

Abstract
The current International Organization for Standardization (ISO) standard (ISO 8600-3: 1997 including Amendment 1: 2003) for determining endoscope field of view (FOV) does not accurately characterize some novel endoscopic technologies such as endoscopes with a close focus distance and capsule endoscopes. We evaluated the endoscope FOV measurement method (the FOVWS method) in the current ISO 8600-3 standard and proposed a new method (the FOVEP method). We compared the two methods by measuring the FOV of 18 models of endoscopes (one device for each model) from seven key international manufacturers. We also estimated the device to device variation of two models of colonoscopes by measuring several hundreds of devices. Our results showed that the FOVEP method was more accurate than the FOVWS method, and could be used for all endoscopes. We also found that the labelled FOV values of many commercial endoscopes are significantly overstated. Our study can help endoscope users understand endoscope FOV and identify a proper method for FOV measurement. This paper can be used as a reference to revise the current endoscope FOV measurement standard.
OCIS codes: (120.0120) Instrumentation, measurement, and metrology; (120.4800) Optical standards and testing
1. Introduction
The angular field of view (FOVA) of an imaging device is defined as the angle in object space over which objects are viewed or recorded on a film or video sensor. The term of FOVA is often simplified as field of view (FOV) and used interchangeably with angle of view (AOV). On the other hand, FOV sometimes means the visible size in object space which can be expressed as a two-dimensional area (e.g., 11 cm × 14 cm or 18 cm diameter at a working distance of 75 cm) or one-dimensional length (e.g., 11 cm in the horizontal direction at the working distance of 75 cm) at a given distance [1]. Defining the FOV as the visible area or length is useful for an imaging device with a fixed focus lens that is intended for use at a single, specific working distance. However, an endoscope usually has an objective lens with a large FOV and a relatively long depth of field (DOF), which enables observing objects at different working distances. Focusing at different working distances is usually achieved by the observer’s eyes or by moving the coupler lens of an attached video camera. Some endoscopic cameras have zoom lenses whose focal length can be adjusted. For an imaging device with varying working distances, the visible area or length increases with increasing working distance.
Endoscopes usually have a wide FOV because of the restricted space and required range of movement during an endoscopy procedure [2]. For an endoscope with a smaller FOV, the endoscope operator needs to move and refocus the endoscope more frequently, which makes hand-eye coordination and smooth manipulation more difficult, increasing the endoscopy procedure time. As a result, endoscope manufacturers are seeking to design endoscopes with a large FOV. However, the current consensus endoscope FOV measurement method based on ISO 8600-3 [3] is not accurate, especially for endoscopes with a close focus distance and capsule endoscopes. Therefore, the labeled FOV values provided by different manufacturers might not be comparable and might be misleading to end users.
In this paper, we studied endoscope FOVA measurement methods. To be consistent with ISO endoscope standards [3,4], the term of FOV is used to represent FOVA in this paper, unless otherwise specified. While the FOV of an endoscope traditionally has a cone shape, the advancement of endoscopic imaging technologies has introduced novel endoscopes with non-traditional FOV designs. Wang et al. developed a catadioptric endoscope objective with forward and side views [5]. Han et al. developed a novel wide FOV scanning endoscope based on contact image sensor technology to scan the anal canal for 360° and obtain a cylindrical surface image of the canal [6]. Commercial endoscopes exist that can achieve 330° FOV by overlapping the FOV of several lenses located in the front and on the side of the endoscope distal tip (Fuse, EndoChoice, Inc., Alpharetta, Georgia), or even 360° FOV by incorporating a miniature omni-directional camera (Aer-O-Scope, GI-View, Israel). It is difficult to establish a general method for FOV measurement of these novel endoscopes. This paper only focuses on the FOV measurement of an endoscope with a single cone-shape FOV that is less than 180° along any directions on a plan that is orthogonal to the central axis of the FOV.
Endoscope FOV depends on the focal length of the lens and the physical size of the image sensor (film or digital). For an endoscope with the lens’s focal length of f and image sensor size of h along one direction, a shorter f or a higher h will yield a larger FOV along this direction. Besides f and h, the endoscope FOV is practically limited by the small physical dimensions of the endoscope and the F/# of the objective lens. While an endoscope usually can work at different distances and hence the visible size can change, its FOV is constant for a given focal length and size of the image sensor.
In this paper, we analyzed the FOV measurement method in the current ISO standards [3] and developed a new method. These methods were evaluated by measuring FOV of endoscopes of different types and from different manufacturers.
2. Shortcoming of current endoscope FOV standards
2.1 Endoscope FOV definition and measurement method in ISO standards
Endoscope international standards are overseen by ISO/TC 172 (Optics and Photonics)/SC 5 (Microscopes and Endoscopes)/WG 6 (Endoscopes), under the ISO 8600 standard series. In the ISO 8600-1 standard [4], FOV is defined as “view of an endoscope with optics as stated by the manufacturer or distributor, expressed as the vertex angle (in degrees) of the cone whose vertex is at the distal window surface (WS) of the endoscope ”. [4] To distinguish this method from other measurement methods, we name the FOV with the cone vertex at the distal WS of the endoscope as FOVWS. This definition is based on the FOV measurement method defined in ISO 8600-3 [3]. In this ISO standard, a planar target with concentric circles is placed 50 ± 0.2 mm away from the distal WS of the endoscope. The test setup is adjusted so that the central axis of FOVWS is perpendicular to the target and aligned with the target center (Fig. 1). The FOVWS of the endoscope can be calculated as
| (1) |
where r is the radius of the largest visible circle on the target with unit of mm. To simplify, the concentric circles are directly labelled with angle values according Eq. (1). If the working distance of the endoscope is less than 50 mm, the target should be put at the working distance. Then the number 50 in Eq. (1) should be replaced with the actual target distance with the unit of mm.
