

Abstract
Rheumatoid arthritis (RA) is a systemic inflammatory disease associated with a number of extra-articular organ manifestations. Ocular manifestations involved with RA are keratoconjunctivitis sicca, episcleritis, scleritis, corneal changes, and retinal vasculitus. The etiopathogenesis of this autoimmune disorder is still unknown. Aim of our study was to present different ocular manifestations of RA and their frequency. We have examined 691 patient with the diagnoses of RA. All examined patients were in I or II stage of the disease according to criteria of The American College of Rheumatology. Ophthalmological exam obtained: visual acuity by Snellen sings, biomicroscopy of anterior segment, Schirmer test, tear break-up time (BUT), applanation tonometry and indirect ophthalmoscopy. In all patients with retinal vasculitis fotofundus and in indicated cases fluorescein angiography was preformed. The most common manifestation of ocular involvement was keratoconjunctivitis sicca. Episcleritis was diagnosed in 5.06% patients with RA, while scleritis was present in 2.06% of patients. Diffuse scleritis was present in one patient, while nodular was present in 13 patients. There were no patients with posterior or necrotizing scleritis among examined patients. Sclerosing keratitis was diagnosed in 11 female patients. It is characterized with peripheral thickening and opacification of the stroma adjacent to the site of inflammation. Posterior scleritis or scleromalacia of cornea was not present in our patients, because all of them were in I or II stage of disease. Retinal vasculitis was present in three patients, two male and one female patient (0.45%). Ocular manifestation was present in 27.2% of patients. Women were more affected.
Keywords: rheumatoid arthritis, keratoconjunctivitis sicca, scleritis, retinal vasculitus
INTRODUCTION
Rheumatoid arthritis (RA) is a systemic inflammatory disease, which is associated with a number of extra-articular organ manifestations, such as pericarditis, pleuritis, major cutaneous vasculitis, Felty’s syndrome, neuropathy, ocular manifestations, glomerulonephritis, and other types of vasculitis [1, 2, 3, 4, 5]. The etiopathogenesis of this autoimmune disorder is still unknown. There are many different theories [3, 4, 15, 16, 18]. Extra-articular manifestation in RA are present in 10-20% of patients which are more frequent in seropositive patients [3]. Ocular manifestations involved with RA are keratoconjunctivitis sicca, episcleritis, scleritis, corneal changes, and and retinal vasculitus [4, 6, 7]. Keratoconjunctivitis sicca is common in individuals with RA and is often the initial manifestation [6, 7]. Episcleritis is an inflammatory condition affecting the episcleral tissue that lies between the conjunctiva and the sclera. Episcleritis is usually a mild, self-limiting, recurrent disease. Most cases are idiopathic; although up to one third have an underlying systemic condition [6, 7, 8]. Scleritis is a chronic, painful, and potentially blinding inflammatory disease that is characterized by edema and cellular infiltration of the scleral and episcleral tissues. It may be classified into anterior and posterior. Anterior scleritis can be diffuse, nodular, necrotizing with inflammation (necrotizing), and necrotizing without inflammation (scleromalacia perforans) [8]. The most common clinical forms are diffuse scleritis and nodular scleritis. Necrotizing scleritis with or without inflammation is much less frequent, more ominous, and frequently associated with systemic autoimmune disorders. Posterior scleritis is characterized by flattening of the posterior aspect of the globe, thickening of the posterior coats of the eye (choroid and sclera), and retrobulbar oedema [9, 10]. RA is common disorder to affect peripheral cornea. Corneal changes such as sclerosing keratitis, peripheral corneal thinning, acute stromal keratitis and acute corneal melting are manifestations [7, 8]. Vasculitis affects patients with established RA in approximately 1 to 5% [3]. Retinal vasculitis is usually present on periphery of retina and involves veins and arteries peripheral branches. Aim of our study was to present different ocular manifestations of RA and their frequency.
