

Abstract
Background
Uptake of delivery and postnatal care remains low in Low and Middle-Income Countries (LMICs), where 99% of global maternal deaths take place. However, the potential impact of antenatal depression on use of institutional delivery and postnatal care has seldom been examined. This study aimed to examine whether antenatal depressive symptoms are associated with use of maternal health care services.
Methods
A population-based prospective study was conducted in Sodo District, Southern Ethiopia. Depressive symptoms were assessed during pregnancy with a locally validated, Amharic version of the Patient Health Questionnaire (PHQ-9). A cut off score of five or more indicated possible depression. A total of 1251 women were interviewed at a median of 8 weeks (4–12 weeks) after delivery. Postnatal outcome variables were: institutional delivery care utilization, type of delivery, i.e. spontaneous or assisted, and postnatal care utilization. Multivariate logistic regression was used to examine the association between antenatal depressive symptoms and the outcome variables.
Results
High levels of antenatal depressive symptoms (PHQ score 5 or higher) were found in 28.7% of participating women. Nearly two-thirds, 783 women (62.6%), delivered in healthcare institutions. After adjusting for potential confounders, women with antenatal depressive symptoms had increased odds of reporting institutional birth [adjusted Odds Ratio (aOR) =1.42, 95% Confidence Interval (CI): 1.06, 1.92] and increased odds of reporting having had an assisted delivery (aOR = 1.72, 95% CI: 1.10, 2.69) as compared to women without these symptoms. However, the increased odds of institutional delivery among women with antenatal depressive symptoms was associated with unplanned delivery care use mainly due to emergency reasons (aOR = 1.62, 95% CI: 1.09, 2.42) rather than planning to deliver in healthcare institutions.
Conclusion
Improved detection and treatment of antenatal depression has the potential to increase planned institutional delivery and reduce perinatal complications, thus contributing to a reduction in maternal morbidity and mortality.
Keywords: Antenatal depressive symptoms, Delivery care use, Postnatal care use, Assisted delivery, Planned institutional delivery, Ethiopia
Background
Depressive disorders constitute a public health challenge that contributes a substantial proportion of years lived with disability, globally [1, 2]. In World Health Organization (WHO) Global health estimates, depressive disorders were single largest contributors to non-fatal health loss with more than 80% of this non-fatal disease burden in Low and Middle Income Countries (LMICs) [3]. In the general population, depression is associated with a number of adverse impacts, including poorer quality of life [4], physical ill-health [2, 4], reduced adherence to medical recommendations [5, 6], increased use of health care services [7] arising because of increased medically unexplained symptoms [5], reduced social support, increased worries [8], co-morbid illness [5], and increased health risk behaviours and reduced self-care [9].
Among perinatal women, depression is additionally associated with particular adverse public health consequences [2, 10–14] such as adverse effects on perinatal outcomes and the growth, health and development of the child [1, 15, 16], as well as adverse effects on maternal health. During pregnancy, depression has multiple negative effects independent of postnatal depression [1, 15, 16] and is highly prevalent, with estimates ranging from 10 to 20% [17–22] worldwide, while higher prevalence levels are reported in LMICs (20%–39%) [17, 18, 23–27]. Most maternal deaths (99% of global maternal deaths) occur in LMICs [28, 29] due to undetected and/or inadequately treated complications such as infection, haemorrhage, unsafe abortion, hypertension and obstructed labour [28, 30–33]. These complications are mostly preventable by improving the uptake of maternal health care services [34, 35] in general, and through the improvement of skilled delivery in health care facilities, in particular [36–40]. The WHO has proposed skilled institutional delivery as a key strategy towards reducing maternal deaths across the globe [41].
Established factors associated with institutional delivery in Ethiopia are higher levels of education for the woman [34, 37, 38, 42–44] or her partner [29, 34], better socioeconomic status [43], urban residence [34, 37, 38, 43, 45, 46], previous experience of attending antenatal care [34, 37, 43, 47], increased women’s autonomy [48, 49], media exposure, and prior experience of obstetric complications [50, 51]. However, the impact of maternal depression on women’s use of maternal health care has received little attention in the literature. The authors were only able to identify one relevant study from Ghana [22] where no association was found between antenatal depression and uptake of institutional delivery, although the analysis did not control for important confounders, such as comorbid medical conditions and obstetric complications.
Investigating the potential impact of antenatal depressive symptoms on uptake of delivery care and postnatal care utilisation is essential to design future intervention strategies in LMIC settings, where perinatal outcomes are poor [52] and prevalence of antenatal depressive symptoms high [19, 21]. We hypothesized that antenatal depressive symptoms would, independent of socio-economic and demographic factors, reduce uptake of institutional delivery and postnatal care due to several behavioural features associated with depression: loss of motivation and interest in common activities including self-care [9]; reduced social support [8], increased cognitive deficit to make decisions and evaluate alternatives [53] and reduced adherence to healthcare practitioner recommendations [5, 6]. Thus, improved detection and treatment of antenatal depressive symptoms, albeit not prioritized [54], is hypothesized to shift these behavioural manifestations and thus increase rates of planned institutional delivery and improve maternal and perinatal outcomes.
Thus, this study aimed to investigate prospectively the association between women’s antenatal depressive symptoms, uptake of institutional delivery (planned and unplanned), and postnatal care utilisation after controlling for socioeconomic, demographic, obstetric and medical factors.
Methods
Study design and setting
A population-based, prospective study was conducted in Sodo District, located in the Southern Nations, Nationalities and People’s Region (SNNPR) of Ethiopia. The district has 54 rural and four urban sub-districts (“kebeles”), the smallest administrative unit in Ethiopia. The official language of the region and the district is Amharic. An estimate of about 161,000 people (79,000 men; 82,000 women) resided in Sodo in 2007. The majority of the inhabitants belong to the Sodo Gurage ethnic group (85%), with the remaining population being mostly Oromo and Amhara in ethnicity [52]. Agriculture is the main economic activity within the region.
Cohort identification
The cohort was formed by recruiting all consenting pregnant women in the district in their second and third trimester of pregnancy, between early September and end of November 2014. In the current Ethiopian healthcare system, community based health workers (Health Extension Workers, HEWs) are tasked with community health prevention and promotion activities. They are also tasked with identification and monitoring of pregnant women and to keep accurate and up-to-date maternal records in health posts (frontline primary healthcare facility staffed by HEWs).
In support of these activities, HEWs coordinate with the health development army, a community-based network of health education volunteers, each of whom covers five families. The members of the health development armies are required to notify HEWs of all pregnant women in their respective areas. In this study, HEWs, members of health development armies, kebele chairmen and pregnant women themselves acted as key informants to identify all pregnant women in their respective sub-districts. Through home to home visits of identified women, the data collectors obtained informed consent from potential participants and conducted the baseline interviews. A minimum of three visits were carried out before considering participants ‘unavailable’ or ‘unidentifiable’.
Eligibility criteria for participation in the study included: (1) being in the second or third trimester of pregnancy; (2) continuously resident in the area for a minimum of 6 months; (3) no hearing or cognitive impairment that would affect their capacity to communicate adequately; (4) giving informed consent.
Sample size
Sample size was estimated using EpiInfo version 7 [55] assuming a statistical power of 80% with a two tailed 5% margin of error; 11.7% of institutional delivery utilization among women without antenatal depression [52]; a 10% difference between women with and without antenatal depressive symptoms, which was assumed to be clinically significant. A three to one ratio for women with and without antenatal depressive symptoms was used based on the rates of antenatal depression cited in the literature for LMICs settings [17–19, 23–25]. On this basis, the target sample size was 1174 pregnant women (294 with antenatal depressive symptoms and 880 women without antenatal depressive symptoms). However, all 1311 antenatal baseline participants (356 with antenatal depressive symptoms and 955 without antenatal depressive symptoms) formed the cohort for this study [56].
