

Abstract
Objectives
Marijuana use rates peak during emerging adulthood (ages 18 to 25 years). Although marijuana use quantity reliably predicts substance-related problems, considerable individual differences characterize this association. The aims of the present study were to examine the influence of community disadvantage in amplifying the effects of marijuana use on downstream substance use problems, as well as the mediating influence of social disengagement in the path linking marijuana use frequency to related problems.
Method
We conducted a 3-year longitudinal study with 505 Black men from rural communities in Georgia, age 20.3 years at baseline. Three waves of data were collected at 18-month intervals in participants’ homes or convenient community settings. Men completed audio computer-assisted self-interviews concerning their substance use, engagement in conventional roles and relationships, community characteristics, and substance use problems.
Results
Community disadvantage moderated the association of marijuana use with changes in substance use problems across time. In disadvantaged communities, a robust effect emerged between marijuana use frequency and related problems, whereas in less disadvantaged communities, marijuana use quantity and problems were not significantly associated. Increases in social disengagement mediated the influence of marijuana use on substance use problems in the context of community disadvantage.
Conclusions
For young Black men, residence in a disadvantaged neighborhood appears to amplify the impact of marijuana use on substance use problems. This effect appears to be a consequence of increases in social disengagement.
Keywords: African American/Black, men, marijuana use, marijuana consequences, community disadvantage
1. Introduction
Marijuana is the most commonly used illicit drug in the United States, with the percentage of Americans who reported using it more than doubling between 2001 and 2013. Young adults are at highest risk for marijuana use and abuse (Hasin et al., 2015; Substance Abuse and Mental Health Services Administration, 2014). More than 1 in 5 young people ages 18 to 25 years report using marijuana during the past month, and approximately 7.5% meet criteria for a marijuana use disorder. Although many young people use marijuana, considerable heterogeneity exists in the consequences of use. The majority of emerging adult users, even heavy users, do not develop serious substance-related problems (Haberstick et al., 2014). Individual differences in the link between frequency of use and substance-related consequences, however, are poorly understood.
The reasons why some young people do not “mature” out of substance use and the mechanisms that underlie the escalation in problem use are unclear. Extant research typically implicates early onset of use (Windle & Windle, 2012) and current dose in forecasting the development of substance abuse problems. These factors have limited predictive utility, however. A number of studies indicate that some young people experience a pattern of heightened substance use consequences that includes a relatively rapid progression from recreational use to the experience of substance use problems despite a delayed onset of use (Chen & Jacobson, 2012). Studies of dose generally indicate that risk of dependence increases with frequency of cannabis use; however, there is considerable variability in the likelihood that even heavy users will become dependent. For example, recent research indicates that between 20% to 50% of heavy users will develop dependence (Lopez-Quintero et al., 2011; Wagner & Anthony, 2002).
Considerable research links residence in disadvantaged communities to substance use and related problems, particularly among youth (Brooks, Magnusson, Spencer, & Morgan, 2012; Clark, Nguyen, & Belgrave, 2011). Most of these studies, however, were designed to document community disadvantage as a risk factor for substance use. We are aware of no prior research that has investigated the potential for challenging communities to amplify the negative consequences of marijuana use. This distinction is critical because, among many emerging adults, substance use is viewed as normative (Stone, Becker, Huber, & Catalano, 2012), a part of a developmental phase that the majority of young people will “outgrow” (Bachman, Wadsworth, O’Malley, Johnston, & Schulenberg, 2009).
The concept of community disadvantage has been used to characterize neighborhood environments with few economic resources, structural dilapidation, and high crime rates. Residence in disadvantaged communities is more stressful than in better resourced ones. Studies reveal that disadvantaged environments take a toll on health in general and increase vulnerability to substance use in particular (Jang & Johnson, 2001; Latkin, Curry, Hua, & Davey, 2007). Experimental studies with animals underscore the importance of common environmental stressors, such as lack of resources, interindividual conflict, and social defeat, in amplifying the progression from first use to addiction (Bardo, Neisewander, & Kelly, 2013).
The potential for stressful environments to amplify the negative consequences of marijuana use among young people has not been studied. Social bonding and development perspectives offer insights into the reasons why disadvantaged community environments may amplify the influence of marijuana use. These perspectives emphasize the role of conventional social bonds in substance use escalation and desistance among young adults (Bachman et al., 2012). Social bonds include prosocial commitments to significant others such as parents and peers, involvement in and commitment to conventional roles such as work or school, and involvement in religious or civil institutions. These bonds reinforce conventional value systems and norms that deter antisocial behavior in general and drug use in particular (Sampson & Laub, 1990; White & Jackson, 2004/2005). Conversely, young people who are marginalized from educational and occupational systems and have few close relationships with conventional peers or family members experience few reinforcements for abstinence or moderate use. These young adults typically affiliate with substance-using peers who reinforce use.
We use the term social disengagement to refer to the status of young people who form relatively few conventional bonds. Our approach to assessing social disengagement is based on cumulative models of contextual influences on substance use. Empirical and theoretical research indicates that the numbers of social bonds that young people form have the most robust influence on their abuse of substances. In contrast, investigations of individual bonds are generally less consistent and have less predictive power (Jessor, Van Den Bos, Vanderryn, Costa, & Turbin, 2016; Whitson, Bernard, & Kaufman, 2013). It thus appears that, for many youth, it is the extent to which one lacks bonds across multiple situations that has the most profound influence on substance abuse behavior.
