

Abstract
Introduction
African American and Latino children experience higher rates of traumatic injury and mortality, but the extent to which parents of different races and ethnicities disparately enact injury prevention behaviors has not been fully characterized. The objective of this study is to evaluate the association between caregiver race/ethnicity and adherence to injury prevention recommendations.
Methods
This was a cross-sectional analysis of caregiver-reported baseline data from the Greenlight study, a cluster-randomized pediatric obesity prevention trial. Data were collected between 2010 and 2012 in four academic pediatric practices and analyzed in 2015. Non-adherence to injury prevention recommendations was based on five domains: car seat safety, sleeping safety, fire safety, hot water safety, and fall prevention.
Results
Among 864 caregiver–infant pairs (17.7% white, non-Hispanic; 49.9% Hispanic; 27.7% black, non-Hispanic; 4.7 % other, non-Hispanic), mean number of non-adherent injury prevention behaviors was 1.8 (SD=0.9). In adjusted regression, Hispanic caregivers had higher odds of non-adherence to car seat safety (AOR=2.1, 95% CI=1.2, 3.8), and lower odds of non-adherence with fall prevention (AOR=0.4, 95% CI=0.3, 0.7) compared with whites. Black, non-Hispanic caregivers had higher odds of non-adherence to car seat safety (AOR=2.4, 95% CI=1.3, 4.4) and sleeping safety (AOR=2.1, 95% CI=1.3, 3.2) but lower odds of fall prevention non-adherence (AOR=0.5, 95% CI=0.3, 0.8) compared with whites.
Conclusions
A high prevalence of non-adherence to recommended injury prevention behaviors is common across racial/ethnic categories for caregivers of infants among a diverse sample of families from low-SES backgrounds.
Introduction
Sudden infant death syndrome and unintentional injuries are two leading causes of infant mortality, with rates increasing over the last decade.1 The Centers for Disease Control and Prevention reports that in 2013 sudden infant death syndrome accounted for 6.7% of infant deaths and unintentional injury accounted for 4.9% of infant deaths.2 In 2011, the American Academy of Pediatrics published a report highlighting the importance of providing a safe sleep environment to prevent sudden infant death syndrome and other forms of sleep-related deaths, including suffocation, asphyxia, and entrapment (collectively known as sudden unexpected infant death).3 In children aged <1 year, leading causes of unintentional injuries include falls, motor vehicle crashes, and fire-related injuries.4 These causes of infant death are largely preventable, but caregiver safety practices often do not match well-established injury prevention recommendations.5–7 African American and Latino children have disproportionately higher rates of traumatic injury and suffer worse outcomes from those injuries.8,9 The greatest disparities have been reported for safe car seat use: African American children are less likely to be both seated in a car seat and properly restrained.10,11
However, several gaps remain in understanding why there are racial disparities in infant injuries. Specifically, previous studies have focused largely on a single injury prevention behavior instead of a broad range of recommended practices. Additionally, most studies compare injury rates and behaviors in African American families with white families. Data are limited on injury prevention behaviors of Latino families or the extent to which acculturation is related to adherence to recommended behaviors. In previous work, the authors have demonstrated associations between health literacy and injury prevention behaviors among caregivers of 2-month-old infants, indicating that this is an important age group in which to consider mutable behaviors to reduce unintentional injury.12 Furthermore, injury prevention approaches often employ social marketing techniques focused on specific communities, underscoring the importance of recognizing how these injury prevention behaviors might vary based on race or ethnicity. Therefore, the purpose of this study is to explore variation by race/ethnicity in a broad range of injury prevention behaviors among a racially diverse sample of families from low-SES backgrounds.
Methods
The authors performed a cross-sectional analysis of baseline data from the Greenlight study, which is a cluster-randomized trial to prevent obesity in the first 2 years of life. The Greenlight study was conducted at pediatric resident primary care clinics at four university-affiliated medical centers:
New York University/Bellevue Hospital Center;
Vanderbilt University;
University of North Carolina–Chapel Hill; and
University of Miami/Jackson Memorial Medical Center.
