

Abstract
Background: Little is known about extensor tendon failure following drill injury at the time of volar plate fixation. Our goals were to analyze extensor tendon injury following simulated drill penetration, and change in tendon displacement during cyclic loading following simulated drill penetration injury. Methods: Extensor pollicis longus (EPL) and extensor carpi radialis brevis (ECRB) tendons were harvested from 9 fresh frozen cadaveric arms. Eighteen EPL and 18 ECRB samples were created from harvested tendons. Drill penetration injury was performed in either a continuous or an oscillating mode. Injured tendons were subjected to 1200 cycles at 1- to 15-kg cyclic load at a frequency of 1 Hz, and analyzed for failure at drill sites and change in displacement throughout the testing cycle. Results: Ten EPL samples and 16 ECRB samples completed testing without failure. Tendon type (ECRB, EPL), mode of injury (continuous, oscillating), and location (proximal, distal) did not affect tendon displacement during loading. A single EPL tendon failed following continuous drill penetration injury. Extensor carpi radialis brevis samples had a mean change in displacement of 2.8 (standard deviation [SD]: 1.5 mm) and 5.9 mm (SD: 4.7 mm) for oscillating and continuous modes, respectively. Six EPL samples had a mean change in displacement of 4.7 (SD: 2.7 mm) and 4.3 mm (SD: 1.8 mm) for oscillating and continuous modes, respectively. Conclusions: Complete extensor tendon failure due to drill penetration was rare. Drill mode did not affect the degree of elongation. Increasing cyclic loading of extensor tendons after drill injury caused modest extensor tendon elongation.
Keywords: biomechanics, iatrogenic injury, extensor tendon failure, distal radius, fracture
Background
Fractures of the distal radius are very common and are increasingly being treated surgically with volar plate fixation.5,6 Volar plating has resulted in good to excellent outcomes in multiple studies.7,14,17 In spite of good clinical outcomes, extensor tendon injury and failure due to rupture remains a known complication of volar plate fixation.1,3,9,23 The incidence of tendon rupture after volar plate fixation is between 0.8% and 12%, with the extensor pollicis longus (EPL) tendon being the most frequently affected.8,9,22 One proposed cause of iatrogenic injury is drill bit penetration.1,2,8,9,16,20,22 However, little is known about extensor tendon failure. Although prior studies have analyzed injury, rupture, and repair of flexor tendons in the setting of laceration,10,13,15,18 extensor tendon injury and rupture after iatrogenic drill penetration sustained during surgical fixation of distal radius fractures remains unknown. The primary goal of this study was to analyze the differences in tendon injury caused by either a continuous or an oscillating drill mode. A secondary goal was to analyze change in extensor tendon displacement during cyclic loading following simulated drill penetration injury.
Materials and Methods
Arms from 3 males and 2 females, mean age of 82.8 years (range: 57-96 years), were collected. Ten fresh frozen cadaveric arms were harvested from the midhumerus distally. Nine of the cadaveric arms were utilized for the testing protocol, and a single arm was used prior to testing to verify parameters of the testing protocol. The arms were dissected over the dorsal compartment of the forearm, and the EPL and extensor carpi radialis brevis (ECRB) tendons were removed. Tendons were harvested at their most proximal musculotendinous junction and distally at their insertion, with EPL tendons released distally at the distal phalanx of the thumb and ECRB tendons released at the attachment to the base of the long finger metacarpal. Following harvesting, tendons were measured using a standardized medical ruler and then sectioned into 2 samples of equal 6-cm lengths. A 1-cm distance from the insertion and musculotendinous junction was removed prior to sectioning of the samples to provide the most robust tendon sample. A 6-cm distance was measured from the distal end, and the tendon was marked. A second 6-cm distance was measured from the most proximal end and marked. Each of the measured marks was sharply incised with a 10-blade scalpel to create a clean tendon sample. Samples were labeled anatomically as proximal or distal. A total of 18 EPL and 18 ECRB samples were harvested for testing. Tendon samples were then marked in 2-cm increments using a surgical marker and photographed. Each sample was then lightly soaked with sterile normal saline solution prior to testing.