Fig. 1.
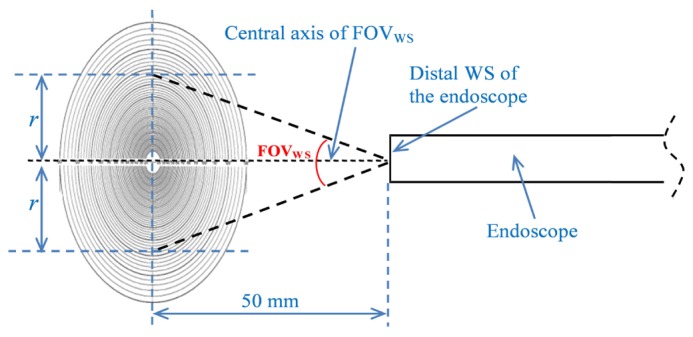
Endoscope FOVWS definition and measurement in ISO 8600-1 and −3 [3,4].
2.2 Endoscope FOVWS measurement error
Theoretically, the FOV of an endoscope is the maximum angular size of the object as seen from the entrance pupil (EP), not the distal WS. In practice, the EP (i.e., the vertex of the FOV) of an endoscope is rarely located at the distal WS, from which working distance is measured, and is only used as an approximation for the EP unless the EP location is known. The method to measure the FOVWS of an endoscope in ISO 8600-3 [3] is acceptable for a traditional tubular rigid or flexible endoscope whose EP is located at the distal WS or whose working/measuring distance (d) is much longer than the distance between the distal WS and the EP (dEP). If this is not the case, the distance from the EP to the target (d + dEP) should be used to calculate the FOV, which is named FOVEP in this paper. For example, some gastrointestinal (GI) endoscopes have a near focus mode with a DOF of 2-6 mm [7]. In such a case, the target is placed close to the distal WS and therefore the assumption that the working distance is much longer than the dEP is invalid.
The percentage error (Err) of the FOVWS measurement compared to the FOVEP measurement is calculated as follows.
| (2) |
where r is the radius of the largest visible circle, d is the distance from the target to the distal WS, and is the distance from the distal WS to the EP (Fig. 2). Equation (2) can be simplified as
| (3) |
If FOVEP is known, Err can be calculated as
Fig. 2.
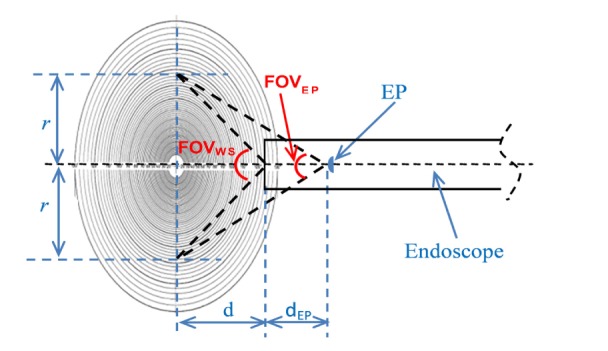
FOVWS and FOVEP measurement of an endoscope with a near focus mode.
| (4) |
According to ISO 8600-3 [3], the FOVWS measuring distance is set as 50 mm from the distal WS (d = 50mm). We can estimate the FOVWS measurement error as a function of FOVEP for different designs according to Eq. (4) (Fig. 3). From Fig. 3, the percentage FOVWS error is greater for smaller FOVEP and greater dEP. For most tubular rigid and flexible endoscopes, the EP is 0.5-3.5 mm inside the WS of the endoscope. Therefore, the FOVWS measurement can have an error in the range of 0.2% to 5.2% for FOVEP range of 170° to 70° respectively (Fig. 3(b)).
Fig. 3.

FOVWS measurement error for several different designs at 50 mm target distance: (a) 0-180° FOVEP and (b) 70-170° FOVEP.
For an endoscope with a known FOVEP and , to ensure the measured FOVWS has an error less than a preset error value of Err, the required minimum d can be calculated with Eq. (5) that is modified from Eq. (4).
| (5) |
From Eq. (5), the minimum d is proportional to to ensure the measured FOVWS error is less than Err. Based on Eq. (5), Fig. 4 can be obtained. From this figure, the manufacturer can chose a proper testing distance to control the measured FOVWS error within a certain range if the designed FOVEP and the EP position are known. For example, for an endoscope with designed FOVEP of 70° and the EP position of 3 mm behind the distal WS, the target should be placed more than 75mm from the distal WS to control the measured FOVWS error within 3% (Fig. 4(b)). Equation (5) and Fig. 4 show that a proper target-endoscope distance for FOVWS measurement is determined by dEP and the error range requirement.
Fig. 4.

Minimum d to control FOVWS measurement error within: (a) 1%, (b) 3%, (c) 5%
The main problem with the current FOVWS method in ISO 8600-3 [3] is that the current method can cause larger errors for novel endoscopic technologies such as endoscopes with a close focus distance and capsule endoscopes. Take a capsule endoscope as an example (Fig. 7(a)). If the FOVEP of the capsule endoscope is 120°, the is 5.5 mm (the radius of a typical capsule) and the measuring distance is 4.5 mm (typical working distance for a capsule), then the measured FOVWS according to current ISO 8600-3 is 150.9°, a 26% error compared with the FOVEP. If the measuring distance is 3 mm, the error is 31%. For this reason, the current ISO 8600-3 standard should not be used for such endoscopes.