MATERIALS AND METHODS
Patients
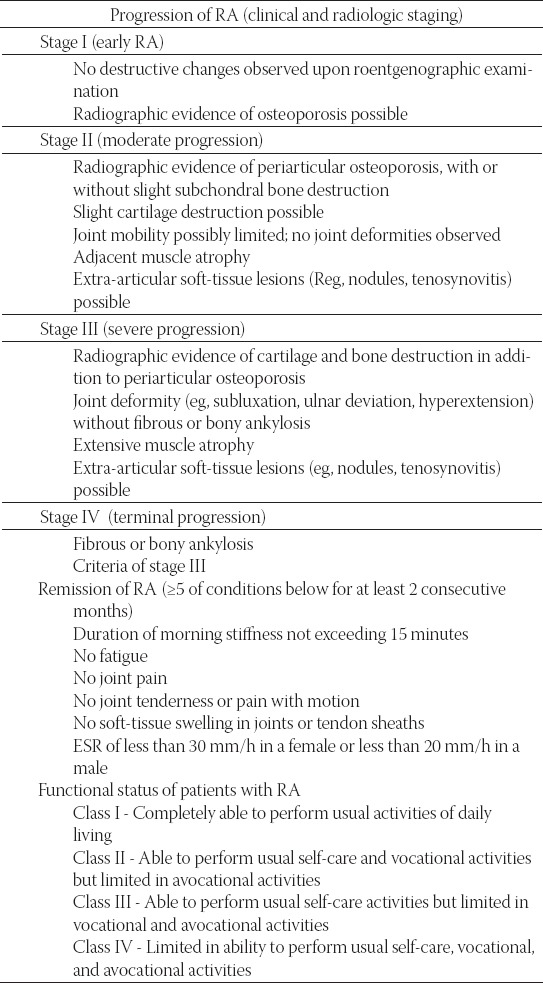
During the period from 1998-2009, we have examined 691 patients with diagnose of RA. All examined patients were in I or II stage of disease according to criteria of The American College of Rheumatology (Table 1) [10]. The presence of Rheumatoid factor (RFIgM) in serum was evaluated by standard test methods based on principle of agglutination (Waaler-Rose and Latex tests) in Immunological Laboratory in Niš. All patients were seropositive. Ophthalmological exam obtained: visual acuity by Snellen sings, biomicroscopy of anterior segment, Schirmer test, tear break-up time (BUT), applanation tonometry and indirect ophthalmoscopy. In all patients with retinal vasculitis fotofundus documentation, and in indicated case fluorescein angiography was done.
TABLE 1.
The American College of Rheumatology criteria in determining the progression, remission, and functional status of patients with RA.
RESULTS
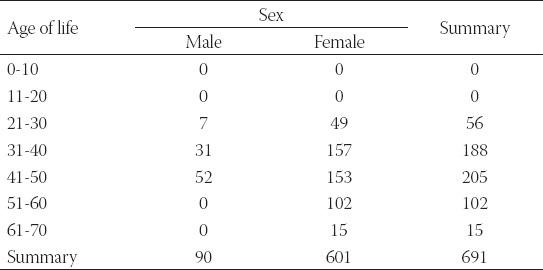
Age of life and sex of patients with ocular manifestations of RA are presented in Table 2. The frequency of RA increases with age and peaks in persons aged 3150 years. RA is more common in females than in males.
TABLE 2.
Age of life and sex of patients with ocular manifestations of RA
Ocular manifestations among examined 691 patients were present in 182 patients or in 27.2% (Table 3). Scleritis as manifestation of RA may have different forms such as diffuse, nodular and necrotizing. The frequency of these forms of scleritis in our patients is given in Table 4.
TABLE 3.
Ocular manifestation in patients with RA
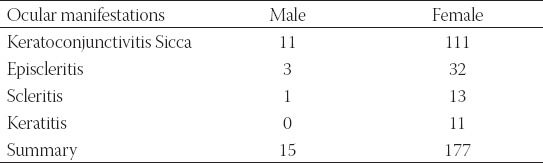
TABLE 4.
