there is no work to our knowledge specifically addressing the effect of the economic downturn from 2008 to 2009, researchers in Belgium note of consistent increasing spine surgery trends through 2010.20 In addition, Swedish researchers have utilized the Swedish Spine Register to demonstrate an increasing trend in surgical lumbar spine interventions over our years of interest, which suggests that the economic downturn may not have affected spinal procedures within Sweden as well.21
The incidence of elective lumbar spine surgery relative to the employed population increased during the economic downturn from 2008 to 2009 (4.9%). In addition, the relationship from 2003 to 2013 between the incidence of elective lumbar spine surgery and National Health Expenditure and GDP was not statistically significant (Table 3). However, the relationship between the incidence of elective lumbar spine surgery and the S&P 500 Index was statistically significant (Table 3). Given these results, this could suggest that employed individuals will take advantage of their insurance coverage that may be coming from their employee during this time. Therefore, economic theory would suggest that employed individuals would be presumed to save the money they earn and utilize other means, such as private health insurance, to cover as much of the cost as possible. This finding, along with the fact that there was minimal impact of the economic downturn on lumbar spine surgery rates in the population, suggests that elective lumbar spine surgery is not a procedure that individuals tend to delay, regardless of economic conditions, and that may be due to other parties covering the costs.
The most surprising result of the analyses conducted with the macroeconomic factors was the noncorrelation between elective lumbar surgery trends and the National Health Expenditure. Elective lumbar spine surgery is an expensive, resource-heavy procedure that one could imagine as a driver for high health expenditures. Our results show that the incidence of elective lumbar spine surgeries is not likely a principal force driving the increasing National Health Expenditure.
The decrease in overall elective lumbar spine surgeries from 2010 to 2013 may be due to a number of factors outside of the delivery of care. For example, the passage of the ACA in 2010 brought the US health care system into an unknown territory. Indeed, many believed that such a law would cause a large disruption in the manner health care is delivered, including spine surgery. The changes to the current health care system are already underway with the experimentation of bundled payment solutions5,6,22,23 and a clear outline to move toward value-based reimbursement incentives over the coming years.24 In our study, in the years following the implementation of the ACA there was a negative impact on the rates of elective lumbar spine surgeries, both on the aggregate and individual elective surgery types. While one would think the ACA would lead to an increase in the rate of elective lumbar spine procedures due an increased access to health care, our results suggest otherwise.
In addition, private insurance companies in some states, such as North Carolina, implemented restrictive policies regarding reimbursement for spinal fusion for degenerative disc disease.9 This publicized policy may have been emulated by other insurance carriers in other states with even more to implement similar policies post-2013. Therefore, this change in private insurance coverage may have caused the decline seen in elective lumbar spine surgeries from 2010 to 2013.
Although overall rates of lumbar spine surgery increased during the economic downturn of 2008 to 2009, we specifically found that lumbar fusions increased (5.2%) while lumbar discectomies and laminectomies decreased by 1.3% and 2.2%, respectively. In the setting of an economic recession, patients may forgo the decompression procedure if symptoms are tolerable or if surgical recovery can affect their ability to return to work. Moreover, the surgeon may want to emphasize nonoperative management during an economic downturn if the initial surgical indications are borderline or as in the case of lumbar discectomies if there is evidence that in the long-term nonoperative management can be as effective as surgical intervention.25
Previous research by Kurtz et al indicated that the economic downturn from 2008 to 2009 had no impact on the rate of total knee and hip arthoplasties.13 Other work by Weinstein et al showed that lumbar fusion rates increased steadily from 1992 to 2003.3 In addition, Deyo et al showed that lumbar surgical rates declined from 2002 to 2007 but spinal fusion procedures increased dramatically.4 An important result from our study is that from 2010 to 2013, lumbar spinal fusion was the only elective lumbar spine surgery that saw any growth. This growth was from 2012 to 2013 (0.9%). The years 2010 to 2011 and 2011 to 2012 were the only decreases in the lumbar spine fusion rate since 2003.
Unlike Kurtz et al, we did not find a strong correlation between lumbar spine surgery and the National Health Expenditure. We also found that the economic downturn had no impact on the rate of lumbar spine surgery. Similar to Weinstein et al and Deyo et al, we saw an increasing trend in lumbar spinal fusions. However, we also witnessed a decline in lumbar surgical rates overall from 2010 to 2013.