Data collection and quality control
Data collection was conducted by trained interviewers using an Amharic version of the questionnaires. Forty experienced data collectors and four supervisors were trained for 2 days by the main coordinator of the study (TB) on administration of the instruments, objectives of the study and ethical issues. Training methods included lectures, demonstrations and role-plays. TB closely monitored and supervised the conduct of the study through weekly meetings with the data collectors and supervisors. Completed questionnaires were checked carefully for consistency, adherence to instructions and missing data, first by the supervisors and then by the coordinator and data entry clerks. The data were double entered using EpiData version 3.1 [55] while data collection was proceeding. Completed questionnaires deemed missing or inconsistent were returned back to data collectors for investigation and correction. Data reporting was made in adherence to a STROBE statement checklist [57] to maintain standard of reporting for cohort data.
Measurement
Outcome variables
Main outcomes were whether delivery occurred in a healthcare institution or at home without skilled birth attendatnt; (2) whether delivery in a healthcare setting was planned or unplanned and (3) whether postnatal care was utilized. The outcome variables were prospectively assessed at a median of 8 weeks postpartum (interquartile range of 6–11 weeks postpartum) using the lay interviewer-administered questionnaires. The delivery setting was dichotomized into home delivery vs. institutional delivery. The method of delivery was dichotomised as spontaneous vaginal delivery (SVD) or assisted delivery (instrumental vaginal delivery or Caesarean Section). Women who delivered in health care institutions were also asked whether this had been planned, or had arisen “due to prolonged labour”, and or “due to referral linked to complications” (the latter two responses were subsequently coded as ‘unplanned’). Postnatal care utilization was rated positive if there was at least one visit to a health care professional within 4 weeks of delivery.
Primary exposure
The primary exposure was the occurrence of depressive symptoms antenatally. A locally validated Amharic version of the Patient Health Questionnaire (PHQ-9) [58] was used to screen for antenatal depressive symptoms at baseline, during the second and third trimesters of pregnancy. In studies from high-income countries, the cut-off scores indicating possible major depressive disorder cluster around 10 points [59], however, validation studies of the PHQ-9 in rural areas of low-income countries of sub-Saharan Africa, have found a lower optimal cut-off point. In Ethiopia, the PHQ-9 has been validated in antenatal women and in primary care settings in the neighbouring district of the current study, with the optimal cut-off point indicating probable depression identified as 5 or more in primary care attendees [60]. In a community sample of postnatal women in Ghana, the optimal cut-off to indicate probable depression was also 5 or more [22]. Therefore, in this study, a PHQ score of 5 or more was taken to indicate probable antenatal depression.
Potential confounders
Potential confounding variables were reviewed from the literature and assessed at baseline, during the second and third trimesters of pregnancy. A five item scale, the Women’s Abuse Screening Test (WAST) [61, 62] was used to assess intimate partner violence (IPV). WAST was chosen for its brevity and the acceptability of the wording. A score of one or more on WAST indicates women who have experienced IPV [61, 62]. A three item scale, the Oslo Social Support scale (OSS-3) [63], was used to assess social support. The OSS-3 scale has been used in a community based study in the same setting [64].
Questions from the 2011 Ethiopian Demographic Health Survey (EDHS) were used to collect information on previous stillbirth, spontaneous abortion, neonatal and infant mortality, and comorbid medical conditions, including HIV, tuberculosis, renal or cardiac diseases, hypertension, anaemia or gastritis. Pregnancy intention was coded as ‘intended’ if the woman intended the pregnancy to happen; ‘mistimed’ if the woman would have preferred the pregnancy to have happened at a future date and ‘unwanted’ if the woman did not want to be pregnant at all. The number of antenatal care (ANC) visits was also asked and it was adjusted to gestational age by dividing the number of actual ANC visits by expected number of ANC contacts for a given gestation [one, two, three and four ANC contacts were expected for women at 16th, 28th, 32nd and 40th weeks of gestation respectively based on WHO recommendations [41]]. Birth preparedness was also assessed using items taken from EDHS and other similar studies that asked mothers whether they had planned the means of transport, prepared a delivery kit, identified a health facility and obtained the money required for expenses during delivery [50, 52, 65].
A seven-item scale was used to assess the accessibility of health care facilities for women. This tool assessed the level of difficulty, distance to reach the nearest health facility, and travel time taken as well as affordability and availability of health facilities [66]. Pregnancy complications were assessed using a list of key danger signs during pregnancy as obtained from the EDHS [52]. Close-ended questions were used to assess socio-demographic and socio-economic variables, including residence, marital status, estimated monthly income and educational level of participants.
Data analysis
Stata version 13.1 (Stat Corp, 2013) was used to analyse the data. Monthly income was divided into tertiles and labelled as “high”, “medium”, and “low” income categories. The profile of exposures and outcomes was described using simple descriptive summary values. The number of women lost to follow up was 4.6% including missing data in outcome variables of seven women (Fig. 1). Thus, complete case analysis was used as it was suggested that less than 5% lost to follow up was of little concern [67, 68].
Fig. 1.
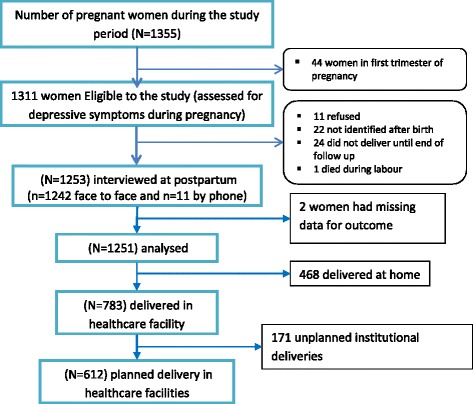
A diagram of sample recruitment procedure
Binary logistic regression was used to examine the association between antenatal depressive symptoms and the outcome variables. Bayesian Information Criterion (BIC) test was used to test model goodness of fit as a result of which ‘number of ANC visits’ was removed from two models. Socio-demographic and socioeconomic variables, interpersonal and life adversities (IPV, lack of social support), obstetric and medical conditions (experience of adverse perinatal outcomes, pregnancy complications, comorbid medical conditions, pregnancy intention, experience of institutional delivery and birth preparedness) were included in all analyses as potential confounders.
Ethical considerations
Ethical approval (ref. number: 024/14/psy dated 23/03/14) was obtained from the Institutional Review Board of the College of Health Sciences, Addis Ababa University. Women with a very high level of depressive symptoms (PHQ-9 ≥ 15) and those with suicidal ideation, as assessed by a particular item in the PHQ-9, were referred to health centres to access free primary care-based mental health services. Women with a PHQ-9 score above the validated cut off were not referred to health care facilities to avoid causing unnecessary concern among women with false positive symptoms, as the PHQ-9, as a screening tool, has low positive predictive validity [58, 69, 70].
Results
From a baseline of 1311 pregnant participants, a total of 1251 women were prospectively interviewed (n = 1240 face to face and n = 11 by phone) about their delivery setting, method of delivery and postnatal care utilization with a response rate of 95.5% (Fig. 1). Women who were in the baseline sample were not significantly different from women who were in the follow-up sample with respect to selected baseline variables (Table 1).
Table 1.