We hypothesize that, for young men living in disadvantaged communities, marijuana use has an elevated potential to lead to substance use problems and that social disengagement mediates this association. Studies suggest that marijuana use undermines consistent employment or educational pursuits, economic stability (Aseltine & Gore, 2000, 2005), and the maintenance of supportive relationships with family, peers, and romantic partners (Lander, Howsare, & Byrne, 2013). In the context of low-resource communities, these effects are expected to be heightened as young people have fewer “safety nets” in family and community systems to support the maintenance of positive developmental trajectories (Swartz, Kim, Uno, Mortimer, & O’Brien, 2011). Studies also suggest that, in low-resource communities, young adult marijuana use is viewed with greater concern than is evident in well-resourced communities because it is more likely to be associated with a high-risk lifestyle and affiliation with antisocial peers (Gibson, Perley, Bailey, Barbour, & Kershaw, 2015; Mawson, Best, Beckwith, Dingle, & Lubman, 2015). Thus, in the context of disadvantaged communities, conventional peers and adults are likely to withdraw from users, increasing the users’ alienation from sources of support associated with the diminution of substance use and related consequences among young adults (Bachman et al., 2012; Martin, Blozis, Boeninger, Masarik, & Conger, 2014).
The study hypotheses are summarized in Figure 1. We expected that marijuana use would forecast increases in substance use-related problems such as legal, vocational, health, and interpersonal difficulties directly associated with substance use or linked with the aftereffects of use. We also hypothesized that this influence of marijuana use on substance use problems would be moderated by exposure to community disadvantage (Figure 1a), such that environmental disadvantage would be associated positively with substance use-related problems. We further expected (Figure 1b) interaction of community disadvantage and substance use to predict increases in substance use problems indirectly, via effects on changes in social disengagement. Because binge drinking was also common in our sample, we controlled for its influence on substance use-related problems to provide a more rigorous test of the influence of marijuana per se. Participants rarely reported use of drugs other than marijuana and alcohol.
Fig. 1.
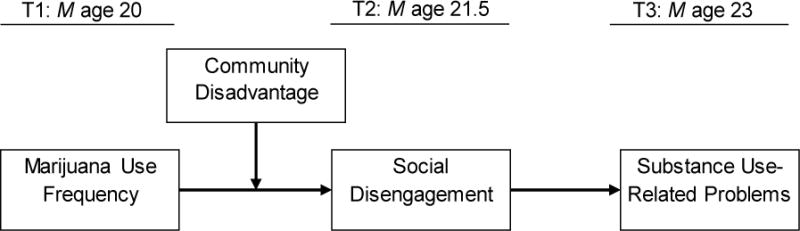
Conceptual model: Social disengagement, defined as low engagement with work or school, family, and community mentors, and high affiliation with substance-using peers, will mediate the interaction effects of marijuana use and community disadvantage on substance use-related problems.
We investigated the pathways linking marijuana use to the development of substance use problems using three waves of data from a sample of young Black men (mean ages 20, 21.5, and 23 years at data collection) living in rural communities. Focusing on this population of men brings a number of novel elements to this study. Epidemiological data indicate that many young Black men are disproportionately likely to live in challenging environments and, despite a later onset of use, experience heightened negative consequences. It is thus an ideal sample with which to examine hypotheses regarding contextual factors that amplify and sustain the influence of substance use, given variability in the numbers of men who delay onset of use and evince a telescoping of marijuana use consequences. Moreover, despite evidence that young Black men may experience heightened substance use consequences (Zapolski, Pedersen, McCarthy, & Smith, 2014), little prospective research has examined the factors associated with such consequences in this population. Thus, the results will have heuristic value for understanding substance use amplification and continuity processes in general, as well as providing ecologically relevant information with which future intervention programs for this population can be developed.
2. Method
2.1. Participants
Participants included 505 African American men who resided in one of 11 rural counties in South Georgia, an area representative of a geographic concentration of rural poverty across the southern coastal plain (Crockett, Carlo, & Temmen, 2016). Men were 19 to 22 years of age (M = 20.26; SD = 1.08) at the baseline interview (Time 1; T1). Participants were recruited using respondent-driven sampling (RDS), which combines a prescribed chain-referral recruitment method with a mathematical model that allows for post-stratification sample weighting. Community liaisons recruited 45 initial seed participants from targeted counties to complete a baseline survey. Each participant was then asked to identify three other men in his community from his personal network who met the criteria for inclusion in the study (Black, age 19–22, and living in the targeted area). Project staff contacted the referred potential participants, and the referring participant received $25 per person who completed the survey. After completing the survey, each referred participant, in turn, was asked to refer three men in his network. The RDS protocols and weighting system are designed to attenuate the influence of biases common in chain-referral samples and to improve approximation of a random sample of the target population (Heckathorn, 1997, 2002). Analyses of network data related to substance use and other risky behavior at T1 (Kogan et al., 2016) indicated that the sample evinced negligible levels of common biases observed in chain-referral samples arising from the characteristics of the initial seed participants, the recruitment efficacy of individual participants, and differences in the sizes of participants’ networks.
2.2. Data collection procedures and retention
Black research staff visited participants in the participants’ homes or at convenient community locations, where participants completed an audio computer-assisted self-interview on a laptop computer. This allowed participants to navigate the survey privately with the help of voice and video enhancements, eliminating literacy concerns. Approximately 18.30 (SD = 4.19) months after the baseline survey, when men’s mean age was 21.85 years (SD = 1.27), a follow-up data collection visit (Time 2; T2) was conducted in the same manner. A third visit (Time 3; T3) occurred 19.68 months after T2; men’s mean age at T3 was 23.12 (SD = 1.26). Of the 505 men who participated at T1, 423 (84%) completed the T2 survey and 409 (81%) completed the T3 survey. Retention status was not associated with any study variables. Participants received $100 at each time point for completing the surveys. Participants provided written informed consent at baseline, and all study protocols were approved by the Institutional Review Board of the university at which the study was conducted.
2.3. Measures
2.3.1. Marijuana use frequency
Men reported the average numbers of days per month on which they used marijuana. Test-retest reliability for past-month recall of marijuana use is typically high, with kappas exceeding .70 (Brener et al., 2002; Ramo, Liu, & Prochaska, 2012).