The inconsistency with being able to predict the total number of elective lumbar spine surgeries poses a challenge. Indeed, some years show an increase in procedures while the next year shows a decrease with no clear explanation for the shift. Not being able to make an accurate year-to-year projection may hurt hospital budgeting, as spinal and orthopedic procedures are generally profitable. Additionally, the full impact of the ACA has not likely been felt, as the law implements different elements over time.26 Thus, the effect of the ACA on elective lumbar spine surgery must continue to be followed.
Our study has several limitations. Although we focused on the initial recession of 2008-2009, it is possible the ramifications of the recession may not have manifested until some years afterwards. In addition, intercensal data from the US Census Bureau are uncertain estimations that could alter our calculated trend of elective lumbar spine surgery relative to the different portions of the population. Another limitation is that NIS does not include ambulatory spine surgery data. Nationally there has been has an increase in outpatient lumbar spine surgeries.27,28 Since the NIS is limited to inpatient data it is possible the decrease in rates of lumbar discectomy and laminectomy seen in our study may be a lack of capture of the outpatient procedures. During our study period minimally invasive surgeries such as the lateral interbody fusion became popular. Lateral interbody fusion can lead to an increased foraminal height and some surgeons may forgo doing an open posterior decompression and rather place posterior-based percutaneous instrumentation only. In our analysis this may be reflected as a decrease in the rates of lumbar decompression. Last, we have the inherent limitations of relying on an administrative database (NIS). The data is reliant on proper entry of codes and limited by that quality of data input.
Conclusion
For the first time, our work provides an analysis of recent macroeconomic factors (Great Recession) and elective lumbar spine surgery trends up to the year 2013, which includes a timeframe of key health care policy changes. The economic downturn (2008-2009) did not affect the overall national trend of elective lumbar spine surgeries. While the passage of the ACA occurred in 2010, the ramifications of the new law and its impact on health care has numerous moving parts that make it challenging to know exactly the result of each change. Future works will be able to expand on our research by following the effects of the ACA and private insurance policy changes in more detail and over a longer time horizon. Further research can utilize our template to analyze the effects of the economic recession on cervical procedures as well as outpatient spine surgeries.
Footnotes
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Davis H. Increasing rates of cervical and lumbar spine surgery in the United States, 1979-1990. Spine (Phila Pa 1976). 1994;19:1117–1124. [DOI] [PubMed] [Google Scholar]
- 2. Deyo RA, Gray DT, Kreuter W, Mirza S, Martin BI. United States trends in lumbar fusion surgery for degenerative conditions. Spine (Phila Pa 1976). 2005;30:1441–1445. [DOI] [PubMed] [Google Scholar]
- 3. Weinstein JN, Lurie JD, Olson PR, Bronner KK, Fisher ES. United States’ trends and regional variations in lumbar spine surgery: 1992-2003. Spine (Phila Pa 1976). 2006;31:2707–2714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Deyo RA, Mirza SK, Martin BI, Kreuter W, Goodman DC, Jarvik JG. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA. 2010;303:1259–1265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Ugiliweneza B, Kong M, Nosova K, et al. Spinal surgery: variations in health care costs and implications for episode-based bundled payments. Spine (Phila Pa 1976). 2014;39:1235–1242. [DOI] [PubMed] [Google Scholar]
- 6. Rossi VJ, Ahn J, Bohl DD, Tabaraee E, Singh K. Economic factors in the future delivery of spinal healthcare. World J Orthop. 2015;6:409–412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Acosta FL, Jr, Ames C, Hsieh PC, McCarthy IM. Introduction: costs and benefits of modern-day spine care. Neurosurg Focus. 2014;36:Introduction. doi:10.3171/2014.4.FOCUS14124. [DOI] [PubMed] [Google Scholar]