Protocol Verification
Prior to testing, a single cadaveric arm was used to evaluate the testing protocol and to ensure that testing of tendon samples under an increasing cyclic load would not exceed the load to failure of injured tendon samples. One EPL and 1 ECRB practice tendon were harvested and sectioned as described above, creating 2 samples of each tendon. Tendon samples were then secured into a custom clamp mounted on a servohydraulic uniaxial mechanical testing system (Bionix; MTS Systems, Eden Prairie, Minnesota). A 2-cm long central piece of tendons remained free between the clamps (Figure 1). To our knowledge, no studies have been conducted to determine the passive tensile force to which extensor tendons are subjected during physiologic motion. A previous investigation on tensile loading of flexor tendons determined that a flexor tendon is subjected to an average of 0.9-kg tensile force during active digital motion against no resistance.21 As such, 1 kg was selected as the simulated physiological preload applied to each tendon sample. A Stryker System 3 drill (Stryker, Inc, Kalamazoo, Michigan) with a 2.8-mm drill bit (Acumed, Hillsboro, Oregon) was used, by hand, to penetrate the central portion of the clamped tendon sample. Drill penetration injuries of all samples were performed by the first author. Due to the variability of tendon sample size and shape, we made 2 punctures, side by side, to ensure sufficient tendinous injury. One EPL and 1 ECRB sample were punctured with the drill in an oscillating mode; 1 EPL and 1 ECRB sample were punctured with the drill in a continuous mode. The 4 tendon samples were distracted at a rate of 0.2 mm/s to a load of greater than 30 kg without failure at the injury site. These pretest findings ensured our cyclic loading parameters would not exceed the load to failure strength of our samples.
Figure 1.
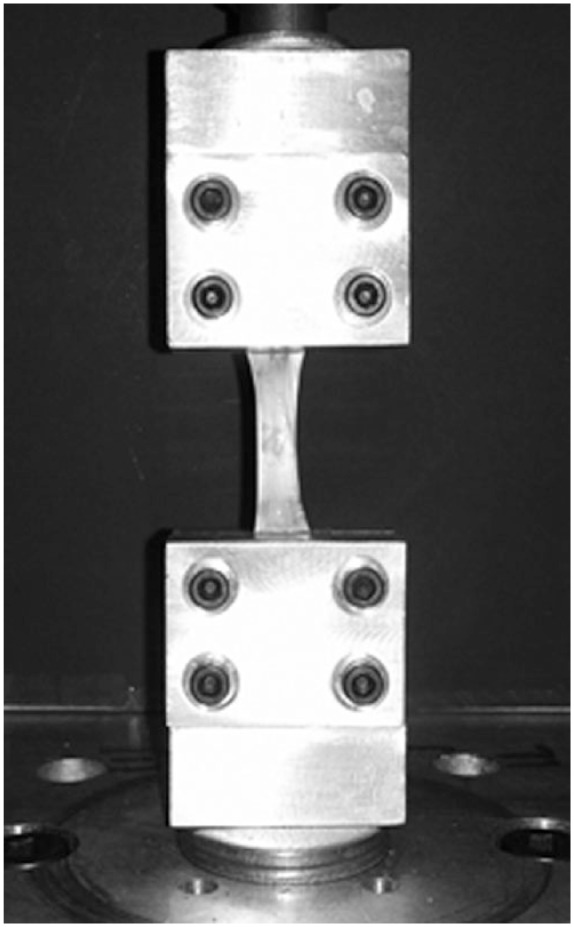
Tendon sample secured in custom clamp and attached to the test machine.