2.3.2. Substance use-related problems
At T1 and T3, men reported their substance use-related problems on a 9-item scale. Items indexed the frequency during the past 6 months with which the use of “alcohol or drugs” led to a range of difficulties that included problems with family, missing work, driving vehicles while intoxicated, and substance-related legal problems. Possible responses were 0 (0 days), 1 (1 day), 2 (2 days), 3 (3 days), 4 (4–6 days), 5 (7–10 days), and 6 (11 or more days). Cronbach’s alphas were .86 at T1 and .92 at T2.
2.3.3. Social disengagement
Consistent with past research that suggests the number of social bonds has a more robust influence on substance use than any particular role or relationships (Sullivan & Farrell, 1999), we developed a social disengagement index to evaluate the numbers of bonds present. Social disengagement was assessed at T1 and T2 with single items and multi-item scales that indexed a total of seven variables. Scores on multi-item inventories were dichotomized based on a median split (0 = low disengagement, 1 = high disengagement). All dichotomous indicators of disengagement were summed to form indices ranging from 0 to 7. Indivdiual items included student or employment status (0 = yes, 1 = no), number of residential moves in the past 6 months (0 = no moves, 1 = 1 or more moves) and relationship with a supportive older mentor figure in the community (0 = yes, 1 = no). Men reported their vocational engagement on a 10-item scale that Gore, Aseltine, and Schilling (2007) developed. Example items incuded, “I have trouble keeping jobs” (reverse coded) and “I am a dependable employee.” The response scale ranged from 1 (strongly disagree) to 4 (strongly agree). Cronbach’s alphas were .80 at T1 and .82 at T2. Men reported the frequency of contact with their primary caregivers using two items referring to telephone conversations and in-person visits (0 = never, 1 = a few times per year, 2 = a few times per month, 3 = a few times per week, 4 = everyday). These items were significantly correlated and averaged to form a contact frequency index. Men reported the proportions of their close friends who engaged in antisocial behaviors (stealing, fighting) and substance use (drug use, alcohol use) on an 11-item scale with a response set ranging from 0 (none of them) to 4 (most of them). Cronbach’s alphas were .90 at T1 and .92 at T2. Religious involvement was assessed with an 8-item measure (Levin, Taylor, & Chatters, 1995) assessing subjective religiosity and participation in formal and informal religious practices. Example items included, “How often do you usually attend religious services?” “How often do you pray?” and “How religious would you say you are?” Cronbach’s alphas exceeded .73.
2.3.4. Community disadvantage
Community disadvantaged was assessed at T1 and T2 with the Community Problems measure (Forehand et al., 2000). Participants were asked, “How much of a problem does your community have in terms of…”, followed by 18 items indicative of community problems (e.g., no place to get jobs, no place to get a college education, vacant and run-down buildings, trash and abandoned cars). These were rated on a scale ranging from 1 (not a problem in my community) to 3 (a big problem in my community). Cronbach’s alphas were .91 at T1 and .92 at T2. To take into account the clustered nature of the community disadvantage variable, the community disadvantage scores of men living in the same census tract were averaged. Participants’ residential addresses at T1 and T2 were geocoded and matched to census tracts. At T1, 63 tracts were identified; 58 tracts were identified at T2. Among the participants, 76.0% reported the same census tract at both T1 and T2. To capture the community context across the 18 months separating T1 and T2, we summed the two scores of community disadvantage based on the census tracts to form the community disadvantage indicator.
2.3.5. Demographic and binge drinking covariates
Age at baseline was assessed as a continuous variable. Men reported the number of days during the past month on which they engaged in binge drinking (four or more drinks at one sitting).
2.4. Plan of Analysis
Hypotheses were tested with path analyses using the maximum likelihood estimator as implemented in Mplus 7.13 (Muthén & Muthén, 1998–2015). Parameters were estimated and missing data were managed with full information likelihood estimation (FIML). The FIML estimator tests hypotheses with all available data; no cases are dropped. Age and binge drinking were controlled in all analyses. Because participants were clustered within census tracts, the complex analysis feature was used to adjust parameter standard errors for interdependence in the data.
First, we tested the moderating influence of community disadvantage on the link between marijuana use and substance use problems using a multigroup analysis. This involved comparing groups based on a median split of the community disadvantage measure; a significant difference between groups on chi-square values for the parameter linking quantity to problems indicates a moderation effect. Second, we examined the conditional indirect effect of marijuana use on substance use problems via social disengagement using multigroup procedures and tested for the significance of indirect effects using bootstrapping.
3. Results
Table 1 presents descriptive information on all study variables. At T1, 46.7% of the participants reported marijuana use at least once per month; their mean number of reported substance use-related problems was 3.82 (SD = 7.23). Table 2 presents the correlations among the study variables we used to test our hypotheses.
Table 1.
Descriptive results among study variables.
| Study variables | M (SD) | N (%) |
|---|---|---|
| Age, T1 | 20.26 (1.08) | |
| Binge drinking, T1 | 1.63 (3.10) | |
| Marijuana use, T1 | 8.44 (12.13) | |
| Social disengagement, T1 | 2.90 (1.43) | |
| Not employed or pursuing higher education | 145 (28.7) | |
| 1 or more residential moves in the past 6 months | 188 (37.2) | |
| Absence of a supportive older mentor figure | 265 (52.7) | |
| Affiliation with friends engaging in antisocial behaviors | 0.65 (0.52) | |
| Frequency of contact with primary caregivers | 3.38 (0.81) | |
| Vocational engagement | 3.42 (0.40) | |
| Religious involvement | 0.00 (4.38) | |
| Social disengagement, T2 | 3.09 (1.43) | |
| Not employed or pursuing higher education | 122 (28.8) | |
| 1 or more residential moves in the past 6 months | 145 (34.3) | |
| Absence of a supportive older mentor figure | 267 (63.1) | |
| Affiliation with friends engaging in antisocial behaviors | 0.64 (0.55) | |
| Frequency of contact with primary caregivers | 3.21 (0.82) | |
| Vocational engagement | 3.41 (0.44) | |
| Religious involvement | 0.00 (4.35) | |
| Substance use-related problems, T1 | 3.82 (7.23) | |
| Substance use-related problems, T3 | 3.35 (8.10) | |
| Community disadvantage, T1 and T2 | 1.91 (0.16) | |
| Community disadvantage, T1 | 1.94 (0.18) | |
| Community disadvantage, T2 | 1.86 (0.20) |
Table 2.
