

Abstract
Background:
For patients undergoing spine surgery, the literature attributes significant increased perioperative risks/adverse events (AE) complications, longer length of stay (LOS), and higher 30-day readmission/reoperation rates to those with diabetes. Diabetics are often divided into those with insulin dependent diabetes (IDDM), and non-insulin dependent diabetes (NIDD). However, other series also compare those with uncontrolled diabetes (UCDM) vs. those with controlled DM (CDM).
Methods:
We found a marked variation in the size and quality of studies identified in PubMed regarding the impact of diabetes on spinal surgery (e.g., focusing on complications, AE, outcomes, morbidity, and mortality).
Results:
Of the 197,461 lumbar fusions in one NIS (Nationwide Inpatient Sample 1988–2003), 11,000 (5.6%) diabetics (DM) had higher infection rates, transfusion rates, more pneumonias, higher in-hospital mortality rates, greater costs, and longer LOS than those undergoing similar procedures without DM. For 3726 ACS-NSQIP patients undergoing anterior cervical fusions, 270 NIDDM had more urinary tract infections and returns to the operating room; the 171 IDDM required more reoperations, 30 day readmission, and longer LOS (by 5 days) vs. 3285 non DM. Of the 5627 patients undergoing posterior cervical fusions (ACS-NSQIP), 2029 (36.1%) had AE directly related to DM. In another NSQUIP study of 51277 patients undergoing lumbar spine surgery, IDDM and NIDDM demonstrated longer LOS, plus IDDM showed more surgical AE and 30 day readmissions vs. those with no DM.
Conclusions:
Patients with IDDM or NIDDM undergoing spine surgery exhibited more perioperative complications/AE/morbidity, longer LOS, and higher readmission/reoperation rates vs. non DM.
Keywords: Diabetes: spinal surgery, insulin dependent DM (IDDM), more adverse events, more complications, poorer outcomes: non-insulin dependent DM (NIDDM)
INTRODUCTION
For patients undergoing spinal surgery, the literature attributes significantly increased morbidity, adverse events (AE), complications and even mortality to diabetes [Tables 1–3]. Many studies clearly distinguished between insulin dependent diabetics (IDDM), non-insulin dependent diabetes (NIDD) vs. non-DM. Others defined newly diagnosed DM, uncontrolled DM (UCDM) vs. controlled DM (CDM). Notably, for those with more severe DM (IDDM), greater morbidity, AE, 30-day readmission/reoperation rates, and poor overall outcomes were observed.
Table 1.
Increased risks of spine surgery in diabetic patients references 2007-2013

Table 3.
Increased risks of spine surgery in diabetic patients: (references 2016–2017)

In this study, we queried PubMed utilizing the following search engines; diabetes, spinal surgery, complications/adverse events (AE), outcomes, morbidity, and mortality. The 27 studies identified varied markedly in quality and design, ranging from small series to large national database analyses. In the Browne et al. (2007) report, that included an evaluation of 197,461 NIS (Nationwide Inpatient Sample 1988–2003) patients undergoing lumbar spine fusions, there were 11000 (5.6%) diabetics (based on HbA1c testing); the diabetic patients exhibited higher rates of infection, pneumonia, in-hospital mortality, hospital costs, required more transfusions, and had longer lengths of stay (LOS) vs. non-DM patients [Table 1].[2] In Phan et al. (2016) using the ACS-NSQUIP database comprising 3726 patients undergoing anterior cervical discectomy/fusion, the 270 patients who were diagnosed as NIDDM had more urinary tract infections and returns to the operating room vs. those without a diagnosis of DM. Furthermore the 171 IDDM required more reoperations, 30-day readmissions, and had longer LOS (by 5 days) compared with non-DM [Table 3].[19] In another ACS-NSQIP study of 5627 patients undergoing posterior cervical fusions, Medvedev et al. the authors found that 2029 (36.1%) had AE largely attributed to DM (e.g., more wound complications) and smoking, correlating with higher preoperative American Association of Anesthesia (ASA) scores [Table 3].[14] In a further NSQIP study involving 51277 patients, Qin et al. (2016) looked at outcomes for patients with NIDDM, IDDM, or non DM; greater LOS was seen in both diabetic populations, whereas IDDM had higher surgery-related AE and 30 day readmissions rates vs. those without in the study [Table 3].[20] These and multiple other studies largely confirmed DM patients [e.g., IDDM, NIDDM, controlled DM (CDM), and uncontrolled DM (UCDM)] exhibited more perioperative morbidity/AE/complications, longer LOS, higher 30-day readmission/reoperation rates, and in some cases mortality compared with non-DM patients.