Characteristics of participants (N = 1251)
| Characteristics | Baseline (N = 1311) N (%) |
Followed Up (N = 1251) N (%) |
chi2 (p-value) | |
|---|---|---|---|---|
| PHQ Status | PHQ < 5 | 924 (70.5) | 892 (71.3) | 0.2098 (p = 0.647 |
| PHQ ≥ 5 | 387 (29.5) | 359 (28.7) | ||
| Marital Status | Married | 1293 (98.6) | 1235 (98.7) | |
| single, divorced or widowed | 18 (1.4) | 16 (1.3) | 0.0432 (p = 0.835) | |
| Residence | Urban | 103 (7.9) | 101 (8.1) | 0.0411 (p = 0.839) |
| Rural | 1208 (92.1) | 1150 (91.9) | ||
| Household Income* | High | 459 (35.0) | 438 (35.0) | |
| Medium | 423 (32.3) | 397 (31.7) | 0.1109 (p = 0.946) | |
| Low | 429 (32.7) | 416 (33.3) | ||
| Mother’s Education | Non-literate | 878 (67.0) | 844 67.5) | |
| Primary Schooling (Grade 1–8) | 380 (29.0) | 357 (28.5) | 0.0714 (p = 0.965) | |
| Grade 9 & more | 53 (4.0) | 50 (4.0) | ||
| Experience of Intimate Partner Violence | None | 573 (43.7) | 552 (44.1) | 0.0453 (p = 0.831) |
| One or more in life time | 738 (56.3) | 699(55.9) | ||
| Pregnancy Intention | Wanted | 734 (56.0) | 701 (56.0) | |
| Mistimed (wanted but not now) | 102 (7.8) | 93 (7.4) | 0.1168 (p = 0.943) | |
| Unwanted | 475 (36.2) | 457 (37.3) | ||
| Self-reported Pregnancy Complications | None | 655 (50.1) | 632 (50.5) | 0.0594 (p = 0.808) |
| One or more | 656 (49.9) | 619 (49.5) | ||
| Chronic Illness | None | 871 (66.4) | 824 (66.4) | 0.0001(0 = 0.994) |
| One or more | 440 (33.6) | 416 (34.6) | ||
| Previous institutional delivery | Yes | 160 (12.2) | 152 (12.2) | 0.0018 (p = 0.967) |
| No/primiparous | 1151 (87.8) | 1099 (87.8) | ||
| Delivery Care Utilisation | Home delivery | -- | 468 (37.4) | -- |
| Institutional delivery | -- | 783 (62.6) | -- | |
| Type of Delivery | Normal vaginal | -- | 1115 (89.1) | -- |
| Assisted or operative | -- | 136 (10.7) | -- | |
| One or more Postnatal care Visits: | No | -- | 568 (45.8) | -- |
| Yes | -- | 672 (54.2) | -- | |
| Reason for use of inst. delivery | Planned | -- | 612 (78.3) | -- |
| Unplanned | -- | 171 (21.7) | -- | |
Single Marital Status = unmarried, widowed, divorced
*Income was categorized into tertiles as low, medium and high
CS Caesarian Section
Characteristics of the participants
Most women were married (98.7%), were rural residents (91.9%) and were illiterate (67.5%). Nearly two thirds of women (62.6%) delivered in health institutions. Over half of the women (55.6%) reported experiencing some form of intimate partner violence in their life time and 43.8% had an unintended pregnancy (7.3% mistimed and 37.3% unwanted) (Table 1).
Antenatal depressive symptoms and institutional delivery
High levels of antenatal depressive symptoms (PHQ score 5 or higher) were found in 28.7% of participating women. In the adjusted model (Table 2), women with high levels of antenatal depressive symptoms had increased odds of delivering in health care institutions [adjusted Odds Ratio (aOR) =1.42, 95% Confidence Interval (CI): 1.06, 1.92] independent of pregnancy complications and comorbid medical conditions. Increased access to a health care facility (aOR = 1.10, 95% CI: 1.04, 1.16), primary level education (compared to no education) (aOR = 1.51, 95% CI: 1.10, 2.08), having a previous delivery in a health care institution (aOR = 2.21, 95% CI: 1.36, 3.58) and increased birth preparedness (aOR = 1.32, 95% CI: 1.20, 1.46) were also associated with increased odds of institutional delivery. Rural residence (aOR = 0.39, 95% CI: 0.18, 0.89) and increasing parity (aOR = 0.90, 95% CI: 0.84, 0.97) were associated with reduced odds of institutional delivery.
Table 2.
Use of Institutional Delivery care as a function of antenatal depressive symptoms
| Variables | Odds of Institutional delivery (vs. home) (n = 1251) | Odds of unplanned Institutional delivery (vs. Planned)(n = 783) | ||
|---|---|---|---|---|
| (cOR, 95% CI) | (aOR, 95% CI) | (cOR, 95% CI) | (aOR, 95% CI) | |
| Depressive Symptoms: PHQ9 ≥ 5 | 1.09 (0.85, 1.41) | 1.42 (1.06, 1.92)* | 1.57 (1.10, 2.35)* | 1.62 (1.09, 2.42)* |
| Access to Health Facility | 1.16 (1.10, 1.22)** | 1.10 (1.04, 1.16)* | 0.97 (0.90, 1.04) | 0.99 (0.91, 1.07) |
| Marital Status: Single | 0.77 (0.28, 2.07) | 0.70 (0.24, 2.06) | 0.45 (0.06, 3.60) | 0.37 (0.04, 3.10) |
| Residence: Rural | 0.13 (0.06, 0.27)** | 0.39 (0.18, 0.89)* | 1.02 (0.60, 1.72) | 0.78 (0.39 1.56) |
| Household Income: | ||||
| Low | 1 | 1 | 1 | 1 |
| Medium | 1.13 (0.85, 1.49) | 0.89 (0.65, 1.20) | 1.44 (0.95, 2.19) | 1.67 (1.07, 2.60)* |
| High | 1.31 (0.99, 1.73) | 1.05 (0.77, 1.45) | 1.03 (0.68, 1.58) | 1.37 (0.86, 2.18) |
| Educ. Level: | ||||
| Illiterate | 1 | 1 | 1 | 1 |
| Primary Schooling | 2.25 (1.71, 2.95)** | 1.51 (1.10, 2.08)* | 0.70 (0.48, 1.02) | 0.65 (0.41, 1.01) |
| ≥ Secondary | 19.01 (4.59, 78.71** | 3.99 (0.87, 18.27) | 0.73 (0.34, 1.55) | 0.57 (0.22, 1.51) |
| Intimate Partner violence | 0.97 (0.94, 1.01) | 0.97 (0.93, 1.02) | 0.98 (0.92, 1.04) | 0.95 (0.89, 1.02) |
| Social Support | 1.01 (0.95, 1.07) | 0.95 (0.88, 1.01) | 0.90 (0.83, 0.98)* | 0.93 (0.85, 1.02) |
| Institutional Delivery of previous baby: Yes | 3.62 (2.30, 5.68)** | 2.21 (1.36, 3.58)* | 1.15 (0.93, 1.43) | 1.39 (0.85, 2.26) |
| Birth Preparedness | 1.5(1.32, 1.56)** | 1.32 (1.20, 1.46)** | 0.81 (0.72, 0.92)* | 0.81 (0.71, 0.93)* |
| Parity (Birth Order) | 0.83 (0.79, 0.88)** | 0.90 (0.84, 0.97)* | 1.00 (0.92, 1.08) | 0.93 (0.83, 1.03) |
| Pregnancy Intention: | ||||
| Wanted | 1 | 1 | 1 | 1 |
| Mistimed | 0.62 (0.40, 0.96)* | 0.70 (0.44, 1.11) | 0.86 (0.42, 1.77) | 0.87 (0.41, 1.83) |
| Unwanted | 0.64 (0.51, 0.82)** | 0.84 (0.64, 1.11) | 1.03 (0.71, 1.48) | 0.95 (0.63 1.43) |
| Symptoms of Pregnancy Comp.: ≥1 | 0.88 (0.70, 1.11) | 0.88 (0.68, 1.15) | 1.16 (0.83, 1.64) | 1.01 (0.69, 1.47) |
| Comorbid medical conditions: ≥1 | 1.32 (1.04, 1.67)* | 1.23 (0.95, 1.59) | 0.99 (0.70, 1.39) | 0.96 (0.67, 1.38) |
*significant at <0.05, **significant at <0.001
Access to health care facility score: minimum = 5; Maximum = 15; Mean = 11.98; SD = 2.40
Birth Preparedness score: Minimum = 0; Maximum = 4; Mean = 1.61; SD = 1.42
Intimate Partner violence score: minimum = 9; Maximum = 16; Mean = 2.14; SD = 2.88
Social support score: minimum = 3; Maximum = 14; Mean = 10.68; SD = 2.00
Parity score: minimum = 0; Maximum = 12; Mean = 2.74; SD = 2.09
Among women who delivered in healthcare institutions, there was greater odds of unplanned institutional delivery, mainly due to emergency reasons such as prolonged labour and bleeding, among those with antenatal depressive symptoms (aOR = 1.62, 95% CI: 1.09, 2.42) (Table 2). Among other predictors, being in the medium income category (aOR = 1.67, 95% CI: 1.07, 2.60) was associated with increased odds of unplanned institutional delivery while each increment in birth preparedness score (aOR = 0.81, 95% CI: 0.81, 0.71, 0.93) was associated with reduced odds of unplanned institutional delivery as compared with planned institutional delivery.