Two sites received an obesity prevention intervention and two sites received an attention control condition focusing on injury prevention. The full methods of Greenlight have been previously published.13
Caregiver–child dyads were consecutively recruited to participate in the Greenlight study from April 28, 2010 to August 30, 2012 at 2-month well-child visits. Inclusion criteria for caregiver–child dyads were:
infant aged 6–16 weeks presenting for a 2-month well-child visit with a pediatric resident;
a caregiver who spoke English or Spanish, who
reported that they planned to return to the clinic for all well-child visits through age 2 years.
Child-related exclusion criteria were:
<34 weeks gestation;
birth weight <1,500 grams;
weight for length <third percentile at 2-month visit; or
diagnosis of failure to thrive or other medical problem known to affect child growth (e.g., cleft palate).
Caregiver-related exclusion criteria were:
age <18 years
significant mental/neurological illness; or
poor visual acuity (Rosenbaum Pocket Screener; worse than 20/50 corrected vision).
Written informed consent was obtained from all participants. IRB approval was obtained from all four participating academic medical centers. Data for this analysis were obtained by in-person interviews at the 2-month well-child visit. Questionnaires were administered in English or Spanish, based on caregiver preference. Study data were managed using the secure Research Electronic Data Capture tools hosted at Vanderbilt University.14
Measures
The primary independent variable for this study was caregiver race/ethnicity. To measure race, caregivers were asked to select from the following six options: American Indian or Alaskan Native, Asian, black or African American, Native Hawaiian or other Pacific Islander, white, or other. A brief description of people who might identify with each race followed each option and participants were allowed to select more than one response. To measure ethnicity, caregivers were asked: Do you consider yourself Hispanic/Latino? Based on responses to these items, caregiver race/ethnicity was categorized as four mutually exclusive categories: Hispanic; white, non-Hispanic; black, non-Hispanic; or other, non-Hispanic. This grouping was chosen as the “other” group consisted of multiple smaller groups that were too small to consider individually.
The primary outcomes of interest were caregiver reports of injury prevention practices. For this analysis, injury prevention practices were analyzed within five injury prevention domains that the authors had developed for a previous analysis.12 Injury prevention domains were based on recommendations by the American Academy of Pediatrics, The Injury Prevention Program, and the leading causes of preventable injuries in children.3,4 Injury prevention practices were assessed using a questionnaire developed by the Greenlight study team and other national experts in injury prevention.12 The following domains were selected a priori and analyzed for this study:
car seat safety;
sleeping safety;
fire safety;
hot water safety; and
fall prevention.
The specific items used to assess these domains, and how non-adherence was defined, are listed in Table 1. Car seat safety was assessed with five items; a respondent was classified as non-adherent with a non-adherent response to any one of those five items. To account for respondents who were non-adherent to more than one injury prevention behavior, an injury prevention risk score (range, 0–9) was created, representing the number of behaviors the respondent reported as non-adherent. For the risk score, each of the five car seat safety items was counted individually.
Table 1.
Injury Prevention Outcomes and Associated Survey Questions
| Domain of AAP injury prevention recommendation | Survey question | Answers qualifying for non-adherent | % (N) non-adherent |
|---|---|---|---|
| Car seat safetya | Do you have a car seat for your child? | No, and child rides in car. | 23.6% (201) |
| Where do you place the car seat? (Front/Back) | Front, and my car has a back seat | ||
| Does your car seat face the front or back? | Front | ||
| In the last 30 days, how many times has [child’s first name] been in a moving car or vehicle without being strapped in the car seat even for a brief moment? | ≥1 | ||
| While in the car, do you ever take [child’s first name] out of the car seat while the car is moving for a short time, like to feed him or if she is fussy? | Yes | ||
| Sleeping safety | In the last 30 days how many times has your child slept on his/her tummy? | ≥1 | 42.8% (364) |
| Fire safety | Do you have a working smoke detector on every level of your home? | No, or I don’t Know | 6.6% (56) |
| Hot water heater | What is the temperature setting on your hot water heater? | >120°F, or I don’t know | 88.8% (756) |
| Fall prevention | To the best of your knowledge, have you or anyone in your family ever left your child alone on a table, sofa, bed, or other high place, even for a brief moment, while they turned or stepped away? | Yes | 22.9% (195) |
These outcomes are based on answers to multiple questions. A non-adherent answer to any one of the questions classifies the respondent as non-adherent for that outcome.
