

Abstract
Purpose
To provide evidence-based, resource-stratified global recommendations to clinicians and policymakers on the management and palliative care of women diagnosed with invasive cervical cancer.
Methods
ASCO convened a multidisciplinary, multinational panel of cancer control, medical and radiation oncology, health economic, obstetric and gynecologic, and palliative care experts to produce recommendations reflecting resource-tiered settings. A systematic review of literature from 1966 to 2015 failed to yield sufficiently strong quality evidence to support basic- and limited-resource setting recommendations; a formal consensus-based process was used to develop recommendations. A modified ADAPTE process was also used to adapt recommendations from existing guidelines.
Results
Five existing sets of guidelines were identified and reviewed, and adapted recommendations form the evidence base. Eight systematic reviews, along with cost-effectiveness analyses, provided indirect evidence to inform the consensus process, which resulted in agreement of 75% or greater.
Recommendations
Clinicians and planners should strive to provide access to the most effective evidence-based antitumor and palliative care interventions. If a woman cannot access these within her own or neighboring country or region, she may need to be treated with lower-tier modalities, depending on capacity and resources for surgery, chemotherapy, radiation therapy, and supportive and palliative care. For women with early-stage cervical cancer in basic settings, cone biopsy or extrafascial hysterectomy may be performed. Fertility-sparing procedures or modified radical or radical hysterectomy may be additional options in nonbasic settings. Combinations of surgery, chemotherapy, and radiation therapy (including brachytherapy) should be used for women with stage IB to IVA disease, depending on available resources. Pain control is a vital component of palliative care. Additional information is available at www.asco.org/rs-cervical-cancer-treatment-guideline and www.asco.org/guidelineswiki. It is the view of ASCO that health care providers and health care system decision makers should be guided by the recommendations for the highest stratum of resources available. The guideline is intended to complement but not replace local guidelines.
INTRODUCTION
The purpose of this guideline is to provide expert guidance to clinicians and policymakers in all resource settings on work-up, treatment, and palliative care for women diagnosed with invasive cervical cancer. The target population is women who have been diagnosed with cervical cancer.
There are large disparities regionally and globally in incidence of and mortality resulting from cervical cancer, in part because of disparities in the provision of mass screening. (A separate ASCO resource-stratified guideline provides guidance on screening.) Treatment of cervical cancer is dependent on the stage of disease. Treatment may include surgical treatments such as conization, hysterectomy or radical hysterectomy, radiation therapy, and/or chemotherapy. Different regions of the world, both among and within countries, differ with respect to access to these treatments. In particular, regions with fewer resources tend to have poorer screening programs, and patients present with more advanced disease that requires either radical surgery or chemoradiotherapy, neither of which is readily available in these areas. For this reason, standard guidelines that assume ideal availability of surgery and radiotherapy may not be applicable. The goal of our guideline is to recommend options in settings in which ideal treatment regimens may not be available.
Approximately 85% of incident cervical cancers occur in less developed regions (also known as low- and middle-income countries [LMICs]) around the world, representing 12% of women’s cancers in those regions. Eighty-seven percent of deaths resulting from cervical cancer occur in these less developed regions.1 Some of the regions in the world with the highest mortality rates include the WHO South-East Asia and Western Pacific regions, followed by India and Africa.1 As a result of these disparities, the ASCO Resource-Stratified Guideline Advisory Group chose cervical cancer as a priority topic for guideline development.
Disparities exist not only among countries and global regions but also within countries. For example, within the United States, some regions have higher incidences of cervical cancer (eg, Texas, 9.2; Arkansas, 9.8; and Mississippi, 9.7 per 100,000 women)2 as well as rates of poverty greater than 17%.3 In the United States, black women experience higher incidence and mortality than women of other races or ethnicities.2 Awareness of these disparities in access to care should be considered in the context of this clinical practice guideline, and health care providers should strive to deliver the highest level of cancer care to all women.
ASCO has established a process for resource-stratified guidelines, which includes mixed methods of guideline development, adaptation of the clinical practice guidelines of other organizations, and formal expert consensus. This article summarizes the results of that process and presents resource-stratified recommendations, which are based, in part, on expert consensus and adaptation from the Canadian Cancer Care Ontario (CCO),4,5 European Society of Medical Oncology (ESMO),6 Japan Society of Gynecologic Oncology (JSGO),7 US National Comprehensive Cancer Network (NCCN),8 and multinational WHO9 guidelines for the care and palliation of women with invasive cervical cancer. Appendix Table A1 lists links to these guidelines.
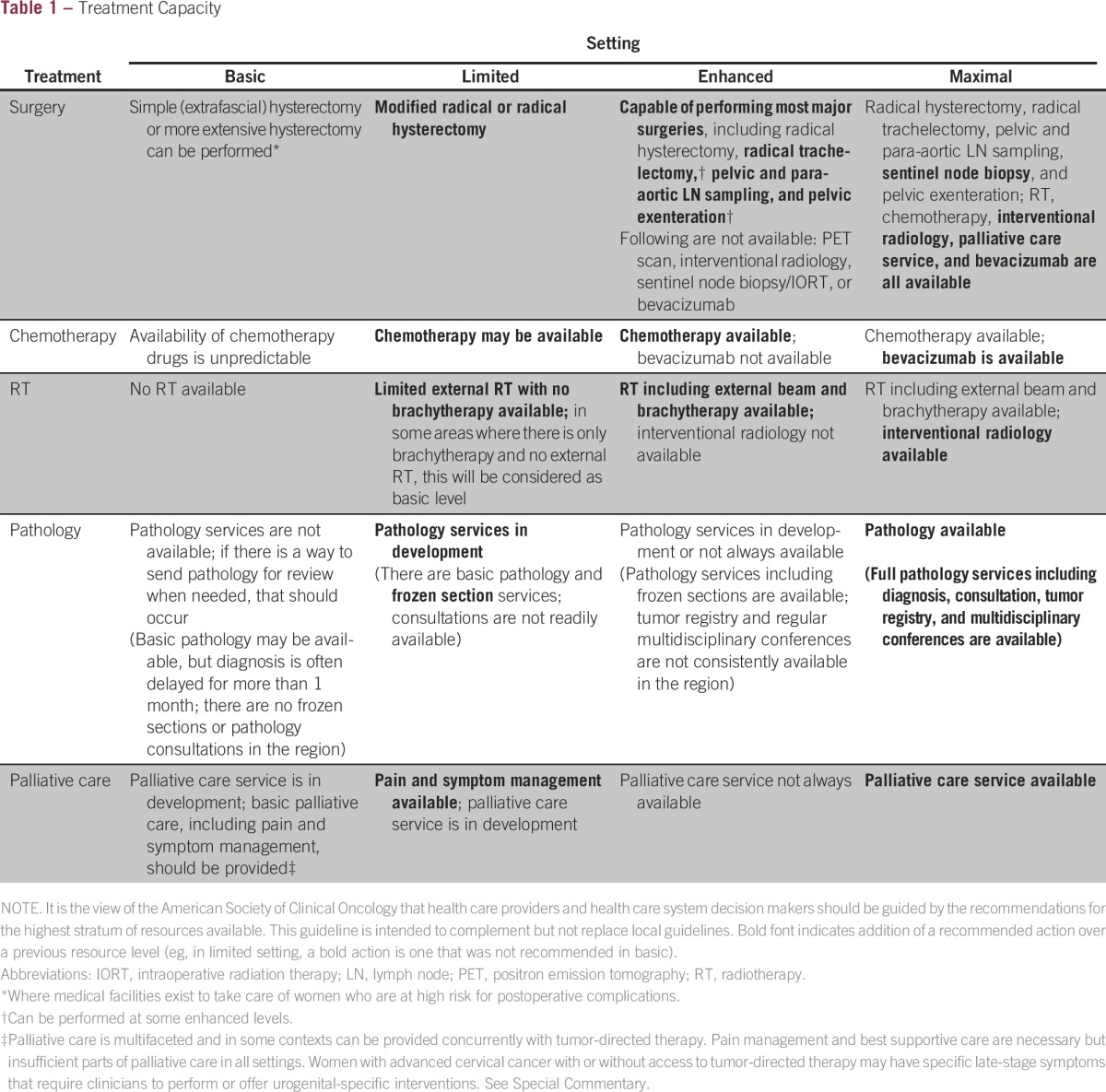
This ASCO guideline reinforces selected recommendations offered in the CCO, ESMO, JSGO, NCCN, and WHO guidelines and acknowledges the effort put forth by the authors and aforementioned societies to produce evidence-based and/or consensus-based guidelines informing practitioners and institutions caring for patients with invasive cervical cancer. In developing resource-stratified guidelines, ASCO has adopted its framework from the four-tier approach (basic, limited, enhanced, and maximal, summarized in Table 1 and Appendix Table A2) developed by WHO and applied by the Breast Health Global Initiative and made modifications to that framework based on Disease Control Priorities 3 and uses an evidence-based approach to inform guideline recommendations.10-12
Table 1.
Treatment Capacity
GUIDELINE QUESTIONS
This clinical practice guideline addresses four overarching clinical questions: In the basic-, limited-, enhanced-, and maximal-resource settings, what are the appropriate care options for women with invasive cervical cancer in work-up, treatment, follow-up and post-treatment surveillance, and palliative care?
METHODS
Guideline Development Process
These recommendations were developed by an ASCO Expert Panel with multinational and multidisciplinary representation. The Expert Panel met via teleconference and in person and corresponded through e-mail. On the basis of the consideration of the evidence, the authors were asked to contribute to the development of the guideline, provide critical review, and finalize the guideline recommendations. Members of the Expert Panel were responsible for reviewing and approving the penultimate version of the guideline, which was then circulated for external review and submitted to a peer-reviewed journal for editorial review and consideration for publication. This guideline was partially informed by the ASCO modified Delphi formal expert consensus methodology, during which the Expert Panel was supplemented by additional experts recruited to rate their agreement with the drafted recommendations. The entire membership of experts is referred to as the ASCO Consensus Panel (Data Supplement provides a list of members). All ASCO guidelines are ultimately reviewed and approved by the Expert Panel and the ASCO Clinical Practice Guideline Committee (CPGC) before publication.
The guideline development process was also informed by the ADAPTE methodology13 and consensus processes used together as an alternative to de novo recommendation development for this guideline. However, a special section on radiation therapy in resource-constrained settings does include de novo expert consensus recommendations. Adaptation of guidelines is considered by ASCO in selected circumstances, when one or more guidelines from other organizations already exist on the same topic. The objective of the ADAPTE process is to take advantage of existing guidelines to enhance efficient production, reduce duplication, and promote the uptake of guideline recommendations.
The ASCO adaptation and formal expert consensus processes begin with a literature search to identify literature including candidate guidelines for adaptation. The panel used literature searches (from 1966 to 2015, with additional searches for literature published in specific areas), existing guidelines and expert consensus publications, some observational studies, and clinical experience as guides.
Adapted guideline manuscripts are reviewed and approved by the ASCO CPGC. The review includes two parts: methodologic review and content review. The former was completed by two ASCO staff members and the latter by members of the Expert Panel (Appendix Table A3) convened by ASCO, which included multinational and multidisciplinary representation.
THE BOTTOM LINE
Management and Care of Women With Invasive Cervical Cancer: American Society of Clinical Oncology Resource-Stratified Clinical Practice Guideline
Guideline Question
In basic-, limited-, enhanced-, and maximal-resource settings, what are the appropriate care options for women diagnosed with invasive cervical cancer?
Target Population
Women at all levels of resource settings diagnosed with invasive cervical cancer.
Target Audience
This clinical practice guideline globally targets health care providers (including gynecologic oncologists, medical oncologists, radiation oncologists, obstetricians and gynecologists, surgeons, nurses, and palliative care clinicians), policymakers, patients, and caregivers.
Methods
A multinational, multidisciplinary Expert Panel was convened to develop clinical practice guideline recommendations based on a systematic review of the medical literature and/or an expert consensus process.
Author’s note.
It is the view of the American Society of Clinical Oncology (ASCO) that health care providers and health care system decision makers should be guided by the recommendations for the highest stratum of resources available. The guidelines are intended to complement but not replace local guidelines.