Method of delivery and antenatal depressive symptoms
After adjusting for potential confounding variables (Table 3), women with antenatal depressive symptoms had increased odds of assisted delivery compared to women without antenatal depressive symptoms (aOR = 1.72, 95% CI: 1.10, 2.69). Factors that remained significantly associated with increased odds of assisted delivery in the adjusted model were increased access to health care facilities (aOR = 1.11, 95% CI: 1.02, 1.22); having a secondary level education (aOR = 2.40, 95% CI: 1.02, 5.67) and having one or more symptoms of pregnancy complications (aOR = 1.54, 95% CI: 1.01, 2.34). Rural residence (aOR = 0.39, 95% CI: 0.21, 0.75) and increasing parity (aOR = 0.72, 95% CI: 0.62, 0.82) were associated with reduced odds of assisted delivery.
Table 3.
Having assisted delivery and use of postnatal care vs antenatal depressive symptoms
| Variables | Assisted delivery vs SVD | Postnatal care use | ||
|---|---|---|---|---|
| (cOR, 95% CI) | (aOR, 95% CI) | (cOR, 95% CI) | (aOR, 95% CI) | |
| Depressive Symptoms: PHQ9 ≥ 5 | 1.31 (0.90, 1.91) | 1.72 (1.10, 2.69)* | 1.12 (0.87, 1.43) | 1.13 (0.85, 1.50) |
| Access to Health Facility | 1.18 (1.09, 1.29)** | 1.11 (1.02, 1.22)* | 1.05 (1.00, 1.10)* | 1.01 (0.96, 1.06) |
| Marital Status: Single | 2.79 (0.89, 8.76 | 2.33 (0.66, 8.17) | 0.74 (0.27, 2.04) | 0.71 (0.24, 2.16) |
| Residence: Rural | 0.18 (0.11, 0.29)** | 0.39 (0.21, 0.75)* | 0.60 (0.39, 0.93)* | 1.42 (0.82, 2.46) |
| Income per family: | ||||
| Low | 1 | 1 | 1 | 1 |
| Medium | 0.91 (0.58, 1.42) | 0.72 (0.45, 1.17) | 0.97 (0.74, 1.28) | 0.91 (0.68, 1.21) |
| High | 1.06 (0.69, 1.62) | 0.80 (0.48, 1.34) | 1.12 (0.86, 1.47) | 0.98 (0.72, 1.33) |
| Educational Level: | ||||
| Illiterate | 1 | 1 | 1 | 1 |
| Primary Schooling | 2.62 (1.78, 3.88)** | 1.29 (0.81, 2.06) | 1.19 (0.92, 1.53) | 1.0 (0.79, 1.43) |
| ≥ Secondary | 10.85 (5.84, 20.16)** | 2.40 (1.02, 5.67)* | 4.03 (1.93, 8.41)** | 3.23 (1.34, 7.77)* |
| Intimate Partner violence | 0.97 (0.91, 1.03) | 0.95 (0.88, 1.02) | 1.09 (2.04, 1.13)** | 1.11 (1.06, 1.16)** |
| Social Support | 1.00 (0.92, 1.09) | 1.03 (0.93, 1.14) | 1.01 (0.95, 1.06) | 0.99 (0.93, 1.05) |
| Institutional Delivery of last baby: Yes | 2.07(1.31, 3.27)* | 1.40 (0.82, 2.37) | - | -- |
| Number of Antenatal Care visits visits adjusted to Gestational Age | -- | -- | 1.72 (1.40, 2.12)** | 1.42 (1.14, 1.76)* |
| Birth Preparedness | 1.21 (1.07, 1.36)* | 1.01 (0.87, 1.17) | 1.32 (1.21, 1.43)** | 1.30 (1.18, 1.42)** |
| Parity | 0.65 (0.58, 0.73)** | 0.72 (0.62, 0.82)** | 0.96 (0.91, 1.02) | 1.01 (0.94, 1.08) |
| Pregnancy Intention: | ||||
| Wanted | 1 | 1 | 1 | 1 |
| Mistimed | 0.62 (0.29, 1.31) | 0.87 (0.39, 1.95) | 1.27 (0.81, 1.99) | 1.26 (0.79, 2.01) |
| Unwanted | 0.54 (0.36, 0.82)* | 1.01 (0.63, 1.62) | 0.80 (0.63, 1.02) | 0.86 (0.66, 1.13) |
| Symptoms of Pregnancy Comp.: ≥1 | 1.48 (1.03, 2.12)* | 1.54 (1.01, 2.34)* | 0.90 (0.72, 1.12) | 0.85 (0.66, 1.10) |
| Comorbid medical conditions: ≥1 | 1.38 (0.96, 1.97) | 1.47 (0.99, 2.19) | 0.94 (0.74, 1.18) | 0.84 (0.66, 107) |
*significant at <0.05, **significant at <0.001
Access to health care facility score: minimum = 5; Maximum = 15; Mean = 11.98; SD = 2.40
Birth Preparedness score: Minimum = 0; Maximum = 4; Mean = 1.61; SD = 1.42
Intimate Partner violence score: minimum = 9; Maximum = 16; Mean = 2.14; SD = 2.88
Social support score: minimum = 3; Maximum = 14; Mean = 10.68; SD = 2.00
Number of ANC visits: minimum = 0; Maximum = 8; Mean = 1.524; SD = 1.50
Parity score: minimum = 0; Maximum = 12; Mean = 2.74; SD = 2.09
Postnatal care utilization and antenatal depressive symptoms
Women having a secondary level education (aOR = 3.23, 95% CI: 1.34, 7.77), increased intimate partner violence (aOR = 1.11, 95% CI: 1.06, 1.16), increased number of antenatal care (ANC) visits (aOR = 1.42, 95% CI: 1.14, 1.76) and an increased birth preparedness score (aOR = 1.30, 95% CI: 1.18, 1.42) had increased odds of having postnatal care visits in both the univariate and adjusted models (Table 3).
Discussion
In this prospective, population-based study from rural Ethiopia, 28.7% of pregnant women were screened to have symptoms of depression. These women had significantly increased odds of unplanned utilisation of institutional delivery care, mostly due to emergency presentations rather than planning to deliver in a healthcare facility. Assisted delivery was also significantly greater in women with antenatal depressive symptoms.
Overall, the prevalence of antenatal depressive symptoms in our study is consistent with studies in Ghana (26.3%) and Cote d’Ivoire (28.3%) which used the same measure [18, 23]. Studies in South Africa [25], Vietnam [17] and Southern Brazil [24] using other screening tools (Self-Reporting Questionnaire and Edinburgh Postnatal Depression Scale) also reported rates of antenatal depressive symptoms of 30–39%.
Prior to the introduction of the health extension programme [71], and until 2011, institutional delivery rates in Ethiopia were very low [52]. Recent trends indicate improving rates, especially in southern Ethiopia, with nearly 50% of women in community-based samples, and nearly three-quarters of women in urbanized areas delivering in health facilities [72–74]. Our study finding that over 60% of women deliver in an institution is in-line with this positive trend.
