

Abstract
Behçet's disease (BD) is an autoimmune multisystemic disease. The precise etiology of BD is not fully understood; however, it is thought that interactions between genetic and environmental factors play an essential role in its pathogenesis. The nuclear receptor coactivator-5 (NCOA5) gene encodes a coregulator for nuclear receptor subfamily 1 group D member 2 (NR1D2) and estrogen receptor 1 and 2 (ESR1 and ESR2). Also, the NCOA5 gene insufficiency leads to an elevated expression of IL-6, and increased levels of IL-6 were found to be related to the pathogenesis of BD. In this study, we aimed to clarify the impact of the NCOA5 rs2903908 polymorphism on susceptibility and clinical findings of BD. This study included 671 participants (300 BD patients and 371 healthy controls). The analyses of NCOA5 rs2903908 polymorphism was performed by using the TaqMan allelic discrimination assay. The frequency of TT genotype of the NCOA5 rs2903908 polymorphism was found significantly higher in BD patients compared to those in healthy controls (p=0.016, OR=1.46, 95 % CI=1.08-1.99). Also, the frequencies of CT genotype was observed significantly higher in BD patients with genital ulceration and uveitis than without genital ulceration and uveitis (p=0.002 and p=0.005, respectively). The most significant association was found between C allele frequencies of BD patients with and without uveitis (p=0.0001). Our study represents for the first time that the NCOA5 rs2903908 polymorphism seemed to be linked to BD susceptibility and clinical findings.
Keywords: Behçet's disease, NCOA5, rs2903908, uveitis
Introduction
Behçet's disease (BD) is a multisystemic, chronic inflammatory autoimmune disease with unknown aetiology and described as a triad of recurrent oral aphthous ulcers, genital ulceration, and uveitis. The other clinical findings include mucocutaneous, articular, neurologic, urogenital, vascular, gastrointestinal, and pulmonary involvements (Gül, 2005[12]). BD is more prevalent in the geographic region along the “Silk Road,” which lies from the Mediterranean to the Far East. The prevalence of BD in Turkey varies from 20 to 420 cases per 100,000 adults, which is the highest prevalence rate identified in the world (Idil et al., 2002[15]; Azizlerli et al., 2003[3]; Cakir et al., 2004[7]). The male-to-female ratio is nearly equal, and the disease occurs in individuals aged 18 to 40 years (Gül, 2005[12]; Alpsoy et al., 2007[1]).
The precise aetiology of BD is not fully understood; however, it is thought that interactions between genetic and environmental factors play an essential role in the pathogenesis of the disease. Detecting interactions between the genes and mechanisms playing roles in the pathogenesis of numerous diseases can be difficult to find, but there are many examples in which common genetic factors take part in the development of several chronic inflammatory autoimmune diseases (Aune et al., 2003[2]; Lee et al., 2012[19]; Oğuz et al., 2016[23]). This suggests that certain gene regions may contribute similar pathways that are shared by various autoimmune diseases. In this field, the CD40 gene was indicated as a susceptible gene for a number of chronic inflammatory and autoimmune diseases (García-Bermúdez et al., 2012[11]; Joo et al., 2013[17]). Additionally, CD40 is a member of tumor necrosis factor receptor superfamily (Foy et al., 1996[9]). The nuclear receptor coactivator-5 (NCOA5) gene, located on the 20q13.1 region (a 400-kb surrounding zone of the CD40 gene), encodes a coregulator for nuclear receptor subfamily 1 group D member 2 (NR1D2) and estrogen receptor 1 and 2 (ESR1 and ESR2). NCOA5 is known to modulate the ESR1 mediated renewal, proliferation, and differentiation of the pluripotent stem cells (Naugler et al., 2007[22]; Böser et al., 2013[5]; Sarachana and Hu., 2013[26]). On the other hand, ESR1 and ESR2 were accepted to take part in regulating autoimmunity in systemic lupus erythematosus by promoting the production of pathogenic autoantibodies (Bynoté et al., 2008[6]). Furthermore, the surrounding of NCOA5 gene region where the CD40 gene is also located includes possible susceptible genes of type 2 diabetes mellitus and rheumatoid arthritis (Raychaudhuri et al., 2008[25]; Lewis et al., 2010[20]). Recently, the significant relationship between the NCOA5 rs2903908 polymorphism and susceptibility to psoriasis, which is a T cell mediated chronic inflammatory disease, was also reported (Zervou et al., 2011[32]). Additionally, genome-wide association studies on psoriasis and BD showed that these diseases share many common genetic risk factors (Lee et al., 2012[19]). Moreover, the NCOA5 gene insufficiency leads to an elevated expression of Interleukin (IL)-6, and increased levels of IL-6 were found to be related to the pathogenesis of BD (Naugler et al., 2007[22]; Talaat et al., 2014[27]). These similarities led us to consider the NCOA5 gene as a candidate for BD. Any association between the susceptibility and clinical outcomes of BD and the NCOA5 rs2903908 polymorphism have not yet been clarified. Therefore, we aimed to clarify the impacts of the NCOA5 rs2903908 polymorphism on susceptibility and clinical findings of BD.