3. Endoscope FOVEP measurement
A method that can overcome the FOVWS error caused by a non-zero dEP value is shown in Fig. 5. A target with two concentric circles is moved to a distance of d1 where the maximum visible circle has the radius of , then to a distance of d2 where the maximum visible circle has the radius of . The distances of d1 and d2 are from the EP to the target, which are usually unknown to most testers. However, the difference (Δd) between d1 and d2 are known during the measurement. The FOVEP is calculated as
Fig. 5.
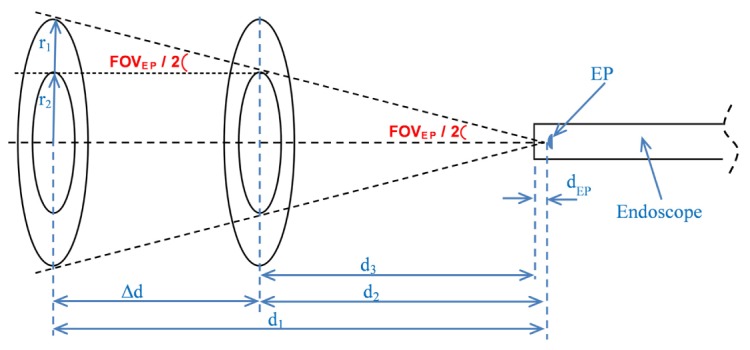
Principle of FOVEP measurement.
| (6) |
Once the FOVEP is known, the EP position (dEP) can also be calculated. In Fig. 5, if the distance from the distal WS to the target (d3) is measured, dEP can be calculated as follows.
| (7) |
In this paper, a positive dEP value means the EP is behind the distal window inside the endoscope.
4. FOV measurements of commercially available endoscopes
The majority of endoscopes can be categorized into rigid endoscopes (most laparoscopes, arthroscopes, hysteroscopes, etc.), flexible endoscopes (most gastroscopes, colonoscopes, etc.), and capsule endoscopes (often called capsules). We selected 18 representative models from these three categories (11 rigid endoscopes, six flexible endoscopes and one capsule) to measure their FOVWS and FOVEP. These endoscopes were from seven established global manufacturers. The FOVWS errors were analyzed with the FOVEP values as references. Since we couldn’t evaluate all endoscopes on the market, we thought it would be unfair to release identifying information (manufacturer, model, etc.) of these endoscopes and therefore give each endoscope an anonymous identification number in this paper.
4.1 FOV measurement of six flexible endoscopes
According to manufacturers’ labels, flexible endoscopes usually have FOV of 90° to 170° and DOF of 1.5 mm to 100 mm. Most GI endoscopes, including gastroscopes and colonoscopes, have FOV of 140° with some GI endoscopes having a FOV of 100°, 120°, or 170° [7]. Most duodenoscopes have FOV of 100°. Thin nasolaryngoscopes usually have a relatively small FOV of 90°.
We measured the FOV of six typical gastroscopes/colonoscopes sold in the United States from two major manufacturers. Targets with concentric circles were used. The setup was aligned so that the endoscope optical axis (i.e., the central axis of the FOV) was perpendicular to the test target and aligned with the target center (i.e., the center of concentric circles). This alignment requirement shall be satisfied during the whole FOV measurement process. For the FOV in the horizontal direction, the target was placed to touch the distal WS and then moved away from the endoscope until a circle was tangent to the two vertical edges, respectively (Fig. 6(a)). Then the target was farther moved away until another circle was tangent to the two vertical edges. The moving distances and the radii of the two circles were recorded to calculate FOVEP and FOVWS. In the same way, we measured the FOVEP and FOVWS in the vertical and diagonal directions.
Fig. 6.

FOV measurement images: a circle tangent to the (a) vertical, (b) horizontal, and (c) diagonal edges.
While we moved the target to change the target-endoscope distance during the FOV measurement, the distance can also be changed by moving the endoscope and the results should be the same. During the measurements, the endoscope’s own light source was used to illuminate the target. If external light sources are used, the image quality of Fig. 6 can be improved and the tangent points can be more easily distinguished.
The measured FOVEP and FOVWS values of the six flexible endoscopes are shown in Table 1. For the first five endoscopes, the measured FOVEP are always smaller than the measured FOVWS, but within 3.2%. For colonoscope #3, the trend is not obvious. That is because this endoscope has larger FOV than other endoscopes and has more severe distortion at the outer edges of the field, which made it difficult to judge the tangency of a circle to an edge and thus caused a larger error.
Table 1. Measurements of FOVWS and FOVEP for six flexible endoscopes (Ga: Gastroscope; Co: Colonoscope).