Correlations, means, and standard deviations among study variables.
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age, T1 | – | .12** | .11* | .14** | .07 | .15** | .06 | .02 | .02 | .01 |
| 2. Binge drinking, T1 | – | .10* | .01 | .03 | .28** | .20** | .04 | .09* | −.01 | |
| 3. Marijuana use, T1 | – | .26** | .19** | .49** | .18** | .08 | .03 | .09 | ||
| 4. Social disengagement, T1 | – | .44** | .17** | .11* | .02 | .01 | .08 | |||
| 5. Social disengagement, T2 | – | .07 | .20** | .01 | .02 | .05 | ||||
| 6. Substance use-related problems, T1 | – | .26** | .08 | .08 | .05 | |||||
| 7. Substance use-related problems, T3 | – | .11* | .04 | .14** | ||||||
| 8. Community disadvantage, T1 & T2 | – | .80** | .80** | |||||||
| 9. Community disadvantage, T1 | – | .23** | ||||||||
| 10. Community disadvantage, T2 | – |
Note. Participants’ mean ages were 20 years at T1, 21.5 years at T2, and 23 years at T3.
p < .05;
p < .01.
Figure 2 presents the results of the multigroup model testing the hypothesis that community disadvantage would moderate the link between marijuana use frequency at T1 and substance use problems at T3. Results from the single-group model indicated that the number of days on which marijuana was used at T1 did not forecast changes in substance-related problems at T3. In the multigroup model, however, change in chi-square indicated significant moderation by community disadvantage, Δχ2/df = 4.16, p < .05. In the context of high levels of community disadvantage, marijuana use was associated significantly with increases in substance use-related problems across the 3 years separating T1 and T3, β = .13, 95% CI = [.025, .272].
Fig. 2.
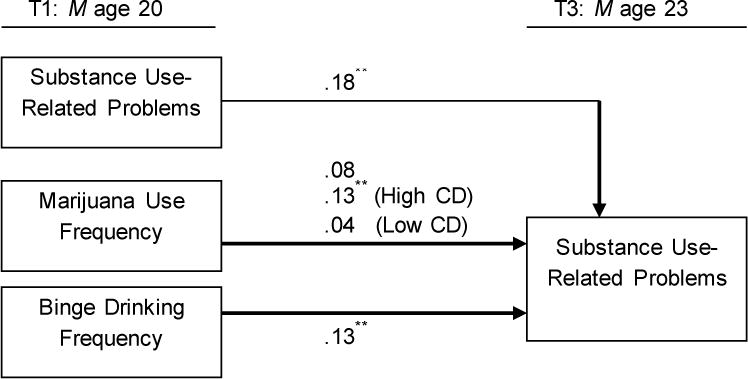
Multigroup analysis of the influence of marijuana use frequency on substance use-related problems.
Note. χ2 = 2.29, df = 3, p = .73. RMSEA = .01. CFI = .99. Standardized coefficients are shown. Participant age was controlled. CD = Community disadvantage at T1 and T2.
*p < .05. **p < .01.
The test of the unconditioned and conditional indirect effect of disengagement is presented in Figure 3. For ease of presentation, baseline controls for social disengagement and substance use problems are not pictured. Results indicate that, for the sample as a whole, marijuana use influenced substance use problems indirectly via increases in social disengagement, β = .11, 95% CI = [.039, .208]. The link between marijuana use and social disengagement was significantly different for high and low disadvantage groups, Δχ2/df = 6.86, p < .01. In the context of high community disadvantage, marijuana use predicted social disengagement, β = .18, 95% CI = [.069, .321], which in turn predicted substance use-related problems, β = .17, 95% CI = [.042, .305]. The conditional indirect effect linking marijuana use to substance use-related problems via social disengagement was significant in the context of elevated community disadvantage, β = .04, 95% CI = [.009, .106].
Fig. 3.
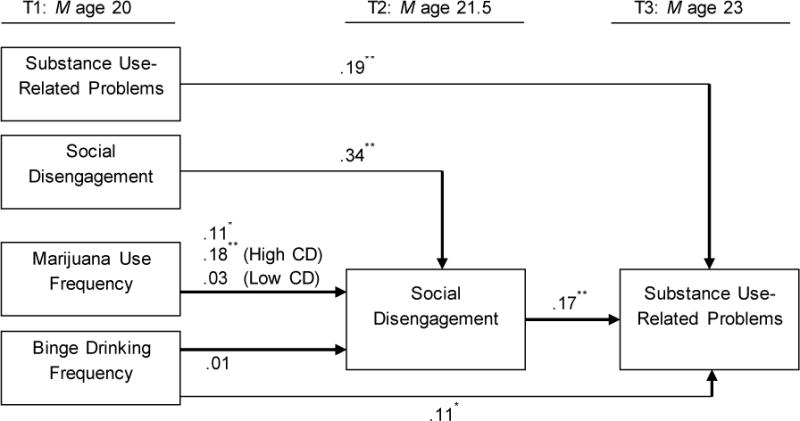
Results of multigroup analysis of the influence of marijuana use on substance use-related problems via effects on social disengagement.
Note. χ2 = .40, df = 3, p = .94. RMSEA = .00. CFI = 1.00. Standardized coefficients are shown. Participant age was controlled. CD = Community disadvantage at T1 and T2.
*p < .05. **p < .01.