AAP, American Academy of Pediatrics
Demographic characteristics, including child age, child gender, caregiver gender, caregiver age, relationship to child (mother, father, other), caregiver education, household Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) status, and household income, were summarized using mean (SD) for continuous variables and using proportions for categorical variables. Education was categorized as less than a high school education, high school graduate/equivalent, some college, or college graduate or higher level. Annual household income was measured by self-report (<$20,000 versus ≥$20,000). Household WIC status was also measured by caregiver self-report, and was coded as enrolled if either the caregiver or child was enrolled at the time of the interview. Among Latino participants, acculturation was also measured using the Short Acculturation Scale for Hispanics and by caregiver nativity (caregiver born in the U.S. versus caregiver not born in the U.S.).15 This is a 12-item scale that measures behavioral and cultural values, consisting of three factors (language, media, and social relationships). Each item is scored on a 5-point Likert scale and items are averaged to create a final score (range, 1–5). Previously validated cut-points have used a score of 2.99, where a person is less acculturated if the score is between 1 and 2.99.16
Statistical Analysis
Differences in demographic characteristics by race/ethnicity were assessed using Pearson chi-square tests. Unadjusted and adjusted associations were assessed between caregiver race/ethnicity and each of the five safety domains using logistic regression. When considering the association between caregiver race/ethnicity and the combined risk score (range, 0–9), adjusted ordered logistic regression was used. Covariates were chosen a priori for adjusted analyses, including:
child age;
child gender;
caregiver age;
household WIC status;
caregiver education; and
study arm (intervention versus control).
This study did not include caregiver gender or caregiver relationship as covariates in adjusted models because >96% of respondents were mothers. The authors also conducted a subgroup analysis of Latino caregivers to determine if acculturation was associated with the outcomes of interest. Data were analyzed in 2015 using Stata, version 14.0. For all analyses, a two-tailed p-value <0.05 was considered statistically significant.
Results
Among the 864 caregiver–child pairs included in this analysis (who had complete race/ethnicity data), the mean age at enrollment for the index child was 9.3 (SD=1.8) weeks. Approximately half of the children enrolled were female (51.3%) and the majority of caregivers were mothers (95.7%). Caregivers enrolled in this study were from low-SES backgrounds, with 85.1% of households enrolled in WIC and 59.6% of household annual incomes <$20,000.
Nearly half (49.9%) of the enrolled sample identified as Hispanic, whereas 153 (17.7%) caregivers identified as white, non-Hispanic, 239 (27.6%) caregivers identified as black, non-Hispanic, and 41 (4.7%) caregivers identified as one of the additional race categories. Fourteen individuals (1.6%) identified as more than one race. Demographic characteristics of the sample are compared across race/ethnicity categories in Table 2. There were significant differences, including higher percentages of WIC enrollment, lower educational attainment, and higher percentages with household incomes <$20,000 among Hispanic and black, non-Hispanic families. The percentage of caregivers not adhering to recommended injury prevention behaviors is summarized in Table 1. On average, each caregiver endorsed almost two non-adherent behaviors (mean=1.8, SD=0.9), with 95% of families engaging in at least one non-adherent behavior, and 10% of families engaging in three non-adherent behaviors. In the domain of car seat safety, 23.6% of families reported non-adherent behaviors: 21.5% reported taking their infant out of the car seat while the car was moving in the last 30 days; 5.1% caregivers reported that their infant was front facing instead of rear; and 0.9% rode in a car without a car seat. In the domain of safe sleep, 15.6% placed their infant on their tummy to sleep one to two times/month, and 11.8% of caregivers placed their infants on their tummy to sleep more than ten times/month. In the domain of fire and burn safety, 6.6% of caregivers did not have or did not know if they had a working smoke detector in their home. Only 11.3% of caregivers reported that their hot water heater was set to ≤120°F, whereas 2.7% knew their hot water heater was >120°F, and 733 (86.0%) did not know the temperature of their hot water heater.
Table 2.