| FOVEP (°) | FOVWS (°) | FOVWS error with FOVEP as reference | ||
|---|---|---|---|---|
| Ga #1 | Horizontal | 114.6 | 115.8 | 1.0% |
| Vertical | 81.9 | 83.3 | 1.7% | |
| Diagonal | 122.1 | 123.0 | 0.7% | |
| Ga #2 | Horizontal | 121.4 | 122.5 | 0.9% |
| Vertical | 87.3 | 88.0 | 0.8% | |
| Diagonal | 137.3 | 137.5 | 0.1% | |
| Ga #3 | Horizontal | 102.5 | 104.0 | 1.4% |
| Vertical | 86.6 | 87.0 | 0.5% | |
| Diagonal | 124.6 | 126.3 | 1.3% | |
| Co #1 | Horizontal | 122.6 | 125.0 | 1.9% |
| Vertical | 87.7 | 90.5 | 3.2% | |
| Diagonal | 138.3 | 140.0 | 1.2% | |
| Co #2 | Horizontal | 122.5 | 123.5 | 0.8% |
| Vertical | 93.6 | 94.0 | 0.4% | |
| Diagonal | 133.5 | 134.0 | 0.4% | |
| Co #3 | Horizontal | 145.0 | 145.0 | 0.0% |
| Vertical | 108.0 | 106.0 | -1.9% | |
| Diagonal | 155.3 | 166.0 | 6.9% |
4.2 FOV measurements of 11 rigid endoscopes
Rigid endoscopes usually have FOV between 70° and 110°, with 70° typically seen for laparoscopes and approximately 100° for most arthroscopes. We measured the FOV of 11 rigid endoscopes sold in the United States from five major manufacturers. Similar methods as described in Section 4.1 were used. The measurements were carried out on a commercial bench test device (EndoBench, Lighthouse Imaging LLC) with preset target-endoscope distances. The target distance can be increased to reduce FOVWS errors, especially if there is a large dEP. The target had two concentric circles with diameters of 35 mm and 17.5 mm. These endoscopes were measured using a large enough image sensor so the lens’s full circular FOV could be seen. The results are shown in Table 2. In general, the FOVWS errors agree with Fig. 4 and Eqs. (4) and (5). For the three scopes with dEP greater than 2.8 mm, the measured FOVWS errors are greater than 5.6% with the FOVEP values as references.
Table 2. Measurements of FOVWS and FOVEP for 11 rigid endoscopes (L: Laparoscope; A: Arthroscope; S: Sinuscope; R: Resectoscope; C: Cystoscope; H: Hysteroscope).
| Insertion diameter (mm) | Direction of view (°) | FOVEP (°) | FOVWS | dEP from Eq. (7) (mm) | dEP from Zemax (mm) | |||
|---|---|---|---|---|---|---|---|---|
| Target distance (mm) | Values (°) | Error compared with FOVEP | ||||||
| L #1 | 10 | 30 | 72 | 40 | 76 | 5.6% | 3.0 | 3.3 |
| L #2 | 10 | 30 | 72 | 40 | 76 | 5.6% | 3.0 | 3.0 |
| L #3 | 10 | 30 | 69 | 40 | 73 | 5.8% | 3.1 | 2.8 |
| L #4 | 5 | 30 | 76 | 40 | 78 | 2.6% | 1.5 | 1.7 |
| A #1 | 4 | 70 | 106 | 20 | 108 | 1.9% | 0.7 | 0.9 |
| S #1 | 4 | 30 | 83 | 20 | 85 | 2.4% | 0.7 | 1.2 |
| R #1 | 4 | 30 | 71 | 20 | 72 | 1.4% | 0.4 | 0.7 |
| R #2 | 4 | 30 | 68 | 20 | 71 | 4.4% | 1.2 | 0.9 |
| C #1 | 4 | 70 | 86 | 20 | 88 | 2.3% | 0.7 | 0.8 |
| H #1 | 4 | 30 | 93 | 20 | 96 | 3.2% | 1.1 | 1.1 |
| H #2 | 2.9 | 30 | 84 | 20 | 86 | 2.4% | 0.7 | 0.9 |
The EP locations (dEP) of the 11 rigid endoscopes were calculated based on the FOVEP measurement data and Eq. (7). They were also estimated through simulations with Zemax (Zemax, LLC, https://www.zemax.com/) based on lens design data. From Table 2, the calculated and simulated dEP values are rather close, indicating Eq. (7) can be a convenient tool to approximate dEP. The FOV values in the table are rounded to degrees. So part of the difference between the last two columns comes from the rounding.
4.3 FOV measurements of a capsule endoscope
Most capsule endoscopes have diameters ranging from 10.8 to 13 mm (11mm is a common diameter) and lengths ranging from 24 to 27.9 mm (26 mm is a common length) [8–10]. According to manufacturers’ labels, capsule endoscopes usually have FOV ranging from 140° to 170° and DOF ranging from 0 mm to 30 mm.
As shown in Fig. 7(a), the lens of a capsule is separated from the target by a distance of roughly the capsule radius (i.e., about 5.5 mm) even if the target touches the distal WS. During the FOV measurement, the target should be within the DOF range, i.e., less than 30 mm from the vertex of the dome. Therefore, it is invalid to assume that the target distance is significant greater than the distance between the distal WS and the EP (usually close to the lens) and thus current ISO 8600-3 [3] should not be used to measure the FOV of a capsule endoscope.
Fig. 7.
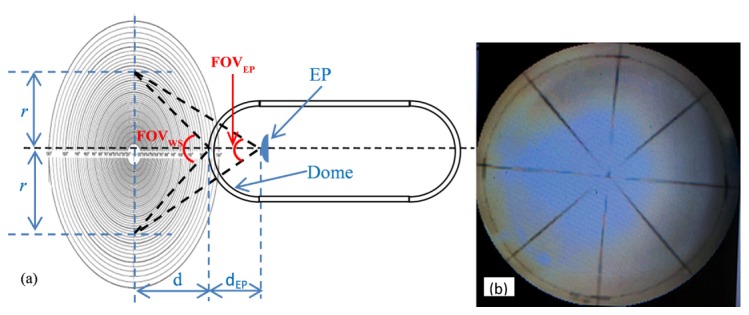
FOVWS and FOVEP measurement of a capsule endoscope: (a) illustration of FOVWS and FOVEP, (b) a low resolution image (4 cm × 4 cm) on a capsule recorder screen.