Study Sample Cyclic Testing
The remaining 36 tendon study samples were then secured into the clamp mounted on the mechanical testing system as described above. As in protocol verification, we applied the 1-kg simulated physiological load to each sample prior to drill penetration injury. Simulated drill injury was performed in either a predetermined continuous or oscillating mode. Ten distal tendon samples (5 EPL and 5 ECRB) were subjected to a continuous drill injury, and 8 distal samples (4 EPL and 4 ECRB) were subjected to an oscillating drill injury (Figure 2). Ten total proximal samples (5 EPL and 5 ECRB) were subjected to an oscillating drill injury, and 8 proximal samples (4 EPL and 4 ECRB) were subjected to a continuous injury. Following injury, samples were cyclically loaded through 1200 cycles at a frequency of 1 Hz while a cyclic load of 1 kg to 15 kg was applied. Displacement, in millimeters, of each sample was continuously recorded throughout the testing cycle. Loads applied to tendon samples were recorded with a 10-kN load cell (MTS Systems), at a sampling frequency of 1 ms. Tendons were then analyzed for complete failure and change in displacement, in millimeters. Complete failure was defined as either complete tendon rupture or tear propagation from the point of drill injury, resulting in tendon failure along the longitudinal axis of the tendon. Change in tendon displacement, measured in millimeters, was selected to represent tendon elongation throughout cyclic loading. Change in displacement was defined as displacement at maximal load at the end of testing cycle compared with initial displacement at the time that the 1-kg physiologic load was initially applied to the sample. Physiologic load (1 kg) was considered to be the zero point for all samples.
Figure 2.

Distribution of samples tested and drill setting (oscillating/continuous). Tendon samples were EPL and ECRB.
Note. EPL = extensor pollicis longus; ECRB = extensor carpi radialis brevis.
Statistical Analysis
Distributions of the physiologic variables were not normally distributed and are represented with means and standard deviations (SDs). Distributions of displacement change were compared according to drilling mode and tendon type with generalized linear regression. When displacement was compared between just 2 groups (eg, drill mode), this model is analogous to a Student’s t test for 2 independent samples. P values of <.05 were considered significant. SAS version 9.2 (SAS Institute, Inc, Cary, North Carolina) was used for statistical analysis.
Results
Ten of the 18 EPL samples (56%) and 16 of the 18 ECRB samples (89%) completed testing without failure (Figure 2). Two EPL samples injured in oscillating mode and 2 injured in continuous mode completed the 1200 cycles of testing but data failed to record; thus the samples were excluded from our analysis. Seven EPL tendon samples were excluded from analysis due to inability to complete cyclic testing; in 5 samples, the tendon sheared completely through all fibers at the clamp site, and in 2 samples, the tendons slipped at the clamp site resulting in delamination with thinning of the tendon sample preventing further testing. One EPL sample sustained failure due to tear propagation from drill penetration sites, which was considered to be a true failure. This sample was injured during continuous drill penetration and sustained failure at 213 cycles with a load of 8 kg. Two ECRB tendon samples did not complete testing due to slippage from the clamp resulting in delamination (Figure 3). Data from 6 EPL samples (3 oscillating and 3 continuous drill) and 16 ECRB samples (8 oscillating and 8 continuous drill) were available for analysis.
Figure 3.

Number of samples tested and samples with complete and incomplete testing. Tendon samples were EPL and ECRB.
Note. EPL = extensor pollicis longus; ECRB = extensor carpi radialis brevis.
The mean change in displacement of all tendon samples regardless of injury type was 4.4 mm (SD: 3.3 mm). The mean change in displacement of EPL samples regardless of injury type was 4.5 mm (SD: 2.0 mm). The mean change in displacement in the ECRB group regardless of injury type was 4.4 mm (SD: 3.7 mm). We then evaluated whether drill mode (injury type) affected displacement change according to the specific tendons. Drill method did not significantly affect displacement in the EPL samples; tendons injured in oscillating mode had a mean change in displacement of 4.7 mm (SD: 2.7 mm) compared with 4.3 mm (SD: 1.8 mm) in tendons injured in continuous mode (Figure 4). Extensor carpi radialis brevis samples injured in oscillating mode had a mean change in displacement of 2.8 mm (SD: 1.5 mm) compared with 5.9 mm (SD: 4.7 mm) in these tendons injured in continuous mode (Figure 4), although this difference was also not significant (P = .19). Sample location also did not significantly affect tendon displacement. Proximal EPL samples displaced by a mean of 4.6 mm (SD: ±2.6), and distal samples displaced by a mean of 4.2 mm (SD: ±0.3 mm). Proximal ECRB samples displaced by a mean of 3.7 mm (SD: ±1.5 mm), and distal samples displaced by a mean of 5.0 mm (SD: ±5.2 mm) (P = .49). Multiple regression analysis of data from both tendons, summarized over location (proximal, distal) and drill modes of injury (oscillating, continuous), revealed no significant group differences (P = .30; Table 1).