4. Discussion
Many emerging adults use marijuana. Although the frequency of use is consistently associated with the consequences experienced, considerable individual differences exist in the strength of this association. Many emerging adults use marijuana with relatively few consequences, whereas others experience heightened substance-related problems and risk for substance use disorders (Johnston, O’Malley, Bachman, & Schulenberg, 2011). The psychosocial factors associated with these differences are poorly understood. We examined the link between marijuana use quantity at age 20 and the development of substance use-related problems at age 23 among a sample of young Black men living in rural communities. Our analysis revealed that, for these young men, (a) living in disadvantaged community environments amplified the influence of marijuana use on the development of substance-related problems, and (b) for young men living in disadvantaged communities, social disengagement mediated the influence of marijuana use on substance-related problems.
Drug use surveillance data and studies of clinical populations suggest that Black men coping with stressful low-SES environments experience disproportionate short- and long-term consequences from marijuana use during the emerging adult years (National Institute on Drug Abuse, 2003). Although Black men generally begin use at a later age than their White peers, studies suggest that Black men’s use confers heightened risk for both short- and long- term consequences associated with poor psychosocial adjustment and chronic drug use problems. Studies indicate that Black men in general, and those from low-SES backgrounds in particular, experience more negative consequences per ounce of alcohol or other drugs consumed than do men from other racial/SES groups (Jones-Webb, 1998; Wallace et al., 2002; Zapolski et al., 2014). These consequences include the likelihood that drug use will lead to accidents, injuries, interpersonal problems, legal problems, and economic difficulties (Gillmore, Catalano, Morrison, & Wells, 1990; Jones-Webb, 1998; Jones-Webb, Hsiao, & Hannan, 1995; Welte & Barnes, 1987).
Few studies have examined the reasons why drug use has outsized effects on low-SES Black men. The explanation most frequently offered for the disproportionate impact of drug use on vulnerable populations involves genetic factors related to alcohol and nicotine metabolism (Fukami et al., 2005; Radel & Goldman, 2001; Randall et al., 1999). Accumulating evidence, however, indicates that individual differences in metabolism do not account for the proliferation of drug use and related problems that emerging adult rural Black men experience. Drug use progression and its consequences are increasingly viewed as responses to exposure to stressful environments (Sinha, 2008; Wand, 2008). Studies with animal models, in which variability in biological vulnerabilities associated with metabolism are carefully minimized, underscore the role of environmental stressors such as early adversity, social defeat, subordination, and a lack of resources in accelerating the progression from onset to problem use (Bardo et al., 2013). Similarly, among adult drug users, social stress and economic resources predict patterns of drug use escalation and desistance as well as variability in rates of relapse and recovery after treatment (Goeders, 2003).
Our findings suggest that residence in stressful low-SES community environments may help to determine why some young men who use marijuana have difficulty maturing out of substance use. The emerging adult years are a time of instability and rapid change, when young people experience increased autonomy and learn to navigate their communities with reduced parental supervision and guidance. During this time, young people may make mistakes and experience crises in dealing with new freedoms, some of which are linked to drug use. For emerging adults from well-resourced environments, we conjecture that families provide assistance in managing the negative consequences of substance use. When drug use-related consequences occur, including mental health concerns, arrest for marijuana use or underage drinking, or school problems, parents facilitate access to treatment, legal resources, financial support, and additional opportunities to complete higher education. In contrast, for Black men from disadvantaged neighborhoods, such safety nets are scarce. Minor legal problems associated with drug use can lead to incarceration and expenses that severely tax the family system. Similarly, if recreational drug use affects a young Black man’s educational progress or ability to find and keep a job, the economic and social capital required to help him get back on track may not be available. In contexts with scarce resources, there is little room for error.
For young men in disadvantaged communities, our data suggest that marijuana use engenders negative consequences via its effect on social disengagement. The combination of marijuana use and disadvantaged community environments undermines men’s engagement in prosocial relationships with peers, family members, and community members, and their connections to conventional institutions such as church, school, and work. As men’s social disengagement increases, they report higher levels of substance use problems. Studies document social segregation processes that isolate drug-using young adults in resource-poor Black communities (Gibson et al., 2015; Mawson et al., 2015). These dynamics operate in part through selection mechanisms, because drug-using young men affiliate primarily with drug-using peers (Wade & Rochlen, 2013). Research also indicates that, in low-SES communities, when young men frequently use drugs, parents, extended family, and prosocial community members may react to them defensively to protect themselves from the potential for chaos that accompanies increasingly unstable lifestyles (Herd, 1994). As these ties weaken, men become estranged from their communities and isolated from social resources that could facilitate engagement in conventional social roles. These findings suggest that substance use intervention and treatment may be needed that focuses on re-integrating men into their communities and identifying conventional sources of socialization and support. In particular, regular employment is likely to be a key means of reducing affiliations with marijuana using-peers and providing reinforcement for abstinence (Zapolski et al., 2014).
4.1. Limitations
Limitations of the present study must be noted. We focused on young Black men in rural environments; findings may not generalize to men from other racial groups or geographic areas. Our measure of substance-related problems was not specific to problems that resulted from marijuana use. This limitation is mitigated by inclusion of binge drinking as a control variable in our models; thus, we were able to examine the unique contribution of marijuana use net of the effect of binge drinking, accounting for the influence of binge drinking on related problems. The substance use problem measure also had areas of overlap with social disengagement. The use of self-reports of community disadvantage would be usefully complemented by objective reports in future research. Finally, although the prospective design is a strength, studies that extend across emerging adulthood are needed to track the development of substance use-related problems and disorders across this developmental transition.
4.2. Future directions
Although in our study we did not investigate cross-group racial differences, the findings have heuristic value for future investigations of racial disparities in the consequences of substance use. Young Black men are disproportionately exposed to challenging community contexts (Hatch & Dohrenwend, 2007). Given evidence of substance use-problem amplification in these communities, disproportionate exposure to disadvantage may help to explain racial disparities in substance use outcomes. Future research with multiracial and multiethnic samples are needed to determine whether variability in community contexts mediates the association between racial or ethnic group and substance use consequences.