Baseline Demographics by Race/Ethnicity
| Race/Ethnicity | |||||
|---|---|---|---|---|---|
|
| |||||
| Overall (n=864) | Hispanic (n=431) | Non-Hispanic, white (n=153) | Non-Hispanic, black (n=239) | Non-Hispanic, other (n=41) | |
|
| |||||
| Mean (SD) or n (%) |
Mean (SD) or n (%) |
Mean (SD) or n (%) |
Mean (SD) or n (%) |
Mean (SD) or n (%) |
|
| Child age (weeks) | 9.3 (1.8) | 9.3 (1.7) | 9.2 (1.8) | 9.4 (1.9) | 9.1 (1.4) |
| Child gender (female) | 443 (51.3%) | 214 (49.7%) | 76 (49.7%) | 132 (55.2%) | 21 (51.2%) |
| WIC status | |||||
| (Caregiver or child enrolled) | 730 (85.1%) | 389 (90.3%) | 96 (62.8%) | 220 (92.1%) | 25 (61.0%) |
| Caregiver age (years) | 27.7 (6.1) | 28.3 (6.0) | 26.9 (5.8) | 26.7 (6.2) | 30.5 (6.4) |
| Caregiver gender, female | 826 (95.6%) | 415 (96.3%) | 148 (96.7%) | 228 (95.4%) | 35 (85.4%) |
| Caregiver education | |||||
| Less than HS graduate | 225 (26.2%) | 176 (40.8%) | 13 (8.5%) | 35 (14.6%) | 1 (2.4%) |
| HS graduate/equiv | 280 (32.6%) | 129 (29.9%) | 44 (28.8%) | 101 (42.3%) | 6 (14.6%) |
| Some college | 200 (23.3%) | 68 (15.8%) | 51 (33.3%) | 69 (28.9%) | 12 (29.3%) |
| College or greater | 153 (17.8%) | 56 (13.0%) | 42 (27.5%) | 33 (13.8%) | 22 (53.7%) |
| Household income | |||||
| <$20,000 | 494 (59.6%) | 282 (65.4%) | 50 (32.7%) | 146 (61.1%) | 15 (36.6%) |
| Site | |||||
| NYU | 229 (26.5%) | 180 (41.8%) | 15 (9.8%) | 22 (9.2%) | 12 (29.3%) |
| Miami | 150 (17.4%) | 76 (17.6%) | 7 (4.6%) | 55 (23.0%) | 12 (12.3%) |
| UNC Chapel Hill | 255 (29.5%) | 97 (22.5%) | 61 (39.9%) | 87 (36.4%) | 10 (24.4%) |
| Vanderbilt | 230 (26.6%) | 78 (18.1%) | 70 (45.8%) | 75 (31.4%) | 7 (17.1) |
Notes: Boldface indicates statistical significance (p<0.05 for χ2).
Demographics are presented as mean (SD) for continuous variables or n (%) for categorical variables by caregiver race/ethnicity.
Column percentages are presented.
WIC, Women, Infants, and Children; HS, high school; NYU, New York University; UNC, University of North Carolina
Unadjusted associations between race/ethnicity and injury prevention behaviors are shown in Figure 1. The highest rate of non-adherence to car seat safety was among black, non-Hispanic (27.8%) and other, non-Hispanic (30.0%) caregivers. The highest rate of sleeping non-adherence was among black, non-Hispanic (56.0%) caregivers. The highest rate of fire safety non-adherence was among other, non-Hispanic (12.5%) caregivers. The highest rate of hot water non-adherence (91.6%) was among Hispanic caregivers. The highest rate of fall non-adherence was among white, non-Hispanic caregivers (38.9%). Overall black, non-Hispanic caregivers reported an average of 2.0 (SD=1.0) non-adherent behaviors, compared to 1.8 (SD=1.0) non-adherent behaviors for white, non-Hispanic caregivers, 1.8 (SD=0.91) non-adherent behaviors for Hispanic caregivers, and 1.7 (SD=0.89) non-adherent behaviors for other, non-Hispanic caregivers (ANOVA, p=0.06). Unadjusted ordered logistic regression showed that caregivers who self-identified as black, non-Hispanic had higher odds of an increased number of non-adherent injury prevention behaviors (OR=1.5, 95% CI=1.02, 2.20, p=0.04) compared with white, non-Hispanic caregivers. Hispanic (OR=1.0, 95% CI=0.74, 1.48, p=0.80) and other, non-Hispanic (OR=0.8, 95% CI=0.40, 1.45, p=0.40) caregivers did not have statistically significant different odds compared to white, non-Hispanic caregivers. In ordered logistic regression models, injury prevention risk was not associated with acculturation when measured by Short Acculturation Scale for Hispanics (OR=0.9, 95% CI=0.76, 1.15, p=0.50) or by caregiver nativity (OR=0.9, 95% CI=0.68, 1.12, p=0.30).
