

Abstract
Aim
To compare day‐to‐day and within‐day variability in glucose‐lowering effect between insulin degludec (IDeg) and insulin glargine 300 U/mL (IGlar‐U300) in type 1 diabetes.
Materials and methods
In this double‐blind, crossover study, patients were randomly assigned to 0.4 U/kg of IDeg or IGlar‐U300 once daily for two treatment periods lasting 12 days each. Pharmacodynamic variables were assessed at steady‐state from the glucose infusion rate profiles of three 24‐hour euglycaemic glucose clamps (days 6, 9 and 12) during each treatment period.
Results
Overall, 57 patients completed both treatment periods (342 clamps). The potency of IGlar‐U300 was 30% lower than IDeg (estimated ratio 0.70, 95% confidence interval [CI] 0.61; 0.80; P < .0001). The distribution of glucose‐lowering effect was stable across 6‐hour intervals (24%‐26%) for IDeg, while IGlar‐U300 had greater effects in the first (35%) and last (28%) intervals compared with 6 to 12 hours (20%) and 12 to 18 hours (17%). Within‐day variability (relative fluctuation) was 37% lower with IDeg than with IGlar‐U300 (estimated ratio IDeg/IGlar‐U300: 0.63, 95% CI 0.54; 0.73; P < .0001). The day‐to‐day variability in glucose‐lowering effect with IDeg was approximately 4 times lower than IGlar‐U300 (variance ratio IGlar‐U300/IDeg: 3.70, 95% CI 2.42; 5.67; P < .0001). The day‐to‐day variability in glucose‐lowering effect assessed in 2‐hour intervals was consistently low with IDeg over 24 hours, but steadily increased with IGlar‐U300 to a maximum at 10 to 12 hours and 12 to 14 hours after dosing (variance ratios 12.4 and 11.4, respectively).
Conclusion
IDeg has lower day‐to‐day and within‐day variability than IGlar‐U300 and a more stable glucose‐lowering effect, which might facilitate titration and enable tighter glycaemic control with a reduced risk of hypoglycaemia.
Keywords: insulin analogues, insulin therapy, pharmacodynamics, type 1 diabetes
1. INTRODUCTION
A predictable glucose‐lowering effect after administering daily insulin doses is one of the fundamental aspects of successful insulin replacement therapy. Particularly for basal insulins, minimal day‐to‐day pharmacodynamic variability as well as low within‐day variability (ie, a peakless metabolic profile) are conducive to optimizing insulin titration, and thereby achieve glycaemic targets with a low risk of hypoglycaemia;1 however, the pharmacodynamic effect of exogenously administered insulin analogues is often variable owing to their physicochemical properties defining the mode of protraction principle and affecting absorption.2, 3
In general, it seems that insulins that stay in solution after subcutaneous (s.c.) injection, for example, insulin detemir, show lower day‐to‐day variability than insulins forming microprecipitates after s.c. injection, such as insulin glargine 100 U/mL (IGlar‐U100) and neutral protamine Hagedorn insulin (NPH).4 Furthermore, it is conceivable that basal insulins with a duration of action lasting considerably longer than 24 hours should also have lower day‐to‐day variability because there are overlapping effects of several injections, so that opposing changes in absorption of these injections are minimized.3 Indeed, ultra‐long acting insulin degludec (IDeg) self‐associates into multi‐hexamers upon s.c. injection, resulting in a soluble depot with continuous insulin release into circulation. It is known that this unique mechanism of protraction of IDeg leads to a half‐life of ~24 hours and thus significantly lower day‐to‐day variability than IGlar‐U100 (coefficient of variation [CV] 20% vs 82%).5 In addition to low day‐to‐day variability, IDeg also had a peakless time–action profile, that is, lower within‐day variability and a more even distribution of the glucose‐lowering effect over a 24‐hour treatment period, compared with IGlar‐U100.6
A higher concentrated formulation of insulin glargine (300 U/mL; IGlar‐U300), is now available and has been shown to have a longer duration of action and a more even activity profile than IGlar‐U1007; however, ultrastructural three‐dimensional visualization showed that IGlar‐U300 forms larger microprecipitates than IGlar‐U100, which probably results in delayed absorption and possibly an uneven release of insulin monomers into the circulation, which in turn may increase day‐to‐day variability and confer lower potency.8, 9
We therefore investigated the pharmacodynamic properties, including potency, distribution of glucose‐lowering effect over 24 hours, and day‐to‐day and within‐day variability of IDeg and IGlar‐U300 at steady‐state in patients with type 1 diabetes (T1D).