The present findings also have implications for intervention and prevention programs. First, findings confirm the importance of targeting prevention efforts to young men in disadvantaged neighborhoods and designing interventions that acknowledge the potential for modest levels of substance use to have disparate consequences among emerging adults. Second, the negative consequences of marijuana use may be related to social disengagement processes. This should be addressed from both individual and community perspectives. Young people who use marijuana are likely to need assistance in reconnecting to community support and obtaining employment. Community efforts to engage marijuana users and mitigate substance use stigma may facilitate this process.
Highlights.
Challenging communities amplify the negative impact of young men’s marijuana use.
Marijuana use increases social disengagement in challenging communities.
Marijuana use has reduced influence on young men in well-resourced communities.
Acknowledgments
We would like to thank Eileen Neubaum-Carlan, MS, for her editorial assistance.
Role of funding sources
Funding for this study was provided by NIDA Grants R01 DA029488 and P30 DA027827. NIDA had no role in the study design; the collection, analysis, or interpretation of the data; the writing of the manuscript; or the decision to submit the paper for publication.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributors
SK supervised the analyses and led the writing. JC conducted the analyses, and GB and SB contributed to the interpretation of the results and to the reviewing and editing of the article.
Conflict of interest
All authors declare that they have no conflicts of interest.
References
- Aseltine RH, Gore SL. The variable effects of stress on alcohol use from adolescence to early adulthood. Substance Use & Misuse. 2000;35:643–668. doi: 10.3109/10826080009148415. http://dx.doi.org/10.3109/10826080009148415. [DOI] [PubMed] [Google Scholar]
- Aseltine RH, Gore S. Work, postsecondary education, and psychosocial functioning following the transition from high school. Journal of Adolescent Research. 2005;20:615–639. http://dx.doi.org/10.1177/0743558405279360. [Google Scholar]
- Bachman JG, O’Malley PM, Schulenberg JE, Johnston LD, Bryant AL, Merline AC. The decline of substance use in young adulthood: Changes in social activities, roles, and beliefs. New York, NY: Psychology Press; 2012. [Google Scholar]
- Bachman JG, Wadsworth KN, O’Malley PM, Johnston LD, Schulenberg JE. Smoking, drinking, and drug use in young adulthood: The impacts of new freedoms and new responsibilities. New York, NY: Psychology Press; 2009. [Google Scholar]
- Bardo M, Neisewander J, Kelly T. Individual differences and social influences on the neurobehavioral pharmacology of abused drugs. Pharmacological Reviews. 2013;65:255–290. doi: 10.1124/pr.111.005124. http://dx.doi.org/10.1124/pr.111.005124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brener ND, Kann L, McManus T, Kinchen SA, Sundberg EC, Ross JG. Reliability of the 1999 Youth Risk Behavior Survey questionnaire. Journal of Adolescent Health. 2002;31:336–342. doi: 10.1016/s1054-139x(02)00339-7. http://dx.doi.org/10.1016/S1054-139X(02)00339-7. [DOI] [PubMed] [Google Scholar]
- Brooks FM, Magnusson J, Spencer N, Morgan A. Adolescent multiple risk behaviour: An asset approach to the role of family, school and community. Journal of Public Health. 2012;34(S1):i48–i56. doi: 10.1093/pubmed/fds001. http://dx.doi.org/10.1093/pubmed/fds001. [DOI] [PubMed] [Google Scholar]
- Chen P, Jacobson KC. Developmental trajectories of substance use from early adolescence to young adulthood: Gender and racial/ethnic differences. Journal of Adolescent Health. 2012;50:154–163. doi: 10.1016/j.jadohealth.2011.05.013. http://dx.doi.org/10.1016/j.jadohealth.2011.05.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark TT, Nguyen AB, Belgrave FZ. Risk and protective factors for alcohol and marijuana use among African-American rural and urban adolescents. Journal of Child & Adolescent Substance Abuse. 2011;20:205–220. doi: 10.1080/1067828X.2011.581898. http://dx.doi.org/10.1080/1067828X.2011.581898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crockett LJ, Carlo G, Temmen C. Ethnic and racial minority youth in the rural United States: An overview. In: Crockett LJ, Carlo G, editors. Rural ethnic minority youth and families in the United States. Cham, Switzerland: Springer International Publishing; 2016. pp. 1–12. http://dx.doi.org/10.1007/978-3-319-20976-0_1. [Google Scholar]
- Forehand R, Brody GH, Armistead L, Dorsey S, Morse E, Morse PS, Stock M. The role of community risks and resources in the psychosocial adjustment of at-risk children: An examination across two community contexts and two informants. Behavior Therapy. 2000;31:395–414. http://dx.doi.org/10.1016/S0005-7894(00)80022-2. [Google Scholar]
- Fukami T, Nakajima M, Higashi E, Yamanaka H, McLeod HL, Yokoi T. A novel CYP2A6*20 allele found in African-American population produces a truncated protein lacking enzymatic activity. Biochemical Pharmacology. 2005;70:801–808. doi: 10.1016/j.bcp.2005.05.029. http://dx.doi.org/10.1016/j.bcp.2005.05.029. [DOI] [PubMed] [Google Scholar]