DIABETES: A MAJOR COMORBIDITY FOR PATIENTS UNDERGOING SPINAL SURGERY
For patients undergoing spinal surgery, Epstein (2012) noted that diabetes (DM) was associated with a higher risk of infection, osteoporosis, and pseudarthrosis, as well as other major medical risk factors.[6] The mortality rates for patients undergoing spine surgery (with or without DM) within six months of having an acute myocardial infarction was 40%. For DM or non DM patients who had a coated stent placed within the last year (e.g. for cardiac, carotid or peripheral vascular disease), anti-platelet therapy could not be stopped; early cessation of this medication could result in acute graft occlusion/death. Diabetes was also highly correlated with other major comorbidities including; obesity/morbid obesity, chronic obstructive pulmonary disease (COPD), perioperative deep venous thrombosis (DVT), and pulmonary embolism (PE).
VARIABLE IMPACT OF DIABETES ON CERVICAL SPINE SURGERY
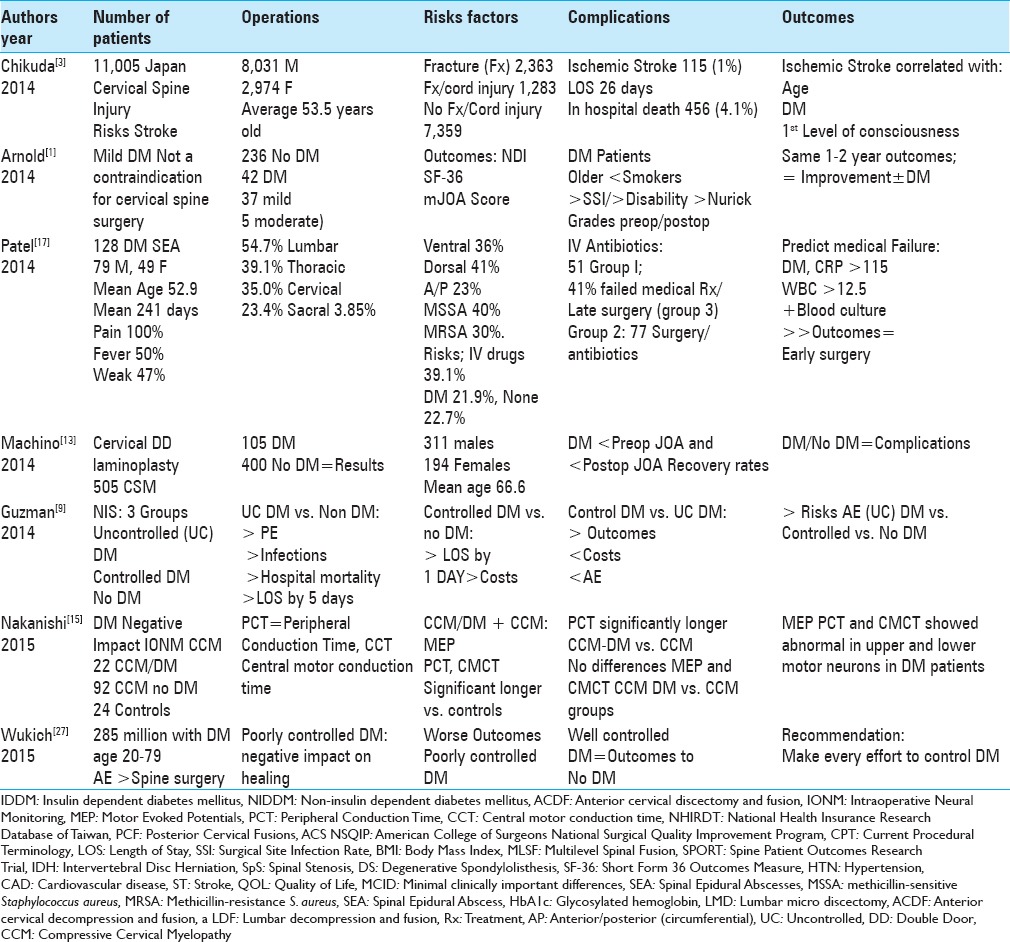
Although one study documented the absence of a negative impact of DM on AE events associated with decompressive cervical spine surgery, three studies did show increased DM-related perioperative morbidity. In the first study, Arnold et al. (2014), evaluated 42 DM (37 mild/5 moderate) vs. 236 non DM: they found that DM had no negative impact on the results of decompressive cervical surgery for cervical spondylotic myelopathy (CSM) [Table 2].[1] Patients in both groups showed similar Neck Disability Index (NDI), Short Form-36 Health Surveys [(2 Health Scales; SF-36v2), modified JOA Scores (mJOA), Nurick Grades], and 1–2 year surgical complications and improvement rates. Three other studies, however, demonstrated the negative impact of DM on cervical spine surgery, likely attributed to their larger sampling sizes [Tables 2 and 3].[3,9,12] Utilizing the Nationwide Inpatient Sample (2002–2011), Guzman (2014) et al. found an increased risk/complication/AE rate for uncontrolled DM (UCDM)/controlled DM (CDM) vs. non-DM undergoing comparable cervical spine operations [Table 2].[9] UCDM patients showed statistically significantly increased respiratory, cardiac, and genitourinary complications, more frequent PE, postoperative infections, in-patient mortality, and increased mean LOS (by almost 5 days) vs. non-DM patients. CDM patients also had increased perioperative AE rates, and increased costs, but less than that for UCDM patients; of interest, however, their mean LOS was only increased by one day vs. non DM patients. Chikuda et al. (2014) evaluated 11005 patients following cervical spine injuries and documented a 1% (115 patients/over 26 day LOS) incidence of ischemic stroke. These patients demonstrated an increased frequency of DM along with more advanced age [Table 2].