2. MATERIALS AND METHODS
2.1. Study design
The design of the present single‐centre, randomized, double‐blind, two‐period, crossover study is shown in Figure 1. The trial was approved by the local ethics committee and health authorities and was conducted between August 28, 2015 and April 14, 2016 in accordance with Good Clinical Practice Guidelines (International Conference on Harmonization) and the Declaration of Helsinki. Written informed consent was obtained from all participants prior to initiation of any study‐related activity. This study is registered on clinicaltrials.gov (Identifier: NCT02536859).
Figure 1.
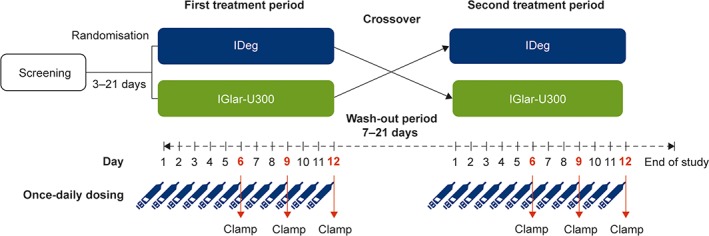
Study design
2.2. Participants
Men and women (18‐64 years old) with T1D for ≥12 months were enrolled at Profil, Neuss, Germany. Treatment periods were standardized with the menstrual cycle for women. Additional inclusion criteria were body mass index (BMI) 18.5 to 29.0 kg/m2, glycated haemoglobin (HbA1c) ≤9.0%, fasting C‐peptide <0.3 nmol/L, multiple daily insulin injections or continuous s.c. insulin infusion for ≥12 months (total daily insulin <1.2 U/kg/d) and a daily basal insulin requirement ≥0.2 U/kg/d. Participants with clinically relevant diseases and a history of recurrent severe hypoglycaemia or hypoglycaemic unawareness were excluded.
2.3. Treatments
Participants were randomly assigned (1:1) to receive 0.4 U/kg of IDeg 200 U/mL (Tresiba; Novo Nordisk, Bagsvaerd, Denmark) or IGlar‐U300 (Toujeo; Sanofi, Frankfurt, Germany) once daily for 12 days (first treatment period), followed by a complete crossover to the other treatment during the second treatment period. The treatment periods were separated by a wash‐out period lasting 7 to 21 days to ensure that there were no carryover effects from the previous period. Both treatments were administered s.c. into a lifted skin fold in the thigh at approximately 8:00 pm at the investigational site by a person otherwise not involved in the trial, in accordance with the double‐blind design. A strict injection interval of 24 hours was maintained for each individual. Carryover effects of previously used insulins were avoided by switching patients on IDeg to NPH 72 hours prior to administration of the trial product in each treatment period, and those on insulin detemir or IGlar were switched to NPH 48 hours in advance. The last injection of NPH was administered no later than 12 hours before the first study dose. During treatment periods, except on clamp days where no additional insulin administration was allowed, only insulin aspart was used as additional bolus insulin to adjust the blood glucose (BG) level, in case the fixed basal dose of 0.4 U/kg was too low to maintain normoglycaemia. The last injection of insulin aspart was administered no later than 10 hours before the trial product was injected on clamp days.
2.4. Clamp
The euglycaemic clamp procedure was performed using ClampArt (Profil) that continuously measured BG and adjusted glucose infusion rates (GIRs) every minute to achieve a target BG concentration of 5.5 mmol/L (100 mg/dL). The participants, who had been fasting on arrival at the investigational site, received a variable intravenous infusion of human soluble insulin (15 IU Actrapid [100 IU/mL, Novo Nordisk, Bagsvaerd, Denmark] in 49 mL saline and 1 mL of the patients’ blood) or glucose to obtain the target BG level, approximately 5 hours before the trial product administration on the clamp days. Insulin infusion, if applied, was stopped immediately before trial product administration. The glucose clamp lasted for 24 hours after dosing and was prematurely terminated if BG levels consistently exceeded 11.1 mmol/L (200 mg/dL) without glucose infusion for at least 30 minutes. Throughout the procedure patients remained in a semi‐supine position and were in a fasting state, with water intake permitted.
2.5. Assessments
The GIR and BG concentrations were measured during each treatment period for every 24‐hour euglycaemic clamp on days 6, 9 and 12 (ie, at steady‐state). The primary endpoint was day‐to‐day variability in glucose‐lowering effect, evaluated as within‐patient variance for AUCGIR,τ,SS, where AUCGIR,τ,SS is the area under the GIR curve during 1 dosing interval (0‐24 hours,τ) at steady‐state. Secondary endpoints that supported the primary endpoint included within‐patient variance for AUCGIR,2‐24h,SS, maximum GIR at steady‐state (GIRmax,SS) and AUCGIR,x,SS over 2‐hour intervals, where x = 0 to 2 hours, 2 to 4 hours, 4 to 6 hours, up to 22 to 24 hours. Additionally, potency (total glucose‐lowering effect estimated using AUCGIR,τ,SS), within‐day variability, and the distribution of glucose‐lowering effects (AUCGIR,SS over 6‐hour intervals) were evaluated. Safety and tolerability were monitored throughout the trial. Hypoglycaemia episodes were defined as confirmed when they were either “severe”, as per the American Diabetes Association classification,10 or verified by plasma glucose levels <3.1 mmol/L (56 mg/dL).