Materials and Methods
Sampling and genotyping
This study included 300 patients with BD and 371 ethnicity-matched healthy controls. All of the patients had been diagnosed according to the criteria of the International Study Group for BD (International Team for the Revision of the International Criteria for Behçet's Disease, 2014[16]). Informed consent was obtained from all participants before they enrolled in this study. The study was performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Gaziosmanpasa University, Faculty of Medicine. Patients, who had any autoimmune systemic inflammatory diseases, such as rheumatoid arthritis or genetic diseases, were excluded from the study.
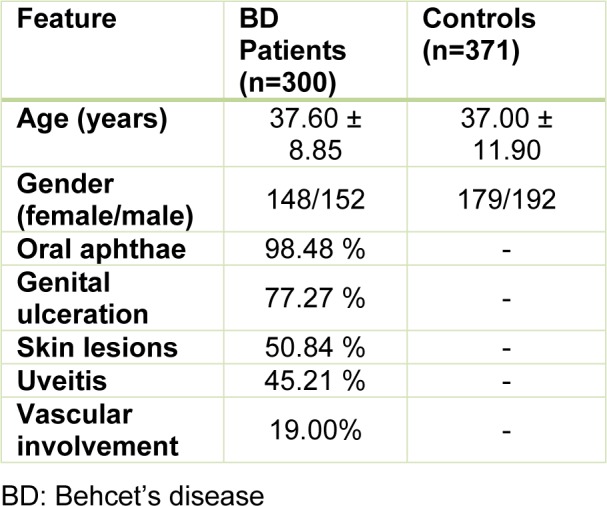
The age and gender data of the all participants are given in Table 1(Tab. 1). Clinical findings of oral aphthae, genital ulceration, skin lesions, uveitis, and vascular involvement of the patients were noted as present or absent. Skin lesions consisted of erythema nodosum or papulopustular lesions.
Table 1. The demographical and clinical findings of all participants.
We performed DNA purification with DNA isolation kits from peripheral venous blood samples (preserved in EDTA tubes) of the patient and control groups. Genetic analyses were performed by using the TaqMan allelic discrimination assay. All SNPs were genotyped in the same centre by using a TaqMan SNP genotyping assay in a StepOnePlus Real-Time Polymerase Chain Reaction (PCR) system by following the conditions recommended by the manufacturer (Applied Biosystems, Foster City, CA, USA).
We examined the distribution of the NCOA5 rs2903908 genotypes and alleles in all participants. For further evaluation, we investigated whether the NCOA5 rs2903908 polymorphism had impacts on the development of any clinical findings such as genital ulceration, skin lesions, uveitis, or vascular involvement.
Statistical analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) software version 15.0 for Windows (SPSS Inc., Chicago, IL). Mean and standard deviation were used for the presentation of continuous quantitative variables. Frequencies and percentages were used for categorical data. The NCOA5 rs2903908 overall genotype distribution was compared by chi-square (χ2) test, and the specific genotype and allele distributions were compared by using Fisher's exact test. The p-values smaller than 0.05 were considered significant. The odds ratios (ORs) and 95 % confidence intervals (CIs) were used to determine the relationships between the NCOA5 allelic and genotypic variants and their occurrence in the patients. The NCOA5 rs2903908 genotype distributions in both the patients and the healthy controls were analyzed according to the Hardy-Weinberg Equilibrium (HWE).