[3] When Liu et al. (2017) evaluated 38680 patients from 6 studies undergoing cervical spine surgery for CSM, patients with DM exhibited more wound infections, epidural/wound hematomas, chronic lung disease, and cardiac complications vs. non DM patients [Table 3].[12] They strongly recommended better control of diabetes prior to cervical spinal surgery (e.g., more screened with preoperative HbA1c levels) to reduce AE, and strongly recommended DM patients be followed with more stringent diabetic/insulin-based protocols postoperatively to improve outcomes.
Table 2.
Increased risks of spine surgery in diabetic patients (references 2014-2015)
NEGATIVE IMPACT OF DIABETES ON ANTERIOR CERVICAL DISKECTOMY/FUSION
Out of 3726 patients undergoing ACDF obtained from an ACS NSQIP (American College of Surgeons-National Surgical Quality Improvement Program) database, Phan et al. (2016) showed that IDDM (171 patients) and NIDDM (270 patients) exhibited higher risks, complication rates, AE, and greater 30-day reoperation/readmission rates [Table 3].[19] Compared with those who did not have DM, IDDM had higher reoperation/readmission rates, and longer average LOS (mean >5 days), whereas NIDDM experienced more urinary tract infections (UTI) and returns to the operating room (OR).
VARIABLE IMPACT OF DIABETES ON POSTERIOR CERVICAL SURGERY
DM had a variable impact on the frequency of AE and outcomes doe for posterior cervical surgery [e.g., including laminoplasty and posterior cervical fusion (PCF)]. Over 12 months following double door laminoplasty performed for CSM (mean 66.6 years of age), Machino (2014) showed comparable AE/outcomes for 105 DM vs. 400 non DM patients [Table 2].[13] Alternatively, in Medvedev et al. (2016) analysis of the ACS-NSQIP database (2011–2012) for 5627 patients undergoing posterior cervical fusion revealed 26.3% (1482 patients) of AE were related to transfusions whereas diabetes largely contributed to the remaining 9.8% of AE. Other risk factors included; prolonged intubation (>1.5%), reintubation in 72 (1.3%), readmission in 398 (7.8%) patients, and reoperations (4.9%) in 273 patients (e.g. most for infections) [Table 3].[14] Additional risk factors included; female sex, longer surgical time, combined anterior-posterior surgery, preoperative inpatient status, smoking, ASA class 3 or higher, and older age. Lee et al. (2016) additionally showed that residents performing 223 (43.1%) of 448 PCF posterior cervical fusions (PCF: ACS NSQIP database (2005–2012) increased transfusion rates, LOS (by >5 days), and OR times (>4 hours) [Table 3].[11] Interestingly, DM, age ≥81, and multilevel fusions were independent risk factors increasing complication rates with/without resident involvement.