2.6. Statistical methods
Day‐to‐day variability was estimated using within‐participant variance of log‐transformed AUCGIR,τ,SS derived from individual GIR profiles. The standard locally weighted scatterplot smoothing (LOESS) procedure, with a pre‐specified smoothing factor of 0.25, was applied to individual GIR curves. Area under the individual smoothed GIR curves from each clamp (AUCGIR,τ,SS) was calculated using the trapezoidal technique on interpolated points. For each participant and treatment, the variance of log‐transformed AUCGIR,τ,SS from the three clamps in each treatment period was calculated (one variance in each treatment period for every participant). Within‐participant variances were then compared between the two treatments using a multiplicative linear mixed effect model, with treatment and period as fixed effects and participant as a random effect. The geometric mean within‐participant variances for each of the treatments, variance ratios and corresponding 95% confidence intervals (CIs) were estimated from this model. Secondary endpoints supporting day‐to‐day variability were investigated using the same model as for the primary endpoint. Potency was estimated by analysing the geometric means of AUCGIR,τ,SS from the three clamps for each patient and treatment using the same model as for the primary endpoint.
Within‐day variability (ie, fluctuation) was calculated as cumulated AUCs of an individual's GIR profile above and below the mean GIR over 24 hours (AUCFGIR,τ,SS) for each clamp. Because of the different potency of the study insulins, relative fluctuation (AUCFGIR,τ,SS as percent of the AUCGIR,τ,SS) rather than absolute fluctuation was assessed (post hoc analysis). The geometric means of relative fluctuation from 3 clamps in each treatment were analysed using the same model as for the primary endpoint.
An additional statistical analysis was pre‐planned, in which participants with low GIR responses were excluded from the primary analysis. The participants were identified based on blinded inspection of the GIR and BG profiles. In these participants, BG was higher than the clamp target and GIR was 0 for the majority of the 24‐hour period in any clamp in either treatment period.
3. RESULTS
3.1. Participant disposition and baseline characteristics
Of 71 people screened, 60 were randomized and exposed to either IDeg or IGlar‐U300. Pharmacodynamic data from 57 participants who completed both treatment periods are presented, while the safety analysis included all randomized participants. During the first treatment period, 3 participants (IDeg, n = 2; IGlar‐U300, n = 1) discontinued as a result of investigator decision (low HbA1c and several hypoglycaemic episodes), withdrawal of consent and protocol violation (dose miscalculated by site personnel), respectively. Before study discontinuation, 2 participants receiving IDeg had completed 2 clamps each and 1 participant receiving IGlar‐U300 had completed 3 clamps. At baseline, the mean age was 45.1 years, BMI was 25.6 kg/m2, diabetes duration was 21.9 years, HbA1c was 7.3% and basal insulin dose was 0.32 units/kg (Table S1, Supporting Information).
3.2. Potency, distribution of glucose‐lowering effect and within‐day variability
The potency of IGlar‐U300 was 30% lower than that of IDeg (estimated ratio of AUCGIR,τ,SS IGlar‐U300/IDeg: 0.70, 95% CI 0.61; 0.80; P < .0001).
The mean smoothed 24‐hour GIR profiles were based on 171 individual GIR profiles (3 clamps each, in 57 participants per treatment arm; Figure 2A,B). The distribution of glucose‐lowering effect (AUCGIR as a proportion of AUCGIR,τ,SS) was more flat and stable for IDeg than for IGlar‐U300. Across 6‐hour intervals, the proportion of glucose‐lowering effect was maintained at 24% to 26% for IDeg (Figure 2C), whereas IGlar‐U300 showed a U‐shaped distribution, with significantly greater effect in the first and last 6‐hour intervals compared with the 6‐ to 12‐hour and 12‐ to 18‐hour intervals (P < .0001; Figure 2D). IDeg had 37% lower relative within‐day variability compared with IGlar‐U300 (estimated ratio IDeg/IGlar‐U300: 0.63, 95% CI 0.54; 0.73; P < .0001).
Figure 2.