Figure 1. Rates of non-adherence to five injury prevention recommendations by caregiver race/ethnicity.
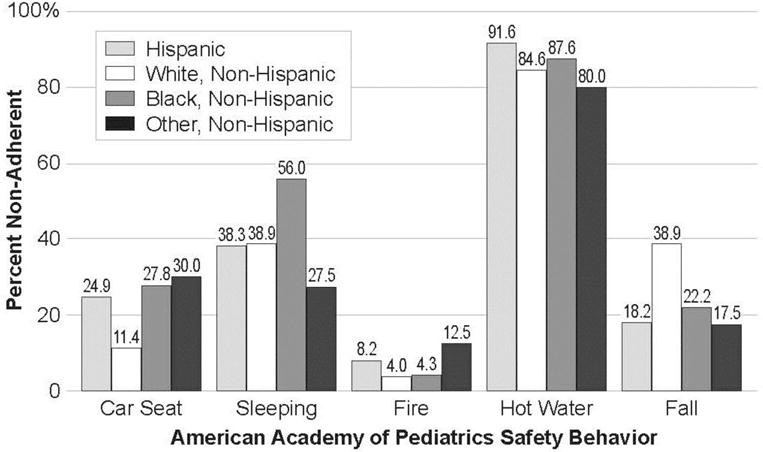
Notes: χ2 indicates that car seat safety, sleeping safety, and fall prevention are all significantly different by caregiver race/ethnicity (p<0.001) and that hot water safety is significantly different by caregiver race/ethnicity (p<0.05). There is no difference in the percent of caregivers adherent to fire safety based on caregiver race/ethnicity.
Results from adjusted logistic regression models are displayed in Table 3. Disparities in injury prevention behaviors were present in car seat safety, sleeping safety, and fall prevention safety. Compared with white, non-Hispanic caregivers, Hispanic (AOR=2.1, 95% CI=1.2, 3.8), black, non-Hispanic (AOR=2.4, 95% CI=1.3, 4.4), and other, non-Hispanic (AOR=3.5, 95% CI=1.5, 8.3) caregivers all had increased odds of non-adherence to recommended car seat safety behaviors. Compared with white, non-Hispanic caregivers, black, non-Hispanic caregivers had increased odds of non-adherence to recommended safe sleep behaviors (AOR=2.1, 95% CI=1.3, 3.2). Compared with white, non-Hispanic caregivers, Hispanic (AOR=0.4, 95% CI=0.3, 0.7), black, non-Hispanic (AOR=0.5, 95% CI=0.3, 0.8), and other, non-Hispanic (AOR=0.3, 95% CI=0.1, 0.8) caregivers had decreased odds of non-adherence to fall safety recommendations. Adjusted ordered logistic regression testing the association between the total number of non-adherent behaviors and race/ethnicity showed that black, non-Hispanic caregivers had increased odds (AOR=1.5, 95% CI=1.00, 2.3) of non-adherence compared with white, non-Hispanic caregivers. A pre-specified subgroup analysis of Latino caregivers did not show any difference in adherence to recommended behaviors based on acculturation.
Table 3.
Adjusted Odds of Non-Adherence to Injury Prevention Practices Based on Caregiver Race/Ethnicity
| White, non-Hispanic | Hispanic | Black, non-Hispanic | Other, non-Hispanic | ||
|---|---|---|---|---|---|
|
| |||||
| Injury prevention practice | n | Adjusted OR for non-adherence a (95% CI) | |||
| Car seat safety | 829 | ref | 2.1 (1.2, 3.8) * | 2.4 (1.3, 4.4) * | 3.5 (1.5,8.3) * |
| Sleeping safety | 828 | ref | 1.0 (0.7,1.6) | 2.1 (1.3, 3.2) * | 0.7 (0.3, 1.5) |
| Fire safety | 829 | ref | 2.0 (0.8, 5.3) | 1.1 (0.4, 3.1) | 3.3 (0.9, 11.9) |
| Hot water heater | 829 | ref | 1.6 (0.8, 3.0) | 1.1 (0.6, 2.2) | 0.9 (0.4, 2.3) |
| Fall prevention | 829 | ref | 0.4 (0.3, 0.7) ** | 0.5 (0.3, 0.8) * | 0.3 (0.1, 0.8) * |
| Total injury prevention Practices | 829 | ref | 1.0 (0.7, 1.5) | 1.5 (1.0, 2.3) * | 0.9 (0.5, 1.7) |
Notes: Adjusted for child age, child gender, household WIC status, caregiver age, caregiver education, and study site.