Results
In this study, a total of 300 unrelated Turkish patients with BD and 371 individuals without any established disease diagnoses were evaluated for the rs2903908 polymorphism of the NCOA5 gene. The demographical and clinical findings of all participants are summarized in Table 1(Tab. 1). The mean age of the patients was 37.60 ± 8.85 years, and the mean age of the healthy controls was 37.00 ± 11.90 years. There was no significant difference in terms of age and gender between the BD patients and the healthy controls (p>0.05). Oral aphthae were seen in the majority of patients (98.48 %).
The distributions of the genotypes and alleles of the patients and healthy controls for the NCOA5 rs2903908 polymorphism are presented in Table 2(Tab. 2). The frequency of TT genotype of the NCOA5 rs2903908 polymorphism was significantly higher in patients compared to those in healthy controls (p=0.016, OR=1.46, 95 % CI=1.08-1.99). We found significantly higher levels of the CT genotype of the NCOA5 rs2903908 polymorphism in healthy controls compared to those in patients with BD (p=0.014, OR=0.66, 95 % CI=0.49-0.92) (Table 2(Tab. 2)). The genotype distribution of the rs2903908 polymorphism of the NCOA5 gene in the patients and controls was compatible to HWE (p>0.05 for all) (data not shown).
Table 2. The distribution of genotypes and alleles of NCOA5 rs2903908 polymorphism in patients and controls.

We also compared genotype and allele distribution of NCOA5 rs2903908 polymorphism between patients and controls by gender basis, and we found statistical differences for CT and TT genotypes between female patients and controls (Table 3(Tab. 3)). In accordance with the general result, the CT genotype was higher in controls (p=0.014), and the TT genotype was higher in patients (p=0.026) (Table 3(Tab. 3)).
Table 3. The distribution of genotypes and alleles of NCOA5 rs2903908 polymorphism in patients and controls by the gender basis.

The CT genotype of the NCOA5 rs2903908 polymorphism was significantly higher in BD patients with genital ulceration (p=0.002, OR=3.03, 95 % CI=1.51-6.08), and the TT genotype was higher in BD patients without genital ulceration (p=0.014, OR=0.46, 95 % CI=0.25-0.84). Frequencies of C allele and genotypes including C allele (CC and CT) were significantly higher in the patients with uveitis compared to those without uveitis (p=0.0001, OR=2.19, 95 % CI=1.48-3.23 and p=0.0002, OR=2.49, 95 % CI=1.55-3.99, respectively) (Table 4(Tab. 4)).
Table 4. The distribution of genotypes and alleles of NCOA5 rs2903908 polymorphism in BD patients with and without genital ulceration, skin lesions, uveitis and vascular involvement.

Discussion
BD is an inflammatory disorder with recurrent oral aphthous ulcers, genital ulcers, and uveitis of which etiology and pathogenesis have not been fully elucidated (Gül, 2005[12]). Genetic analysis of the multicase families and populations demonstrated associations between BD and genetic factors. Whereas some authors reported human leukocyte antigen (HLA)-related genes as the predominant genetic risk factors for BD (Kirino et al., 2013[18]; Ortiz-Fernández et al., 2016[24]), others suggested several non-HLA genes (Chen et al., 2012[8]).
NCOA5 is a nuclear protein with both coactivator and corepressor domains. It encodes a coregulator for ESR1, ESR2 and NR1D2 (Naugler et al., 2007[22]; Bento et al., 2008[4]; Lewis et al., 2010[20]). NR1D2 was demonstrated to be upregulated in monocytes from psoriatic patients, and this upregulation enabled disease stage estimation with an accuracy rate of 86 % based on gene expression patterns (Hornung et al., 2002[13]). However, it was reported that NR1D2 gene expression patterns from the peripheral blood of rheumatoid arthritis patients did not differ from that of healthy individuals (Naugler et al., 2007[22]). On the other hand, NCOA5 deficiency resulted in elevated IL-6 expression (Liu and Feng, 2014[21]). NCOA5 is a known regulator of ESR1 and ESR2 which negatively regulate nuclear factor kappa B-induced IL-6 expression. NCOA5 haploinsufficiency increases the IL-6 levels by disrupting ESR1 mediated repression of IL-6 transcription (Naugler et al., 2007[22]). Talaat et al. (2014[27]) showed that BD patients with active disease had significantly higher levels of IL-6 compared to patients in remission. In addition, many other genes indicated an association with BD (Chen et al., 2012[8]; Yazici et al., 2012[31]; Hou et al., 2013[14]; Kirino et al., 2013[18]; Tasliyurt et al., 2013[28]; Tizaoui et al., 2014[29]; Xiang et al., 2014[30]). However, none of these genes are fully linked to BD.