- 8. Borden WB, Chiang YP, Kronick R. Bringing patient-centered outcomes research to life. Value Health. 2015;18:355–357. [DOI] [PubMed] [Google Scholar]
- 9. Martin BI, Deyo RA, Lurie JD, Carey TS, Tosteson AN, Mirza SK. Effects of a commercial insurance policy restriction on lumbar fusion in North Carolina and the implications for national adoption. Spine (Phila Pa 1976). 2016;41:647–655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Jancuska JM, Hutzler L, Protopsaltis TS, Bendo JA, Bosco J. Utilization of lumbar spinal fusion in New York state: trends and disparities. Spine (Phila Pa 1976) 2016;41:1508–1514. [DOI] [PubMed] [Google Scholar]
- 11. Stain SC, Hoyt DB, Hunter JG, Joyce G, Hiatt JR. American surgery and the Affordable Care Act. JAMA Surg. 2014;149:984–985. [DOI] [PubMed] [Google Scholar]
- 12. Hoyt DB, Schneidman DS. The American College of Surgeons: an enduring commitment to quality and patient care. Am J Surg. 2015;209:436–441. [DOI] [PubMed] [Google Scholar]
- 13. Kurtz SM, Ong KL, Lau E, Bozic KJ. Impact of the economic downturn on total joint replacement demand in the United States: updated projections to 2021. J Bone Joint Surg Am. 2014;96:624–630. [DOI] [PubMed] [Google Scholar]
- 14. Healthcare Cost and Utilization Project. NIS database documentation. Rockville, MD: Agency for Healthcare Research and Quality; https://www.hcup-us.ahrq.gov/db/nation/nis/nisdbdocumentation.jsp. Accessed June 1, 2015. [Google Scholar]
- 15. US Census Bureau. Population estimates: intercensal estimates. http://www.census.gov/popest/data/intercensal/index.html. Accessed March 23, 2016.
- 16. US Department of Labor, Bureau of Labor Statistics. Labor force statistics from the Current Population Survey. http://www.bls.gov/web/empsit/cpseea01.htm. Accessed March 23, 2016.
- 17. Center for Medicare & Medicaid Services. National health expenditure data, historical. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/NationalHealthAccountsHistorical.html. Accessed March 23, 2016.
- 18. US Department of Commerce, Bureau of Economic Analysis. GDP & personal income, national data. http://www.bea.gov/iTable/index_nipa.cfm. Accessed March 23, 2016.
- 19. Yahoo! Finance. S&P 500, Historical prices. http://finance.yahoo.com/q/hp?s=%5EGSPC&a=00&b=1&c=2004&d=00&e=2&f=2013&g=m&z=66&y=66. Accessed March 23, 2016.
- 20. Du Bois M, Szpalski M, Donceel P. A decade’s experience in lumbar spine surgery in Belgium: sickness fund beneficiaries, 2000–2009. Eur Spine J. 2012;21:2693–2703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Strömqvist B, Fritzell P, Hägg O, Jönsson B, Sandén B. Swedish Society of Spinal Surgeons. Swespine: the Swedish spine register: The 2012 report. Eur Spine J. 2013;22:953–974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Centers for Medicare & Medicaid Services. Bundled Payments for Care Improvement (BPCI) initiative: general information. http://innovation.cms.gov/initiatives/bundled-payments/. Accessed June 21, 2015.
- 23. Froimson MI, Rana A, White RE, Jr, et al. Bundled payments for care improvement initiative: the next evolution of payment formulations: AAHKS Bundled Payment Task Force. J Arthroplasty. 2013;28:157–165. [DOI] [PubMed] [Google Scholar]
- 24. US Department of Health & Human Services. Better, smarter, healthier: In historic announcement, HHS sets clear goals and timeline for shifting Medicare reimbursements from volume to value. http://www.hhs.gov/news/press/2015pres/01/20150126a.html. Accessed June 27, 2015.
- 25. Kerr D, Zhao W, Lurie JD. What are long-term predictors of outcomes for lumbar disc herniation? A randomized and observational study. Clin Orthop Relat Res. 2015;473:1920–1930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. The Henry J. Kaiser Family Foundation. Health reform implementation timeline. http://kff.org/interactive/implementation-timeline/. Accessed July 14, 2015.
- 27. Bekelis K, Missios S, Kakoulides G, Rahmani R, Simmons N. Selection of patients for ambulatory lumbar discectomy: results from four US states. Spine J. 2014;14:1944–1950. [DOI] [PubMed] [Google Scholar]
- 28. Gray DT, Deyo RA, Kreuter W, et al. Population-based trends in volumes and rates of ambulatory lumbar spine surgery. Spine (Phila Pa 1976). 2006;31:1957–1963. [DOI] [PubMed] [Google Scholar]