We measured the FOV of a capsule endoscope using a similar method as described in Section 4.1. The target we used had three circles with radii of 1.5 cm, 2.5 cm and 3.5 cm respectively. The distances from the dome vertex to the target ranged from 2 mm to 18 mm when the smallest and largest circles overlapped the FOV edge. The FOV of the capsule was measured several times and the FOVEP values were calculated with the combination of any two of the three circles during each measurement. In total, we obtained 10 sets of data to calculate 10 FOVEP values. The average FOVEP value was 117.7° based on Eq. (6) with the standard deviation (SD) of 4.4° (3.7% of the average FOVEP). Based on Eq. (7), we also estimated that the EP is approximately 6 mm behind the distal WS. The measured FOVWS values were 156°, 141° and 132° when the target was 3 mm, 9 mm and 16 mm away from the distal WS respectively, indicating 33%, 20% and 12% larger values than the FOVEP. A closer target-capsule distance will cause a larger FOVWS error with the FOVEP as reference.
5. Discussion
5.1 FOV in different directions
For a rigid scope, the field stop is contained within the scope itself and is generally circular. This defines the natural FOV of the endoscope (i.e., the endoscope FOV if the image sensor is infinite large) when it is used with the eye alone. For a video endoscope system, the image sensor may act as the field stop if it cuts off the natural FOV of the endoscope. The size of the image sensor determines how much of the endoscope’s natural FOV is utilized. Some endoscopes have electronic field stops that may cut off the image corners or even reduce the usable image sensor pixels to a smaller rectangle.
As a result, the image frame from an endoscope can have different shapes (Fig. 8). Figure 8(a) shows the case where the natural FOV of the endoscope is completely contained within the usable area of the sensor. Figure 8(b) shows the effect of an electronic field stop, which blocks the image at the corners of the display. Figure 8(c) illustrates the case where the natural FOV of the endoscope is larger than the image sensor. For an endoscope to form a circular frame (Fig. 8(a)), only one FOV value is needed. For an endoscope to form a rectangular frame (Fig. 8(c)), three FOV values need to be given – the horizontal, vertical, and diagonal FOV values. For an endoscope to form an irregular frame (Fig. 8(b)), multiple FOV values may be needed, but the horizontal, vertical and diagonal FOV values are still the preferred ones.
Fig. 8.

Three typical endoscope frame shapes: (a) circular FOV, (b) irregular FOV, and (c) rectangular FOV.
5.2 FOV measurement accuracy
Theoretically, the FOV of an endoscope should be an angle with the EP as the vertex (i.e., the FOVEP). If the working/measuring distance (d) is much longer than dEP, the angle with the distal WS as the vertex (FOVWS) can be used to approximate FOVEP. The difference between FOVWS and FOVEP is caused by the measuring method, denoted here as method error (Errmethod). On the other hand, FOV can be measured several times with the same method (FOVWS or FOVEP) and the variation between these repeated measurements is denoted here as measurement error (Errmeasure). Besides the method error and measurement error, there is device to device variation, denoted here as device error (Errdevice).
5.2.1 Measurement error and method error of the FOV of a flexible endoscope
Gastroscope #1 was used to evaluate the effect of measuring distances and concentric circles radii on the FOV measurement error and method error of a flexible endoscope. The method described in Section 4.1 was used. The test target has 9 concentric circles with radii of 1.5 cm to 9.5 cm in 1 cm intervals (Fig. 9). For the FOV in the horizontal direction, the target was placed close to the distal WS and then moved away from the endoscope until each circle was tangent to the two vertical edges of the image. The locations where each of the 9 circles was tangent to the vertical edges were recorded. We therefore obtained 9 location/radius data sets to study how the relative sizes and measuring distances of the two circles affects the measurement error and method error of FOV measurements. Since any 2 of the 9 data sets can be used to calculate the FOVEP according to Eq. (6), we used all the 36 possible combinations of two data sets () to calculate the FOVEP and obtained 36 FOVEP values. We also calculated the FOVWS according to the ISO 8600-3 endoscope standard [3] based on the 9 location/radius data sets and obtained 9 FOVWS values. In the same way, we measured the FOVEP and FOVWS in the vertical and diagonal directions. The statistical results are shown in Table 3.
Fig. 9.
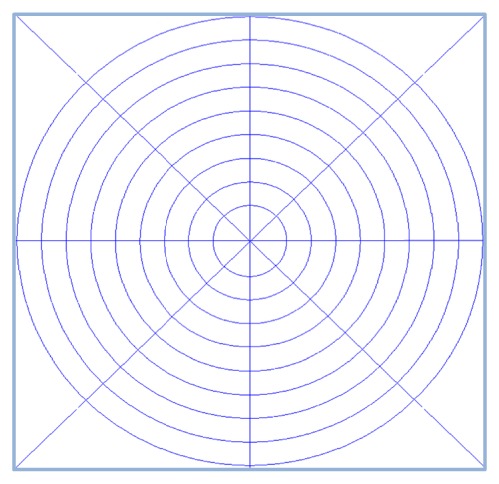
FOV measurement target.
Table 3. Statistical FOV measurement results (in unit of °) in three different directions.
| Directions | FOVEP based on 36 values | FOVWS based on 9 values | Method error of FOVWS | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Minimum | Maximum | Mean | SD | Minimum | Maximum | ||
| Horizontal | 114.6 | 0.2 | 114 | 114.8 | 115.8 | 0.7 | 115.1 | 117.5 | 1.2 |
| Vertical | 81.9 | 0.5 | 81.5 | 84.0 | 83.3 | 1.1 | 82.4 | 85.9 | 1.4 |
| Diagonal | 122.1 | 0.2 | 121.5 | 122.4 | 123.0 | 0.6 | 122.5 | 124.5 | 0.9 |
The measurement error can be expressed as the SD (absolute value) or coefficient of variation (i.e., the ratio of the SD value to the mean value, percentage value) of repeated measurements. From Table 3, the greatest measurement errors are for FOVEP and FOVWS of 0.5° and 1.1° respectively, in terms of SD. The measurement errors for FOVEP are much less than those for FOVWS in all three directions.