We hypothesized that antenatal depressive symptoms are associated with a reduction in women’s uptake of institutional delivery through reduced self-care, social support and reduced women’s adherence to healthcare practitioners’ recommendations. In contradiction with our hypothesis, we found a significantly increase in uptake of institutional delivery among women with antenatal depressive symptoms independent of pregnancy complications and comorbid medical conditions. Increased emergencies related to labour complications might explain this contradiction.
The increased odds of assisted delivery and uptake of unplanned institutional delivery among women with antenatal depressive symptoms supports others’ findings that women with depressive symptoms have an increased risk of labour complications [11, 75–77]. We found the main reasons for institutional delivery of women with antenatal depressive symptoms to be emergencies related to labour complications endorsed as ‘prolonged labour’ and or ‘referral due to labour complications’. Our findings reflect those of a study in Ghana where antenatal depression was associated with assisted delivery and other perinatal complications, including prolonged labour, vaginal tears, loss of consciousness, heavy vaginal bleeding, surgery to repair or remove the womb and blood transfusion [22]. Similarly, a previous community based cohort study in Ethiopia [14] and studies in China [78] and Ghana [22] demonstrated that antenatal depression was associated with prolonged labour or non-progressive preterm contractions [76]. Studies in Peru [79] and in Finland [80] also demonstrated increased odds of preeclampsia among women with antenatal depression while studies in California [77] and Canada [76] demonstrated increased odds of infection among this group of women. These perinatal complications are thus, more likely to increase unplanned institutional delivery and assisted delivery among women with depressive symptoms. There are also biological explanations for the association of depression with perinatal complications. In these explanations, depression is purported to hyper stimulate Hypothalamus-Pituitary-Adrenal (HPA) axis to produce hormones that have adverse effects on the uterine environment [81–83].
Furthermore, studies have demonstrated that women with antenatal depressive symptoms are more likely to have somatic complaints, co-morbid medical conditions [6, 84] and other perinatal complications [12, 14, 85, 86] as well as increased fear of childbirth and worries about death and survival during labour [8, 87] which may increase the likelihood of institutional deliveries in this group.
Our study showed that rural residence was associated with reduced odds of institutional delivery and reduced odds of having assisted delivery, while increased access to health care was associated with increased odds of institutional delivery and having an assisted delivery. These results support consistently findings from others’ work [34, 37, 38, 43, 45, 46, 73, 88, 89]. Increased parity was associated with reduced odds of institutional delivery and assisted delivery, which is also consistent with other local studies [45, 46, 88, 89]. This may be due to decreased likelihood of prolonged labour with increase in parity.
The strength of our study is that it was prospective and used a locally validated measure of depressive symptoms. Selection bias was also minimized in this population-based study as a robust method was used to identify all cases during the study period. However, we cannot be entirely certain if all eligible participants in the district were identified during the time period of the study. Respondent recall bias was minimized by measuring outcome variables within 6–11 weeks of birth. Furthermore, a broader range of confounders such as pregnancy complication and comorbid illnesses were controlled in our models.
Our study did not however, consider the cultural beliefs of women regarding seeking postnatal care. This is pertinent in rural Ethiopia where women are not encouraged to leave their homes until 2–3 weeks postpartum. This might explain the non-significant finding in the association between antenatal depressive symptoms and postnatal care utilization. Because of the low predictive value of PHQ-9 [69, 70], as a screening tool, it is likely that a proportion of PHQ-9 positive women do not meet criteria for a diagnosis of depression. Nonetheless, we found an important association of antenatal depressive symptoms with maternal health care utilization.
Conclusion
Among women with antenatal depressive symptoms, there was increased odds of institutional delivery in general, and increased unplanned institutional delivery utilisation mainly due to emergency reasons. Assisted delivery was also increased among this group of women, which might have been due to labour complications. Thus, improved detection and treatment of antenatal depression has the potential to increase planned institutional delivery and reduce perinatal complications, thus contributing to a reduction in maternal morbidity and mortality, as well as improved neonatal health.
Acknowledgements
We are grateful to Professor Martin Prince, Professor Larry Wissow and Dr. Rosie Mayston for their valuable comments while the study design was being developed. We gratefully acknowledge the support of the Sodo District Health Bureau. The project was supported by a special grant from the PRIME project. Special thanks to all of the participants of this study.
Funding
The study was supported through the small grants initiative of the Programme for Improving Mental healthcare (PRIME) provided to TB from the Department of International Development (PO 5248). However, the funding body did not play any role in the design of study, data collection, interpretation of data or in writing or submission of the manuscript.
Availability of data and materials
The datasets generated and analysed during the current study are not publicized at present. (1) Data were collected as part of a cross-country study and will be available for further cross-country work; (2) This was also part of a PhD project and the student needs to use the data for his PhD work before data could be made available; (3) We have not received consent from participants to share the data on the web but, will be available from the corresponding author on reasonable request.
Authors’ contributions
Involved in the development of the proposal: TB, CH, AF, EK. Participated in data collection: TB, CH, AF. Participated in analysis: TB, CH, AF, SH, MO. Prepared the draft: TB, AF, CH, SH, MO. Revised drafts of the paper: TB, AF, CH, EK, SH, MO. All authors have read and approved the final version of this manuscript.
Authors’ information
TB: PhD fellow in Mental Health Epidemiology, Department of Psychiatry, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; Department of Psychology, Institute of Education and Behavioral Sciences, Debre Markos University, Debre Markos, Ethiopia.
AF: Associate Professor of Psychiatry (MD, PhD, MRCPsych), Addis Ababa University, Addis Ababa, Ethiopia.
CH: Associate Professor of Psychiatry (MD, PhD, MRCPsych), Addis Ababa University, Addis Ababa, Ethiopia.
EK: Assistant professor of obstetrics and gynecology (MD), Addis Ababa University, Addis Ababa, Ethiopia.
SH: Director of Perinatal Mental Health Project (MD), Alan J. Flisher Centre for Public Mental Health, Department of Psychiatry and Mental Health, University of Cape Town, South Africa.
MO: Perinatal Mental Health Project (MPH), Alan J. Fisher Centre for Public Mental Health, Department of Psychiatry and Mental Health, University of Cape Town, South Africa.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Ethical approval (ref. number: 024/14/psy dated 23/03/14) was obtained from the Institutional Review Board of the College of Health Sciences, Addis Ababa University. Written consent (with thumb prints for non-literates) was obtained from all participants after explanation about the study. Women with very high level of depressive symptoms (PHQ-9 ≥ 15) and those with suicidal ideation, as assessed by an item in the PHQ-9, were referred to health centres to access free primary care-based mental health services.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- ANC
Antenatal Care
- aOR
adjusted Odds Ratio
- CI
Confidence Interval
- cOR
crude Odds Ratio
- CS
Caesarian Section
- LMIC
Low and Middle Income Countries
- SVD
Spontaneous Vaginal Delivery
- WHO
World Health Organization
Contributor Information
Tesera Bitew, Phone: +251 911 17 36 56, Email: tesera2016@gmail.com.com.
Charlotte Hanlon, Email: charlotte.hanlon@kcl.ac.uk.
Eskinder Kebede, Email: eskinderkebede@yahoo.com.
Simone Honikman, Email: simone.honikman@uct.ac.za.
Michael N. Onah, Email: Michael.onah@uct.ac.za
Abebaw Fekadu, Email: abe.wassie@kcl.ac.uk.