Figure 4.
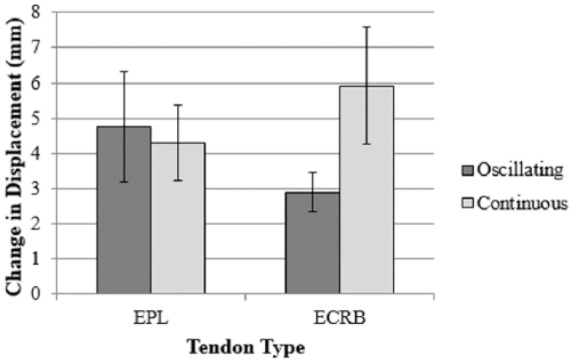
Change in displacement (mean ± standard error of the mean) based on mode of injury for EPL and ECRB tendon groups.
Note. Results from oscillating versus continuous drill modes for ECRB did not differ significantly (P = .19). Sample size was insufficient in the EPL group for statistical analysis. EPL = extensor pollicis longus; ECRB = extensor carpi radialis brevis.
Table 1.
Multiple Regression Analysis Testing Independent Effects of All Tendon Samples Based on Location and Mode of Drill Injury. (P < 0.05 considered significant).
| Displacement (mm, mean ± standard deviation) | ||||
|---|---|---|---|---|
| Location | Drill mode | n | Displacement | P value |
| Distal | Continuous | 5 | 7.3 ± 5.5 | .30 |
| Oscillating | 5 | 2.5 ± 1.4 | ||
|
| ||||
| Proximal | Continuous | 6 | 4.0 ± 1.8 | |
| Oscillating | 6 | 4.1 ± 2.2 | ||
All samples with recorded data (EPL, Figure 5A; ECRB, Figure 5B) demonstrated continued displacement throughout cyclic loading with a progressive increase in displacement. The single EPL tendon that failed due to tear propagation from the drill penetration sites showed marked displacement prior to failure at cycle 213 (Figure 5A).
Figure 5.

(a) Extensor pollicis longus displacement versus time and (b) extensor carpi radialis brevis displacement versus time.
Discussion
Complete extensor tendon failure due to drill penetration injury was rare, occurring in only a single EPL tendon sample. The single EPL tendon sample that failed was the distal tendon segment from a 96-year-old female, and thus, both age and gender of the sample may have been contributing factors to failure.12 However, given the advancing age of the patient population undergoing distal radius fracture repair, this particular tendon failure could be representative of an actual in vivo situation. The rarity of complete failure due to simulated injury is a finding consistent with a prior study analyzing flexor tendon failure.10 Hariharan et al10 demonstrated that flexor tendons with partial laceration of 50% and 75% of the tendon width failed only at forces that well exceeded the normal physiologic load. Prior studies differ in that flexor tendons were stressed monotonically to failure, rather than using a cyclic load, and nearly all tendon samples remained intact through loads that were within normal physiologic levels.10,19 Though extensor and flexor tendons have different characteristics both biomechanically and anatomically,11 our findings suggest that a larger initial injury or perhaps a sustained insult to the extensor tendon, such as would occur with prominent hardware, is needed to cause complete failure.1
All tendon samples underwent progressive tendon elongation change with cyclic loading. Extensor carpi radialis brevis tendon injury following continuous drill penetration resulted in greater displacement with increasing cycles; however, this difference did not reach statistical significance. In comparison with prior studies, Sanders et al18 analyzed lacerated flexor tendons under cyclic loading, demonstrating a linear pattern of tendon displacement up to approximately 2 mm occurring at 56 cycles of testing, with a sharp increase in displacement at 60 cycles and near immediate failure at 63 cycles. However, in that study, displacement was analyzed in the setting of flexor tendon repair, not primary injury.18 We selected change in tendon displacement to serve as a surrogate measurement for tendon elongation. It can be speculated that tendon elongation could place tendons at risk for eventual failure, but this was not determined by our study and the effects of extensor tendon displacement are not known at this time. While drilling with impunity during volar plate fixation of distal radius fracture should be avoided, one can infer from our study that drill penetration injury with subsequent cyclic loading of the tendon carries a low risk of rupture due to drill injury regardless of the mode of drilling.