Total Injury Prevention Practices (range 0–9) represents the sum of non-adherent responses measured by 9 items in each of the 5 listed injury prevention domains.
Boldface indicates statistical significance:
p<0.05;
p<0.001
Discussion
In this sample of low-income caregiver–child pairs, the data show both high rates of non-adherence and racial/ethnic differences in well-established injury prevention behaviors for caregivers of 2-month-old infants. The mean number of non-adherent behaviors among all caregivers in this sample is 1.8 (SD=0.9), with 95% of families engaging in at least one non-adherent behavior and 10% of families engaging in three or more non-adherent behaviors. Black, non-Hispanic caregivers had increased odds of engaging in a higher number of non-adherent behaviors, when compared with non-black caregivers. For specific domains, however, no consistent pattern of ethnic/racial differences was found in safety behaviors. For example, white, non-Hispanic caregivers had increased odds of being non-adherent to fall-prevention recommendations, when compared with non-white caregivers; Hispanic caregivers had increased odds of being non-adherent to car-safety recommendations, when compared with most non-Hispanic caregivers; and black, non-Hispanic caregivers had increased odds of being non-adherent for sleeping safety, when compared with non-black caregivers. These unique patterns of adherence to injury prevention behaviors highlight the potential opportunities to tailor injury prevention strategies to specific communities. Although tailored injury prevention approaches for racial/ethnic groups disparately affected by adverse outcomes should be examined, the high rates of non-adherence to recommended safety behaviors among all race/ethnicity groups suggest universal opportunities to improve caregivers’ injury-related health behaviors in early infancy.
Previous literature has consistently identified disparate rates of injury and injury prevention behaviors among low-income populations from traditionally under-represented minorities.8,9 These findings align with previous studies that reported lower seat belt use and sleeping safety among black, non-Hispanic and white, non-Hispanic families.11,17,18 In one study of 1,268 children (average age of 9.8 years), black children were less likely to be appropriately restrained in a motor vehicle than white children (22.2% vs 12.7%, p<0.001).10 Also, in another study, black and Hispanic caregivers had different behaviors related to safe infant sleep, with black infants more likely to be placed prone.18 This study builds on this literature by showing that these non-adherence behaviors are prevalent as early as 2 months. The data also showed increased odds of non-adherence to car seat safety not only for black, non-Hispanic families, but also for Hispanic and other, non-Hispanic families. However, among the subset of participants who identified as Latino, acculturation was not associated with adherence to recommended injury prevention behaviors. Finally, this is the first report that white, non-Hispanic families are more likely to be non-adherent to fall prevention behaviors.
Race and ethnicity are important social determinants of health, and it is a clear public health imperative to reduce health disparities based on race and ethnicity. However, the causal mechanism between race/ethnicity and health disparities is more elusive. By including markers of SES in adjusted models, these results indicate that race and ethnicity have a unique contribution to injury prevention behaviors beyond socioeconomics. Whether race/ethnicity serves as a marker for cultural differences or another unmeasured factor is difficult to ascertain, given the vast variation in culture among such coarse groupings of racial/ethnic categories used in this analysis. As society strives to reduce racial/ethnic health disparities, the authors urge the research community to consider additional and more-refined approaches to measuring and assessing the role of race and ethnicity. Specifically, future research should focus on the etiology of these health disparities (e.g., the role of culture, local laws, possible provider bias) that may influence adherence to injury prevention recommendations so that appropriate preventive recommendations can address barriers in a wide range of contexts.