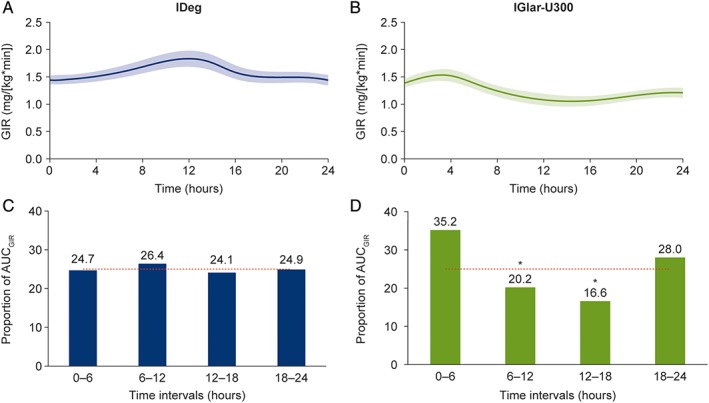
Pharmacodynamic profiles: 24‐hour GIR profiles and distribution of glucose‐lowering effect at steady state for IDeg (A and C) and IGlar‐U300 (B and D). Shaded bands represent the standard error of mean in (A) and (B). (C) and (D) present AUCGIR for each 6‐hour interval as a percentage of AUCGIR ,τ, SS . *P < .0001 compared with the 0‐ to 6‐hour and 18‐ to 24‐hour intervals
3.3. Blood glucose profiles
The 171 individual BG profiles of the participants after IDeg treatment appeared relatively stable around the clamp target (Figure 3A). By contrast, the lower potency of IGlar‐U300 was also reflected in the individual profiles showing BG levels >7 mmol/L in 14 patients (19 of 171 profiles) during the middle of the dosing interval, suggesting a period of low insulin activity during this period. Subsequently, these BG levels decreased to the clamp target again (Figure 3B). Because of the feedback mechanism of the clamp, GIR was 0 during the time these deviations in BG occurred in the individual profiles. The BG deviations therefore align with the finding of a U‐shaped distribution of the IGlar‐U300 GIR profile seen in Figure 2D. Despite the BG deviations, glucose clamp quality (as evaluated by fluctuations in BG and mean BG deviation from target) was high in general (Table S2, Supporting Information).
Figure 3.
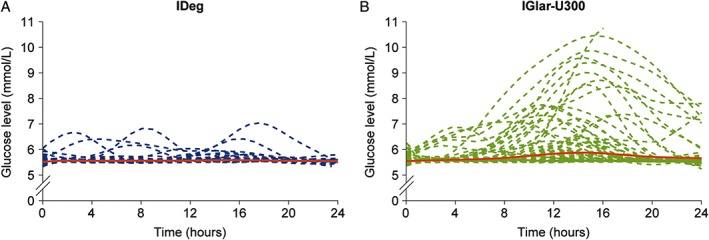
Individual BG profiles for patients treated with IDeg (A) and IGlar‐U300 (B). Red dotted line = mean BG in each treatment group; number of patients = 57; BG target in the clamp was 5.5 mmol/L (100 mg/dL)
3.4. Day‐to‐day variability in glucose‐lowering effect
Day‐to‐day variability was significantly lower with IDeg than with IGlar‐U300 for all pharmacodynamic endpoints assessed (Figure S1, Supporting Information). The day‐to‐day variability for the primary endpoint (AUCGIR,τ,SS) was approximately 4 times lower with IDeg than IGlar‐U300 (variance ratio IGlar‐U300/IDeg: 3.70, 95% CI 2.42; 5.67; P < .0001). The significant difference in variability in AUCGIR,τ, SS did not change after exclusion of 7 participants with a low GIR response (variance ratio IGlar‐U300/IDeg: 3.70, 95% CI 2.36; 5.80; P < .0001). Compared with IGlar‐U300, individual day‐to‐day variability in ranked order was consistently lower in the majority of participants after IDeg treatment (Figure 4 and Figure S2, Supporting Information).
Figure 4.
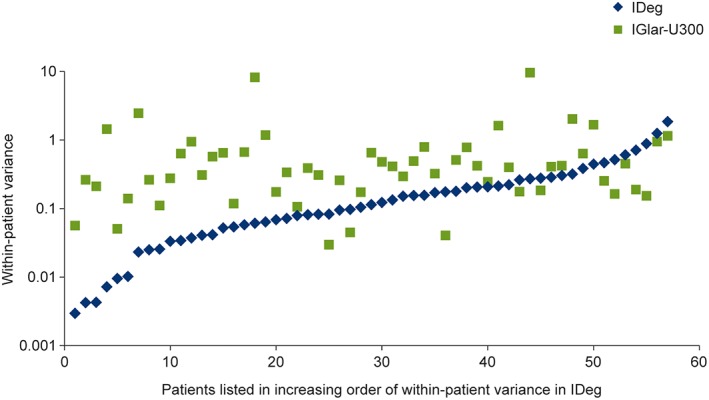
Patient‐specific day‐to‐day variability in AUCGIR ,τ, SS. SS, steady‐state
Day‐to‐day variability was also assessed in 2‐hour intervals to investigate changes over 24 hours. For IDeg, variability across all intervals remained low and stable. The variance for IGlar‐U300 was significantly higher than that for IDeg for all intervals after 2 hours, with the highest difference observed during the 10‐ to 12‐hour and 12‐ to 14‐hour intervals (IGlar‐U300/IDeg ratio 12.4 and 11.4, respectively; Figure 5).