DIABETES NEGATIVE IMPACT ON INTRAOPERATIVE NEURAL MONITORING FOR SPINE SURGERY
DM had a negative impact on intraoperative neural monitoring (IONM) for patients undergoing decompressive cervical surgery for myelopathy (CCM) [Tables 2 and 3].[15,18] Nakanishi et al. (2015) compared the results of IONM for 22 patients with CCM/DM vs. 92 with CCM/no DM vs. 24 controls/no DM undergoing decompressive cervical surgery [Table 2].[15] Correlating JOA scores 1 year postoperatively with intraoperative Motor Evoked Potentials (MEPs), Peripheral conduction time (PCT), and Central Motor Conduction Times (CMCT) all potentials were abnormal for DM in both the upper and lower motor neurons. Pease et al. (2016) also found DM was one of the several variables contributing to significant IONM changes (e.g., sensitivity/specificity of IONM in detecting new neurological deficits) during 1373 posterior cervical procedures [Table 3].[18] Other variables included; length of surgery, age, sex, BMI (body mass index), hypertension (HTN), coronary artery disease (CAD), cerebrovascular disease, and smoking.
DIABETES: VARIABLE IMPACT ON ADVERSE EVENTS/LENGTH OF STAY FOR ELECTIVE GENERAL ORTHOPEDIC PROCEDURES
Two studies demonstrated the variable impact of DM on AE/LOS/outcomes for general orthopedic procedures [Tables 2 and 3].[10,27] Kerr et al. (2016) found 1 of 3 hospitalized adults in California (CA) had DM; this did not significantly increase LOS for elective general orthopedic surgery [Table 3].[10] Of 11,476,073 discharges from 309 CA hospitals, DM did not significantly increase LOS following hip, spine, or knee surgery (n = 318,861 patients). The Public Use California Patient Discharge Data Files (CPDDF) (2010-2012) showed 16% of discharges included a diagnosis of diabetes; however, the average LOS was comparable with (3.40 days with DM) vs. without DM (3.11 days without DM). Alternatively, Wukich (2015) observed, following orthopedic spine surgery, that poorly controlled DM resulted in poorer wound healing, and higher rates of AE, neuropathy, peripheral artery disease, and end-stage renal disease [Table 2].[27]
The marked disparity in results for orthopedic procedures involving DM patients utilizing such large database analyses remains difficult to explain. One question is who was doing the surgery? When residents were involved, greater morbidity typically follows (e.g., greater LOS and more transfusions), a finding typically attributed to their inexpert technical/surgical skills. Here, better supervision by more senior surgeons/physicians may improve results. On the other hand, there may be great disparities in different settings (e.g., private practice vs. academia with residents) regarding how patients are selected for surgery. Some surgeons may choose to operate on patients irrespective of their comorbidities, whereas others may perform surgery without sufficient indications (e.g., unnecessary surgery). Another major consideration is whether the data entered into the various large databases (ACS-NSQIP, CPDDF, NIS) were correct, relevant, and appropriate for the problem under investigation. Certainly, these questionnaires may miss the critical factors that may be truly impacting outcomes.