There are some limitations to this study. Our design was based on prior analysis of flexor tendon injuries,15,18 although flexor and extensor tendons exhibit different characteristics11 that may not be equivalent biomechanically. In addition, the limited number of tendon samples available for analysis in the EPL groups limited our ability to assess whether continuous or oscillating drill modes resulted in increased tendon displacement. As EPL remains the most commonly injured tendon as a result of iatrogenic causes and is a known injury site with distal radius fractures,4 a more robust number of samples is needed to assess the impact of oscillating versus continuous drill injury to the EPL tendon. Another limitation is that our simulated study in cadaveric material does not take into account the inflammatory process that occurs following an injury. Our study also did not include a control, noninjured group. Therefore, we could not make comparisons in tendon elongation between injured and intact samples. However, our primary goal was to determine whether drill mode affected tendon elongation and failure, and this did not require a control group. Finally, while we drilled within the central portion of the tendon under a simulated resting physiologic load, we understand that at the time of surgical fixation, this resting tension may be different and therefore may both affect the condition of the tendon at the time of injury and alter the location of injury.
The strengths of this investigation lie in the fact that we investigated 2 tendon regions (proximal and distal) that are conceivably iatrogenically injured during volar plate fixation in 2 different extensor tendons (EPL and ECRB). In addition, we created injuries using both continuous and oscillating drill modes to include all possible injury modes. Cyclic loading over time resulted in increasing extensor tendon elongation, though its significance is not yet known and merits further investigation with a noninjured control group. We found that proximal and distal regions of EPL and ECRB tendons were robust to drill penetration, and thus conclude that complete extensor tendon failure due to drill penetration injury is rare.
Acknowledgments
We would like to acknowledge Marie Kane for her assistance with the preparation of this article.
Footnotes
Ethical Approval: This study was approved by our institutional review board.
Statement of Human and Animal Rights: All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent: Due to the cadaver-based nature of this study, written consent was not obtained from the local institutional review board.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Al-Rashid M, Theivendran K, Craigen MA. Delayed ruptures of the extensor tendon secondary to the use of volar locking compression plates for distal radial fracture. J Bone Joint Surg Br. 2006;88(12):1610-1612. [DOI] [PubMed] [Google Scholar]
- 2. Arora R, Lutz M, Hennerbichler A, Krappinger D, Espen D, Gabl M. Complications following internal fixation of unstable distal radius fracture with a palmar locking-plate. J Orthop Trauma. 2007;21(5):316-322. [DOI] [PubMed] [Google Scholar]
- 3. Benson EC, DeCarvalho A, Mikola EA, Veitch JM, Moneim MS. Two potential causes of EPL rupture after distal radius volar plate fixation. Clin Orthop Relat Res. 2006;451:218-222. [DOI] [PubMed] [Google Scholar]
- 4. Berglund L, Messer TM. Complications of volar plate fixation for managing distal radius fractures. J Am Acad Orthop Surg. 2009;17(6):369-377. [DOI] [PubMed] [Google Scholar]