References
- 1.Bonari L, Pinto N, Einarson A, Steinereir M, Koren G. Perinatal risks of untreated depression during pregnancy. Can J Psychiatr. 2004;49(11):726–735. doi: 10.1177/070674370404901103. [DOI] [PubMed] [Google Scholar]
- 2.Senturk V, Hanlon C, Medihin G, Dewey M, Araya M, Alem A, Prince M, Stewart R. Impact of Perinatal somatic and common mental disorder symptoms on functioning on Ethiopian women: the P-MaMiE population based cohort study. J Affect Disord. 2012;136:340–349. doi: 10.1016/j.jad.2011.11.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.WHO . Depression and other common mental disorders: global health estimates. Geneva: WHO; 2017. [Google Scholar]
- 4.Noel P, Williams J, Unutzer J, Worchel J, Lee S, Cornell J, et al. Depression and comorbid illness in elderly primary care patients: impact on multiple domains of health status and well-being. Ann Fam Med. 2004;2(6):555–562. doi: 10.1370/afm.143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.DiMatteo R, Lepper H, Croghan T. Depression is a risk factor for noncompliance with medical treatment meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160:2101–2107. doi: 10.1001/archinte.160.14.2101. [DOI] [PubMed] [Google Scholar]
- 6.Katon W. Epidemiology and treatment of depression in patients with chronic medical illness. Dialogues Clin Neurosci. 2011;13(1):7–23. doi: 10.31887/DCNS.2011.13.1/wkaton. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Beekman A, Deeg D, Braam A, Tilburg W. Consequences of major and minor depression in later life : a study of disability, well-being and service utilization. Psychol Med. 1997;27:1397–1409. doi: 10.1017/S0033291797005734. [DOI] [PubMed] [Google Scholar]
- 8.Hanlon C, Whitley R. Wondimagegn D, Alem a, Prince M. Between life and death: exploring the socio-cultural aspect of antenatal mental distress in rural Ethiopia. Arch Womens Ment Health. 2010;13(5):385–393. doi: 10.1007/s00737-010-0149-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Carney R, Freedlanda K, Millerb G, Jaffec A. Depression as a risk factor for cardiac mortality and morbidity a review of potential mechanisms. J Psychosom Res. 2002;53:897–902. doi: 10.1016/S0022-3999(02)00311-2. [DOI] [PubMed] [Google Scholar]
- 10.Andersson L, Sundstrom-Poromaa I, Wulff M, Astrom M, Bixo M. Implications of antenatal depression and anxiety for obstetric outcome. Obstet Gynecol. 2004;104(3):467–476. doi: 10.1097/01.AOG.0000135277.04565.e9. [DOI] [PubMed] [Google Scholar]
- 11.Dayan J, Creveuil C, Herlicoviez M, Herbel C, Baranger E, Savoye C, et al. Role of anxiety and depression in the onset of spontaneous preterm labor. Am J Epidemiol. 2002;155(4):293–301. doi: 10.1093/aje/155.4.293. [DOI] [PubMed] [Google Scholar]
- 12.Grigoriadis S, VanderPorten E, Mamisashvili L, Tomlinson G, Dennis C. Et a. The impact of maternal depression during pregnancy on perinatal outcomes: a systematic review and meta-analysis. J Clin Psychiatry. 2013;74(4):321–341. doi: 10.4088/JCP.12r07968. [DOI] [PubMed] [Google Scholar]
- 13.Grote N, Bridge J, Gavin A, Melville J, Iyengar S, Katon W. A meta-analysis of depression during pregnancy and the risk of preterm birth, low birth weight, and intrauterine growth restriction. Arch Gen Psychiatry. 2010;67(10):1012–1024. doi: 10.1001/archgenpsychiatry.2010.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hanlon C, Medihin G, Alem A, Tesfaye F, Lakew Z, Worku B. Impact of antenatal common mental disorders upon perinatal outcomes in Ethiopia: the P-MaMiE population-based cohort study. Trop Med Int Health. 2008;14(2):156–166. doi: 10.1111/j.1365-3156.2008.02198.x. [DOI] [PubMed] [Google Scholar]
- 15.Rahman A, Bunn J, Lovel H, Creed F. Association between antenatal depression and low birthweight in a developing country. Acta Psychiatr Scand. 2007;115:481–486. doi: 10.1111/j.1600-0447.2006.00950.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Stein A, Pearson R, Goodman S, Rapa E, Rahman A, McCallum M, et al. Effects of perinatal mental disorders on the fetus and child. Lancet. 2014;384:1800–1819. doi: 10.1016/S0140-6736(14)61277-0. [DOI] [PubMed] [Google Scholar]
- 17.Fisher J, Tran T, La B, Kriitma K, Rossenthal D, Tran T. Common perinatal mental disorders in northern Viet Nam: community prevalence and health care use. Bull World Health Organ. 2010;88:737–745. doi: 10.2471/BLT.09.067066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bindt C, Appiah-Poku J, Te Bonle M, Schoppen S, Feldt T, Barkmann C, et al. Antepartum depression and anxiety associated with disability in African women: cross-sectional results from the CDS study in Ghana and cote d'Ivoire. PLoS One. 2012;7(10):48396. doi: 10.1371/journal.pone.0048396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dibaba Y, Fantahun M, Hindin M. The association of unwanted pregnancy and social support with depressive symptoms in pregnancy: evidence from rural southwestern Ethiopia. BMC Pregnancy Childbirth. 2013;13:135. doi: 10.1186/1471-2393-13-135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Shakya R, Situala S, Shyangwa P. Depression during pregnancy in a tertiary care center of eastern Nepal. J Nepal Med Assoc. 2008;47(171):128–131. [PubMed] [Google Scholar]
- 21.Medihin G, Hanlon C, Dewey M, Alem A, Tesfaye F, Lakew Z, et al. The effect of maternal common mental disorders on infant undernutrition in Butajira, Ethiopa: P-MaMiE study. BMC Psychiatry. 2010;10:32. doi: 10.1186/1471-244X-10-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Weobong B, Asbroek A, Soremekun S, Manu A, Owusu-Agyei S, Prince M, et al. Association of antenatal depression with adverse consequences for the mother and newborn in rural Ghana: findings from the don population-based cohort study. PLoS One. 2014;9(12):e116333. doi: 10.1371/journal.pone.0116333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Guo N, Bindt C, Te Bonle M, Appiah-Poku J, Koffi M, Posdzich S, et al. Association of antepartum and postpartum depression in Ghanaian and Ivorian women with febrile illness in their offspring: a prospective birth cohort study. Am J Epidemiol. 2013;178(9):1394–1402. doi: 10.1093/aje/kwt142. [DOI] [PubMed] [Google Scholar]
- 24.Anselmi L, Barros F, Minten G, Gigante D, Horta B, Victora C. Prevalence and early deteminants of common mental disorders in the 1982 birth cohort, Pelotas, South Brazil. Rev Saude Publica. 2008;42(12):26–33. doi: 10.1590/S0034-89102008000900005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hartley M, Tomlinson M, Greco E, Comulada S, Stewart J, Roux J, Mbewu N, Rotheram-Borus N. Depressed mood in pregnancy: prevalence and correlates in two Cape town peri-urban settlements. Reprod Health. 2011;8:9. doi: 10.1186/1742-4755-8-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Fisher J, Mello M, Patel V, Rahman A, Tran T, Holtn S, et al. Prevalence and determinants of common perinatal mentala disorders in low income and lower middle income countries: a systematic review. Bull World Health Organ. 2012;90:139–149. doi: 10.2471/BLT.11.091850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lancaster C, Gold K, Flynn H, Yoo H, Marcus S, Davis M. Risk factors for depressive symptoms during pregnancy: a systematic review. Am J Obstet Gynecol. 2010;202(1):5–14. doi: 10.1016/j.ajog.2009.09.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Say L, Chou D, Gemmill A, Tuncalp O, Moller A, Daniels J, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Global Health. 2014;2(6):323–333. doi: 10.1016/S2214-109X(14)70227-X. [DOI] [PubMed] [Google Scholar]
- 29.WHO . Trends in maternal mortality: 1990 to 2015. Geneva: The Maternal Mortality Estimation Inter-Agency Group; 2015. [Google Scholar]