Key Points*
If follow-up is available, the Expert Panel recommends cone biopsy for women with stage IA2 disease in basic settings and cone biopsy plus pelvic lymphadenectomy in limited settings. In enhanced and maximal settings, radical trachelectomy is recommended for patients with stage IB1 cervical cancer with tumor size up to 2 cm who desire fertility-sparing surgery.
In basic settings where patients cannot be treated with radiation therapy, extrafascial hysterectomy either alone or after chemotherapy may be an option for women with stage IA1 to IVA cervical cancer.
In basic settings, for women with larger tumors or advanced-stage cervical cancer, neoadjuvant chemotherapy is recommended, whenever chemotherapy is available, for the purpose of shrinking the tumor before performing hysterectomy.
Concurrent radiotherapy and chemotherapy is standard in enhanced and maximal settings for women with stage IB to IVA disease.
The panel stresses the addition of low-dose chemotherapy during radiotherapy but not at the cost of delaying radiation therapy if chemotherapy is not available.
In limited-resource settings where there is no brachytherapy, the ASCO Expert Panel recommends extrafascial hysterectomy or its modification for women who have residual tumor 2 to 3 months after concurrent chemoradiotherapy and additional boost.
For patients with stage IV or recurrent cervical cancer, single-agent chemotherapy (carboplatin or cisplatin) is recommended in basic settings.
If the resources are available and the patient cannot receive treatment with curative intent, palliative radiotherapy should be used to relieve symptoms of pain and bleeding.
Where resources are constrained, single- or short-course radiotherapy schemes can be used with retreatments if feasible for persistent or recurrent symptoms.
Qualifying Statements
ASCO believes that cancer clinical trials are vital to inform medical decisions and improve cancer care and that all patients should have the opportunity to participate.
Palliative care and pain management are part of the treatment of cancers, including cervical cancer, to avoid unnecessary suffering during the final stages of disease. Pain control is a vital component of palliative care, a basic human right often neglected in cancer control programs.
Additional Resources
More information, including a Data Supplement with additional evidence tables, a Methodology Supplement with information about evidence quality and strength of recommendations, slide sets, and clinical tools and resources, is available at www.asco.org/rs-cervical-cancer-treatment-guideline. Patient information is available at www.cancer.net.
*Not all recommendations for all settings are listed. Please see Tables 3-7.
The guideline recommendations were crafted, in part, using the Guidelines Into Decision Support (GLIDES) methodology and accompanying BRIDGE-Wiz software.14 Detailed information about the methods used to develop this guideline is available in the Methodology Supplement and Data Supplement at www.asco.org/rs-cervical-cancer-treatment-guideline.
The ASCO Expert Panel and guideline staff will work with co-chairs to keep abreast of any substantive updates to the guideline. On the basis of a formal review of the emerging literature, ASCO will determine the need to update this guideline. This is the most recent information as of the publication date. Visit the ASCO Guidelines Wiki at www.asco.org/guidelineswiki to submit new evidence.
Guideline Disclaimer
The clinical practice guideline and other guidance published herein are provided by ASCO to assist providers in clinical decision making. The information herein should not be relied upon as being complete or accurate, nor should it be considered as inclusive of all proper treatments or methods of care or as a statement of the standard of care. With the rapid development of scientific knowledge, new evidence may emerge between the time information is developed and when it is published or read. The information is not continually updated and may not reflect the most recent evidence. The information addresses only the topics specifically identified herein and is not applicable to other interventions, diseases, or stages of diseases. This information does not mandate any particular course of medical care. Furthermore, the information is not intended to substitute for the independent professional judgment of the treating provider, because the information does not account for individual variation among patients. Recommendations reflect high, moderate, or low confidence that the recommendation reflects the net effect of a given course of action. The use of words like “must,” “must not,” “should,” and “should not” indicates that a course of action is recommended or not recommended for either most or many patients, but there is latitude for the treating physician to select other courses of action in individual cases. In all cases, the selected course of action should be considered by the treating provider in the context of treating the individual patient. Use of the information is voluntary. ASCO provides this information on an as-is basis and makes no warranty, express or implied, regarding the information. ASCO specifically disclaims any warranties of merchantability or fitness for a particular use or purpose. ASCO assumes no responsibility for any injury or damage to persons or property arising out of or related to any use of this information or for any errors or omissions.
Guideline and Conflicts of Interest
The Expert Panel was assembled in accordance with the ASCO Conflicts of Interest Policy Implementation for Clinical Practice Guidelines (found at www.asco.org/rwc). All members of the panel completed the ASCO disclosure form, which requires disclosure of financial and other interests, including relationships with commercial entities that are reasonably likely to experience direct regulatory or commercial impact as a result of promulgation of the guideline. Categories for disclosure include employment; leadership; stock or other ownership; honoraria; consulting or advisory role; speaker’s bureau; research funding; patents, royalties, other intellectual property; expert testimony; travel, accommodations, expenses; and other relationships. In accordance with the ASCO policy, the majority of the members of the panel did not disclose any relationships constituting a conflict under the policy.
RESULTS
As part of the systematic literature review, PubMed, SAGE, Cochrane Systematic Review, and National Guideline Clearinghouse databases were searched for guidelines, systematic reviews, and meta-analyses published between1966 and January 2015. Additional searches were conducted in PubMed in February, May, July, and August 2015. Inclusion criteria included publications with a population of women with invasive cervical cancer that addressed treatment, follow-up, and/or palliative care and were developed by experts as part of a recognized organizational effort. To inform recommendations for basic- or limited-resource settings, preference was given to studies conducted in these settings.
Searches for cost-effectiveness analyses were also conducted. Articles were excluded from the systematic review if they were meeting abstracts; books, editorials, commentaries, letters, news articles, case reports, or narrative reviews; or publications in a language other than English.
A total of 13 guidelines and seven systematic reviews were found in the literature search.4-7,15-31 On the basis of content and methodology reviews, the Expert Panel chose five sets of guidelines—one from Japan, one from Western Europe, two from Canada, and one from the United States—to form the evidentiary basis for the guideline recommendations.4-7,15-18 In addition, the WHO Palliative Care Chapter (Chapter 7) in the “WHO Guideline on Comprehensive Cervical Cancer Control: A Guide to Essential Practice” was identified and deemed eligible for adaptation.9 An additional eight systematic reviews26-33 and economic analyses34-36 were selected to provide indirect but supporting information to supplement formal consensus.
The identified guidelines were published between 2012 and 2015; however, only one set considered resources (from NCCN). The CCO guidelines were systematic review–based guidelines; the WHO guideline had the largest global constituency, and all the selected guidelines were developed in maximal resource–level settings. Appendix Table A1 lists links to these guidelines, and the Data Supplement provides an overview of these guidelines, including information on their clinical questions, target populations, development methodology, and key evidence.
ASCO METHODOLOGIC REVIEW
The methodologic review of the guidelines was completed by two ASCO guideline staff members using the Rigour of Development subscale of the AGREE II instrument. The score for the Rigour of Development domain is calculated by summing the scores across individual items in the domain and standardizing the total score as a proportion of the maximum possible score. Detailed results of the scoring and the AGREE II assessment process for this guideline are available in the Methodology Supplement.
Searches for evidence on specific aspects (eg, radiation therapy use, treatment in developing countries, conization for small tumors, and lymph node biopsy at the time of hysterectomy performed after chemoradiotherapy) were conducted by ASCO guideline staff to identify relevant randomized clinical trials, systematic reviews, meta-analyses, and guidelines to supplement the original search. The English-language and other inclusion criteria listed under Literature Search were applied to the search results.
FINAL RECOMMENDATIONS
The recommendations were developed by a multinational, multidisciplinary group of experts using evidence from existing guidelines, supplementary literature, and clinical experience as a guide. All recommendations gained formal consensus. The ASCO Expert Panel underscores that health care practitioners who implement the recommendations presented in this guideline should first identify the available resources in their local and referral facilities and endeavor to provide the highest level of care possible with those resources. All providers should provide minimum supportive and palliative care to all patients. Complete recommendations with ratings of evidence and strength of recommendations are listed in Tables 2-6. Recommendations labeled as evidence based are supported by existing guidelines.
Table 2.
Work-Up
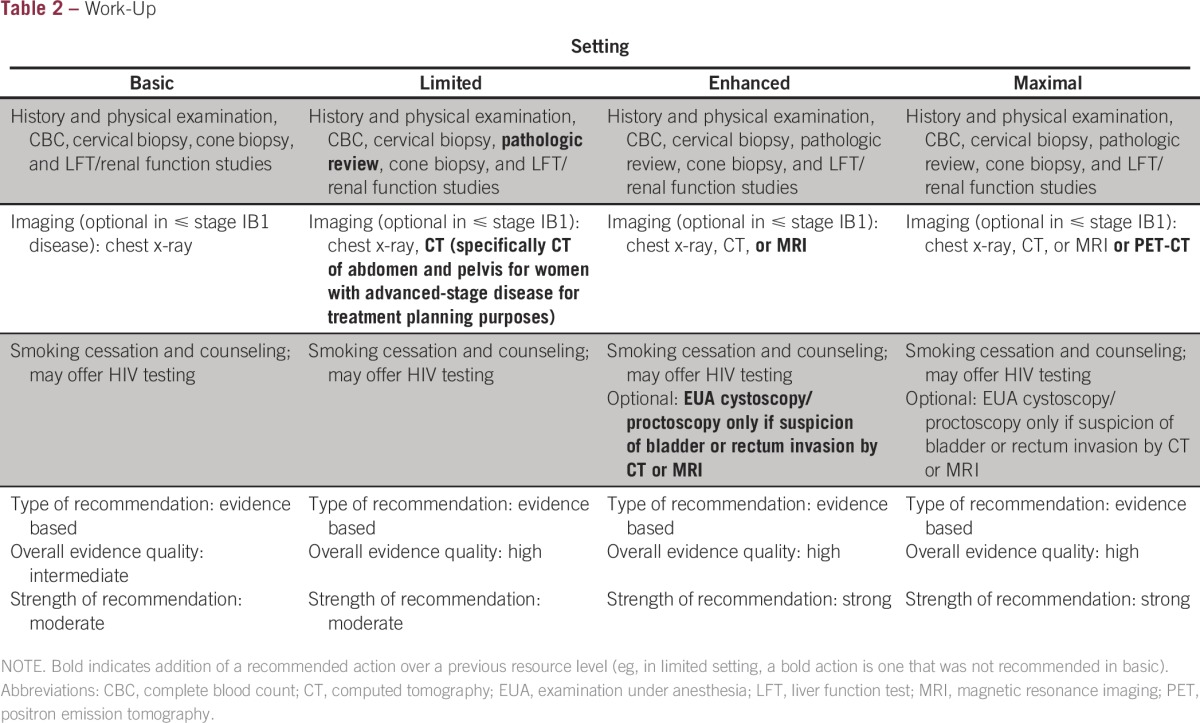
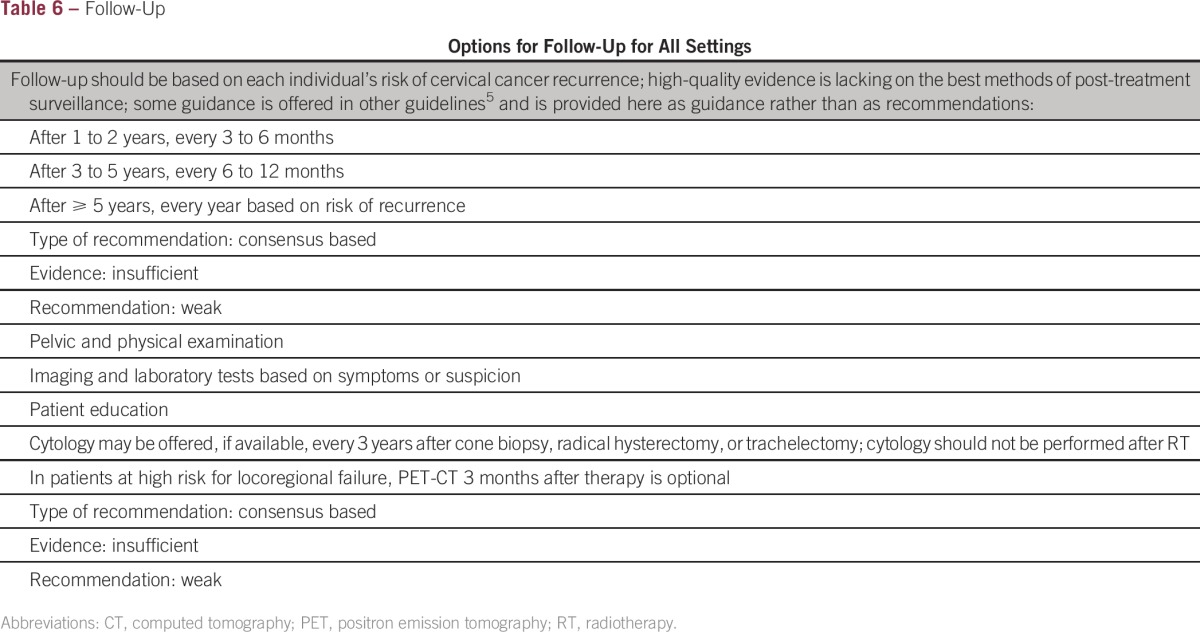
Table 6.