Because NCOA5 can affect many factors and pathways, and it can work both as a coactivator and corepressor, perhaps NCOA5 may have an impact on BD, especially in females, by a way that is not yet undisclosed. This hypothesis was supported by Gao et al. who showed that the deletion of both IL-6 alleles does not completely block hepatocellular carcinoma (HCC) development in NCOA5+/ male mice, and other downstream targets of NCOA5 may also contribute to hepatocarcinogenesis (Gao et al., 2013[10]).
Previously, heterozygous deletion in the NCOA5 gene was found to be related to increased susceptibility to both glucose intolerance and HCC, partially by elevated IL-6 expression (Gao et al., 2013[10]). Conversely, NCOA5 polymorphisms, including rs2903908, were reported not to be related to type 2 diabetes mellitus (Lewis et al., 2010[20]). However, in a genome-wide association study of type 2 diabetes mellitus, the results of NCOA5 gene polymorphisms were conflicting (Bento et al., 2008[4]). Moreover, in the present study, significant relationship between the NCOA5 rs2903908 polymorphism and BD were found. Namely, we found that TT genotype and the T allele of the NCOA5 rs2903908 polymorphism were related to an increased (approximately one and half-fold) susceptibility to BD and it has a protective role for genital ulceration and uveitis in this study. Also, the CT genotype of the NCOA5 rs2903908 polymorphism was found to be associated with an increased development of uveitis (approximately two-fold) and genital ulceration (approximately three-fold) as well as to have a protective role on the development of BD (Table 4(Tab. 4)). Due to overexpression of IL-6 associated with genital ulceration and uveitis (Talaat et al., 2014[27]), and considering the results of recent studies that NCOA5 haploinsufficiency is causing an increase in IL-6 expression (Sarachana and Hu, 2013[26]; Gao et al., 2013[10]), the CT genotype for rs2903908 polymorphism may also be causing NCOA5 haploinsufficiency. The rs2903908 polymorphism is a T to C transition in the intronic region of the NCOA5 gene. In the literature, we could not find any studies showing the effect of the rs2903908 polymorphism on the expression of NCOA5 gene. A variant in intronic region may form a cryptic splice site that enhance the use of that site by making it more similar or identical to the normal splice site. Therefore, we can consider that the C allele reduces the expression of NCOA5. However, confirmation of this hypothesis is needed, especially when considering why the CC genotype is not significantly higher in patients with genital ulcers and uveitis. Inconsistent with our results, Zervou and colleagues (2011[32]) reported significantly higher levels of the CC genotype and the C allele of the NCOA5 rs2903908 polymorphism in patients with psoriasis, and they emphasized that the CC genotype and the C allele of the NCOA5 rs2903908 polymorphism might be related to an elevated susceptibility to psoriasis (Zervou et al., 2011[32]). Our study did not find a significant difference for the CC genotype between the patients and the control group. These discordant results may be due to the various underlying pathogenetic mechanisms of the diseases, as well as different ethnic basis and environmental factors. The study of Gao et al. (2013[10]) showed that the NCOA5 gene may be impacted positively and negatively by more factors than we previously mentioned. Nevertheless, this discrepancy may be clarified by future studies investigating the impacts of the NCOA5 rs2903908 polymorphism on several chronic inflammatory diseases.