- 30.Ahmed F, Moussa K, Petterson K, Asamoah B. Assessing knowledge, attitude, and practice of emergency contraception: a cross- sectional study among Ethiopian undergraduate female students. BMC Public Health. 2012;12:110. doi: 10.1186/1471-2458-12-110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Alemayehu M, Belachew T, T T. Factors associated with utilization of long acting and permanent contraceptive methods among married women of reproductive age in Mekelle town, Tigray region, north Ethiopia. BMC Pregnancy Childbirth. 2012;12:6. doi: 10.1186/1471-2393-12-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Mersha A, Jira C, Demessie S. Community based study on maternal mortality in Jimma town, south western Ethiopia. Indian J Public Health. 1996;40(2):30–34. [PubMed] [Google Scholar]
- 33.Khan K, Wojdyla D, Say L, Gülmezoglu M, Van L. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006;367:1066–1074. doi: 10.1016/S0140-6736(06)68397-9. [DOI] [PubMed] [Google Scholar]
- 34.Amano A, Gebeyehu A, Birhanu Z. Institutional delivery service utilization in Munisa Woreda, south East Ethiopia: a community based cross-sectional study. BMC Pregnancy Childbirth. 2012;12:105. doi: 10.1186/1471-2393-12-105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Costello A, Azad K, Barnett S. An alternative strategy to reduce maternal mortality. Lancet. 2006;368:1477–1479. doi: 10.1016/S0140-6736(06)69388-4. [DOI] [PubMed] [Google Scholar]
- 36.Worku A, Fantahun M. Factors affecting utilization of skilled maternal care in Northwest Ethiopia: a multilevel analysis. BMC Int Health Hum Rights. 2013;13:20. doi: 10.1186/1472-698X-13-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Abebe F. Factors associated with home delivery in Bahirdar, Ethiopia: a case control study. BMC Res Notes. 2012;5:653. doi: 10.1186/1756-0500-5-653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Abera M, G/mariam A, Belachew T. Predictors of safe deliery serice utilizion in Arsi zone, south-East Ethiopia. Ethiop J Health Sci 2011;21:95-106. [PMC free article] [PubMed]
- 39.Teferra A, Alemu F, Woldeyohannes S. Institutional delivery service utilization and associated factors among mothers who gave birth in the last 12 months in Sekela District, north west of Ethiopia: a community - based cross sectional study. BMC Pregnancy Childbirth. 2012;12:74. doi: 10.1186/1471-2393-12-74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Worku A, Yalew A, Afework M. Maternal complications and women’s behavior in seeking care from skilled providers in north gondar, Ethiopia. PLoS One. 2013;8(3):e60171. doi: 10.1371/journal.pone.0060171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.WHO . Trends in maternal mortality: 1990 to 2010. Geneva: WHO; 2012. [Google Scholar]
- 42.Regassa N. Antenatal and postnatal care service utilization in southern Ethiopia: a population-based study. Afr Health Sci. 2011;11(3):390–397. [PMC free article] [PubMed] [Google Scholar]
- 43.Mengesha Z, Biks G, Ayele T, Tessema G, Koye D. Determinants of skilled attendance for delivery in northwest Ethiopia: a community based nested case control study. BMC Public Health. 2013;13:130. doi: 10.1186/1471-2458-13-130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Mekonnen M, Yalew K, Umer J, Melese M. Determinants of delivery practices among afar pastoralists of Ethiopia. Pan Afr Med J. 2012;13:17. [PMC free article] [PubMed] [Google Scholar]
- 45.Mekonnon Y, Mekonne A. Factors influencing the use of maternal healthcare services in Ethiopia. J Health Popul Nutr. 2003;21(4):374–382. [PubMed] [Google Scholar]
- 46.Fikre A, Demissie M. Prevalence of institutional delivery and associated factors in Dodota Woreda (district), Oromia regional state, Ethiopia. Reprod Health. 2012;9:33. doi: 10.1186/1742-4755-9-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Tsegay Y, Gebrehiwot T, Goicolea I, Edin K, Lemma H, Sebastian MS. Determinants of antenatal and delivery care utilization in Tigray region, Ethiopia: a cross-sectional study. Int J Equity Health. 2013;12(1):30. doi: 10.1186/1475-9276-12-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Aktar S. Healthcare seeking behavior for safe motherhood: findings from rural Bangladesh. Bangladesh e-J Sociol. 2012;9(2):57–70. [Google Scholar]
- 49.Woldemichael G. Women's autonomy and maternal health seeking behvior in Ethiopia. Matern Child Health J. 2010;14(6):988–998. doi: 10.1007/s10995-009-0535-5. [DOI] [PubMed] [Google Scholar]
- 50.Kabakyenga J, Östergren P, Turyakira E, Pettersson K. Knowledge of obstetric danger signs and birth preparedness practices among women in rural Uganda. Reprod Health. 2011;8:33. doi: 10.1186/1742-4755-8-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Mekonnen Y. Patterns of maternity care service utilization in southern Ethiopia: evidence from a community and family survey. Ethiop J Health Dev. 2003;17(1):27–33. doi: 10.4314/ejhd.v17i1.9779. [DOI] [Google Scholar]
- 52.CSA . Ethiopia demographic and health survey 2011. Addis Ababa: Central Statistical Authority; 2011. [Google Scholar]
- 53.Calderon J, Flores P, Babul M, Aguirre JM, Slachevsky A, Padilla O, et al. Systemic lupus erythematosus impairs memory cognitive tests not affected by depression. Lupus. 2014;23(10):1042–1053. doi: 10.1177/0961203314536247. [DOI] [PubMed] [Google Scholar]
- 54.Baron E, Hanlon C, Mall S, Honikman S, Breuer E, Kathree T, et al. Mental health in primary care in five low and middle income countries: a situtational analysis. BMC Health Serv Res. 2016;16(53):1293–1316. doi: 10.1186/s12913-016-1291-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.CDC . Advanced management and analysis of data using EpiInfo for windows. 2000. [Google Scholar]
- 56.Bitew T, Hanlon C, Kebede E, Medihn G, Fekadu A. Antenatal depressive symptoms and maternal health care utilisation: a population-based study of pregnant women in Ethiopia. BMC Pregnancy Childbirth. 2016;16:301. doi: 10.1186/s12884-016-1099-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Von Elm E, Altman D, Egger M, Pocock S, Gøtzsche P, Vandenbroucke J. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Epidemiology. 2007;18(6):800–804. doi: 10.1097/EDE.0b013e3181577654. [DOI] [PubMed] [Google Scholar]
- 58.Kroenke K, Spitzer R, Wiliams J. Validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–613. doi: 10.1046/j.1525-1497.2001.016009606.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Manea L, Gilbody S, McMillan D. Optimal cut-off score for diagnosing depression with the patient health questionnaire (PHQ-9): a meta-analysis. CMAJ. 2012;184(3):191–196. doi: 10.1503/cmaj.110829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Hanlon C, Medhin G, Selamu M, Breuer E, Worku B, Hailemariam H, et al. Validity of brief screening questionnaires to detect depression in primary care in Ethiopia. J Affect Disord. 2015;186:32–39. doi: 10.1016/j.jad.2015.07.015. [DOI] [PubMed] [Google Scholar]
- 61.Rabin R, Jennings J, Campbell J, Bair-Merritt M. Intimate partner violence screening tools. Am J Prev Med. 2009;36(5):439–445. doi: 10.1016/j.amepre.2009.01.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Zink T, Levin L, Putnam F, Beckstrom A. Accuracy of five domestic violence screening questions with nongraphic language. Clin Pediatr. 2007;46(2):127–134. doi: 10.1177/0009922806290029. [DOI] [PubMed] [Google Scholar]
- 63.Boen H. Characteristics of senior centre users – and the impact of a group programme on social support and late-life depression. Norsk Epidemiologi. 2012;22(2):261–269. doi: 10.5324/nje.v22i2.1574. [DOI] [Google Scholar]
- 64.Fekadu A, Medhin G, Selamu M, Hailemariam M, Alem A, Giorgis T, et al. Population level mental distress in rural Ethiopia. BMC Psychiatry. 2014;14:194. doi: 10.1186/1471-244X-14-194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.JHPIEGO. Monitoring birth preparedness and complication readiness tools and indicators for maternal and newborn health. Maternal and Neonatal Health. 2004. http://reprolineplus.org/resources/monitoring-birth-preparedness-and-complication-readiness-tools-and-indicators-maternal-and (199.230.115.126). Accessed 26 June 2017.