DIABETES RESULTED IN GREATER MORBIDITY/MORTALITY AND POORER OUTCOMES WITH LUMBAR FUSIONS VS. THOSE WITHOUT DIABETES MELLITUS
Multiple studies documented increased complication/AE rates for DM patients undergoing lumbar fusions [Tables 1–3].[2,4,7,20,22,23] Browne et al. (2007) used the NIS database (1988–2003) to study perioperative morbidity and mortality rates for 197,461 patients undergoing lumbar fusions; 11000 patients (5.6%) had a postoperative diagnosis of DM (using HbA1c levels) that increased the risk for postoperative infection, transfusions, pneumonia, in-hospital mortality, non-routine discharges, higher total charges, and LOS. [Table 1].[2] Freedman et al. (2011) in the Spine Patient Outcomes Research Trial (SPORT) found DM (199 patients) had better outcomes (SF-36, ODI) without LDH surgery [Table 1].[7] DM were also older, had higher BMIs, and greater frequencies of hypertension, stroke, cardiovascular disease, and joint pathology. In Takahashi et al. (2013) series, poor outcomes followed lumbar fusions in DM (41 patients; lower17.9 VAS score) vs. non-DM (124 patients; higher VAS scores 29.3) patients 50 years of age or older [Table 1].[23] DM also correlated with higher rates of pseudarthrosis (20% with DM vs. 3% without DM), and residual postoperative back pain. In addition, using the National Health Insurance Research Database of Taiwan involving 6949 patients undergoing instrumented spinal fusion. Chiu et al. (2016) found DM had higher frequencies of delayed postoperative vertebral compression fractures (VCFs) [Table 3].[4] When Qin et al. (2016) studied the NSQIP database of 51277 patients undergoing lumbar surgery, LOS was significantly increased for NIDDM (3.2 days) and IDDM (3.9 days) who also had more medical complications vs. non DM (2.6 days) [Table 3].[20] Notably, IDDM also exhibited greater surgical complications and higher 30-day unplanned readmission rates. Silverstein et al. (2016) looked at the impact of DM (212 patients) vs. no DM on patients undergoing lumbar decompressions; non DM showed significant improvements in EQ-5D (EuroQol five dimensions questionnaire), PDQ (Parkinson's disease Questionnaire), and PHQ-9 (Patient Health Questionnaire-9), as well as on postoperative quality of life (QOL) questionnaires utilizing minimal clinically important differences (MCIDs) [Table 3].[22] It would certainly appear that larger the study, the more clearly the negative impact of DM for patients undergoing for patients undergoing spinal surgery.
VARIABLE IMPACT OF DIABETES ON SCOLIOSIS FUSION SURGERY
Two series, one very small, and another every large (NIS), demonstrated very different conclusions regarding the impact of DM vs. no DM on scoliosis surgery [Tables 1 and 3].[5,21] Cho et al. (2012) found comparable major/minor complications/outcomes for scoliosis surgery performed in their very small series involving just 23 NIDDM vs. 23 controls (non-DM) over a minimum 2-year period [Table 1].[5] Alternatively, Shin et al. (2016) large NIS database (2002–2011) series focusing on non DM, CDM, and UCDM patients undergoing fusions for idiopathic scoliosis (>45 years of age), documented poor glycemic control in DM had a major negative impact on morbidity/mortality rates [Table 3].[21] Furthermore, CDM patients exhibited significantly higher rates of acute renal failure (ARF), whereas UCDM patients had more acute postoperative hemorrhages, deep vein thrombosis, and in-patient mortality. Here, the Shin et al. study's much larger patient sample allowed for documentation of significantly greater morbidity for DM vs. non DM patients undergoing spinal surgery.
DIABETES: A MAJOR RISK FACTOR FOR SPINAL EPIDURAL ABSCESS (SEA)
DM is a major risk factor for patients to develop SEA following spinal surgery, it could also contribute to the postoperative risk of SEA. When Patel et al. (2014) examined 128 consecutive bacterial SEA extending over an average of 3.85 disc levels, DM was a major risk factor (21.9%) along with intravenous (IV) drug abuse (39.1%) [Table 2].[17] Thirty of 51 patients were successfully treated with antibiotics alone (group 1), whereas 21 (41%; group 3) failed medical management and warranted delayed surgery. Factors contributing to failure of antibiotics alone to treat seA included; DM, C-reactive protein >115, white blood count >12.5, and positive blood cultures. The remaining 77 group 2 patients were successfully initially managed with surgery, followed by IV antibiotic therapy.