To the best of our knowledge, this preliminary study represents, for the first time, the association between the NCOA5 rs2903908 polymorphism and the susceptibility and clinical findings of BD. We arrived at three main results. First, the frequency of TT genotype of the NCOA5 rs2903908 polymorphism was significantly higher in the female BD patients compared to those in the healthy controls, and this genotype and allele seemed to be related to an increased (approximately one and half-fold) risk of BD development (p=0.026, OR=1.67, 95 % CI=1.08-2.59). In addition, the CT genotype of the NCOA5 rs2903908 polymorphism appeared to prevent individuals from developing BD. Second, the CT genotype of the NCOA5 rs2903908 polymorphism seemed to predispose the BD patients to develop both genital ulceration and uveitis more frequently (approximately three-fold for genital ulceration and two-fold for uveitis), whereas the TT genotype of NCOA5 rs2903908 polymorphism was found to have protective impacts on developing genital ulceration or uveitis in the patients with BD. Finally, we found that the BD patients who are carrying the C allele at the NCOA5 rs2903908 locus may be more prone to developing uveitis. Although CC genotype was observed 3 times more in patients with uveitis than without uveitis, the statistically significance was not found (8.24 % vs. 2.91 %; p=0.070, OR=2.80, 95 % CI=0.93-8.23) (Table 4(Tab. 4)).
In conclusion, our study identified that the NCOA5 rs2903908 polymorphism seemed to be linked to BD susceptibility in females and in clinical findings. Additionally, the CD40 gene, which is located near the region of the NCOA5 gene, was previously related to several chronic autoimmune inflammatory diseases. We conclude that the NCOA5 gene may be a good candidate for future studies investigating genetic tendencies for chronic inflammatory and autoimmunity diseases that share similar pathogenic pathways. How the rs2903908 variant affects the NCOA5 mRNA or protein expression and function and how this polymorphism influences the pathogenesis of BD and its symptoms remain mysteries to be solved.
Acknowledgements
The manuscript was professionally edited by www.scribendi.com. We thank Osman Demir for his help in statistical analyses.
The study was supported by a grant from Scientific Research Projects of Gaziosmanpasa University, project number #2012/20.
Declaration of interest
The authors report no declarations of interest.
References
- 1.Alpsoy E, Donmez L, Onder M, Gunasti S, Usta A, Karincaoglu Y, et al. Clinical features and natural course of Behçet's disease in 661 cases: a multicentre study. Br J Dermatol. 2007;157:901–906. doi: 10.1111/j.1365-2133.2007.08116.x. [DOI] [PubMed] [Google Scholar]
- 2.Aune TM, Maas K, Moore JH, Olsen NJ. Gene expression profiles in human autoimmune disease. Curr Pharm Des. 2003;9:1905–1917. doi: 10.2174/1381612033454360. [DOI] [PubMed] [Google Scholar]
- 3.Azizlerli G, Köse AA, Sarica R, Gül A, Tutkun IT, Kulaç M, et al. Prevalence of Behçet's disease in Istanbul, Turkey. Int J Dermatol. 2003;42:803–806. doi: 10.1046/j.1365-4362.2003.01893.x. [DOI] [PubMed] [Google Scholar]
- 4.Bento JL, Palmer ND, Zhong M, Roh B, Lewis JP, Wing MR, et al. Heterogeneity in gene loci associated with type 2 diabetes on human chromosome 20q13.1. Genomics. 2008;92:226–234. doi: 10.1016/j.ygeno.2008.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Böser A, Drexler HC, Reuter H, Schmitz H, Wu G, Schöler HR, et al. SILAC proteomics of planarians identifies Ncoa5 as a conserved component of pluripotent stem cells. Cell Rep. 2013;5:1142–1155. doi: 10.1016/j.celrep.2013.10.035. [DOI] [PubMed] [Google Scholar]