Figure 5.
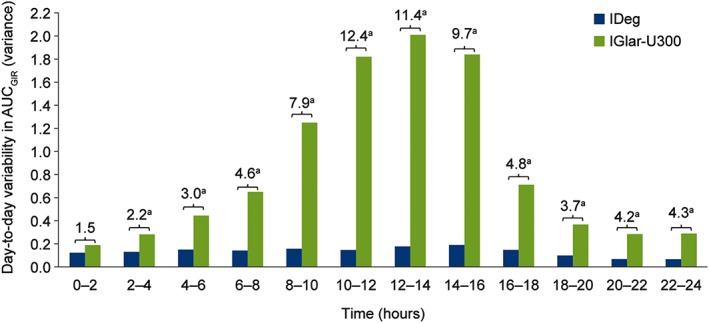
Day‐to‐day variability in glucose‐lowering effect over 24 hours at steady‐state. Differences between the treatments expressed as the variance ratio of IGlar‐U300:IDeg; a P < .05
3.5. Safety
Overall, both treatments were well tolerated. The frequency of adverse events was similar in the IDeg (22.0%) and IGlar‐U300 (22.4%) groups. No serious adverse events occurred in either group. Treatment‐emergent hypoglycaemia using a fixed dose of 0.4 U/kg (thus not individualized to participant needs), was reported in 35.6% of participants (50 episodes) after IDeg and 25.9% of participants (30 episodes) after IGlar‐U300, which might also reflect the lower potency of IGlar‐U300. No events of severe hypoglycaemia were reported.
4. DISCUSSION
This study showed that both day‐to‐day and relative within‐day variability in the glucose‐lowering effect are low with IDeg and significantly lower than IGlar‐U300 in patients with T1D. Low day‐to‐day variability in glucose‐lowering effect between injections is important for insulin titration and should lead to tighter glycaemic control over time. Along with minimal within‐day variability in a 24‐hour dosing interval, it also aids in maintenance of a reliable insulin action, thus reducing the risk of hypoglycaemia.
In addition, IGlar‐U300 showed a 30% lower potency compared with IDeg. This finding is consistent with the previously reported 27% reduction in potency with IGlar‐U300 compared with IGlar‐U100.11 Both IDeg and IGlar‐U300 were dosed at a fixed dose of 0.4 U/kg once daily, which is considered to be a clinically relevant dose expected to yield an adequately high pharmacodynamic response.5, 6 Moreover, the appropriateness of the 0.4 U/kg dose was confirmed because it was close to the normal daily basal insulin dose observed at baseline for the participants with T1D in the present study (Table S1, Supporting Information). Yet, because of its lower potency, a higher dose of IGlar‐U300 would be needed to achieve the same level of glycaemic control as that with IDeg owing to rather high BG elevations observed with IGlar‐U300, but not with IDeg, in the middle of the dosing interval in some experiments. This observation was also reflected in the U‐shaped distribution of glucose‐lowering effect seen with IGlar‐U300, suggesting low activity in the 6‐ to 12‐hour and the 12‐ to 18‐hour intervals (ie, early and late morning hours; Fig. 2D). With evening injections this distribution might be disadvantageous because insulin needs in people with T1D are often higher in these time periods12 than at other times of the day. Thus, under these circumstances, a dose of 0.4 U/kg of IGlar‐U300 is insufficient to maintain stable BG in all patients. The distribution of metabolic effect of IGlar‐U300 should be taken into account for the timing of the injection. Also, the most appropriate dosing strategy for IGlar‐U300 should be investigated in clinical trials. In contrast, IDeg maintained a flat and even distribution of the glucose‐lowering effect across 6‐hour intervals that closely mimics an ideal distribution pattern of 25% for each interval, in line with previously published findings with regard to IDeg in T1D and type 2 diabetes (T2D).5, 6, 13 It should be noted that the mean GIR curves alone could be misleading for the interpretation of the flat insulin profile because they represent an average of several individual profiles; therefore, the mean distribution of the GIR effect in 6‐hour intervals was calculated, as it might be a better indicator of flatness. The even distribution of the glucose‐lowering effect with IDeg was also supported by a 37% lower relative within‐day variability compared with IGlar‐U300. We estimated relative rather than absolute within‐day variability to allow a correction of the difference in potency between IDeg and IGlar‐U300. While a higher dose of IGlar‐U300 might have corrected for (the known) lower potency, this would have been difficult in a double‐blind design. In addition, there is no dose‐conversion factor that would be applicable between IDeg and IGlar‐U300 in all patients, and the IGlar‐U300 Summary of Product Characteristics prescribing information recommends a 1‐on‐1 unit conversion from once‐daily basal insulins.11, 14 We also considered the use of individualized doses but this would have required a long titration period, which would have considerably added to the burden for participants.