Limitations
There are several limitations to the reported findings. This is a cross-sectional analysis; therefore, causal inferences cannot be drawn. Furthermore, the authors did not have the capacity to consider mechanisms that would potentially explain the relationships between race/ethnicity and non-adherence to injury prevention recommendations. The study was initiated in 2010, so contemporaneous recommendations about safe sleep were used, though these do not account for more recent recommendations by the American Academy of Pediatrics for safe sleep.3 The injury prevention outcomes were based on self-reported survey data that may not reflect actual injury prevention behaviors or injury outcomes. For example, when asked about the temperature of their hot water heater, a participant may have answered I don’t know when the temperature may have been safely set or a participant may not have known the correct answer based on how some heaters have ordinal (low, medium, high) settings. Furthermore, participants may have been susceptible to social desirability bias, which may have differed by the exposure (race/ethnicity) making the direction of the bias difficult to predict. However, the reported prevalence of injury prevention behaviors was high, suggesting either that under-reporting may not have been problematic or that the rates of non-adherence to injury prevention behaviors is even worse than noted here.
Conclusions
This study identifies a high prevalence of non-adherence to recommended injury prevention behaviors across racial and ethnic categories for caregivers of infants among a diverse sample of families of low SES. Future work should focus on causal relationships between a wide range of social determinants of health, including race/ethnicity, and injury prevention behaviors. Recognizing the high and disparate rate of non-adherence to injury prevention behaviors is important for both pediatric healthcare providers as they provide anticipatory guidance and for public health officials who design policies and programs to reduce the rates of injury. In particular, these data identify opportunities to tailor specific interventions for racial/ethnic groups disparately affected by adverse injury outcomes. In the meantime, these findings call for universal approaches to injury prevention counseling for all parents of young infants and highlight the need for further research to determine the etiologic underpinnings behind certain infant safety practices.
Acknowledgments
This research was supported with funding from NIH/National Institute of Child Health and Human Development (NICHD) (R01 HD049794), NIH (NICHD and OBSSR), and the Centers for Disease Control and Prevention supplements to examine injury prevention issues (R01HD059794-04S1, R01HD059794-04S2), NIH/National Center for Advancing Translational Sciences (NCATS) (U54 RR023499 and UL1RR025747), the New York University CTSI (UL1 TR000038), and the KiDS of New York University Foundation. Dr. Heerman’s time was supported by a K12 grant from the Agency for Healthcare Research and Quality (1K12HS022990). Clinical Trial Registry Name and Number: Addressing Health Literacy and Numeracy to Prevent Childhood Obesity; NCT01040897.
Footnotes
No financial disclosures were reported by the authors of this paper.
References
- 1.CDC. Vital signs: Unintentional injury deaths among persons aged 0–19 years - United States, 2000–2009. MMWR Morb Mortal Wkly Rep. 2012;61:270–276. [PubMed] [Google Scholar]
- 2.CDC. WISQARS Leading Causes of Death Reports, National and Regional, 2013. 2013 Accessed September 18, 2015. http://webappa.cdc.gov/sasweb/ncipc/leadcaus10_us.html.