Different forms of scleritis among examined patients with RA

Keratoconjunctivitis sicca (Figure 1) was present in 122 patients or 17.65 % of all patients. Episcleritis (Figure 2) was diagnosed in 35(5.06%) patients with RA, while scleritis was present in 14 (2.06%) of patients. Diffuse scleritis was present in one patient while nodular was present in 13 patients. There were no patients with posterior or necrotizing scleritis among examined patients. Sclerosing keratitis was diagnosed in 11 female patients. Peripheral thickening and opacification of the stroma adjacent to the site of inflammation characterize it (Figure 3). Retinal vasculitis was present in three patients, two male and one female patient (0.45%). In all patients diagnose of RA was established from one to three years before the retinal vasculitis was diagnosed. Retinal vasculitis is usually present on periphery of retina and involves veins and arteries peripheral branches (Figure 4).
FIGURE 1.

Keratoconjunctivitis sicca
FIGURE 2.

Episcleritis
FIGURE 3.

Sclerosing keratitis
FIGURE 4.
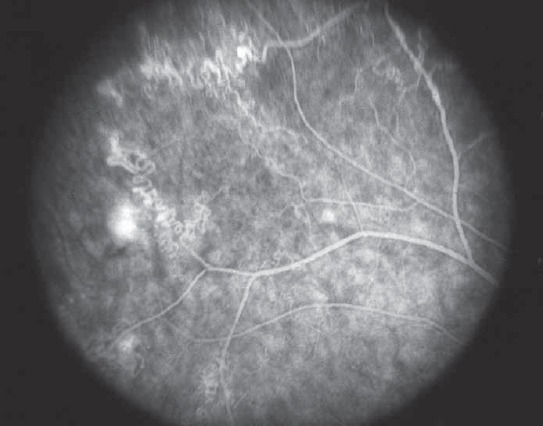
FA of peripheral branch vein inflammation in patient with RA
DISCUSSION
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease of unknown cause that primarily affects the peripheral joints in a symmetric pattern. There are many theories of pathogenesis of RA [3, 4, 15, 16, 18]. The majority of scientists support the immunology based theory on discovery of RF. RF is an antiimunglobuline with a course against fragment Fc of IgG human molecule. Probably, CD 4 T cells, mononuclear phagocytes, fibroblasts, osteoclasts, and neutrophils play major cellular roles in the pathophysiology of RA, while B lymphocytes produce autoantibodies (ie, [RF’s]). Abnormal production of numerous cytokines, chemokines, and other inflammatory mediators (has been demonstrated in patients with RA. RF may be present in other inflammatory disorders and be present in healthy person and can’t be pathognomonic sign of RA. Persistently increased RF is more predisposing factor to developing RA [3]. Other leading theory is genetic. RA has a significant genetic component, and the shared epitope of the HLA-DR 4/DR 1 cluster is present in up to 90% of patients with RA. Genetic factors and immune system abnormalities contribute to disease development and propagation. Inflammation and exuberant proliferation of synovium leads to destruction of various tissues, including cartilage, bone, tendons, ligaments, and blood vessels. Extra-articular involvement of organs such as the skin, heart, lungs, and eyes is significant [1, 2, 3, 6] and is present in 10-20% of patients, more frequent in seropositive patients [3]. The most common manifestation of ocular involvement was keratoconjunctivitis sicca in 17.65%. The incidence keratoconjunctivitis sicca is between 11, 6% to 50%, in literature [11, 12, 13]. The keratoconjunctivitis in RA is classically described as an aqueous tear deficiency. Those patients with this disorder need supplementation of artificial tears for lifetime. Hori, Maeda and Sakamoto proved that in patients with due to an altered ocular environment or chronic topical medication use demonstrate a disruption of the natural flora with a marked increase in antibioticresistant organisms [14]. Sometimes disease-modifying anti rheumatic drugs (DMARDs) systemic immunosuppressive agents may be necessary to improve tear production and to resolve severe sucu as keratoconjunctivitis like Cyclosporin A, or a monoclonal antibody to TNF-alpha such as infliximab [15, 16, 17, 18-28]. Episcleritis was diagnosed in 35 patients. In the most of the cases, treatment was not necessary. The inflammatory response is localized to the superficial episcleral vascular network, and histopathology shows nongranulomatous inflammation with vascular dilatation and perivascular infiltration [19]. The 2 clinical types are simple and nodular [16]. The most common type is simple episcleritis, in which there are intermittent bouts of moderate-to- severe inflammation that often recur at 1- to 3-month intervals. The episodes usually last 7-10 days and most resolve after 2-3 weeks. Prolonged episodes may be more common in patients