Follow-Up
Work-Up
The purpose of work-up is to assess a patient’s overall health status and gather data to inform treatment. Modalities include history and physical examination, biopsies, blood tests, and imaging. Tests available in maximal settings, such as magnetic resonance imaging or positron emission tomography (PET) –computed tomography (CT), are optional.
Treatment
The treatment of women with invasive cervical cancer consists of surgery, chemotherapy, and radiation therapy, sometimes in combination. The recommendations for women with stage IA1 to IV disease and women with recurrence are listed in Tables 3-5, and selected treatment recommendations are discussed in the following sections.
Table 3.
Recommendations for Stage IA, IB, and IIA Disease

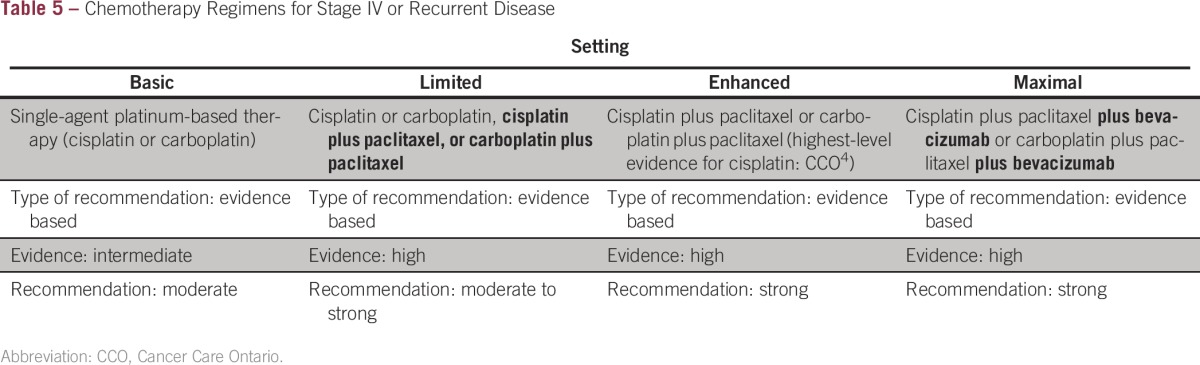
Table 5.
Chemotherapy Regimens for Stage IV or Recurrent Disease
DISCUSSION OF SELECTED TREATMENT ISSUES
Early-Stage and Locally Advanced Disease
Three sets of treatment guidelines from maximal settings recommended radical hysterectomy, pelvic lymphadenectomy, and para-aortic lymph node sampling8 or concurrent chemoradiotherapy6,7 for women with early-stage or locally advanced disease (Table 3). There was no literature to inform practice in the basic setting. Therefore, the panel chose to make consensus recommendations and relied on clinical experience, training, and judgment to formulate these recommendations, given that there were no conclusive data regarding this question.
In contrast to other guidelines, this ASCO resource-stratified guideline addresses settings where there are no or limited personnel with sufficient surgical expertise to perform radical hysterectomies for patients with cervical cancer. For a patient who has early-stage disease (stage IA2, IB1, or IIA1), if the surgeon can remove the tumor safely, with negative margins, the Expert Panel recommends performing extrafascial hysterectomy. In basic settings where surgery capacity is absent or lacking, and patients cannot be treated with radiation therapy, extrafascial hysterectomy may be offered to women with stage IB cervical cancer. For women with stage IA2 or IB1 disease with tumors smaller than 2 cm in size and 1 cm in depth in the non–fertility-sparing setting, studies are ongoing exploring whether cone biopsy or extrafascial hysterectomy with pelvic lymphadenectomy is adequate. For women with larger tumors or advanced-stage cervical cancer, the Expert Panel recommends neoadjuvant chemotherapy (NACT) whenever chemotherapy is available, for the purpose of shrinking the tumor before performing hysterectomy. The specific chemotherapy agents may be carboplatin, cisplatin, or paclitaxel plus carboplatin. There are two randomized phase III trials (EORTC [European Organisation for Research and Treatment of Cancer] 55994 and ClinicalTrials.gov identifier NCT00193739) comparing NACT followed by surgery with chemoradiotherapy in these patients. The EORTC 55994 trial was recently closed for accrual, whereas the NCT00193739 trial is ongoing (more information is provided in Future Directions). Extrafascial hysterectomy may be used for patients with stage IB2 or IIA2 to IIIA disease after NACT.
For women with locally advanced cervical cancer, the role of surgery has been debated for many years. Studies with other comparisons involving hysterectomy after chemoradiotherapy or radiotherapy (with or without brachytherapy) were analyzed in a 2015 Cochrane systematic review, which found little benefit for most women.26
Concurrent radiotherapy and chemotherapy is standard in enhanced and maximal settings for women with stage IB to IVA disease (Tables 3 and 4), as stated by the National Cancer Institute; this is based on seven clinical trials.38 However, the Expert Panel is aware of some negative trials on concurrent chemoradiotherapy regimens. For example, two randomized controlled trials were conducted, neither of which found an overall survival (OS) difference. One of these found a statistically significantly improved disease-free interval.39,40 Therefore, the panel stresses the addition of low-dose chemotherapy during radiotherapy, but not at the cost of delaying radiation therapy if chemotherapy is not available.
Table 4.
Recommendations for Stage IIB, III, IVA, and IVB and Recurrent Disease
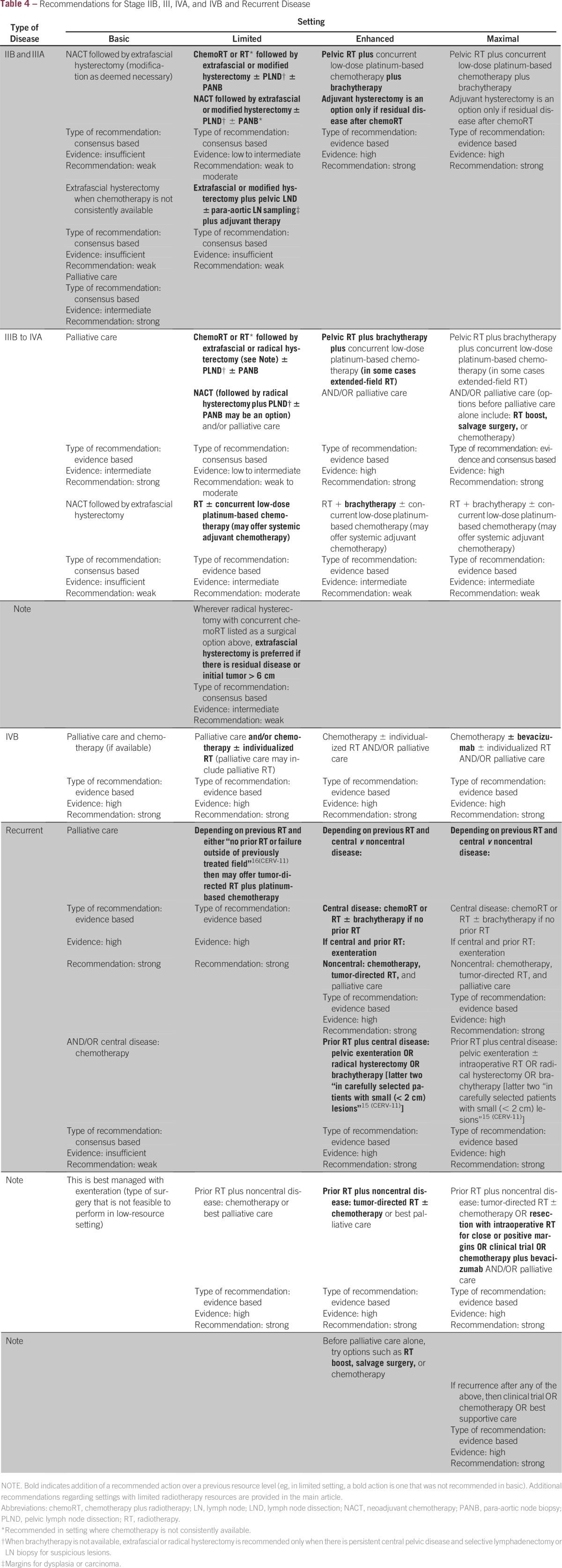
In limited-resource settings, where brachytherapy is not available, the panelists considered a phase III randomized trial involving participants with stage IB2 to IIB cervical cancer, conducted in Mexico, to evaluate if radical hysterectomy and pelvic lymphadenectomy performed after concurrent chemoradiotherapy was equivalent to treatment with brachytherapy.41 The Cochrane review included this trial, which demonstrated equivalent survival and progression-free survival outcomes for women who underwent radical hysterectomy compared with women who were treated with brachytherapy. In that study, 72% (62 of 86) of the patients receiving surgery alone had pathologic complete response, with no residual tumor in the radical hysterectomy specimen.26 Because of the concern of the risks associated with performing radical hysterectomy in limited settings, the ASCO Expert Panel recommends extrafascial hysterectomy or its modification for women who have residual tumor 2 to 3 months after concurrent chemoradiotherapy and additional boost in place of brachytherapy. For some women without these risks factors, the potential harms of surgery may outweigh incremental potential risk factors (informal consensus based on subset analyses of patients with bulky stage IB disease).42 If women do not receive surgery, they should be closely monitored; however, the panel acknowledges the serious issue of loss to follow-up, especially when women lack access to transportation and/or face other high potential opportunity costs to attend follow-up.
The Expert Panel also discussed adjuvant chemotherapy after chemoradiotherapy. The phase III, open-label, randomized study comparing concurrent gemcitabine plus cisplatin and radiotherapy followed by adjuvant gemcitabine and cisplatin versus concurrent cisplatin and radiotherapy in patients with stage IIB to IVA carcinoma of the cervix by Dueñas-González et al43 was the first adjuvant chemotherapy study. In this study, there was improved efficacy in the adjuvant therapy arm but also more adverse events (both statistically significant). The primary outcome was 3-year progression-free survival, which was 74.4% (95% CI, 68% to 79.8%) in the intervention arm versus 65% (95% CI, 58.5% to 70.7%; P = .029). There were more grade 3 to 4 adverse events in intervention arm (eg, neutropenia), and there were two potentially study-related deaths. There is one ongoing trial examining different adjuvant chemotherapy agents: OUTBACK, a phase III trial of adjuvant chemotherapy after chemoradiotherapy as primary treatment of locally advanced cervical cancer compared with chemoradiotherapy alone (ClinicalTrials.gov identifier NCT01414608). This trial is investigating the addition of adjuvant carboplatin and paclitaxel after chemoradiotherapy versus concurrent cisplatin and radiotherapy in patients with stage IB to IVA carcinoma of the cervix. An additional phase III trial of concurrent chemotherapy and pelvic irradiation with or without adjuvant carboplatin and paclitaxel is open for high-risk patients with stage IA2, IB, or IIA cervical carcinoma after radical hysterectomy (RTOG [Radiation Therapy Oncology Group] 0724/GOG [Gynecologic Oncology Group] 0724; ClinicalTrials.gov identifier NCT00980954).