The impact of the lower potency of IGlar‐U300 leading to BG deviations from target in some clamps (and thereby neglecting the basic principle of keeping BG constant for a glucose clamp) on the outcomes of the study, in particular on day‐to‐day variability as the primary endpoint, is minor. A sensitivity analysis excluding all participants with low GIR confirmed the main result, ie, a 4‐fold lower day‐to‐day variability (based on variances) with IDeg compared with IGlar‐U300 at steady‐state. Similar results were observed when all randomized participants were included in the analysis (Figure S1, Supporting Information). Expressed as CV, which was used in previous studies,5 day‐to‐day variability was 33% for IDeg and 67% for IGlar‐U300. Both, the variance ratio and CV are estimates of pharmacodynamic variability; however, we have used the former as the prespecified primary endpoint in this study as the variances do not need any further transformation.
Because of longer duration of action, we can expect IGlar‐U300 to have lower day‐to‐day variability compared with IGlar‐U100. Nevertheless, because of its mechanism of protraction (ie, the formation of microprecipitates) IGlar has the inherent predisposition to pharmacodynamic variability.2, 3 Microscopic precipitation studies have shown that higher concentrations of IGlar correspondingly lead to the formation of larger heterogeneous microprecipitates, which might lead to an uneven and lower, but potentially more variable, rate of absorption (release of insulin monomers into the circulation)8, 9; therefore, one could speculate that IDeg shows lower day‐to‐day variability than both IGlar‐U100 and ‐U300 because of the formation of multi‐hexamers after s.c. injection that steadily dissociate monomers in circulation.3 Indeed, when participants were switched from IGlar‐U300 to IDeg, 25 of 29 participants (86%) showed an improvement in day‐to‐day variability. By contrast, 20 of 28 participants (71%) experienced worsening in day‐to‐day variability after switching from IDeg to IGlar‐U300 (Figure 4).
Furthermore, day‐to‐day variability assessed in 2‐hour intervals remained low and stable over 24 hours, allowing a flexible dosing schedule. Whereas, after a dose at 8:00 pm, the highest day‐to‐day variability with IGlar‐U300 was observed approximately between 4:00 am and 12:00 pm, corresponding to intervals between 8 and 16 hours after dosing (Figure 5). During these intervals, the low (Figure 2D) and highly variable glucose‐lowering effect of IGlar‐U300 might make it difficult, at least for some patients, to maintain good glycaemic control.
Pharmacodynamic variability is usually investigated with the euglycaemic clamp technique which is widely recognised as the “gold standard” for pharmacokinetic and pharmacodynamic analyses.16 We used a complete crossover study design to minimize the influence of confounding factors such as inter‐patient variability and individual differences in insulin sensitivity. We also precluded any potential residual effects of endogenous insulin secretion by performing the study in patients with T1D, who were selected using stringent inclusion criteria to represent a homogeneous population required for clamp studies. Most importantly, we tried to achieve very high clamp quality by using a modern automated device (ClampArt) that attains highly reliable outcomes by measuring BG continuously while GIR is adapted every minute.16 In general, sufficient clamp quality is confirmed when BG fluctuations during the clamp, that is, precision, expressed as CV, is <5% and the mean deviation, that is, control deviation, is low.17 Indeed, both precision as well as control deviation were low in the present study, indicating excellent clamp quality in either treatment arm (Table S2, Supporting Information). The observed deviations in BG after IGlar‐U300 treatment are therefore due to the variability in the insulin effect rather than induced by low clamp quality. In addition to the high clamp quality and study design, the major strength of the present study is that the pharmacodynamic assessments were based on 3 clamps for each participant in both treatment groups (~171 clamps per treatment), indicating that the reported estimates are robust.
Another challenge in glucose clamps, in particular when performed under steady‐state conditions, is the stabilization of BG at the clamp target level pre‐dosing using glucose or insulin infusions. In order to exclude any potential bias through these pre‐dosing procedures AUCGIR,2‐24h,SS, in addition to AUCGIR,τ,SS, covering 0 to 24 hours was calculated.5 There was no substantial difference in the treatment ratios between AUCGIR,2‐24h,SS and AUCGIR,τ,SS, indicating that the variability assessments were representative of the entire dosing period (Figure S1, Supporting Information).