The relative sizes of the two circles and the target distance change () during the measurement did not affect the measurement error of FOVEP. Our measurements showed that if in Eq. (6) is greater than 1 cm, the measurement errors of FOVEP range from 0.2° to 0.5° (or 0.2% to 0.6%) and that of FOVWS range from 0.6° to 1.1° (or 0.5% to 1.3%).
The method error can be expressed as the difference between mean FOVWS and mean FOVEP values (absolute error) and the ratio of the difference to the mean FOVEP (percentage error). From Table 3, the method errors of FOVWS range from 0.9° to 1.4° (or 0.7% to 1.7%). It can be seen that smaller FOV causes greater method error, which is consistent with Fig. 3.
The FOVWS method errors are directly related to the measuring distance. We summarize FOVWS errors as a function of measuring distance in Fig. 10. From this figure, if the target-endoscope distance is 5 cm or greater, according to the current ISO 8600-3 standard [3], the FOVWS method errors in all directions can be controlled within 2%. However, the error increases exponentially with decreasing measuring distance. While a similar trend as shown in Fig. 10 can also be seen from other endoscopes, the actual value might be different, since different endoscopes might have different WS to EP distances.
Fig. 10.
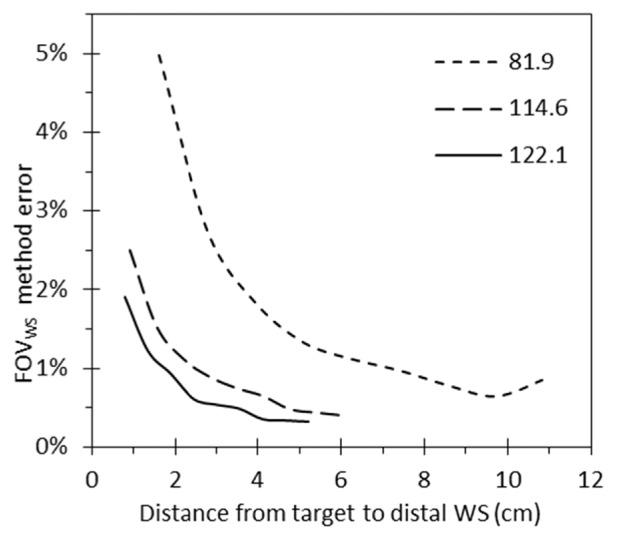
FOVWS method errors at different measuring distances for FOVEP of 81.9°, 114.6° and 122.1°.
5.2.2 Device error of two flexible endoscope models
Different device units of the same model might have slightly different FOV because of the device to device variation, denoted here as device error (Errdevice). To evaluate device error, we sampled two models of colonoscopes – 248 devices of Colono#4 and 261 devices of Colono#5 – to measure their FOVWS. The mean, SD, minimum and maximum FOVWS values for the 248 devices of Colono#4 are 138.1°, 1.2°, 135° and 141° respectively, and the values for the 261 devices of Colono#5 are 138.5°, 1.9°, 132° and 146° respectively. Therefore, the FOVWS for Colono#4 and Colono#5 can be expressed as 138.1° ± 1.2° (or 138.1° ± 0.9%) and 138.5° ± 1.9° (or 138.5° ± 1.4%) respectively. Since each device was only measured once, the SD values for these two models include both measurement error and device error.
5.2.3 Measurement error of the FOV of a capsule endoscope
From Section 4.3, the FOVWS method errors at 3 mm, 9 mm and 16 mm target distances are 33%, 20% and 12% respectively. The large errors indicated that the FOVWS method should not be used to measure the FOV of a capsule endoscope, i.e., the FOVWS should not be used to approximate FOVEP. The measured FOVEP based on the average of ten values was 117.7° with SD of 4.4° (i.e., the measurement error). The FOVEP can therefore be expressed as 117.7° ± 4.4° or 117.7° ± 3.7%.
The measurement error of the capsule FOV is greater than that of the flexible endoscope FOV we measured. The main reason is that the images from the capsule were directly shown on a small recorder screen (approximately 4 cm by 4 cm for the system we measured) with low resolution (Fig. 7(b)) and could not be directly viewed from a high resolution monitor. As a result, it is relatively difficult to align the setup and judge whether a circle overlaps with the FOV edge.
5.3 Proper FOV measuring accuracy requirements
The current ISO 8600-3 standard [3] requires the minimum FOV measuring accuracy to be ± 5% of the reading for rigid endoscopes and ± 10% of the reading for flexible endoscopes. As mentioned above, there exists measurement error (i.e., the error from repeated measurements of the same device with the same method), method error (i.e., the difference between FOVWS and FOVEP for the same device with different method), and device error (i.e., the difference from device to device with the same method). The current standard only includes one method (FOVWS), and thus apparently does not assume the presence of a method error in the assigned ± 5% or ± 10% error budget. Also since it is a measurement standard, device to device error is not discussed. Therefore, the standard can be understood as only considering measurement error.