Management of women who have early cervical cancer and desire fertility preservation requires careful counseling, because radical trachelectomy requires surgical expertise not usually available in basic or limited settings. Although prospective clinical trials to evaluate the outcomes of cone biopsy and pelvic lymphadenectomy for women with stage IB1 cervical cancer with tumor size smaller than 2 cm are ongoing, retrospective studies have suggested equivalent outcomes can be achieved with the less aggressive approach. If follow-up is available, the Expert Panel recommends cone biopsy for women with stage IA2 disease in basic settings and cone biopsy plus pelvic lymphadenectomy for those in limited settings. In enhanced and maximal settings, radical trachelectomy is recommended for patients with stage IB1 cervical cancer with tumor size up to 2 cm. Because the risk of metastasis increases with tumor size between 2 and 4 cm,44,45 radical trachelectomy and pelvic lymphadenectomy have been performed after NACT in the research setting, but there is no conclusive evidence to support their routine use. Complete hysterectomy may be used in patients with stage IB disease with high risk factors, including positive margins and lymph node metastasis.46 (The presence of lymphovascular space invasion [LVSI] is one of the three highest risk factors for disease recurrence. Radical trachelectomy may be considered if only one of these risk factors is present. See definitions of Sedlis et al37 regarding risk factors under Definition.)
The Expert Panel recommends pelvic lymphadenectomy in the enhanced and maximal settings for the purpose of fertility preservation; this is based on the current evidence for patients with stage IA1 to IA2 disease and positive LVSI. Fertility sparing is recommended as an option clinicians should offer to women in their reproductive years (up to approximately 45 years of age) and with a desire for fertility preservation. The ASCO guideline on fertility preservation discusses these issues in depth.47 That guideline states for conservative gynecologic surgery, “it has been suggested that radical trachelectomy (surgical removal of the uterine cervix) should be restricted to stage IA2 to IB cervical cancer with diameter < 2 cm and invasion < 10 mm.”47(p2503) For the purposes of the current guideline, the authors suggest that for women with stage IA1 to IA2 disease who are approximately 45 years of age and have a desire for fertility preservation, radical trachelectomy and pelvic lymphadenectomy may be an option in enhanced and maximal settings. Three ongoing clinical trials will help determine if cone biopsy or extrafascial hysterectomy and pelvic lymphadenectomy may have equivalent outcomes for these patients (see Future Directions).
Late-Stage or Advanced Disease
For patients with stage IV or recurrent cervical cancer, single-agent chemotherapy (carboplatin or cisplatin) is recommended in basic settings. The purpose is to minimize the increased toxicity associated with the doublet chemotherapy regimen or to offer treatment when doublet chemotherapy is not readily available and/or there is limited capacity for managing adverse effects women experience from chemotherapy (Table 4). On the basis of the recent report by the JSGO, in which carboplatin plus paclitaxel was not found to be inferior to a cisplatin plus paclitaxel combination, the panel recommends carboplatin as the first-line chemotherapeutic agent; it is associated with a favorable therapeutic index.48 In the Cochrane Database Systematic Review in 2012, single-agent cisplatin resulted in a lower response rate (relative risk [RR], 0.60; 95% CI, 0.44 to 0.81) but was associated with less toxicity when compared with a platinum-based combination, including less serious (grade 3 to 4) neutropenia (RR, 0.04; 95% CI, 0.02 to 0.12) and thrombocytopenia (RR, 0.16; 95% CI, 0.05 to 0.48). Overall survival was longer in the combination versus single-agent group (13 to 15 v 7 to 9 months). In settings where resources are limited, single-agent cisplatin or carboplatin is a reasonable alternative.32 The GOG 240 study reported a 3.7-month survival benefit with the addition of bevacizumab to the combination chemotherapy regimen in patients with advanced or recurrent cervical cancer.49 The Expert Panel recommends the inclusion of this agent with carboplatin or cisplatin and paclitaxel combination in maximal settings, with careful attention to potential toxicities of this regimen. In addition, this guideline contains suggestions on modifications to radiation therapy protocols in limited-resource settings; please see Radiation Therapy in Resource-Constrained Settings.
Lymphadenectomy
Throughout the treatment recommendations, the Expert Panel primarily recommends para-aortic lymph node sampling rather than complete lymphadenectomy; however, if the clinician finds enlarged nodes, he or she may remove those. This is performed for prognostic purposes and does not have therapeutic implications.
RADIATION THERAPY IN RESOURCE-CONSTRAINED SETTINGS
Radiation therapy is a mainstay of cervical cancer treatment. For women with advanced cervical cancer in maximal resource–level settings (≥ bulky stage IB), treatment involves radiotherapy with concurrent platinum-based chemotherapy. This radiotherapy includes both external-beam radiation therapy (EBRT) and brachytherapy. However, radiation therapy is limited or nonexistent in some settings, and there is little evidence to guide clinicians in these situations. In settings with more limited resources, the most appropriate management must depend on the available treatments, including surgical and radiation oncology expertise, available chemotherapy agents, EBRT and brachytherapy equipment, and trained physics and dosimetry personnel. De novo expert consensus–based recommendations on alternative management of patients with cervical cancer in settings with no or limited radiation oncology resources are provided as follows.
Clinical Question R1
Which alternative treatment options can be offered when there is a lack of radiation therapy machines or physics supports?
Recommendation R1A: Basic setting.
As listed in the recommendations table (Table 3), for patients with stage IA cervical cancer, qualified surgeons may perform extrafascial hysterectomy (without LVSI). For larger tumors (stage IB1 to IIA1), if there is surgical expertise, extrafascial hysterectomy or its modification may be performed if the tumor can be removed completely without cutting through gross disease. If chemotherapy is available and the patient’s tumor is too large to remove completely, NACT may be used to shrink the tumor to make it surgically removable. If the patient’s tumor does not shrink and is not resectable with negative margins, palliative measures, including best supportive care, should be used. (This recommendation concurs with the other recommendations [Table 3].)
Recommendation R1B: Limited-resource settings, with limited EBRT and no brachytherapy available.
If chemotherapy is available and the patient’s tumor is too large to remove completely (≥ stage IB2), NACT may be used to shrink the tumor to make it removable by surgery. (Evidence quality: intermediate. Strength of recommendation: moderate. Qualifying statement: There are ongoing trials regarding NACT, and on publication, the Expert Panel may reconsider this recommendation.) Additional adjuvant therapies may potentially be used if risk factors exist on the hysterectomy specimen. If EBRT is available, up to 50 Gy external radiation followed by an additional radiation boost of 18 to 20 Gy (portal size, 10 × 10 or 12 × 12 cm) may be used. (Evidence quality: intermediate. Strength of recommendation: moderate.) Extrafascial hysterectomy or its modification may be performed if there is limited residual tumor on the cervix. (Evidence quality: low. Strength of recommendation: weak.) If the tumor does not shrink after NACT or radiotherapy, palliative measures, including best supportive care, should be used. (Evidence quality: intermediate. Strength of recommendation: strong. Qualifying statement: If a patient has a large inoperable tumor, chemotherapy is available, and it is possible to perform surgery if the tumor shrinks, NACT may be used. If NACT does not shrink the tumor, radical radiation therapy may be used. If after this the tumor does not shrink and/or there is more than limited residual disease and the tumor is inoperable, palliative measures, including best supportive care, should be used.)
Discussion of R1.
With no radiotherapy available in some settings, treatment must rely on other available resources. The Expert Panel is in favor of NACT followed by surgery compared with surgery followed by chemotherapy. In settings where resources are limited, risks associated with surgery in locally advanced cervical cancer may be minimized with the administration of NACT. NACT can frequently shrink tumors, but hysterectomy should be performed only if negative surgery margins can be achieved. The evidence for NACT comes primarily from retrospective studies. There are two ongoing randomized controlled trials comparing NACT plus surgery with chemoradiotherapy, which may inform recommendations regarding NACT in the future.
Clinical Question R2
Which alternative treatment options should be offered where there is limited availability of radiotherapy resources? What is the reasonable minimal fractionation?
Recommendation R2A: Limited setting.
Where the number of patients requiring radiotherapy overwhelms the available EBRT resources, providers may have to triage patients. This would include the whole population and may involve using resources for those with higher likelihood of potential cure. Radiotherapy could possibly be used for palliative treatment in those least likely to be cured. Implementation of these suggestions is dependent on the setting and local conditions. Shorter radiation fractionation schemes with curative intent may be used where resources are constrained. (Evidence quality: intermediate. Strength of recommendation: moderate.)
If surgical expertise is available and there is limited radiotherapy for those with resectable disease, clinicians may potentially perform surgery after NACT. Type of surgery is listed by stage and setting in Table 3 (eg, extrafascial hysterectomy or modified radical hysterectomy plus pelvic lymph node resection if there are positive margins). (Evidence quality: weak. Strength of recommendation: low.)
Recommendation R2B: When brachytherapy is not available or there is residual tumor after radiotherapy.
Ideally, if EBRT and sufficient resources are available and the decision has been made to treat a patient with curative intent, radical irradiation should include an initial whole-pelvic dose of 45 to 50 Gy of EBRT, using 1.8- or 2.0-Gy fractions. If brachytherapy is not available, clinicians should use an external-beam boost up to a dose of 68 to 70 Gy. (Evidence quality: intermediate. Strength of recommendation: moderate.) The field volume for the boost should be reduced so that the superior border is at the lower sacroiliac joint and the volume encompassing residual disease.
In a situation of constrained radiotherapy resources but an intent to provide cure, clinicians may use fewer fractions of radiation in a higher dose per fraction. Where this may result in higher complication rates, the initial pelvic volume to be treated can be reduced (eg, the superior level of the field may be at the inferior S-I joint, because failure is most likely to occur in the low pelvis). (Evidence quality: low. Strength of recommendation: moderate.)
If residual central disease persists in the pelvis at 2 months after treatment completion and there is no overt distant disease, surgery to remove the residuum should be an option. (Evidence quality: low. Strength of recommendation: weak. Qualifying statement: If the surgeon feels that there is a reasonable chance of resecting residual persistent tumor after an incomplete response to radiation therapy, an extrafascial hysterectomy could be attempted. Expert opinion is that in these circumstances, resectability is more likely when the tumor size is < 4 cm in its greatest dimension.)
Recommendation R2C.
If patients have disease with a low likelihood of cure, a palliative approach may be used (ie, limited number of larger-fraction treatments delivered to a smaller field of irradiation [eg, 3.7 Gy twice per day for 2 days, repeated up to 3 times every 2 to 4 weeks] or a single fraction of 8 to 10 Gy, possibly repeated once per month up to 3 times). (Evidence quality: intermediate. Strength of recommendation: moderate.)
Discussion of R2.
In a situation with high volumes of cervical cancer and limited numbers of radiotherapy treatment machines, the goal should be optimizing the use of resources. For patients who cannot adequately be treated with surgery or the combination of NACT and surgery, radiotherapy is the optimal treatment approach. Curative radiotherapy generally consists of 45 to 50 Gy of EBRT, using 1.8- or 2.0-Gy fractions. Brachytherapy, which may not be available in limited-resource settings, is introduced in the third to fifth week of EBRT or after its completion. Once initiated, every effort should be made to complete all treatment in approximately 55 days. Treatment breaks should be avoided, because prolongation of treatment time decreases cure rates. With more patients with cervical cancer to be treated than available radiotherapy machine resources, triaging of patients can be important for improving disease control outcomes for patients with potentially curative disease and maximizing symptom control for patients with advanced disease.
If the resources are available and the patient cannot receive treatment with curative intent, irradiation should be used to relieve symptoms of pain and bleeding (Table 7).33 A single large fraction or palliative approach may be used, as may a limited number of large-fraction treatments delivered to a smaller irradiation field. No phase III data have established an optimal fractionation, but available data as examples of possible fractionation schemes are listed in Table 7.33 The approach used in RTOG 8502 of 3.7 Gy twice per day for 2 days and repeated up to 3 times every 2 to 4 weeks showed 76% and 31% of patients with cervical cancer experiencing significant improvement in bleeding and pain, respectively.50 Although it is commonly taught that higher doses of protracted radiation provide better palliation in terms of symptom relief and duration of such, randomized data in patients with bladder or lung cancer comparing shorter versus longer schedules with higher total doses do not suggest an advantage.33 Therefore, where resources are constrained, single- or short-course schemes can be used with retreatments if feasible for persistent or recurrent symptoms.