with associated systemic conditions. Some patients note that episodes are more common in the spring or fall. Patients with nodular episcleritis have prolonged attacks of inflammation that are typically more painful than simple episcleritis [17]. However, some patients with mild symptoms demand treatment and may benefit from the use of artificial tears. Nodular episcleritis have an associated systemic disease. Simple episcleritis often requires no treatment. Artificial tears are useful for patients with mildto-moderate symptoms. Patients with severe or prolonged episodes may require artificial tears and/or topical corticosteroids. Nodular episcleritis is more indolent and may require local corticosteroid drops or anti-inflammatory agents. Topical ophthalmic 0.5% prednisolone, 0.1% dexamethasone or 0.1% betamethasone daily may be used. If nodular episcleritis is unresponsive to topical therapy, systemic antiinflammatory agents may be useful. Flurbiprofen (100 mg tid) is usually effective until inflammation is suppressed. If there is no response to flurbiprofen, indomethacin should be used; 100 mg daily and decreased to 75 mg when there is a response. Many patients who do not respond to one nonsteroidal anti-inflammatory agent (NSAID) may respond to another NSAID [20]. Scleritis may be the initial or only presenting clinical manifestation of these potentially lethal disorders. The correct and rapid diagnosis and the appropriate systemic therapy can halt the relentless progression of both ocular and systemic processes, thus preventing destruction of the globe and prolonging survival [16]. Scleritis may be classified into anterior and posterior. Anterior scleritis can be diffuse, nodular, necrotizing with inflammation (necrotizing), and necrotizing without inflammation (scleromalacia perforans). The most common clinical forms are diffuse scleritis and nodular scleritis. Necrotizing scleritis with or without inflammation is much less frequent, more ominous, and frequently associated with systemic autoimmune disorders. Posterior scleritis is characterized by flattening of the posterior aspect of the globe, thickening of the posterior coats of the eye (choroid and sclera), and retrobulbar edema [16, 17, 18]. Ocular complications of scleritis, which cause vision loss and eye destruction, appear as a result of the extending scleral inflammation. Peripheral ulcerative keratitis (13-14%), uveitis (about 42%), glaucoma (12-13%), cataract (6-17%), and fundus abnormalities (about 6.4%). These complications are most common in necrotizing scleritis, the most destructive type of scleritis [16]. Scleritis was present in 2.06% of all patients that is according to similar literature studies. Anterior scleritis was diagnosed in all patients. The primary sign was redness. It may be localized in one sector or involve the whole sclera; most frequently, it is in the interpalpebral area. This discoloration does not blanche after topical applications of routine sympathomimetic dilating agents (Neo-Synephrine 2.5%). Other symptoms of scleritis were pain, tearing or photophobia, tenderness. By biomicroscopy examination of anterior segment in scleritis, maximum congestion is in the deep episcleral network with some congestion in the superficial episcleral network. Treatment of scleritis requires systemic therapy such as nonsteroidal anti-inflammatory drugs (NSAID’s), corticosteroids, or DMARDs are indicated [15, 20]. Posterior scleritis or scleromalacia of cornea was not present in our patients, because all of them were in I or II stage of disease. Retinal vasculitis is one of the ocular manifestations of RA. It affects patients with established RA in approximately 1 to 5% [1]. In our patients with retinal vasculitis diagnose of RA was established one to three years before diagnosed vasculitis. All of them had seropositive RA. Retinal vasculitis is usually present on periphery of retina and involves veins and arteries peripheral branches. Therapy includes topical corticosteroid, NSAID’s, systemic corticosteroid and therapy known as biological therapy [27, 28]. There are new data that new bio-tech therapies, such as Rituximab provide significant efficiacy and safety [28].