- 3.Task Force on Sudden Infant Death S. Moon RY. SIDS and other sleep-related infant deaths: expansion of recommendations for a safe infant sleeping environment. Pediatrics. 2011;128(5):1030–1039. doi: 10.1542/peds.2011-2284. http://dx.doi.org/10.1542/peds.2011–2284. [DOI] [PubMed] [Google Scholar]
- 4.Agran PF, Anderson C, Winn D, Trent R, Walton-Haynes L, Thayer S. Rates of pediatric injuries by 3-month intervals for children 0 to 3 years of age. Pediatrics. 2003;111(6 Pt 1):e683–692. doi: 10.1542/peds.111.6.e683. http://dx.doi.org/10.1542/peds.111.6.e683. [DOI] [PubMed] [Google Scholar]
- 5.Gielen AC, McDonald EM, Wilson ME, et al. Effects of improved access to safety counseling, products, and home visits on parents’ safety practices: results of a randomized trial. Arch Pediatr Adolesc Med. 2002;156(1):33–40. doi: 10.1001/archpedi.156.1.33. http://dx.doi.org/10.1001/archpedi.156.1.33. [DOI] [PubMed] [Google Scholar]
- 6.Gielen AC, Wilson ME, McDonald EM, et al. Randomized trial of enhanced anticipatory guidance for injury prevention. Arch Pediatr Adolesc Med. 2001;155(1):42–49. doi: 10.1001/archpedi.155.1.42. http://dx.doi.org/10.1001/archpedi.155.1.42. [DOI] [PubMed] [Google Scholar]
- 7.Brice JH, Overby BA, Hawkins ER, Fihe EL. Determination of infant-safe homes in a community injury prevention program. Prehosp Emerg Care. 2006;10(3):397–402. doi: 10.1080/10903120600726007. http://dx.doi.org/10.1080/10903120600726007. [DOI] [PubMed] [Google Scholar]
- 8.Brown RL. Epidemiology of injury and the impact of health disparities. Curr Opin Pediatr. 2010;22(3):321–325. doi: 10.1097/MOP.0b013e3283395f13. http://dx.doi.org/10.1097/MOP.0b013e3283395f13. [DOI] [PubMed] [Google Scholar]
- 9.Falcone RA, Jr, Brown RL, Garcia VF. The epidemiology of infant injuries and alarming health disparities. J Pediatr Surg. 2007;42(1):172–176. doi: 10.1016/j.jpedsurg.2006.09.015. discussion 176–177. http://dx.doi.org/10.1016/j.jpedsurg.2006.09.015. [DOI] [PubMed] [Google Scholar]
- 10.Rangel SJ, Martin CA, Brown RL, Garcia VF, Falcone RA., Jr Alarming trends in the improper use of motor vehicle restraints in children: implications for public policy and the development of race-based strategies for improving compliance. J Pediatr Surg. 2008;43(1):200–207. doi: 10.1016/j.jpedsurg.2007.09.045. http://dx.doi.org/10.1016/j.jpedsurg.2007.09.045. [DOI] [PubMed] [Google Scholar]
- 11.Briggs NC, Schlundt DG, Levine RS, Goldzweig IA, Stinson N, Jr, Warren RC. Seat belt law enforcement and racial disparities in seat belt use. Am J Prev Med. 2006;31(2):135–141. doi: 10.1016/j.amepre.2006.03.024. http://dx.doi.org/10.1016/j.amepre.2006.03.024. [DOI] [PubMed] [Google Scholar]
- 12.Heerman WJ, Perrin EM, Yin HS, et al. Health literacy and injury prevention behaviors among caregivers of infants. Am J Prev Med. 2014;46(5):449–456. doi: 10.1016/j.amepre.2014.01.005. http://dx.doi.org/10.1016/j.amepre.2014.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sanders LM, Perrin EM, Yin HS, Bronaugh A, Rothman RL, Greenlight Study T “Greenlight study”: a controlled trial of low-literacy, early childhood obesity prevention. Pediatrics. 2014;133(6):e1724–1737. doi: 10.1542/peds.2013-3867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi: 10.1016/j.jbi.2008.08.010. http://dx.doi.org/10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Marin G, Sabogal F, Marin BV, Oterosabogal R, Perezstable EJ. Development of a Short Acculturation Scale for Hispanics. Hisp J Behav Sci. 1987;9(2):183–205. http://dx.doi.org/10.1177/07399863870092005. [Google Scholar]
- 16.Davis LE, Engel RJ, Gurin P. Measuring race and ethnicity. New York: Springer; 2011. http://dx.doi.org/10.1007/978-1-4419-6697-1. [Google Scholar]
- 17.Chu T, Hackett M, Simons H. Maternal nativity and sleep-related infant injury deaths in New York City. Early Hum Dev. 2015;91(1):13–17. doi: 10.1016/j.earlhumdev.2014.10.005. http://dx.doi.org/10.1016/j.earlhumdev.2014.10.005. [DOI] [PubMed] [Google Scholar]
- 18.Mathews AA, Joyner BL, Oden RP, Alamo I, Moon RY. Comparison of Infant Sleep Practices in African-American and U.S. Hispanic Families: Implications for Sleep-Related Infant Death. J Immigr Minor Health. 2015;17(3):834–842. doi: 10.1007/s10903-014-0016-9. http://dx.doi.org/10.1007/s10903-014-0016-9. [DOI] [PMC free article] [PubMed] [Google Scholar]