- 66.Fotso J, Mukiira C. Perceived quality of and access to care among poor urban women in Kenya and their utilization of delivery care: harnessing the potential of private clinics? Health Policy Plan. 2011:1–11. [DOI] [PubMed]
- 67.Fewtrell M, Kennedy K, Singhal A, Martin R, Ness A, Hadders-Algra M, et al. How much loss to follow up is acceptable in long terp randomized controlled trials and prospective studies. Arch Dis Child. 2008;93(6):458–461. doi: 10.1136/adc.2007.127316. [DOI] [PubMed] [Google Scholar]
- 68.Kristman V, Manno M, Cotte P. Loss to follow-up in cohort studies: how much is too much? Eur J Epidemiol. 2004;19:751–760. doi: 10.1023/B:EJEP.0000036568.02655.f8. [DOI] [PubMed] [Google Scholar]
- 69.Gelaye B, Williams M, Lemma S, Deyessa N, Bahretibeb Y, Shibre T, et al. Validity of the patient health questionnaire-9 for depression screening and diagnosis in East Africa. Psychiatry Res. 2013; [DOI] [PMC free article] [PubMed]
- 70.Hanlon C, Medihin G, Selamu M, Breuer E, Worku B, Hailemariam M, et al. Validity of brief screening questionaire to detect depression in primary care in Ethiopia. J Affect Disord. 2015;186:32–39. doi: 10.1016/j.jad.2015.07.015. [DOI] [PubMed] [Google Scholar]
- 71.El-Saharty S, Kebede S, Olango P, Siadat B. Ethiopia: Improving health service delivery. Health, Nutrition, Population Discussion Papeer. 2009. http://siteresources.worldbank.org/HEALTHNUTRITIONANDPOPULATION/Resources/281627-1095698140167/EthiopiaHealthSystemDelivery.pdf. Accessed 26 June 2017.
- 72.Daniel O, Desalegn S. Institutional delivery service utilization and associated factors among child bearing age women in Goba woreda. Ethiopia J Gynecol Obstet. 2014;2(4):63–70. doi: 10.11648/j.jgo.20140204.14. [DOI] [Google Scholar]
- 73.Gedefaw A, Muluken A, Tesfaye S. Factors associated with institutional delivery service utilization among mothers in Bahir Dar City administration, Amhara region: a community based cross sectional study. Reprod Health. 2014;11:22. doi: 10.1186/1742-4755-11-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Hailemichael F, Woldie M, Tafese F. Predictors of institutional delivery in Sodo town, southern Ethiopia. Afr J Prm Health Care Fam Med. 2013;5(1):544. [Google Scholar]
- 75.Jablensky A, Morgan V, Zubrick S, Bower C, Yellachich L. Pregnancy, delivery, and neonatal complications in a population cohort of women with schizophrenia and major affective disorders. Am J Psychiatry. 2005;162(1):79–91. doi: 10.1176/appi.ajp.162.1.79. [DOI] [PubMed] [Google Scholar]
- 76.Lutsiv O, McKinney B, Foster G, Taylor V, Pullenayegum E, McDonald S. Pregnancy complications associated with the co-prevalence of excess maternal weight and depression. Int J Obes. 2015;39:1710–1716. doi: 10.1038/ijo.2015.119. [DOI] [PubMed] [Google Scholar]
- 77.Thornton D, Guendelman S, Hosang N. Obstetric complications in women with diagnosed mental illness: the relative success of California’s county mental health system. Health Serv Res. 2010;45:1. doi: 10.1111/j.1475-6773.2009.01058.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Qiao Y, Wang J, Li J, Wang J. Effects of depressive and anxiety symptoms during pregnancy on pregnant, obstetric and neonatal outcomes: a follow-up study. J Obstet Gynaecol. 2012;32:237–240. doi: 10.3109/01443615.2011.647736. [DOI] [PubMed] [Google Scholar]
- 79.Qiu C, Sanchez S, Lam N, Garcia P, Williams M. Associations of depression and depressive symptoms with preeclampsia: results from a Peruvian case-control study. BMC Womens Health. 2007;7:15. doi: 10.1186/1472-6874-7-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Kurki T, Hiilesmaa V, Raitasalo R, Mattila H, Ylikorkala O. Depression and anxiety in early pregnancy and risk for preeclampsia. Obstet Gynecol. 2000;95:487–490. doi: 10.1016/s0029-7844(99)00602-x. [DOI] [PubMed] [Google Scholar]
- 81.Chrousos G, Torpy D, P G. Interactions between the hypothalamic-pituitary-adrenal axis and the female reproductive system: clinical implications. Ann of Intern Med. 1998;129:229–240. doi: 10.7326/0003-4819-129-3-199808010-00012. [DOI] [PubMed] [Google Scholar]
- 82.Sandman C, Wadhwa P, Dunkel-Schetter C, Chicz-DeMet A, Belman J, ao PM. Psychobiological influences of stress and HPA regulation on the human fetus and infant birth outcomes. Ann N Y Acad Sci. 1994;739:198–210. doi: 10.1111/j.1749-6632.1994.tb19822.x. [DOI] [PubMed] [Google Scholar]
- 83.Smith R, Cubis J, Brinsmead M, Lewin T, Singh B, ao OP. Mood changes, obstetric experience and alterations in plasma cortisol, beta-endorphin and corticotrophin releasing hormone during pregnancy and the puerperium. J Psychosom Res. 1990;34(1):53–69. doi: 10.1016/0022-3999(90)90008-R. [DOI] [PubMed] [Google Scholar]
- 84.Katon J, Russo J, Gavin A, Melville J, Katon W. Diabetes and depression in pregnancy: Is there an association?. Journal of Women's Health. 2011;20(7):983–9. [DOI] [PMC free article] [PubMed]
- 85.Benute G, Nomura R, Siracuza R, Fraguas R, Jr, Lucia M, Zugaib M. Depression during pregnancy in women with a medical disorder: risk factors and perinatal outcomes. Clinics. 2010;65(11):1127–1131. doi: 10.1590/S1807-59322010001100013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Zeleke B, Ayele T, Woldetsadik M, Bisetegn T, Adane A. Depression among women with obstetric fistula, and pelvic organ prolapse in northwest Ethiopia. BMC Psychiatry. 2013;13:236. doi: 10.1186/1471-244X-13-236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Stewart R, Umar E, Gleadow-Ware S, Creed F, Bristow K. Perinatal distress and depression in Malawi: an exploratory qualitative study of stressors, supports and symptoms. Arch Womens Ment Health. 2015;18:177–185. doi: 10.1007/s00737-014-0431-x. [DOI] [PubMed] [Google Scholar]
- 88.Geneti K. Statistical analysis of determinants of maternal institutional delivery service utilization in Ethiopia. Am J Theoretical App Stat. 2015;4(3):71–77. doi: 10.11648/j.ajtas.20150403.11. [DOI] [Google Scholar]
- 89.Fekadu M, Regassa N. Skilled delivery care service utilization in Ethiopia: analysis of rural-urban differentials based on national demographic and health survey (DHS) data. Afr Health Sci. 2014;14(4):974–984. doi: 10.4314/ahs.v14i4.29. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated and analysed during the current study are not publicized at present. (1) Data were collected as part of a cross-country study and will be available for further cross-country work; (2) This was also part of a PhD project and the student needs to use the data for his PhD work before data could be made available; (3) We have not received consent from participants to share the data on the web but, will be available from the corresponding author on reasonable request.