VANCOMYCIN POWDER WITH ROUTINE INTRAVENOUS ANTIBIOTICS DECREASED THE RISK OF SURGICAL SITE INFECTION FOLLOWING INSTRUMENTED FUSION
Ten percent of patients undergoing posterior spinal instrumented infections secondary to trauma typically develop surgical site infection (SSI: deep or superficial) (deep/superficial) [Table 1].[16] Over a 2-year period, O’Neill et al. (2011) observed a reduced 0% incidence of SSI for 56 patients undergoing instrumented posterior spine fusions who had received local vancomycin powder/IV antibiotics (cefazolin) vs. a 13% frequency of SSI for 54 control patients receiving IV cefazolin alone [Table 1].[16] However, in Gaviola et al. series (2016), they documented only a “trend” favoring the reduction of SSI following multilevel spinal fusions (MLSF) using Vancomycin powder; SSI occurred in 5.2% (6/116 patients) utilizing topical Vancomycin/IV cefazolin vs. 11% (23/210 patients) receiving cefazolin alone [Table 3].[8] Major risk factors contributing to the risk for SSI notably included DM along with female sex, and greater invasiveness.
DIABETES ALONE OR WITH OTHER MAJOR COMORBIDITIES INCREASED TOTAL HOSPITAL COSTS AND LENGTH OF STAY FOR SPINE SURGERY
For patients undergoing spine surgery, DM alone or combined with other major comorbidities, including hypothyroidism, elevated BMI, older age, and depression, increased total hospital costs, and LOS. When Walid et al. (2010) tested elevated glycosylated hemoglobin levels (HbA1c) >/=6.1) for patients undergoing lumbar microdiskectomy (LMD), ACDF, or lumbar decompression/fusion (LDF), they discovered 13.3% were known DM, 14.3% were unknown DM (e.g., prior to surgery), and 72.4% had no DM [Table 1].[24] Notably, the unknown DM undergoing LDF demonstrated significantly higher costs and LOS vs. non DM, prompting the authors to subsequently perform routine preoperative screening for DM with HbA1c levels. Evaluation of patients undergoing LMD (N = 237), ACDF (N = 339), and LDF (N = 211), revealed that 32.5% of 643 patients had elevated HbA1c levels (≥6.1%=DM); an additional 4.3% had both DM and hypothyroidism [Table 1].[25] LDF patients with both DM/hypothyroidism exhibited the longest LOS (8 days), and highest hospital costs ($71352). Subsequent evaluation of (2011) 816 patients (2005 and 2008) undergoing LMD (20.5%), ACDF (60.3%), and LDF (19.2%) revealed increased costs due not only to DM but also to elevated BMI and older age [Table 1].[26] For females undergoing ACDF, DM and severe obesity alone significantly increased the average charge to $34943 vs. $25633. For females undergoing LDF, costs were also significantly higher for those with both DM and depression ($65782) vs. DM alone ($53504). The economics of spine surgery indicate that DM either alone or combined with other major risk factors significantly contributed to more prolonged LOS and higher hospital costs. Screening for DM prior to surgery with routine HbA1c levels may better prepare the surgeon, patient, and hospital for increased perioperative challenges.[24]
CONCLUSION
The vast majority of the larger series utilizing major U.S. patient databases, documented that diabetic patients (e.g., IDDM, NIDDM, CDM, UCDM) undergoing spine surgery exhibited more perioperative morbidity/AE/complications, longer LOS, higher 30-day readmission/reoperation rates, and increased mortality compared with non DM. Only a subset of smaller studies, too small to yield “significant findings,” demonstrated no negative impact of DM on the results of spinal surgery. Future routine preoperative screening for DM with HbA1c levels would likely be worthwhile (e.g., one series demonstrated 14.3% of patients were “unknown DM”), as this could facilitate better preoperative, intraoperative, and postoperative management.[24]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Footnotes