- 6.Bynoté KK, Hackenberg JM, Korach KS, Lubahn DB, Lane PH, Gould KA. Estrogen receptor-alpha deficiency attenuates autoimmune disease in (NZB x NZW)F1 mice. Genes Immun. 2008;9:137–152. doi: 10.1038/sj.gene.6364458. [DOI] [PubMed] [Google Scholar]
- 7.Cakir N, Dervis E, Benian O, Pamuk ON, Sonmezates N, Rahimoglu R, et al. Prevalence of Behçet's disease in rural western Turkey, a preliminary report. Clin Exp Rheumatol. 2004;22:53–55. [PubMed] [Google Scholar]
- 8.Chen F, Hou S, Jiang Z, Chen Y, Kijlstra A, Rosenbaum JT, et al. CD40 gene polimorphisms confer risk of Behçet’s disease but not of Vogt-Koyanagi-Harada syndrome in Han Chinese population. Rheumatology. 2012;51:47–51. doi: 10.1093/rheumatology/ker345. [DOI] [PubMed] [Google Scholar]
- 9.Foy TM, Aruffo A, Bajorath J, Buhlmann J, Noelle RJ. Immune regulation by CD40 and its ligand GP39. Annu Rev Immunol. 1996;14:591–617. doi: 10.1146/annurev.immunol.14.1.591. [DOI] [PubMed] [Google Scholar]
- 10.Gao S, Li A, Liu F, Chen F, Williams M, Zhang C, et al. NCOA5 haploinsufficiency results in glucose intolerance and subsequent hepatocellular carcinoma. Cancer Cell. 2013;24:725–737. doi: 10.1016/j.ccr.2013.11.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.García-Bermúdez M, González-Juanatey C, López-Mejías R, Teruel M, Corrales A, Miranda-Filloy JA, et al. Study of association of CD40-CD154 gene polymorphisms with disease susceptibility and cardiovascular risk in Spanish rheumatoid arthritis patients. PLOS One. 2012;7:e49214. doi: 10.1371/journal.pone.0049214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gül, A Behçet's disease as an autoinflammatory disorder. Curr Drug Targets Inflamm Allergy. 2005;4:81–83. doi: 10.2174/1568010053622894. [DOI] [PubMed] [Google Scholar]
- 13.Hornung V, Rothenfusser S, Britsch S, Krug A, Jahrsdörfer B, Giese T, et al. Quantitative expression of toll-like receptor 1-10 mRNA in cellular subsets of human peripheral blood mononuclear cells and sensitivity to CpG oligodeoxynucleotides. J Immunol. 2002;168:4531–4537. doi: 10.4049/jimmunol.168.9.4531. [DOI] [PubMed] [Google Scholar]
- 14.Hou S, Qi J, Zhang Q, Liao D, Li Q, Hu K, et al. Genetic variants in the JAK1 gene confer higher risk of Behcet's disease with ocular involvement in Han Chinese. Hum Genet. 2013;132:1049–1058. doi: 10.1007/s00439-013-1312-5. [DOI] [PubMed] [Google Scholar]
- 15.Idil A, Gürler A, Boyvat A, Caliskan D, Ozdemir O, Isik A, et al. The prevalence of Behçet's disease above the age of 10 years. The results of a pilot study conducted at the Park Primary Health Care Center in Ankara., Turkey. Ophthalmic Epidemiol. 2002;9:325–331. doi: 10.1076/opep.9.5.325.10338. [DOI] [PubMed] [Google Scholar]
- 16.International Team for the Revision of the International Criteria for Behçet's Disease (ITR-ICBD) The International Criteria for Behçet's Disease (ICBD), a collaborative study of 27 countries on the sensitivity and specificity of the new criteria. J Eur Acad Dermatol Venereol. 2014;28:338–347. doi: 10.1111/jdv.12107. [DOI] [PubMed] [Google Scholar]
- 17.Joo YB, Park BL, Shin HD, Park SY, Kim I, Bae SC. Association of genetic polimorphisms in CD40 with susceptibility to SLE in Korean population. Rheumatology. 2013;52:623–630. doi: 10.1093/rheumatology/kes339. [DOI] [PubMed] [Google Scholar]
- 18.Kirino Y, Bertsias G, Ishigatsubo Y, Mizuki N, Tugal-Tutkun I, Seyahi E, et al. Genome-wide association analysis identifies new susceptibility loci for Behçet's disease and epistasis between HLA-B*51 and ERAP1. Nat Genet. 2013;45:202–207. doi: 10.1038/ng.2520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lee YH, Choi SJ, Ji JD, Song GG. Genome-wide pathway analysis of a genome-wide association study on psoriasis and Behcet's disease. Mol Biol Rep. 2012;39:5953–5959. doi: 10.1007/s11033-011-1407-9. [DOI] [PubMed] [Google Scholar]