- Gibson C, Perley L, Bailey J, Barbour R, Kershaw T. Social network and census tract-level influences on substance use among emerging adult males: An activity spaces approach. Health & Place. 2015;35:28–36. doi: 10.1016/j.healthplace.2015.06.004. http://dx.doi.org/10.1016/j.healthplace.2015.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gillmore MR, Catalano RF, Morrison DM, Wells EA, Iritani B, Hawkins JD. Racial differences in acceptability and availability of drugs and early initiation of substance use. American Journal of Drug & Alcohol Abuse. 1990;16:185–206. doi: 10.3109/00952999009001583. [DOI] [PubMed] [Google Scholar]
- Goeders NE. The impact of stress on addiction. European Neuropsychopharmacology. 2003;13:435–441. doi: 10.1016/j.euroneuro.2003.08.004. http://dx.doi.org/10.1016/j.euroneuro.2003.08.004. [DOI] [PubMed] [Google Scholar]
- Gore S, Aseltine RH, Jr, Schilling EA. Transition to adulthood, mental health, and inequality. In: Avison WR, McLeod JD, Pescosolido BA, editors. Mental health, social mirror. New York, NY: Springer Science+Business Media; 2007. pp. 219–237. http://dx.doi.org/10.1007/978-0-387-36320-2_10. [Google Scholar]
- Haberstick BC, Young SE, Zeiger JS, Lessem JM, Hewitt JK, Hopfer CJ. Prevalence and correlates of alcohol and cannabis use disorders in the United States: results from the national longitudinal study of adolescent health. Drug and Alcohol Dependence. 2014;136:158–161. doi: 10.1016/j.drugalcdep.2013.11.022. http://dx.doi.org/10.1016/j.drugalcdep.2013.11.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hasin DS, Saha TD, Kerridge BT, Goldstein RB, Chou SP, Zhang H, Smith SM. Prevalence of marijuana use disorders in the United States between 2001–2002 and 2012–2013. JAMA Psychiatry. 2015;72:1235–1242. doi: 10.1001/jamapsychiatry.2015.1858. http://dx.doi.org/10.1016/j.drugalcdep.2013.11.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hatch SL, Dohrenwend BP. Distribution of traumatic and other stressful life events by race/ethnicity, gender, SES and age: A review of the research. American Journal of Community Psychology. 2007;40:313–332. doi: 10.1007/s10464-007-9134-z. http://dx.doi.org/10.1007/s10464-007-9134-z. [DOI] [PubMed] [Google Scholar]
- Heckathorn DD. Respondent-driven sampling: A new approach to the study of hidden populations. Social Problems. 1997;44:174–199. http://dx.doi.org/10.1525/sp.1997.44.2.03x0221m. [Google Scholar]
- Heckathorn DD. Respondent-driven sampling II: Deriving valid population estimates from chain-referral samples of hidden populations. Social Problems. 2002;49:11–34. http://dx.doi.org/10.1525/sp.2002.49.1.11. [Google Scholar]
- Herd D. Predicting drinking problems among Black and White men: Results from a national survey. Journal of Studies on Alcohol. 1994;55:61–71. doi: 10.15288/jsa.1994.55.61. http://dx.doi.org/10.15288/jsa.1994.55.61. [DOI] [PubMed] [Google Scholar]
- Jang SJ, Johnson BR. Neighborhood disorder, individual religiosity, and adolescent use of illicit drugs: A test of multilevel hypotheses. Criminology. 2001;39:109–144. http://dx.doi.org/10.1111/j.1745-9125.2001.tb00918.x. [Google Scholar]
- Jessor R, Van Den Bos J, Vanderryn J, Costa FM, Turbin MS. Problem behavior theory and the dynamics of protection and risk. In: Jessor R, editor. The origins and development of problem behavior theory. Cham, Switzerland: Springer International Publishing; 2016. pp. 131–153. [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national survey results on drug use, 1975–2010. Volume II: College students and adults ages 19–50. Ann Arbor, MI: Institute for Social Research, University of Michigan; 2011. [Google Scholar]
- Jones-Webb R. Drinking patterns and problems among African-Americans: Recent findings. Alcohol Health & Research World. 1998;22:260–264. [PMC free article] [PubMed] [Google Scholar]
- Jones-Webb RJ, Hsiao CY, Hannan P. Relationships between socioeconomic status and drinking problems among Black and White men. Alcoholism: Clinical & Experimental Research. 1995;19:623–627. doi: 10.1111/j.1530-0277.1995.tb01558.x. [DOI] [PubMed] [Google Scholar]
- Kogan SM, Cho J, Barton AW, Duprey EB, Hicks MR, Brown GL. The influence of community disadvantage and masculinity ideology on number of sexual partners: A prospective analysis of young adult, rural Black men. Journal of Sex Research. 2016 Sep 15; doi: 10.1080/00224499.2016.1223798. Advance online publication. http://dx.doi.org/10.1080/00224499.2016.1223798. [DOI] [PMC free article] [PubMed]
- Lander L, Howsare J, Byrne M. The impact of substance use disorders on families and children: From theory to practice. Social Work in Public Health. 2013;28:194–205. doi: 10.1080/19371918.2013.759005. http://dx.doi.org/10.1080/19371918.2013.759005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Latkin CA, Curry AD, Hua W, Davey MA. Direct and indirect associations of neighborhood disorder with drug use and high-risk sexual partners. American Journal of Preventive Medicine. 2007;32:S234–S241. doi: 10.1016/j.amepre.2007.02.023. http://dx.doi.org/10.1016/j.amepre.2007.02.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levin JS, Taylor RJ, Chatters LM. A multidimensional measure of religious involvement for African Americans. Sociological Quarterly. 1995;36:157–173. Retrieved from http://www.jstor.org/stable/4121282. [Google Scholar]
- Lopez-Quintero C, de los Cobos JP, Hasin DS, Okuda M, Wang S, Grant BF, Blanco C. Probability and predictors of transition from first use to dependence on nicotine, alcohol, cannabis, and cocaine: Results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) Drug And Alcohol Dependence. 2011;115:120–130. doi: 10.1016/j.drugalcdep.2010.11.004. http://dx.doi.org/10.1016/j.drugalcdep.2010.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin MJ, Blozis SA, Boeninger DK, Masarik AS, Conger RD. The timing of entry into adult roles and changes in trajectories of problem behaviors during the transition to adulthood. Developmental Psychology. 2014;50:2473–2484. doi: 10.1037/a0037950. http://dx.doi.org/10.1037/a0037950. [DOI] [PubMed] [Google Scholar]
