

Description
A 16-year-old boy presented with complaints of recent onset difficulty in walking, progressive diminution of vision and a long-standing persistent occipital headache. Physical examination suggested cerebellar ataxia, positive cerebellar signs, macrocephaly and bilateral papilloedema. MRI of the brain revealed a mass lesion with prominent striated folial pattern involving the right cerebellar hemisphere and causing obstructive hydrocephalus. The lesion appeared hypointense on T1 (figure 1) and hyperintense on T2 (figure 2) weighted images, with parallel linear striations. A diagnosis of Lhermitte-Duclos disease was made from the classical findings on neuroimaging.
Figure 1.
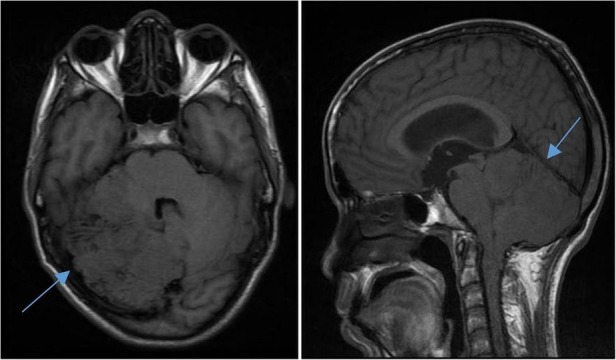
T1 weighted MRI of the brain showing a hypointense mass lesion (blue arrow) of right cerebellar hemisphere with striated folial pattern.
Figure 2.

T2 weighted MRI of brain showing a hyperintense mass lesion (blue arrow) of right cerebellar hemisphere with striated folial pattern.
Lhermitte-Duclos disease, or dysplastic cerebellar gangliocytoma, is a rare hamartomatous lesion due to abnormal development and unilateral hemispheric expansion of the cerebellum. Although the exact aetiology remains unknown, a germline mutation of phosphatase and tensin homologue on chromosome 10q23 is considered widely as the underlying defect.1 Usually occurring in young adults, it manifests with headache, visual disturbances, cerebellar dysfunction, ataxia, cranial nerve palsies and occlusive hydrocephalus.2 Thickening and hypermyelination of outer molecular layer, loss of Purkinje cells and white matter, dysplastic ganglion cells with rounded nuclei and abundant mitochondria invading the inner granular layer are histological hallmarks. MRI of the brain reveals a typical striated, tigroid folial pattern of the cerebellum.3 Often, it occurs in association with Cowden disease, a multiple hamartoma–neoplasia complex. A ventriculoperitoneal shunt aimed at relieving obstructive hydrocephalus followed by resection of the mass has been planned for this patient. Knowledge of the characteristic radiological findings helps in diagnosing this rare disease and spares the need for biopsy in most cases.
Learning points.
Lhermitte-Duclos disease, or dysplastic cerebellar gangliocytoma, is a rare hamartomatous lesion of the cerebellum, mostly occurring in young adults.
Histological hallmarks of the disease are thickening and hypermyelination of the outer molecular layer, loss of Purkinje cells and white matter, dysplastic ganglion cells with rounded nuclei and abundant mitochondria invading the inner granular layer.
A non-enhancing mass in posterior fossa, hypointense on T1 and hyperintense on T2-weighted images with parallel linear striations giving a ‘tigroid’ appearance of cerebellum, is considered diagnostic.
Footnotes
Contributors: SNB contributed to diagnosis of the patient, acquisition of data, concept and design of the paper, drafting of the article and final approval. PPC and SP contributed to diagnosis of the patient, concept and design of the paper, drafting of the article, intellectual input, critical revision and final approval.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Zhou XP, Marsh DJ, Morrison CD et al. Germline inactivation of PTEN and dysregulation of the phosphoinositol-3-kinase/Akt pathway cause human Lhermitte-Duclos disease in adults. Am J Hum Genet 2003;73:1191–8. 10.1086/379382 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Milbouw G, Born JD, Martin D et al. Clinical and radiological aspects of dysplastic gangliocytoma (Lhermitte-Duclos disease): a report of two cases with review of the literature. Neurosurgery 1988;22:124–8. 10.1227/00006123-198801010-00020 [DOI] [PubMed] [Google Scholar]
- 3.Meltzer CC, Smirniotopoulos JG, Jones RV. The striated cerebellum: an MR imaging sign in Lhermitte-Duclos disease (dysplastic gangliocytoma). Radiology 1995;194:699–703. 10.1148/radiology.194.3.7862965 [DOI] [PubMed] [Google Scholar]