Table 7.
Overview of Selected Studies: RT Scheme and Outcome As Proportion of Women With the Complaint

Clinical Question R3A
What should providers do in situations where there is limited brachytherapy?
Recommendation R3A: Limited setting with limited brachytherapy.
No optimal dose per fractionation scheme has been defined. Various schemes are used, most commonly three- to five-dose cervical high-dose rate brachytherapy. The dose per fraction varies with the number used to achieve biologic equivalence (the combined biologically equivalent dose at point A achieved by a combination of EBRT and brachytherapy should ideally approximate 75 to 85 Gy).51 (Evidence quality: high. Strength of recommendation: strong.)
Discussion of R3.
Ideally, definitive cervical irradiation should include brachytherapy; its use shows improved survival and decreased toxicity, but if brachytherapy resources are not available, treatment with an external-beam boost as described in Recommendation R2B should be used. For residual disease 2 months after radiotherapy, surgery may be an option as described in Recommendation R2A.20
In data reported from the United States, although definitive cervical treatment without brachytherapy shows lower survival rates, it does result in long-term survival in some patients. On the basis of US SEER data collected between 1988 and 2009, cervical cancer 4-year cause-specific survival is approximately 13% lower without brachytherapy (64.3% v 51.5%; P < .001), and 4-year overall survival is 12% lower (58.2% v 46.2%; P < .001).52 Among 907 patients with stage IIIB cervical cancer treated with curative intent between 1960 and 1993 at MD Anderson Cancer Center (Houston, TX), 641 were treated with EBRT and brachytherapy, and 266 were treated with EBRT only; 5-year disease-specific survival was approximately 21% lower without brachytherapy (45% v 24%).53 Details on the external-beam boost volume to decrease complications suggest it would be reasonable to use a smaller pelvic field to cover a palpable tumor. A suggested superior border would be mid bony pelvis (this level is approximately 2 cm distal to the inferior sacroiliac joints) or at the inferior sacroiliac joint. For lateralized stage IIB or IIIB disease, the lateral borders would be 2 cm beyond the bony pelvis on plain x-ray. The inferior border should be 2 cm below palpable tumor in the vagina. The field arrangement may be a four-field box or a parallel pair as a second choice, if there are no resources available for delivering a four-field beam arrangement.
Clinical Question R4
Where there are no simulators, what can be used with bony anatomy to target correctly?
Recommendation R4: Setting without simulators.
In basic and limited settings where women do not have access to facilities with simulators at either local or referral institutions, plain diagnostic x-rays visualizing the bony pelvis may be used to guide field placement. Clinicians in enhanced and maximal settings should not apply this recommendation. (Evidence quality: high. Strength of recommendation: strong.)
Discussion of R4.
Where there are no simulators for planning pelvic irradiation, plain diagnostic x-rays visualizing the bony pelvis may be used to guide field placement. The field arrangement is preferably a four-field box, particularly for patients who are obese, but parallel anterior and posterior fields may be used if necessary. The superior and inferior borders of the field are the same for both field arrangements; the superior border may be between L4-5 and L5-S1, and the inferior border is placed 2 cm below palpable disease in the vagina. The lateral borders are placed 2 cm beyond the bony pelvis. Where lateral fields are used for the four-field box, the anterior border should be in front of the pubic arch, and the posterior border varies with the extent of disease and may often include the hollow of the sacrum inferiorly to S4-5. Where there is no means for shielding the superior lateral corners around the potential position of lymph nodes in the common iliac region and the fraction size is higher (> 2 Gy), a lower superior border, such as the mid S-I joint, may be used to spare normal small bowel. Clinical experience has indicated a smaller volume may decrease complications, and the additional curative value of higher superior borders is doubtful.
Alternatively, where there is no simulator and the patient is to be treated with a parallel pair of anterior and posterior fields, with the patient lying supine on the linear accelerator (LINAC) or cobalt-60 (60Co) bed, anterior–posterior separation should be measured. If both a LINAC and 60Co are available, a patient with a larger separation is better treated on the LINAC. To locate the skin mark for the isocenter, 2 cm should be measured superior to the pubic tubercle, and a 16 × 16 or 18 × 18 cm field should be placed at the axis. Before treatment, it should be verified on the treatment unit that the field covers the bony landmarks as described.
POST-TREATMENT FOLLOW-UP
The ASCO Expert Panel concludes that there is insufficient evidence guiding follow-up in all resource settings, especially those that are resource constrained, including supporting the use of visual inspection with acetic acid, human papillomavirus DNA testing, cytology (where tissue samples and/or laboratories are not available), or imaging for follow-up in those settings. In addition, the evidence for using squamous cell carcinoma antigen and/or high-sensitivity C-reactive protein is insufficient; prospective studies are needed. Therefore, this guideline does not recommend their use. ASCO informally endorses the CCO guideline on follow-up for cervical cancer5 and provides similar intervals as a guide (Table 6). Pelvic and physical examinations should be performed at follow-up. Suspicious lesions should be biopsied. Most evidence by expert opinion is that vaginal smear with cytology has been of low value. On the basis of the opinion of the ASCO Expert Panel, cervicovaginal cytology is not recommended for women after radiotherapy. Cytology may assist the diagnosis of early recurrences in cases of women treated with radical hysterectomy, with the caveat that the evidence is insufficient. PET-CT scans are often used in surveillance 3 to 6 months after treatment of patients at risk for treatment failure in high-resource settings. It is not within the scope of this guideline to review the evidence on post-treatment imaging, and the CCO guideline does not recommend PET-CT, because of the lack of prospective studies. However, there are indications that post-treatment PET scans may provide information for prognostic purposes in maximal-resource settings. For example, a prospective cohort study in which 92 women received an [18F]fluorodeoxyglucose-PET scan 3 months after treatment found that abnormal [18F]fluorodeoxyglucose-PET results were statistically significantly associated with lower cause-specific and progression-free survival compared with those in women whose PET scans showed complete response to treatment.54
PALLIATIVE CARE
Palliative care and pain management are part of the treatment of cancers, including cervical cancer. The goal of palliative care is to avoid unnecessary suffering during the final stages of disease. Palliative care is multifaceted and in some contexts can be provided concurrently with tumor-directed therapy. Pain control is a vital (but not the sole) component of palliative care and is a basic human right. This guideline adapts guidance9 on palliative care provided in the WHO guideline on women with cervical cancer, plus other guidelines and additional sources referenced in the Special Commentary under Palliative Care. In its guideline, WHO discusses the team approach. Our guideline encourages all policymakers to follow the WHO declaration on palliative care.55 Women with advanced cervical cancer with or without access to tumor-directed therapy may have specific late-stage symptoms that require clinicians to perform urogenital-specific interventions. The management of primary symptoms, which is discussed in the WHO guideline, includes but is not limited to pain, fistula, loss of appetite, wasting, bleeding, and GI and genitourinary symptoms. WHO provides practice sheets for caregivers to help women with vaginal discharge, fistula, and bleeding. Further discussion occurs in Special Commentary.
SPECIAL COMMENTARY
Radiation Therapy Shortages
There are enormous inequities in the supply of radiotherapy equipment and personnel between maximal and enhanced settings and limited and basic settings.56 There are many publications calling attention to this critical situation; therefore, this section will only briefly touch on it.
In some settings, only 10% of patients have access to radiation therapy; in others, such as in sub-Saharan Africa and Latin America, 0% to 4% of patients do, whereas in upper- and middle-income countries in Europe and Central Asia, 59% to 79% have access.57 Depending on the source, 39 to 55 LMICs have no radiation therapy resources.56-58 One publication states that “it has been estimated that Africa is functioning at 25% of its potential treatable capacity for cervical cancer alone.”59,60(p459) Several organizations are working to increase awareness of this shortage and address supply issues, including the International Atomic Energy Agency, Union for International Cancer Control, Global Task Force on Radiotherapy for Cancer Control, and American Society for Radiation Oncology Association of Residents in Radiation Oncology. This guideline strives to support these efforts and provides guidance to clinicians practicing in resource-constrained settings.
Palliative Care for Women With Advanced Cervical Cancer
This commentary supplements this guideline and is based on additional literature, some of which was not included in the formal adaptation reviews. Palliative care and pain management are part of the treatment of cancers, including cervical cancer, to avoid unnecessary suffering during the final stages of disease. Pain control is a vital component of palliative care; it is a basic human right often neglected in cancer control programs. Pain can be effectively controlled using a combination of medical and nonmedical interventions. Patients and caregivers need training for effective palliative care, including end-of-life counseling. Patients with advanced or recurrent cervical cancer may have any of the following symptoms: vaginal bleeding or discharge, pelvic or back pain, urinary or bowel fistulas, lower-extremity edema, deep-venous thrombosis, dyspnea resulting from anemia or pulmonary involvement, and uremia resulting from ureteral obstruction.
In limited-resource settings where radiation therapy is limited, providers may have to prioritize its use to treat selected patients with advanced-stage disease and palliate symptoms in other patients who normally receive antitumor treatment in maximal-level settings. Interventions to control vaginal bleeding include radiation therapy or brachytherapy, embolization of the uterine arteries, surgical resection, and arterial ligation. Vaginal packing is usually a temporary measure. The type and length of treatment should depend on the patient’s Karnofsky performance status.
Pain is often a disabling symptom of advanced or recurrent cervical cancer. Regional nerve, muscle, and bone infiltration can cause severe pain. Narcotic analgesics are a fundamental component of cancer pain treatment and may be prepared for oral, rectal, vaginal, sublingual, intravenous, intramuscular, epidural, or topical administration.
When pain is directly attributable to specific foci of disease, such as bone metastasis or para-aortic lymph node recurrence, a brief course of palliative radiation therapy yields substantial pain reduction in a high percentage of patients. However, pain relief may not be maximally achieved until weeks after the palliative radiation therapy ends.
Advanced cervical cancer may cause urinary fistulas, with vesicovaginal occurring more commonly than ureterovaginal fistulas. Although not necessarily painful, fistulous drainage can have an extremely negative impact on quality of life because of the constant odor.
Palliation of fistulas may be surgically accomplished by creation of a ureterointestinal conduit or placement of bilateral percutaneous nephrostomies to decompress the ureters. Rectovaginal fistulas may occur from primary tumor invasion of the adjacent rectum. These more often result from radiation injury or tumor recurrence. A diverting colostomy is the surgical procedure of choice. In some lower-resource settings, because the availability of radiotherapy is sometimes difficult or nonexistent, some fistulas and bleeding will be treated with other interventions.
Progressive or recurrent cervical cancer may cause uremia secondary to ureteral obstruction, which may induce nausea, vomiting, somnolence, confusion, and seizures. Ureteral obstruction is relieved by percutaneous nephrostomy or ureteral stents. Treatment of other symptoms is standard in patients needing palliative care, and the reader is referred to Chapter 7 of the WHO comprehensive cervical cancer book.5,8,61
COST IMPLICATIONS
There have been few studies of the cost effectiveness of treatment in LMICs. We can make some inferences as to how cost effective treatment is, using studies from three middle-income countries (Thailand, which is an upper middle–income country, and China and Morocco; both of the latter were lower middle–income countries at the time the studies were conducted).
Katanyoo et al34 compared two different treatment options for stage IIB disease (radical hysterectomy with pelvic lymph node dissection with or without postoperative adjuvant therapy v concurrent chemoradiotherapy). The first option (compared with no intervention) cost $322 per quality-adjusted life-year (QALY), and the second cost $327.4 per QALY in 2012 US dollars. This is considerably below the Thai per capita gross national income ($5,180 in the same year).62 Any intervention costing less than one times the per capita national income per disability-adjusted life-year is considered highly cost effective.63 Although QALYs and disability-adjusted life-years are not identical, they are roughly comparable. Cost of treatment of stage IIB disease in Thailand was $5,218 to $5,281 (ie, slightly greater than per capita income). However, the number of QALYs saved is large (15.9 to 16.4).