The main limitation is the difficulty in translating clamp results into clinical findings. Lower day‐to‐day and within‐day variability should facilitate titration and thereby the achievement of glycaemic targets with a low risk of hypoglycaemia. In this context, it is reassuring that IDeg previously showed lower pharmacodynamic variability than IGlar‐U1005 and lower rates of overall, nocturnal and severe BG confirmed symptomatic hypoglycaemia at similar levels of glycaemic control in a double‐blind clinical trial in people with T1D.18 Similar findings have been reported in patients with T2D as well19; however, head‐to‐head clinical studies comparing IDeg and IGlar‐U300 are warranted to determine the clinical relevance of the findings from this study.
In conclusion, IDeg has lower day‐to‐day and relative within‐day variability in glucose‐lowering effect compared to IGlar‐U300 in people with T1D. Day‐to‐day variability in glucose‐lowering effects remained low and stable for IDeg across 24 hours, while that with IGlar‐U300 increased steadily after 6 to 8 hours and peaked 12 to 14 hours after dosing. The potency of IGlar‐U300 was 30% lower than that of IDeg. Furthermore, the distribution of glucose‐lowering effect was stable and predictable with IDeg across 1 dosing interval, while IGlar‐U300 had reduced activity approximately 6 to 18 hours after dosing. These results imply that patients treated with IDeg could potentially achieve lower glycaemic targets with a reduced risk of hypoglycaemia in comparison to IGlar‐U300.
Supporting information
Figure S1. Variability in pharmacodynamic response.
Figure S2. Patient specific day‐to‐day variability in AUCGIR ,τ, SS ‐ scatter plot of individual variances.
Table S1. Demographic and baseline characteristics.
Table S2. Glucose clamp quality assessments from unsmoothed blood glucose profiles.
ACKNOWLEDGEMENTS
The authors would like to thank Charlotte Thim Hansen, MD, and Michiel C.E. Van Leeuwen, MD, from Novo Nordisk A/S for scientific reviews and Ruchita Kapoor, PhD, Novo Nordisk A/S, for medical writing support.
Conflict of interest
T. H. is shareholder of Profil, which received research funds from Adocia, AstraZeneca, Becton‐Dickinson, Biocon, Boehringer Ingelheim, Dance Biopharm, Eli Lilly, Grünenthal, Gulf Pharmaceutical Industries, Johnson & Johnson, Marvel, MedImmune, Medtronic, Novartis, Novo Nordisk, Roche Diagnostics, Sanofi, Senseonics and Zealand Pharma. In addition, he is a member of advisory panels for Novo Nordisk and received speaker honoraria and travel grants from Eli Lilly, Mylan and Novo Nordisk. M. N. is an employee at Novo Nordisk A/S. H. H. and K. K. are employees and shareholders of Novo Nordisk A/S. L. N. and S. F. have no conflicts of interest to declare.
Author contributions
T. H. contributed to the study design, conduct/data collection, analysis and writing of the manuscript. L. N. contributed to the study conduct/data collection and writing of the manuscript. M. N. and S.F. contributed to the study design, conduct/data collection and writing of the manuscript. K. K. contributed to the data analysis and writing of the manuscript. H. H. contributed to the study design and writing of the manuscript.
Heise T, Nørskov M, Nosek L, Kaplan K, Famulla S and Haahr HL. Insulin degludec: Lower day‐to‐day and within‐day variability in pharmacodynamic response compared with insulin glargine 300 U/mL in type 1 diabetes. Diabetes Obes Metab. 2017;19:1032–1039. https://doi.org/10.1111/dom.12938
Funding Information This study was sponsored by Novo Nordisk A/S.