CONCLUSION
Extra-articular involvement of organs in RA is significant. Ocular manifestations involved with RA are keratoconjunctivitis sicca, episcleritis, scleritis corneal changes, and retinal vasculitis. They were present in 27,2% of patients. Women were more affected. The most common manifestation of ocular involvement was keratoconjunctivitis sicca. Posterior scleritis or scleromalacia of cornea was not present in patients with I or II stage of disease. The new bio-tech therapies provide significant efficiacy and safety. The evaluative disease activity requires intensive treatment with DMARDs including biological therapy for rheumatoid arthritis and its ocular manifestations such as keratoconjunctivitis sicca and retinal vasculitis.
DECLARATION OF INTEREST
Authors declare no conflict of interest.
REFERENCES
- 1.Felson DT, Anderson JJ, Boers M. American College of Rheumatology. Preliminary definition of improvement in rheumatoid arthritis. Arthritis Rheum. 1995;38:727–735. doi: 10.1002/art.1780380602. [DOI] [PubMed] [Google Scholar]
- 2.Turesson C, O’Fallon WM, Crowson CS, Gabriel SE, Matteson EL. Extra-articular disease manifestations in rheumatoid arthritis: incidence trends and risk factors over 46 years. Ann. Rheum. Dis. 2003;62:722–727. doi: 10.1136/ard.62.8.722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sahatçiu-Meka V, Rexhepi S, Manxhuka-Kerliu S, Rexhepi M. Extraaricular manifestation of seronegative and seropositive reumathoid arthritis. Bosn. J Basic Med Sci. 2010;10(1):27–31. doi: 10.17305/bjbms.2010.2729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lilleby V, Gran JT. Systemic rheumatoid arthritis. Tidsskr Nor Laegeforen. 1997;117(29):4223–4225. [PubMed] [Google Scholar]
- 5.Goronzy JJ, Weyand CM. Developments in the scientific under-standing of rheumatoid arthritis. Arthritis Res Ther. 2009;11(5):249. doi: 10.1186/ar2758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cimmino MA, Salvarani C, Macchioni P, et al. Extra-articular manifestations in YZ Italian patients with rheumatoid arthritis. Rheumatol Int. 2000;19(6):213–217. doi: 10.1007/pl00006853. [DOI] [PubMed] [Google Scholar]
- 7.Kanski JJ. The eye in systemic disease. London: Butterworts; 1986. [Google Scholar]
- 8.Whitson WE, Krachmer JH. Adult rheumatoid arthritis. In: Gold DH, Weingeist TA, editors. The eye in systemic disease. Philadelphia: JB Lippincott; 1990. pp. 127–208. [Google Scholar]
- 9.Hakin KN, Ham J, Lightman SL. Use of orbital floor steroids in the management of patients with uniocular non-necrotizing scleritis. Br J Ophthalmol. 1991;75(6):337–339. doi: 10.1136/bjo.75.6.337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Galor A, Jabs DA, Leder HA, Kedhar SR, Dunn JP, Peters GB. Comparison of antimetabolite drugs as corticosteroid-sparing therapy for noninfectious ocular inflammation. Ophthalmol. 2008;115(10):1826–1832. doi: 10.1016/j.ophtha.2008.04.026. [DOI] [PubMed] [Google Scholar]
- 11.Arnett FC, Edworthy SM, Bloch DA. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31:315–324. doi: 10.1002/art.1780310302. [DOI] [PubMed] [Google Scholar]
- 12.Goto E, Matsumoto Y, Kamoi M, Endo K, Ishida R, Dogru M. Tear evaporation rates in Sjögren syndrome and non-Sjögren dry eye patients. Am J Ophthalmol. 2007;144(1):81–85. doi: 10.1016/j.ajo.2007.03.055. [DOI] [PubMed] [Google Scholar]