Cost data are available for treatment of similar-stage disease in Morocco and China. The cost in Morocco in 2008 was $6,883 (total colpohysterectomy, pelvic lymphadenectomy, and postoperative chemotherapy and radiotherapy), approximately 2.7 times the per capita national income of Morocco in that year.35 If QALYs saved were similar to those in Thailand (approximately 16), the cost per QALY saved of $430 would also fall into the cost-effective range.
For China, costs of the treatment components were estimated for a second-level (prefecture) hospital for 2008.36 Cost ranged from $404.73 to $544.39 for hysterectomy (simple to radical), was $281.65 for radiation therapy, and was $125.46 for adjuvant chemotherapy, such that treatment costs for stage IIB disease would be a little less than $1,000, compared with the per capita national income in that year of $2,975. Again, if the QALYs saved compared with no treatment were similar to those of Thailand, the cost per QALY would fall into the cost-effective range (< $100 per QALY).
Thus, treatment of patients with stage IIB disease is likely cost effective in middle-income countries, although the cost per patient is significant (ranging from one third of the per capita income in China to approximately one times the per capita income in Thailand to 2.7 times the per capita income in Morocco). Key needs are therefore to expand surgical capacity and ensure women access treatment sufficiently early in disease progression.63
The risk of metastasis to pelvic lymph nodes in patients with early disease is approximately 15% to 20% and 25% to 40% for patients with stage I and II disease, respectively, so there is a potential for cure in many of these patients whose disease has not yet spread. This is the rationale for extrafascial hysterectomy or its modification in the basic setting, but this recommendation depends on the ability to safely perform these procedures in these low-resource settings. This would depend as well on the ability to perform simple hysterectomies safely in low-resource settings. Concentrating surgical volume in high-risk centers and by high-risk surgeons has been shown in many clinical settings to improve outcomes. Thus, even in countries without trained gynecologic oncologists or access to ideal radiation therapy facilities, surgical outcomes could be improved by concentrating resources and designating experts. These types of changes may be cost effective both by improving clinical outcomes and by optimally using existing resources.
EXTERNAL REVIEW
The draft was submitted to one external reviewer with content expertise. It was rated as high quality, and it was agreed it would be useful in practice. Review comments were reviewed by the co-chairs of the Expert Panel and integrated into the final manuscript before approval by the CPGC.
GUIDELINE IMPLEMENTATION
ASCO guidelines are developed for implementation across health settings. Barriers to implementation include the need to increase awareness of the guideline recommendations among front-line practitioners, survivors of cancer, and caregivers and the need to provide adequate services in the face of limited resources. The guideline Bottom Line Box was designed to facilitate implementation of recommendations. This guideline will be distributed widely, including through the ASCO Practice Guideline Implementation Network and the ASCO Web site.
LIMITATIONS OF RESEARCH
There were several areas where evidence was lacking to make strong recommendations. These areas included the following: optimal post-treatment surveillance for women with cervical cancer at risk for recurrence, including the role of PET scans in maximal-resource settings; using squamous cell carcinoma antigen and/or high-sensitivity C-reactive protein; optimal dose fractionation of brachytherapy; surgery for women with stage IA2 or IB1 disease with tumor smaller than 2 cm in size and 1 cm in depth in the non–fertility-sparing setting; optimal treatment of patients with stage IB1 cervical cancer with tumor size between 2 and 4 cm; optimal fertility-sparing procedures for women with stage IA1 or IA2 disease; and treatment of women with invasive cervical cancer in basic settings, including regarding chemotherapy and radiation therapy.
ASCO believes that cancer clinical trials are vital to inform medical decisions and improve cancer care. All patients should have the opportunity to participate.
FUTURE DIRECTIONS
Further prospective comparative research is needed, conducted especially in basic- and limited-resource settings. There are ongoing studies of treatment for patients with stage IA2 versus 1B1 disease. Radical versus simple hysterectomy (the feasibility and safety of performing cone biopsy or simple hysterectomy) is an active area of investigation:
Nonrandomized GOG 278 (Studying the Physical Function and Quality of Life Before and After Surgery in Patients With Stage I Cervical Cancer) compares cone and pelvic lymphadenectomy versus simple hysterectomy and pelvic lymphadenectomy for patients with stage IA2 versus 1B1IA1 to IB1 disease with tumors smaller than 2 cm (ClinicalTrials.gov identifier NCT01649089)
Similar nonrandomized ConCerv (Conservative Surgery for Women With Low-Risk Early Stage Cervical Cancer) study (ClinicalTrials.gov identifier NCT01048853)
Randomized SHAPE (Radical Versus Simple Hysterectomy and Pelvic Node Dissection in Patients With Low-Risk Early Stage Cervical Cancer) trial of patients with stage IA2 or IB1 disease with tumors smaller than 2 cm, invasion smaller than 10 mm, and invasion less than 50% on magnetic resonance imaging (ClinicalTrials.gov identifier NCT01658930)
Postchemoradiotherapy with adjuvant chemotherapy trials:
OUTBACK (Phase III Trial of Adjuvant Chemotherapy As Primary Treatment of Locally Advanced Cervical Cancer Compared With Chemoradiation Alone) trial (ANZGOG [Australia New Zealand Gynaecological Oncology Group] 0902/GOG 0274/RTOG 1174; ClinicalTrials.gov identifier NCT01414608)
TACO (Triweekly Cisplatin Based Chemoradiation in Locally Advanced Cervical Cancer) trial (ClinicalTrials.gov identifier NCT01561586)
RTOG 0724 (Phase III Randomized Study of Concurrent Chemotherapy and Pelvic Radiation Therapy With or Without Adjuvant Chemotherapy in High-Risk Patients With Early-Stage Cervical Carcinoma Following Radical Hysterectomy) trial (ClinicalTrials.gov identifier NCT00980954)
Selected ongoing trials of NACT:
EORTC 55994 (Randomized Phase III Study of Neoadjuvant Chemotherapy Followed by Surgery vs. Concomitant Radiotherapy and Chemotherapy in FIGO Stage Ib2, IIa > 4 cm, IIb Cervical Cancer) trial (ClinicalTrials.gov identifier NCT00039338)
NACTcervix (Prospective Randomized Trial of Neoadjuvant Chemotherapy and Surgery Versus Concurrent Chemoradiation Therapy in Patients With Stage IB2-IIB Squamous Carcinoma of the Uterine Cervix) trial (ClinicalTrials.gov identifier NCT00193739)
SYSGO002 (Neoadjuvant Chemotherapy and Radical Surgery Versus Concurrent Chemoirradiation in FIGO Stage IIB Cervical Cancer) trial (ClinicalTrials.gov identifier NCT02595554)
DEFINITION
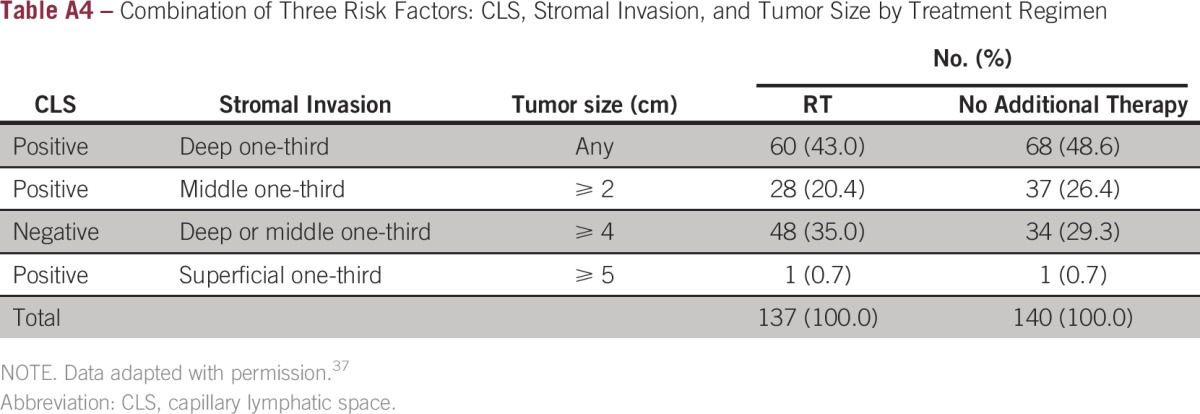
The panel advocates para-aortic lymph node sampling instead of lymphadenectomy. This is performed for the purpose of prognostic and not therapeutic implication. Sedlis et al37 criteria for para-aortic lymph node sampling are as follows (Appendix Table A4): presence of LVSI plus deep one-third cervical stromal invasion and tumor of any size, presence of LVSI plus middle one-third stromal invasion and tumor size of 2 cm or larger, presence of LVSI plus superficial one-third stromal invasion and tumor size of 5 cm or larger, or no LVSI but deep or middle one-third stromal invasion and tumor size of 4 cm or larger.
ADDITIONAL RESOURCES
More information, including a Data Supplement with additional evidence tables, a Methodology Supplement with information about evidence quality and strength of recommendations, slide sets, and clinical tools and resources, is available at www.asco.org/rs-cervical-cancer-treatment-guideline. Patient information is available at www.cancer.net. Visit www.asco.org/guidelineswiki to provide comments on the guideline or submit new evidence.
ACKNOWLEDGMENT
We thank Muhieddine A.F. Seoud, MD, Natasha B. Leighl, MD, Alexi A. Wright, MD, MPH, and the Clinical Practice Guideline Committee for their thoughtful reviews and insightful comments on this guideline document and Lynette Denny, MD, PhD, Allen S. Lichter, MD, Neville F. Hacker, MD, and Shannon McKernin for their assistance.
Appendix
Table A1.
Guidelines Considered in ADAPTE Process
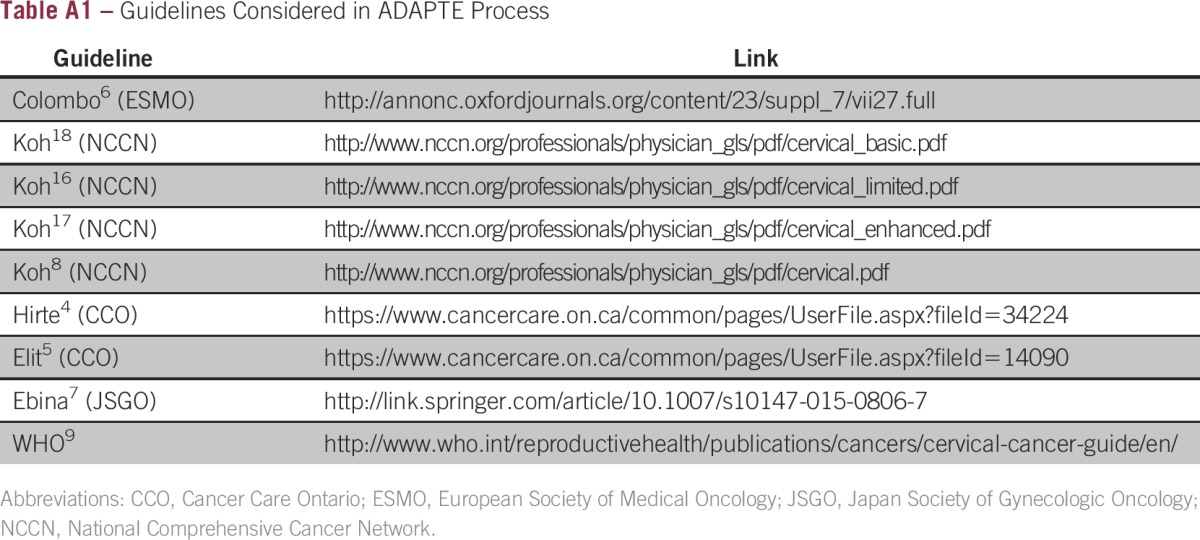
Table A2.