5.3.1 A proper error range for flexible endoscopes
With measurement uncertainty theory, the total uncertainty associated with several factors is calculated by taking the square root of the sum of the squares of the uncertainty associated with each factor [11]. Therefore, the total error (Errtotal) of endoscope FOV measurement can be estimated with the following equation
| (8) |
The measurement error and method error of a gastroscope was evaluated in Section 5.2.1. The results show that the measurement errors of FOVEP range from 0.2° to 0.5° (or 0.2% to 0.6%), the measurement errors of FOVWS range from 0.6° to 1.1° (or 0.5% to 1.3%), and the method errors of FOVWS range from 0.9° to 1.4° (or 0.7% to 1.7%). The combination of measurement error and device error of two flexible endoscope models was evaluated in Section 5.2.2, with the error ranging from 1.2° to 1.9° (or 0.9% to 1.4%). Compared with the aforementioned 0.5% to 1.3% measurement errors, there should only be a small amount of device error, in the 0.9% to 1.4% range. If we assume that half of the 0.9% to 1.4% errors (i.e., 0.45% to 0.7%) are device errors, this error range should be the device error range in the worst-case scenario. We assume the aforementioned error ranges are representative for all flexible endoscopes and we use the largest measurement, method, and device errors to calculate the largest total error. The largest total error is from the FOVWS method, which can be calculated as = 2.25%.
Based on the aforementioned results, the total error in term of SD for the FOV measurement should be less than 2.25% of measured values. If we consider a 95% confidence interval, (i.e., 4.4%) can be used as the accuracy requirement, where n is sample size for SD calculation.
5.3.2 A proper error range for rigid endoscopes
We do not have complete data for all the error sources affecting a rigid endoscope’s FOV. However, the FOV measurement of a rigid endoscope should be easier than the measurement of a flexible endoscope. Therefore, we don’t anticipate the FOV error of a rigid endoscope is larger than that of a flexible endoscope.
5.3.3 A proper error range for capsule endoscopes
Compared with the FOVEP measurements for the tubular endoscopes in Sections 4.1 and 4.2, the FOVEP measurement for a capsule in Section 4.3 is more difficult. The FOV of a capsule endoscope has to be measured with the FOVEP method and thus has no method error. We assume the measurement error of a capsule endoscope is 3.7% as shown in Section 5.2.3, and the maximum device to device variation of capsule endoscopes is 0.7%, the same as that of flexible endoscopes. Then the total error is calculated as 3.8%. If we consider a 95% confidence interval, (i.e., 7.4%) can be used as the accuracy requirement, where n is sample size for SD calculation.
The error for a capsule endoscope is higher than that for a tubular endoscope because the image from a capsule endoscope cannot be directly seen from a high resolution monitor. For the manufacturer, however, it is possible to visualize high resolution images in real time and therefore obtain more accurate results. Some capsule endoscopes have no real time images viewing function, instead saving the image in the memory and then transferring the images to a computer after the endoscopy procedure. In that case, except for the manufacturer, it is hard to measure the FOV, since the alignment would be extremely difficult.
5.4 Current FOV labelling on the market
Based on the data presented above, it is clear that the measurement error of the FOVEP method is much smaller than the stated error range of ± 15% in current ISO 8600-1 [4]. In addition, the systematic offset between the FOVEP and FOVWS methods is consistent with the expected location of the entrance pupils in typical endoscopes. However, as shown below in Table 4, the measured values are consistently lower than the manufacturer’s labeled FOV, sometimes by more than 10%.
Table 4. Measured diagonal FOVEP and labelled FOV by the manufacturers (Ga: Gastroscope; Co: Colonoscope).
| Ga #1 | Ga #2 | Ga #3 | Co #1 | Co #2 | Co #3 | |
|---|---|---|---|---|---|---|
| Diagonal FOVEP (°) | 122.1 | 137.3 | 124.6 | 138.3 | 133.5 | 155.3 |
| Labeled FOV (°) | 140 | 140 | 140 | 140 | 140 | 170 |
| Overstatement (with diagonal FOVEP as reference) | 14.7% | 2.0% | 12.4% | 1.2% | 4.9% | 9.5% |
Table 4 only contains data from the flexible endoscopes in this study, because the FOV is not usually labeled on the body of rigid endoscopes (though the direction of view is). Information on FOV is typically supplied to the end user, so such a study should be possible, One possible source of this systematic error is the use of the FOVWS method, which systematically overstates the FOV for the typical case where the entrance pupil is behind the front window. The one capsule endoscope we measured has a labeled FOV of larger than 150°, which indicates that the FOV was measured with the target closer than 5 mm. In this case, the overestimate of the FOV from using the FOVWS method could be 28% or even larger.
The large range of error given in the current version of ISO8600-1 [4], ± 15%, is several times the measurement error shown in this study. Therefore, this data should be taken into account during the next periodic review of ISO 8600-1, with the error range being reduced in the new version.
6. Conclusions
In this paper, we evaluated the endoscope FOV measurement method that is based on the distal WS position (the FOVWS method) using current international standards and proposed a new method that is based on the EP positon (the FOVEP method). During the measurement, the distance from the target to the distal WS should represent the endoscope’s working distance that is within the DOF of the scope. Although not clearly mentioned in the current ISO 8600-3 standard, the FOVWS method should only be used if the endoscope’s working distance is much longer than the distance between the distal WS and EP. In general, the FOVWS method will overestimate the FOV, since the EP usually located behind the WS in the endoscope. This is especially true for an endoscope with a short working distance and a long distance between the distal WS and EP.
Our results show that the FOVEP method is more accurate than the FOVWS method and can be applied to novel endoscopic technologies such as endoscopes with a close focus distance and capsule endoscopes. Since the FOVEP method is not affected by the relative distances from distal WS to the target and from the distal WS to the EP, it can be used for any endoscopes with a cone-shape FOV.
Endoscope-target alignment is essential for accurate FOV measurement. The endoscope optical axis should be perpendicular to the test target and aligned with the target center (i.e., the center of concentric circles). The alignment requirements need to be satisfied during the whole FOV measurement process by making sure that the translation axis is parallel to optical axis. In general, the alignment of a flexible endoscope is more difficult than a rigid endoscope, meaning measurement of a flexible endoscope needs more time than a rigid one. An alignment method during endoscope distortion measurements can be used [12].