- Mawson E, Best D, Beckwith M, Dingle GA, Lubman DI. Social identity, social networks and recovery capital in emerging adulthood: A pilot study. Substance Abuse Treatment, Prevention, and Policy. 2015;10:1–11. doi: 10.1186/s13011-015-0041-2. http://dx.doi.org/10.1186/s13011-015-0041-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide. 7th. Los Angeles, CA: Muthén & Muthén; 1998–2015. [Google Scholar]
- National Institute on Drug Abuse. Drug use among racial/ethnic minorities, revised. Bethesda, MD: U.S. Department of Health and Human Services; 2003. (NIH Publication No. 03-3888). [Google Scholar]
- Radel M, Goldman D. Pharmacogenetics of alcohol response and alcoholism: The interplay of genes and environmental factors in thresholds for alcoholism. Drug Metabolism & Disposition. 2001;29(4 Pt 2):489–494. Retrieved from http://dmd.aspetjournals.org/content/29/4/489. [PubMed] [Google Scholar]
- Ramo DE, Liu H, Prochaska JJ. Reliability and validity of young adults’ anonymous online reports of marijuana use and thoughts about use. Psychology of Addictive Behaviors. 2012;26:801–811. doi: 10.1037/a0026201. http://dx.doi.org/10.1037/a0026201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Randall CL, Roberts JS, Boca FKD, Carroll KM, Connors GJ, Mattson ME. Telescoping of landmark events associated with drinking: A gender comparison. Journal of Studies on Alcohol. 1999;60:252–260. doi: 10.15288/jsa.1999.60.252. http://dx.doi.org/10.15288/jsa.1999.60.252. [DOI] [PubMed] [Google Scholar]
- Sampson RJ, Laub JH. Crime and deviance over the life course: The salience of adult social bonds. American Sociological Review. 1990;55:609–627. [Google Scholar]
- Sinha R. Chronic stress, drug use, and vulnerability to addiction. Annals of the New York Academy of Sciences. 2008;1141:105–130. doi: 10.1196/annals.1441.030. http://dx.doi.org/10.1196/annals.1441.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stone AL, Becker LG, Huber AM, Catalano RF. Review of risk and protective factors of substance use and problem use in emerging adulthood. Addictive Behaviors. 2012;37:747–775. doi: 10.1016/j.addbeh.2012.02.014. http://dx.doi.org/10.1016/j.addbeh.2012.02.014. [DOI] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration. Results from the 2013 National Survey on Drug Use and Health: Summary of national findings. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2014. (NSDUH Series H-48). [Google Scholar]
- Sullivan TN, Farrell AD. Identification and impact of risk and protective factors for drug use among urban African American adolescents. Journal of Clinical Child Psychology. 1999;28:122–136. doi: 10.1207/s15374424jccp2802_1. [DOI] [PubMed] [Google Scholar]
- Swartz TT, Kim M, Uno M, Mortimer J, O’Brien KB. Safety nets and scaffolds: Parental support in the transition to adulthood. Journal of Marriage and Family. 2011;73:414–429. doi: 10.1111/j.1741-3737.2010.00815.x. http://dx.doi.org/10.1111/j.1741-3737.2010.00815.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wade JC, Rochlen AB. Introduction: Masculinity, identity, and the health and well-being of African American men. Psychology of Men & Masculinity. 2013;14:1–6. http://dx.doi.org/10.1037/a0029612. [Google Scholar]
- Wagner FA, Anthony JC. From first drug use to drug dependence: Developmental periods of risk for dependence upon marijuana, cocaine, and alcohol. Neuropsychopharmacology. 2002;26:479–488. doi: 10.1016/S0893-133X(01)00367-0. http://dx.doi.org/10.1016/S0893-133X(01)00367-0. [DOI] [PubMed] [Google Scholar]
- Wallace JM, Jr, Bachman JG, O’Malley PM, Johnston LD, Schulenberg JE, Cooper SM. Tobacco, alcohol, and illicit drug use: Racial and ethnic differences among U.S. high school seniors, 1976–2000. Public Health Reports. 2002;117(Suppl 1):S67–S75. [PMC free article] [PubMed] [Google Scholar]
- Wand G. The influence of stress on the transition from drug use to addiction. Alcohol Research & Health. 2008;31:119–137. [PMC free article] [PubMed] [Google Scholar]
- Welte J, Barnes G. Alcohol use among adolescent minority groups. Journal of Studies on Alcohol. 1987;48:329–336. doi: 10.15288/jsa.1987.48.329. http://dx.doi.org/10.15288/jsa.1987.48.329. [DOI] [PubMed] [Google Scholar]
- White HR, Jackson K. Social and psychological influences on emerging adult drinking behavior. Alcohol Research & Health. 2004/2005;28:182–190. [Google Scholar]
- Whitson ML, Bernard S, Kaufman JS. The effects of cumulative risk and protection on problem behaviors for youth in an urban school-based system of care. Community Mental Health Journal. 2013;49:576–586. doi: 10.1007/s10597-012-9535-9. http://dx.doi.org/10.1007/s10597-012-9535-9. [DOI] [PubMed] [Google Scholar]
- Windle M, Windle RC. Early onset problem behaviors and alcohol, tobacco, and other substance use disorders in young adulthood. Drug and Alcohol Dependence. 2012;121:152–158. doi: 10.1016/j.drugalcdep.2011.08.024. http://dx.doi.org/10.1016/j.drugalcdep.2011.08.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zapolski TCB, Pedersen SL, McCarthy DM, Smith GT. Less drinking, yet more problems: Understanding African American drinking and related problems. Psychological Bulletin. 2014;140:188–223. doi: 10.1037/a0032113. http://dx.doi.org/10.1037/a0032113. [DOI] [PMC free article] [PubMed] [Google Scholar]