Framework of Resource Stratification: Treatment
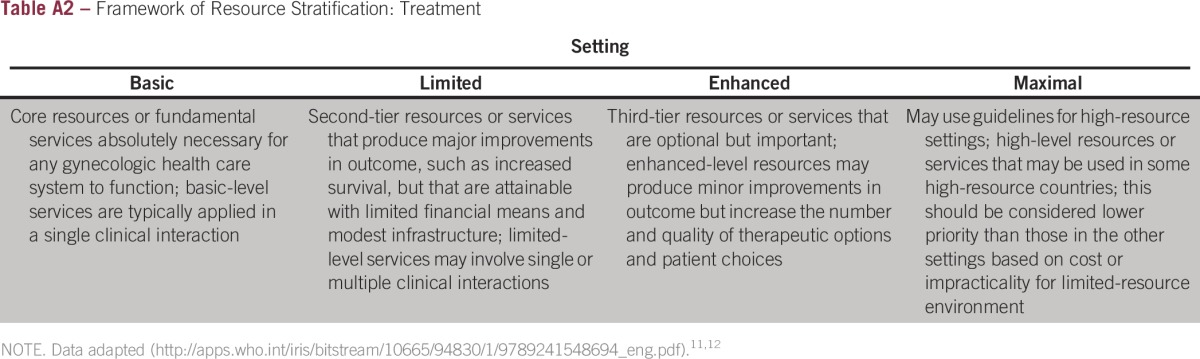
Table A3.
Expert Panel Membership
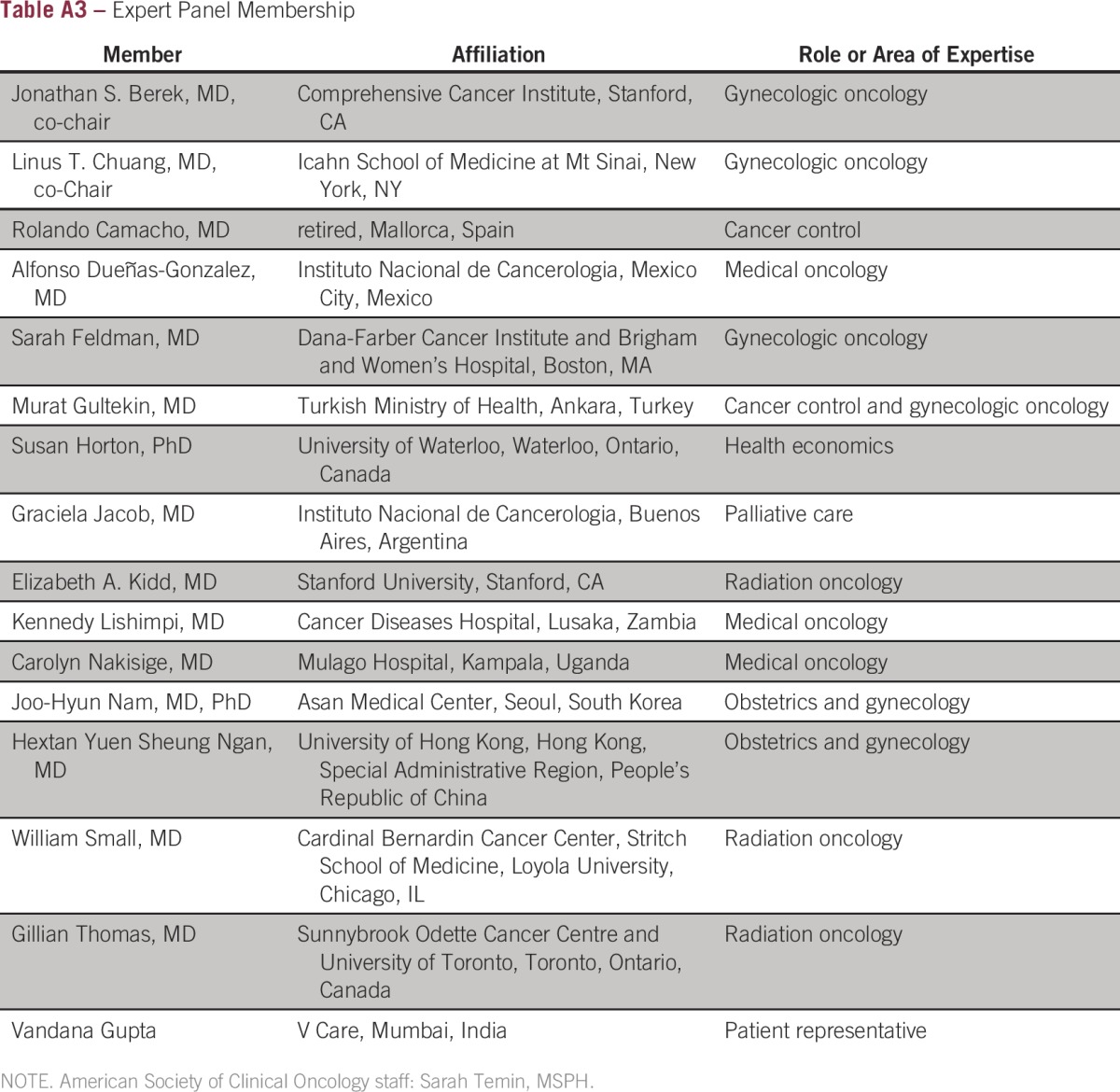
Table A4.
Combination of Three Risk Factors: CLS, Stromal Invasion, and Tumor Size by Treatment Regimen
Footnotes
This guideline has been endorsed by the Society of Gynecologic Oncology.
Authors’ disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Clinical Practice Guideline Committee approved: February 21, 2016.
Editor’s note: This American Society of Clinical Oncology clinical practice guideline provides recommendations, with comprehensive review and analysis of the relevant literature for each recommendation. Additional information, including a Data Supplement with additional evidence tables, a Methodology Supplement, slide sets, clinical tools and resources, and links to patient information at www.cancer.net, is available at www.asco.org/rs-cervical-cancer-treatment-guideline.
Reprint requests: 2318 Mill Rd, Suite 800, Alexandria, VA 22314; e-mail: guidelines@asco.org.
ADDENDUM
This addendum acknowledges the endorsement by Gynecologic Cancer InterGroup, in addition to the endorsement of the Society of Gynecologic Oncology as previously acknowledged in the footnotes.
AUTHOR CONTRIBUTIONS
Administrative support: Sarah Temin
Manuscript writing: All authors
Final approval of manuscript: All authors
AUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO’s conflict of interest policy, please refer to www.asco.org/rwc or jco.ascopubs.org/site/ifc.
Linus T. Chuang
No relationship to disclose
Sarah Temin
No relationship to disclose
Rolando Camacho
No relationship to disclose
Alfonso Dueñas-Gonzalez
No relationship to disclose
Sarah Feldman
No relationship to disclose
Murat Gultekin
No relationship to disclose
Vandana Gupta
No relationship to disclose
Susan Horton
No relationship to disclose
Graciela Jacob
No relationship to disclose
Elizabeth A. Kidd
Research Funding: Siemens
Kennedy Lishimpi
No relationship to disclose
Carolyn Nakisige
No relationship to disclose
Joo-Hyun Nam
Research Funding: AstraZeneca, AbbVie
Hextan Yuen Sheung Ngan
Honoraria: Merck Sharp & Dohme (Asia), Amgen (Asia), Ipsos Healthcare, Chindex Hong Kong, Pfizer
Consulting or Advisory Role: Amgen (Asia)
Speakers’ Bureau: Merck Sharp & Dohme (Asia), Chindex Hong Kong, Pfizer
Research Funding: Amgen (Asia; Inst)
Travel, Accommodations, Expenses: Roche Hong Kong, Chindex Hong Kong, Merck Sharp & Dohme (Asia), Pfizer, AstraZeneca
William Small
Honoraria: Carl Zeiss Meditec
Speakers’ Bureau: Carl Zeiss Meditec
Research Funding: Carl Zeiss Meditec
Travel, Accommodations, Expenses: Carl Zeiss Meditec
Gillian Thomas
No relationship to disclose
Jonathan S. Berek
Consulting or Advisory Role: Atara Biotherapeutics
Research Funding: Tesaro (Inst), AstraZeneca (Inst)
REFERENCES
- 1.International Agency for Research on Cancer GLOBOCAN 2012 Cervical Cancer: Estimated Incidence, Mortality and Prevalence Worldwide in 2012. http://globocan.iarc.fr/old/FactSheets/cancers/cervix-new.asp.
- 2.Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2012. http://seer.cancer.gov/csr/1975_2012/ [Google Scholar]
- 3.Catholic Campaign for Human Development Interrelationships of three-year average state poverty rates: 2011-2013. http://www.povertyusa.org/the-state-of-poverty/poverty-map-state/#.
- 4.Hirte H, Kennedy EB, Elit L, et al. Systemic therapy for recurrent, persistent, or metastatic cervical cancer: A clinical practice guideline. Curr Oncol. 2015;22:211–219. doi: 10.3747/co.22.2447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Elit L, Kennedy EB, Fyles A, et al. doi: 10.3747/co.23.2742. Follow-Up for Cervical Cancer. https://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=340742. [DOI] [PMC free article] [PubMed]
- 6.Colombo N, Carinelli S, Colombo A, et al. Cervical cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012;23(suppl 7):vii27–vii32. doi: 10.1093/annonc/mds268. [DOI] [PubMed] [Google Scholar]
- 7.Ebina Y, Yaegashi N, Katabuchi H, et al. Japan Society of Gynecologic Oncology guidelines 2011 for the treatment of uterine cervical cancer. Int J Clin Oncol. 2015;20:240–248. doi: 10.1007/s10147-015-0806-7. [DOI] [PubMed] [Google Scholar]
- 8.Koh WJ, Greer BE, Abu-Rustum NR, et al. Cervical cancer, version 2.2015. J Natl Compr Canc Netw. 2015;13:395–404. doi: 10.6004/jnccn.2015.0055. quiz 404. [DOI] [PubMed] [Google Scholar]
- 9.World Health Organization . Comprehensive Cervical Cancer Control: A Guide to Essential Practice. ed 2. http://apps.who.int/iris/bitstream/10665/144785/1/9789241548953_eng.pdf. [PubMed] [Google Scholar]
- 10.World Health Organization WHO National Cancer Control Programmes: Policies and Managerial Guidelines—2002. http://www.who.int/cancer/publications/nccp2002/en/
- 11.Anderson BO, Yip CH, Smith RA, et al. Guideline implementation for breast healthcare in low-income and middle-income countries: Overview of the Breast Health Global Initiative Global Summit 2007. Cancer. 2008;113(suppl 8):2221–2243. doi: 10.1002/cncr.23844. [DOI] [PubMed] [Google Scholar]
- 12.Horton S, Gauvreau CL. Cancer in low- and middle-income countries: An economic overview. In: Gelband H, Jha P, Sankaranarayanan R, et al., editors. Cancer Disease Control Priorities. ed 3. Washington, DC: International Bank for Reconstruction and Development/World Bank; 2015. [PubMed] [Google Scholar]
- 13.ADAPTE Collaboration Guideline Adaptation: A Resource Toolkit (version 2.0). http://www.g-i-n.net/document-store/working-groups-documents/adaptation/adapte-resource-toolkit-guideline-adaptation-2-0.pdf.