REFERENCES
- 1.Arnold PM, Fehlings MG, Kopjar B, Yoon ST, Massicotte EM, et al. Mild diabetes is not a contraindication for surgical decompression in cervical spondylotic myelopathy: Results of the AOSpine North America multicenter prospective study (CSM) Spine J. 2014;14:65–72. doi: 10.1016/j.spinee.2013.06.016. [DOI] [PubMed] [Google Scholar]
- 2.Browne JA, Cook C, Pietrobon R, Bethel MA, Richardson WJ. Diabetes and early postoperative outcomes following lumbar fusion. Spine (Phila Pa 1976) 2007;32:2214–9. doi: 10.1097/BRS.0b013e31814b1bc0. [DOI] [PubMed] [Google Scholar]
- 3.Chikuda H, Ohya J, Horiguchi H, Takeshita K, Fushimi K, Tanaka S, et al. Ischemic stroke after cervical spine injury: Analysis of 11,005 patients using the Japanese Diagnosis Procedure Combination database. Spine J. 2014;14:2275–80. doi: 10.1016/j.spinee.2014.01.024. [DOI] [PubMed] [Google Scholar]
- 4.Chiu YC, Tsai TT, Yang SC, Chen HS, Kao YH, Tu YK. Impact of Instrumented Spinal Fusion on the Development of Vertebral Compression Fracture. Medicine (Baltimore) 2016;95:e3455. doi: 10.1097/MD.0000000000003455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cho W, Lenke LG, Bridwell KH, Dorward IG, Shoda N, Baldus CR, et al. Comparison of spinal deformity surgery in patients with non-insulin-dependent diabetes mellitus (NIDDM) versus controls. Spine (Phila Pa 1976) 2012;37:E978–84. doi: 10.1097/BRS.0b013e31824edf42. [DOI] [PubMed] [Google Scholar]
- 6.Epstein NE. How much medicine do spine surgeons need to know to better select and care for patients? Surg Neurol Int. 2012;3(Suppl 5):S329–49. doi: 10.4103/2152-7806.103866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Freedman MK, Hilibrand AS, Blood EA, Zhao W, Albert TJ, Vaccaro AR, et al. The impact of diabetes on the outcomes of surgical and nonsurgical treatment of patients in the spine patient outcomes research trial. Spine (Phila Pa 1976) 2011;36:290–307. doi: 10.1097/BRS.0b013e3181ef9d8c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gaviola ML, McMillian WD\, Ames SE, Endicott JA, Alston WK. A Retrospective Study on the Protective Effects of Topical Vancomycin in Patients Undergoing Multilevel Spinal Fusion. Pharmacotherapy. 2016;36:19–25. doi: 10.1002/phar.1678. [DOI] [PubMed] [Google Scholar]
- 9.Guzman JZ, Skovrlj B, Shin J, Hecht AC, Qureshi SA, Iatridis JC, et al. The impact of diabetes mellitus on patients undergoing degenerative cervical spine surgery. Spine (Phila Pa 1976) 2014;39:1656–65. doi: 10.1097/BRS.0000000000000498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kerr D, Yadollahi M, Bautista HM, Chen X, Dong S, Guerrier SN, et al. Use of a Publicly Available Database to Determine the Impact of Diabetes on Length of Hospital Stay for Elective Orthopedic Procedures in California. Popul Health Manag. 2016;19:439–44. doi: 10.1089/pop.2015.0125. [DOI] [PubMed] [Google Scholar]
- 11.Lee NJ, Kothari P, Kim C, Leven DM, Skovrlj B, Guzman JZ, et al. The Impact of Resident Involvement in Elective Posterior Cervical Fusion. Spine (Phila Pa 1976) 2016 Feb 1; doi: 10.1097/BRS.0000000000001477. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 12.Liu Y, Ban DX, Kan SL, Cao TW, Feng SQ. The Impact of Diabetes Mellitus on Patients Undergoing Cervical Spondylotic Myelopathy: A Meta-Analysis. Eur Neurol. 2017;77:105–12. doi: 10.1159/000453547. [DOI] [PubMed] [Google Scholar]