REFERENCES
- 1. Rossetti P, Ampudia‐Blasco FJ, Ascaso JF. Old and new basal insulin formulations: understanding pharmacodynamics is still relevant in clinical practice. Diabetes Obes Metab. 2014;16:695‐706. [DOI] [PubMed] [Google Scholar]
- 2. Heise T, Mathieu C. Impact of the mode of protraction of basal insulin therapies on their pharmacokinetic and pharmacodynamic properties and resulting clinical outcomes. Diabetes Obes Metab. 2017;19(1):3‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Haahr H, Heise T. A review of the pharmacological properties of insulin degludec and their clinical relevance. Clin Pharmacokinet. 2014;53(9):787‐800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Heise T, Nosek L, Rønn BB, et al. Lower within‐subject variability of insulin detemir in comparison to NPH insulin and insulin glargine in people with type 1 diabetes. Diabetes. 2004;53:1614‐1620. [DOI] [PubMed] [Google Scholar]
- 5. Heise T, Hermanski L, Nosek L, Feldman A, Rasmussen S, Haahr H. Insulin degludec: four times lower pharmacodynamic variability than insulin glargine under steady‐state conditions in type 1 diabetes. Diabetes Obes Metab. 2012;14(9):859‐864. [DOI] [PubMed] [Google Scholar]
- 6. Heise T, Hövelmann U, Nosek L, Hermanski L, Bøttcher SG, Haahr H. Comparison of the pharmacokinetic and pharmacodynamic profiles of insulin degludec and insulin glargine. Expert Opin Drug Metab Toxicol. 2015;11(8):1193‐1201. [DOI] [PubMed] [Google Scholar]
- 7. Becker RH, Dahmen R, Bergmann K, Lehmann A, Jax T, Heise T. New insulin glargine 300 units · mL‐1 provides a more even activity profile and prolonged glycemic control at steady state compared with insulin glargine 100 Units · mL‐1. Diabetes Care. 2015;38(4):637‐643. [DOI] [PubMed] [Google Scholar]
- 8. Seested T, Burgess A, Pyke C, Nishimura E. Ultrastructural 3D visualization of insulin degludec multihexamers upon subcutaneous injection in pig. Diabetes. 2016;65(suppl 1):A236(Poster 918‐P). [Google Scholar]
- 9. Becker R, Hahn A, Boderke P, et al. Long‐acting formulations of insulins. European Patent Office. 2011. https://data.epo.org/publication‐server/rest/v1.0/publication‐dates/20111123/patents/EP2387989NWA2/document.pdf . Accessed December 13, 2016.
- 10. Seaquist ER, Anderson J, Childs B, et al. Hypoglycemia and diabetes: a report of a workgroup of the American Diabetes Association and the Endocrine Society. Diabetes Care. 2013;36(5):1384‐1395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Food and Drug Administration . Toujeo® SoloSTAR® (Insulin glargine recombinant) 300 units/ml. U.S. Label information, 25 February 2015. http://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=206538 . Accessed December 13, 2016.
- 12. Bolli GB, Perriello G, Fanelli CG, De Feo P. Nocturnal blood glucose control in type I diabetes mellitus. Diabetes Care. 1993;16(suppl 3):71‐89. [DOI] [PubMed] [Google Scholar]
- 13. Heise T, Nosek L, Bottcher SG, Hastrup H, Haahr H. Ultra‐long‐acting insulin degludec has a flat and stable glucose‐lowering effect in type 2 diabetes. Diabetes Obes Metab. 2012;14(10):944‐950. [DOI] [PubMed] [Google Scholar]
- 14. Toujeo® 300 units/ml solution for injection in a pre‐filled pen. EU Summary of Product Characteristics (SmPC), 17 February 2015. http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_‐_Product_Information/human/000309/WC500047935.pdf . Accessed December 13, 2016.
- 15. Porcellati F, Bolli GB, Fanelli CG. Pharmacokinetics and pharmacodynamics of basal insulins. Diabetes Technol Ther. 2011;13(suppl 1):S15‐S24. [DOI] [PubMed] [Google Scholar]
- 16. Heise T, Zijlstra E, Nosek L, Heckermann S, Plum‐Mörschel L, Forst T. Euglycaemic glucose clamp: what it can and cannot do, and how to do it. Diabetes Obes Metab. 2016;18(10):962‐972. [DOI] [PubMed] [Google Scholar]
- 17. Benesch C, Heise T, Klein O, Heinemann L, Arnolds S. How to assess the quality of glucose clamps? Evaluation of clamps performed with ClampArt, a novel automated clamp device. J Diabetes Sci Technol. 2015;9(4):792‐800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Lane WS, Bailey TS, Gerety G, et al. Switch 1: reduced hypoglycemia with insulin degludec (IDeg) vs insulin glargine (IGlar) in patients with T1D at high risk of hypoglycemia: a randomized, double‐blind, crossover trial. Diabetes. 2016;65(suppl 1A):87‐LB. [Google Scholar]
- 19. Wysham C, Bhargava A, Chaykin L, et al. SWITCH 2: reduced hypoglycemia with insulin degludec (IDeg) versus insulin glargine (IGlar), both U100, in patients with T2D at high risk of hypoglycemia: a randomized, double‐blind, crossover trial. Diabetes. 2016;65(suppl 1A):90‐LB. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. Variability in pharmacodynamic response.
Figure S2. Patient specific day‐to‐day variability in AUCGIR ,τ, SS ‐ scatter plot of individual variances.
Table S1. Demographic and baseline characteristics.
Table S2. Glucose clamp quality assessments from unsmoothed blood glucose profiles.