During our measurements of flexible and capsule endoscopes, the endoscopes’ own light sources were used to illuminate the targets. Also, the targets used were printed with office printers, with worse quality than commercial targets. Better measurement accuracy can be achieved through the use of an external light source, which improves illumination intensity and uniformity, and a high quality target. The endoscopes used in this study have a fixed focal length. For endoscopic cameras with a zoom lens, the FOV should be measured at different zooming settings. The smallest zoom setting helps to achieve a measurement as close as possible to the natural FOV of the endoscope.
It should be noted that a wider FOV isn’t necessarily better than a narrower FOV. For example, because of severe distortion, vignetting, or other optical characteristics, the image quality at the edge of the wide field may be too compromised to be useful. Even more than image quality, a wide angle endoscope has, by definition, a lower magnification than a narrower FOV scope. Therefore details will be smaller on the monitor. Essentially, large areas of the field are mapped to a small number of pixels. A comprehensive understanding of endoscope FOV should consider the portion of FOV over which the endoscope exhibits good performance.
In summary, the FOVEP method is an accurate method for determining endoscope FOV. It has significant benefits over the FOVWS method described in existing standards. The equations we developed can be used to analytically guide the measurement method design. While this paper focuses on endoscope FOV measurements, the FOVEP methods can be extended to other imaging devices.
Disclaimer
The mention of commercial products, their sources, or their use in connection with material reported herein is not to be construed as either an actual or implied endorsement of such products by the Department of Health and Human Services. All authors are members of the endoscope ISO standard committee of ISO / TC 172 (Optics and Photonics) / SC 5 (Microscopes and Endoscopes) / WG 6 (Endoscopes). Publication of this study does not imply endorsement of its contents by ISO. Except for Dennis Leiner, the authors have no commercial relation relevant to the topic of the study. Dennis Leiner is a minority owner in Lighthouse Imaging LLC that manufactures a device, EndoBench, for testing the optical characteristics of endoscopes, including field of view.
To avoid any potential conflict of interest, this paper doesn’t release any information related to the manufacturers or model numbers of the tested devices, as these data are used to illustrate the range of parameters typically used in current endoscope designs. The main purpose of this paper is to establish a method for field of view measurement that any manufacturer can use, and which is applicable across the range of optical designs now in use.
References and links
- 1.Van Gompel J. J., Tabor M. H., Youssef A. S., Lau T., Carlson A. P., van Loveren H. R., Agazzi S., “Field of view comparison between two-dimensional and three-dimensional endoscopy,” Laryngoscope 124(2), 387–390 (2014). 10.1002/lary.24222 [DOI] [PubMed] [Google Scholar]
- 2.Kobayashi E., Masamune K., Sakuma I., Dohi T., “A wide-angle view endoscope system using wedge prisms,” in Third Int. Conf. on Medical Image Computing and Computer-Assisted Intervention(Springer, 2000), pp. 661–668. 10.1007/978-3-540-40899-4_68 [DOI] [Google Scholar]
- 3.ISO, “ISO 8600-3: Optics and optical instruments - Medical endoscopes and endoscopic accessories - Part 3: Determination of field of view and direction of view of endoscopes with optics,” (the International Organization for Standardization, 1997, 2003).
- 4.ISO, “ISO 8600-1: Endoscopes — Medical endoscopes and endotherapy devices — Part 1: General requirements ” (the International Organization for Standardization, 2013).
- 5.Wang R. C. C., Deen M. J., Armstrong D., Fang Q., “Development of a catadioptric endoscope objective with forward and side views,” J. Biomed. Opt. 16(6), 066015 (2011). 10.1117/1.3593148 [DOI] [PubMed] [Google Scholar]
- 6.Han C., Huangfu J., Lai L. L., Yang C., “A wide field-of-view scanning endoscope for whole anal canal imaging,” Biomed. Opt. Express 6(2), 607–614 (2015). 10.1364/BOE.6.000607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bhat Y. M., Abu D. B., Chauhan S. S., Gottlieb K. T., Hwang J. H., Komanduri S., Konda V., Lo S. K., Manfredi M. A., Maple J. T., ASGE Technology Committee , “High-definition and high-magnification endoscopes,” Gastrointest. Endosc. 80(6), 919–927 (2014). 10.1016/j.gie.2014.06.019 [DOI] [PubMed] [Google Scholar]
- 8.P. Gomes, Medical Robotics: Minimally Invasive Surgery (Elsevier, 2012). [Google Scholar]
- 9.Goenka M. K., Majumder S., Goenka U., “Capsule endoscopy: Present status and future expectation,” World J. Gastroenterol. 20(29), 10024–10037 (2014). 10.3748/wjg.v20.i29.10024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cave D. R., Fleischer D. E., Leighton J. A., Faigel D. O., Heigh R. I., Sharma V. K., Gostout C. J., Rajan E., Mergener K., Foley A., Lee M., Bhattacharya K., “A multicenter randomized comparison of the Endocapsule and the Pillcam SB,” Gastrointest. Endosc. 68(3), 487–494 (2008). 10.1016/j.gie.2007.12.037 [DOI] [PubMed] [Google Scholar]
- 11.JCGM, Guide to the Expression of Uncertainty in Measurement (International Organization for Standardization, 2008). [Google Scholar]
- 12.Wang Q., Cheng W.-C., Suresh N., Hua H., “Development of the local magnification method for quantitative evaluation of endoscope geometric distortion,” J. Biomed. Opt. 21(5), 056003 (2016). 10.1117/1.JBO.21.5.056003 [DOI] [PubMed] [Google Scholar]