- 13.Machino M, Yukawa Y, Ito K, Inoue T, Kobayakawa A, Matsumoto T, et al. Impact of diabetes on the outcomes of cervical laminoplasty: A prospective cohort study of more than 500 patients with cervical spondylotic myelopathy. Spine (Phila Pa 1976) 2014;39:220–7. doi: 10.1097/BRS.0000000000000102. [DOI] [PubMed] [Google Scholar]
- 14.Medvedev G, Wang C, Cyriac M, Amdur R, O’Brien J. Complications, Readmissions, and Reoperations in Posterior Cervical Fusion. Spine (Phila Pa 1976) 2016;41:1477–83. doi: 10.1097/BRS.0000000000001564. [DOI] [PubMed] [Google Scholar]
- 15.Nakanishi K, Tanaka N, Kamei N, Hiramatsu T, Ujigo S, Sumiyoshi N, et al. Electrophysiological assessments of the motor pathway in diabetic patients with compressive cervical myelopathy. J Neurosurg Spine. 2015;23:707–14. doi: 10.3171/2015.3.SPINE141060. [DOI] [PubMed] [Google Scholar]
- 16.O’Neill KR, Smith JG, Abtahi AM, Archer KR, Spengler DM, McGirt MJ, et al. Reduced surgical site infections in patients undergoing posterior spinal stabilization of traumatic injuries using vancomycin powder. Spine J. 2011;11:641–6. doi: 10.1016/j.spinee.2011.04.025. [DOI] [PubMed] [Google Scholar]
- 17.Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: Risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014;14:326–30. doi: 10.1016/j.spinee.2013.10.046. [DOI] [PubMed] [Google Scholar]
- 18.Pease M, Gandhoke GS, Kaur J, Thirumala P, Balzer J, Crammond D, et al. Predictive Value of Intraoperative Neurophysiological Monitoring During Spine Surgery: A Prospective Analysis of 4489 Consecutive Patients. Neurosurgery. 2016;63(Suppl 1):192–3. [Google Scholar]
- 19.Phan K, Kim JS, Lee N, Kothari P, Cho SK. Impact of Insulin Dependence on Perioperative Outcomes following Anterior Cervical Discectomy and Fusion (ACDF) Spine (Phila Pa 1976) 2016 doi: 10.1097/BRS.0000000000001829. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 20.Qin C, Kim JY, Hsu WK. Impact of Insulin Dependence on Lumbar Surgery Outcomes: An NSQIP Analysis of 51,277 Patients. Spine (Phila Pa 1976) 2016;41:E687–93. doi: 10.1097/BRS.0000000000001359. [DOI] [PubMed] [Google Scholar]
- 21.Shin JI, Phan K, Kothari P, Kim JS, Guzman JZ, Cho SK. Impact of Glycemic Control on Morbidity and Mortality in Adult Idiopathic Scoliosis Patients Undergoing Spinal Fusion. Clin Spine Surg. 2016 doi: 10.1097/BSD.0000000000000447. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 22.Silverstein MP, Miller JA, Xiao R, Lubelski D, Benzel EC, Mroz TE. The impact of diabetes upon quality of life outcomes after lumbar decompression. Spine J. 2016;16:714–21. doi: 10.1016/j.spinee.2015.10.041. [DOI] [PubMed] [Google Scholar]
- 23.Takahashi S, Suzuki A, Toyoda H, Terai H, Dohzono S, Yamada K, et al. Characteristics of diabetes associated with poor improvements in clinical outcomes after lumbar spine surgery. Spine (Phila Pa 1976) 2013;38:516–22. doi: 10.1097/BRS.0b013e318273583a. [DOI] [PubMed] [Google Scholar]
- 24.Walid MS, Newman BF, Yelverton JC, Nutter JP, Ajjan M, Robinson JS., Jr Prevalence of previously unknown elevation of glycosylated hemoglobin in spine surgery patients and impact on length of stay and total cost. J Hosp Med. 2010;5:E10–4. doi: 10.1002/jhm.541. [DOI] [PubMed] [Google Scholar]
- 25.Walid MS, Zaytseva N. How does chronic endocrine disease affect cost in spine surgery? World Neurosurg. 2010;73:578–81. doi: 10.1016/j.wneu.2010.02.066. [DOI] [PubMed] [Google Scholar]
- 26.Walid MS, Robinson JS., Jr Economic impact of comorbidities in spine surgery. J Neurosurg Spine. 2011;14:318–21. doi: 10.3171/2010.11.SPINE10139. [DOI] [PubMed] [Google Scholar]
- 27.Wukich DK. Diabetes and its negative impact on outcomes in orthopaedic surgery. World J Orthop. 2015;6:331–9. doi: 10.5312/wjo.v6.i3.331. [DOI] [PMC free article] [PubMed] [Google Scholar]