- 5. Chung KC, Shauver MJ, Birkmeyer JD. Trends in the United States in the treatment of distal radial fractures in the elderly. J Bone Joint Surg Am. 2009;91(8):1868-1873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg Am. 2001;26(5):908-915. [DOI] [PubMed] [Google Scholar]
- 7. Chung KC, Watt AJ, Kotsis SV, Margaliot Z, Haase SC, Kim HM. Treatment of unstable distal radial fractures with the volar locking plating system. J Bone Joint Surg Am. 2006;88(12):2687-2694. [DOI] [PubMed] [Google Scholar]
- 8. Drobetz H, Kutscha-Lissberg E. Osteosynthesis of distal radial fractures with a volar locking screw plate system. Int Orthop. 2003;27(1):1-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Failla JM, Koniuch MP, Moed BR. Extensor pollicis longus rupture at the tip of a prominent fixation screw: report of three cases. J Hand Surg Am. 1993;18(4):648-651. [DOI] [PubMed] [Google Scholar]
- 10. Hariharan JS, Diao E, Soejima O, Lotz JC. Partial lacerations of human digital flexor tendons: a biomechanical analysis. J Hand Surg Am. 1997;22(6):1011-1015. [DOI] [PubMed] [Google Scholar]
- 11. Loren GJ, Lieber RL. Tendon biomechanical properties enhance human wrist muscle specialization. J Biomech. 1995;28(7):791-799. [DOI] [PubMed] [Google Scholar]
- 12. Magnusson SP, Hansen M, Langberg H, et al. The adaptability of tendon to loading differs in men and women. Int J Exp Pathol. 2007;88(4):237-240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Manning DW, Spiguel AR, Mass DP. Biomechanical analysis of partial flexor tendon lacerations in zone II of human cadavers. J Hand Surg Am. 2010;35(1):11-18. [DOI] [PubMed] [Google Scholar]
- 14. Orbay JL, Fernandez DL. Volar fixation for dorsally displaced fractures of the distal radius: a preliminary report. J Hand Surg Am. 2002;27(2):205-215. [DOI] [PubMed] [Google Scholar]
- 15. Pruitt DL, Manske PR, Fink B. Cyclic stress analysis of flexor tendon repair. J Hand Surg Am. 1991;16(4):701-707. [DOI] [PubMed] [Google Scholar]
- 16. Rampoldi M, Marsico S. Complications of volar plating of distal radius fractures. Acta Orthop Belg. 2007;73(6):714-719. [PubMed] [Google Scholar]
- 17. Rozental TD, Blazar PE. Functional outcome and complications after volar plating for dorsally displaced, unstable fractures of the distal radius. J Hand Surg Am. 2006;31(3):359-365. [DOI] [PubMed] [Google Scholar]
- 18. Sanders DW, Minle AD, Dobravec A, MacDermid J, Johnson JA, King GJ. Cyclic testing of flexor tendon repairs: an in vitro biomechanical study. J Hand Surg Am. 1997;22(6):1004-1010. [DOI] [PubMed] [Google Scholar]
- 19. Schuind F, Garcia-Elias M, Cooney WP, III, An KN. Flexor tendon forces: in vivo measurements. J Hand Surg Am. 1992;17(2):291-298. [DOI] [PubMed] [Google Scholar]
- 20. Skoff HD. Postfracture extensor pollicis longus tenosynovitis and tendon rupture: a scientific study and personal series. Am J Orthop. 2003;32(5):245-247. [PubMed] [Google Scholar]
- 21. Urbaniak JR, Cahill JD, Mortenson RA. Tendon suturing methods: analysis of tensile strength. In: Hunter JM, Schneider LH. eds. AAOS Symposium on Tendon Surgery in the Hand St. Louis, MO: C.V. Mosby; 1975:70-80. [Google Scholar]
- 22. White BD, Nydick JA, Karsky D, Williams BD, Hess AV, Stone JD. Incidence and clinical outcomes of tendon rupture following distal radius fracture. J Hand Surg Am. 2012;37(10):2035-2040. [DOI] [PubMed] [Google Scholar]
- 23. Wong-Chung J, Quinlan W. Rupture of extensor pollicis longus following fixation of a distal radius fracture. Injury. 1989;20(6):375-376. [DOI] [PubMed] [Google Scholar]