- 20.Lewis JP, Palmer ND, Ellington JB, Divers J, Ng MC, Lu L, et al. Analysis of candidate genes on chromosome 20q12-13.1 reveals evidence for BMI mediated association of PREX1 with type 2 diabetes in European Americans. Genomics. 2010;96:211–219. doi: 10.1016/j.ygeno.2010.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Liu CY, Feng GS. NCOA5, a molecular link between type 2 diabetes and liver cancer. Hepatobiliary Surg Nutr. 2014;3:106–108. doi: 10.3978/j.issn.2304-3881.2014.04.02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Naugler WE, Sakurai T, Kim S, Maeda S, Kim K, Elsharkawy AM, et al. Gender disparity in liver cancer due to sex differences in MyD88-dependent IL-6 production. Science. 2007;317:121–124. doi: 10.1126/science.1140485. [DOI] [PubMed] [Google Scholar]
- 23.Oğuz AK, Yılmaz ST, Oygür ÇŞ, Çandar T, Sayın I, Kılıçoğlu SS, et al. Behçet's: A disease or a syndrome? Answer from an expression profiling study. PLoS One. 2016;11(2):e0149052. doi: 10.1371/journal.pone.0149052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ortiz-Fernández L, Carmona FD, Montes-Cano MA, García-Lozano JR, Conde-Jaldón M, Ortego-Centeno N, et al. Genetic analysis with the immunochip platform in Behçet disease. Identification of Residues associated in the HLA class I region and new susceptibility loci. PLoS One. 2016;11(8):e0161305. doi: 10.1371/journal.pone.0161305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Raychaudhuri S, Remmers EF, Lee AT, Hackett R, Guiducci C, Burtt NP, et al. Common variants at the CD40 and other loci confer risk of rheumatoid arthritis. Nat Genet. 2008;40:1216–1223. doi: 10.1038/ng.233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sarachana T, Hu VW. Differential recruitment of coregulators to the RORA promoter adds another layer of complexity to gene (dys. regulation by sex hormones in autism. Mol Autism. 2013;4(1):39. doi: 10.1186/2040-2392-4-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Talaat RM, Ashour ME, Bassyouni IH, Raouf AA. Polymorphisms of interleukin 6 and interleukin 10 in Egyptian people with Behcet's disease. Immunobiology. 2014;219:573–582. doi: 10.1016/j.imbio.2014.03.004. [DOI] [PubMed] [Google Scholar]
- 28.Tasliyurt T, Yigit S, Rustemoglu A, Gul U, Ates O. Common MEFV gene mutations in Turkish patients with Behcet's disease. Gene. 2013;530:100–103. doi: 10.1016/j.gene.2013.08.026. [DOI] [PubMed] [Google Scholar]
- 29.Tizaoui K, Kaabachi W, Ouled Salah M, Ben Amor A, Hamzaoui A, Hamzaoui K. Vitamin D receptor TaqI and ApaI polymorphisms, a comparative study in patients with Behçet's disease and Rheumatoid arthritis in Tunisian population. Cell Immunol. 2014;290:66–71. doi: 10.1016/j.cellimm.2014.05.002. [DOI] [PubMed] [Google Scholar]
- 30.Xiang Q, Chen L, Hou S, Fang J, Zhou Y, Bai L, et al. TRAF5 and TRAF3IP2 gene polymorphisms are associated with Behçet's disease and Vogt-Koyanagi-Harada syndrome: a case-control study. PLOS One. 2014;9:e84214. doi: 10.1371/journal.pone.0084214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Yazici A, Cefle A, Savli H. The frequency of MEFV gene mutations in Behcet's disease and their relation with clinical findings. Rheumatol Int. 2012;32:3025–3030. doi: 10.1007/s00296-011-2011-y. [DOI] [PubMed] [Google Scholar]
- 32.Zervou MI, Goulielmos GN, Castro-Giner F, Boumpas DT, Tosca AD, Krueger-Krasagakis S. A CD40 and an NCOA5 gene polymorphism confer susceptibility to psoriasis in a Southern European population: a case-control study. Hum Immunol. 2011;72:761–765. doi: 10.1016/j.humimm.2011.05.014. [DOI] [PubMed] [Google Scholar]