- 13.Barr CC, Davis H, Culberson WW. Rheumatoid scleritis. Ophthalmol. 1981;88:1269–1273. doi: 10.1016/s0161-6420(81)34866-0. [DOI] [PubMed] [Google Scholar]
- 14.Hori Y, Maeda N, Sakamoto M, Koh S, Inoue T, Tano Y. Bacteriologic profile of the conjunctiva in the patients with dry eye. Am J Ophthalmol. 2008;146(5):729–734. doi: 10.1016/j.ajo.2008.06.003. [DOI] [PubMed] [Google Scholar]
- 15.Sobrin L, Kim EC, Christen W, Papadaki T, Letko E, Foster CS. Infliximab therapy for the treatment of refractory ocular infiammatory disease. Arch Ophthalmol. 2007;125(7):895–900. doi: 10.1001/archopht.125.7.895. [DOI] [PubMed] [Google Scholar]
- 16.Sainz de la Maza M, Foster CS, Jabbur NS. Scleritis associated with rheumatoid arthritis and with other systemic immune-mediated diseases. Ophthalmol. 1994;101(7):1281–1286. [PubMed] [Google Scholar]
- 17.Lin CP, Shih MH, Su CY. Scleritis. Surv Ophthalmol. 2006;51(3):288–289. doi: 10.1016/j.survophthal.2006.02.011. [DOI] [PubMed] [Google Scholar]
- 18.Fong LP, Sainz de la Maza M, Rice BA, Kupferman AE, Foster CS. Immunopathology of scleritis Ophthalmol . 1991;98(4):472–479. doi: 10.1016/s0161-6420(91)32280-2. [DOI] [PubMed] [Google Scholar]
- 19.Sainz de la Maza M, Jabbur NS, Foster CS. Severity of scleritis and episcleritis. Ophthalmol. 1994;101(2):389–396. doi: 10.1016/s0161-6420(94)31325-x. [DOI] [PubMed] [Google Scholar]
- 20.Wakefield D, McCluskey P. Cyclosporin therapy for severe scleritis. Br J Ophthalmol. 1989;73(9):743–746. doi: 10.1136/bjo.73.9.743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cazabon S, Over K, Butcher J. The successful use of infliximab in resistant relapsing polychondritis and associated scleritis. Eye. 2005;19(2):222–224. doi: 10.1038/sj.eye.6701457. [DOI] [PubMed] [Google Scholar]
- 22.Murphy CC, Ayliffe WH, Booth A, Makanjuola D, Andrews PA, Jayne D. Tumor necrosis factor alpha blockade with infliximab for refractory uveitis and scleritis. Ophthalmol. 2004;111(2):352–356. doi: 10.1016/S0161-6420(03)00721-8. [DOI] [PubMed] [Google Scholar]
- 23.Sobrin L, Kim EC, Christen W, Papadaki T, Letko E, Foster CS. Infliximab therapy for the treatment of refractory ocular inflammatory disease. Arch Ophthalmol. 2007;125(7):895–900. doi: 10.1001/archopht.125.7.895. [DOI] [PubMed] [Google Scholar]
- 24.Ahmadi-Simab K, Lamprecht P, Nolle B, Ai M, Gross WL. Successful treatment of refractory anterior scleritis in primary Sjogren’s syndrome with rituximab. Ann Rheum Dis. 2005;64(7):1087–1088. doi: 10.1136/ard.2004.027128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lim L, Suhler EB, Smith JR. Biologic therapies for inflammatory eye disease. Clin Exp Ophthalmol. 2006;34(4):365–374. doi: 10.1111/j.1442-9071.2006.01225.x. [DOI] [PubMed] [Google Scholar]
- 26.Sobrin L, Christen W, Foster CS. Mycophenolate mofetil after methotrexate failure or intolerance in the treatment of scleritis and uveitis. Ophthalmol. 2008;115(8):1416–1421. doi: 10.1016/j.ophtha.2007.12.011. [DOI] [PubMed] [Google Scholar]
- 27.Papaliodis GN, Chu D, Foster CS. Treatment of ocular inflammatory disorders with daclizumab. Ophthalmol. 2003;110(4):786–789. doi: 10.1016/S0161-6420(02)01932-2. [DOI] [PubMed] [Google Scholar]
- 28.Sokolović Š, Kasumagić Š, MarkićĐurović M, AganovićMušinović I. The impact of Rituximab therapy on the chromosomes of patients with rheumatoid arthritis. Bosn J Basic Med Sci. 2010;10(2):121–124. doi: 10.17305/bjbms.2010.2706. [DOI] [PMC free article] [PubMed] [Google Scholar]