- 14.Shiffman RN, Michel G, Rosenfeld RM, et al. Building better guidelines with BRIDGE-Wiz: Development and evaluation of a software assistant to promote clarity, transparency, and implementability. J Am Med Inform Assoc. 2012;19:94–101. doi: 10.1136/amiajnl-2011-000172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Koh WJ, Greer BE, Abu-Rustum NR, et al. NCCN Guidelines Version 2.2015: Cervical Cancer Preliminary Resource Stratification—Maximal Level. Fort Washington, PA: National Comprehensive Cancer Network; 2015. [Google Scholar]
- 16.Koh WJ, Greer BE, Abu-Rustum NR, et al. NCCN Guidelines Version 2.2015: Cervical Cancer Preliminary Resource Stratification—Limited Level. Fort Washington, PA: National Comprehensive Cancer Network; 2015. [Google Scholar]
- 17.Koh WJ, Greer BE, Abu-Rustum NR, et al. NCCN Guidelines Version 2.2015: Cervical Cancer Preliminary Resource Stratification—Enhanced Level. Fort Washington, PA: National Comprehensive Cancer Network; 2015. [Google Scholar]
- 18.Koh WJ, Greer BE, Abu-Rustum NR, et al. NCCN Guidelines Version 2.2015: Cervical Cancer Preliminary Resource Stratification—Basic Level. Fort Washington, PA: National Comprehensive Cancer Network; 2015. [Google Scholar]
- 19.Lee LJ, Das IJ, Higgins SA, et al. American Brachytherapy Society consensus guidelines for locally advanced carcinoma of the cervix: Part III—Low-dose-rate and pulsed-dose-rate brachytherapy. Brachytherapy. 2012;11:53–57. doi: 10.1016/j.brachy.2011.07.001. [DOI] [PubMed] [Google Scholar]
- 20.Nagase S, Inoue Y, Umesaki N, et al. Evidence-based guidelines for treatment of cervical cancer in Japan: Japan Society of Gynecologic Oncology (JSGO) 2007 edition. Int J Clin Oncol. 2010;15:117–124. doi: 10.1007/s10147-010-0061-x. [DOI] [PubMed] [Google Scholar]
- 21.Viswanathan AN, Beriwal S, De Los Santos JF, et al. American Brachytherapy Society consensus guidelines for locally advanced carcinoma of the cervix: Part II—High-dose-rate brachytherapy. Brachytherapy. 2012;11:47–52. doi: 10.1016/j.brachy.2011.07.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Oaknin A, Díaz de Corcuera I, Rodríguez-Freixinós V, et al. SEOM guidelines for cervical cancer. Clin Transl Oncol. 2012;14:516–519. doi: 10.1007/s12094-012-0834-y. [DOI] [PubMed] [Google Scholar]
- 23.Small W, Jr, Beriwal S, Demanes DJ, et al. American Brachytherapy Society consensus guidelines for adjuvant vaginal cuff brachytherapy after hysterectomy. Brachytherapy. 2012;11:58–67. doi: 10.1016/j.brachy.2011.08.005. [DOI] [PubMed] [Google Scholar]
- 24.Haie-Meder C, Fervers B, Fondrinier E, et al. SOR guidelines for concomitant chemoradiotherapy for patients with uterine cervical cancers: Evidence update bulletin 2004. Ann Oncol. 2005;16:1100–1108. doi: 10.1093/annonc/mdi220. [DOI] [PubMed] [Google Scholar]
- 25.Ye Q, Yuan HX, Chen HL. Responsiveness of neoadjuvant chemotherapy before surgery predicts favorable prognosis for cervical cancer patients: A meta-analysis. J Cancer Res Clin Oncol. 2013;139:1887–1898. doi: 10.1007/s00432-013-1509-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kokka F, Bryant A, Brockbank E, et al. Hysterectomy with radiotherapy or chemotherapy or both for women with locally advanced cervical cancer. Cochrane Database Syst Rev. 2015;4:CD010260. doi: 10.1002/14651858.CD010260.pub2. [DOI] [PubMed] [Google Scholar]
- 27.Neoadjuvant Chemotherapy for Cervical Cancer Meta-Analysis Collaboration (NACCCMA) Collaboration Neoadjuvant chemotherapy for locally advanced cervix cancer. Cochrane Database Syst Rev. 2004;2:CD001774. doi: 10.1002/14651858.CD001774.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rydzewska L, Tierney J, Vale CL, et al. Neoadjuvant chemotherapy plus surgery versus surgery for cervical cancer. Cochrane Database Syst Rev. 2012;12:CD007406. doi: 10.1002/14651858.CD007406.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Rosa DD, Medeiros LR, Edelweiss MI, et al. Adjuvant platinum-based chemotherapy for early stage cervical cancer. Cochrane Database Syst Rev. 2012;6:CD005342. doi: 10.1002/14651858.CD005342.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kucukmetin A, Biliatis I, Naik R, et al. Laparoscopically assisted radical vaginal hysterectomy versus radical abdominal hysterectomy for the treatment of early cervical cancer. Cochrane Database Syst Rev. 2013;10:CD006651. doi: 10.1002/14651858.CD006651.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Liu R, Wang X, Tian JH, et al. High dose rate versus low dose rate intracavity brachytherapy for locally advanced uterine cervix cancer. Cochrane Database Syst Rev. 2014;10:CD007563. doi: 10.1002/14651858.CD007563.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Scatchard K, Forrest JL, Flubacher M, et al. Chemotherapy for metastatic and recurrent cervical cancer. Cochrane Database Syst Rev. 2012;10:CD006469. doi: 10.1002/14651858.CD006469.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.van Lonkhuijzen L, Thomas G. Palliative radiotherapy for cervical carcinoma: A systematic review. Radiother Oncol. 2011;98:287–291. doi: 10.1016/j.radonc.2011.01.009. [DOI] [PubMed] [Google Scholar]
- 34.Katanyoo K, Praditsitthikorn N, Tangjitgamol S, et al. Cost-utility analysis of treatments for stage IB cervical cancer. J Gynecol Oncol. 2014;25:97–104. doi: 10.3802/jgo.2014.25.2.97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Berraho M, Najdi A, Mathoulin-Pelissier S, et al. Direct costs of cervical cancer management in Morocco. Asian Pac J Cancer Prev. 2012;13:3159–3163. doi: 10.7314/apjcp.2012.13.7.3159. [DOI] [PubMed] [Google Scholar]
- 36.Shi JF, Chen JF, Canfell K, et al. Estimation of the costs of cervical cancer screening, diagnosis and treatment in rural Shanxi Province, China: A micro-costing study. BMC Health Serv Res. 2012;12:123. doi: 10.1186/1472-6963-12-123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sedlis A, Bundy BN, Rotman MZ, et al. A randomized trial of pelvic radiation therapy versus no further therapy in selected patients with stage IB carcinoma of the cervix after radical hysterectomy and pelvic lymphadenectomy: A Gynecologic Oncology Group study. Gynecol Oncol. 1999;73:177–183. doi: 10.1006/gyno.1999.5387. [DOI] [PubMed] [Google Scholar]
- 38.National Cancer Institute Cervical cancer treatment: Health professional version. http://www.cancer.gov/types/cervical/hp/cervical-treatment-pdq.
- 39.Zuliani AC, Esteves SC, Teixeira LC, et al. Concomitant cisplatin plus radiotherapy and high-dose-rate brachytherapy versus radiotherapy alone for stage IIIB epidermoid cervical cancer: A randomized controlled trial. J Clin Oncol. 2014;32:542–547. doi: 10.1200/JCO.2013.50.1205. [DOI] [PubMed] [Google Scholar]
- 40.Srivastava K, Paul S, Chufal KS, et al. Concurrent chemoradiation versus radiotherapy alone in cervical carcinoma: A randomized phase III trial. Asia Pac J Clin Oncol. 2013;9:349–356. doi: 10.1111/ajco.12078. [DOI] [PubMed] [Google Scholar]
- 41.Cetina L, González-Enciso A, Cantú D, et al. Brachytherapy versus radical hysterectomy after external beam chemoradiation with gemcitabine plus cisplatin: A randomized, phase III study in IB2-IIB cervical cancer patients. Ann Oncol. 2013;24:2043–2047. doi: 10.1093/annonc/mdt142. [DOI] [PubMed] [Google Scholar]
- 42.Eifel PJ. Adjuvant surgery after radiotherapy. J Natl Cancer Inst Monogr. 1996;21:85–88. [PubMed] [Google Scholar]
- 43.Dueñas-González A, Zarbá JJ, Patel F, et al. Phase III, open-label, randomized study comparing concurrent gemcitabine plus cisplatin and radiation followed by adjuvant gemcitabine and cisplatin versus concurrent cisplatin and radiation in patients with stage IIB to IVA carcinoma of the cervix. J Clin Oncol. 2011;29:1678–1685. doi: 10.1200/JCO.2009.25.9663. [DOI] [PubMed] [Google Scholar]
- 44.Wethington SL, Sonoda Y, Park KJ, et al. Expanding the indications for radical trachelectomy: A report on 29 patients with stage IB1 tumors measuring 2 to 4 centimeters. Int J Gynecol Cancer. 2013;23:1092–1098. doi: 10.1097/IGC.0b013e318296034e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Li J, Wu X, Li X, et al. Abdominal radical trachelectomy: Is it safe for IB1 cervical cancer with tumors ≥ 2 cm? Gynecol Oncol. 2013;131:87–92. doi: 10.1016/j.ygyno.2013.07.079. [DOI] [PubMed] [Google Scholar]
- 46.Delgado G, Bundy B, Zaino R, et al. Prospective surgical-pathological study of disease-free interval in patients with stage IB squamous cell carcinoma of the cervix: A Gynecologic Oncology Group study. Gynecol Oncol. 1990;38:352–357. doi: 10.1016/0090-8258(90)90072-s. [DOI] [PubMed] [Google Scholar]
- 47.Loren AW, Mangu PB, Beck LN, et al. Fertility preservation for patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2013;31:2500–2510. doi: 10.1200/JCO.2013.49.2678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Kitagawa R, Katsumata N, Shibata T, et al. Paclitaxel plus carboplatin versus paclitaxel plus cisplatin in metastatic or recurrent cervical cancer: The open-label randomized phase III trial JCOG0505. J Clin Oncol. 2015;33:2129–2135. doi: 10.1200/JCO.2014.58.4391. [DOI] [PubMed] [Google Scholar]
- 49.Tewari KS, Sill MW, Long HJ, III, et al. Improved survival with bevacizumab in advanced cervical cancer. N Engl J Med. 2014;370:734–743. doi: 10.1056/NEJMoa1309748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Spanos WJ, Jr, Pajak TJ, Emami B, et al. Radiation palliation of cervical cancer. J Natl Cancer Inst Monogr. 1996;21:127–130. [PubMed] [Google Scholar]
- 51.Einck JP, Hudson A, Shulman AC, et al. Implementation of a high-dose-rate brachytherapy program for carcinoma of the cervix in Senegal: A pragmatic model for the developing world. Int J Radiat Oncol Biol Phys. 2014;89:462–467. doi: 10.1016/j.ijrobp.2013.12.008. [DOI] [PubMed] [Google Scholar]
- 52.Han K, Milosevic M, Fyles A, et al. Trends in the utilization of brachytherapy in cervical cancer in the United States. Int J Radiat Oncol Biol Phys. 2013;87:111–119. doi: 10.1016/j.ijrobp.2013.05.033. [DOI] [PubMed] [Google Scholar]
- 53.Logsdon MD, Eifel PJ. Figo IIIB squamous cell carcinoma of the cervix: An analysis of prognostic factors emphasizing the balance between external beam and intracavitary radiation therapy. Int J Radiat Oncol Biol Phys. 1999;43:763–775. doi: 10.1016/s0360-3016(98)00482-9. [DOI] [PubMed] [Google Scholar]
- 54.Schwarz JK, Siegel BA, Dehdashti F, et al. Association of posttherapy positron emission tomography with tumor response and survival in cervical carcinoma. JAMA. 2007;298:2289–2295. doi: 10.1001/jama.298.19.2289. [DOI] [PubMed] [Google Scholar]
- 55.World Health Organization doi: 10.3109/15360288.2014.911801. Strengthening of palliative care as a component of comprehensive care throughout the life course. http://apps.who.int/gb/ebwha/pdf_files/WHA67/A67_R19-en.pdf. [DOI] [PubMed]
- 56.Jaffray DA, Gospodarowicz M. Bringing global access to radiation therapy: Time for a change in approach. Int J Radiat Oncol Biol Phys. 2014;89:446–447. doi: 10.1016/j.ijrobp.2014.05.019. [DOI] [PubMed] [Google Scholar]
- 57.Zubizarreta EH, Fidarova E, Healy B, et al. Need for radiotherapy in low and middle income countries: The silent crisis continues. Clin Oncol (R Coll Radiol) 2015;27:107–114. doi: 10.1016/j.clon.2014.10.006. [DOI] [PubMed] [Google Scholar]
- 58.Datta NR, Samiei M, Bodis S. Radiation therapy infrastructure and human resources in low- and middle-income countries: Present status and projections for 2020. Int J Radiat Oncol Biol Phys. 2014;89:448–457. doi: 10.1016/j.ijrobp.2014.03.002. [DOI] [PubMed] [Google Scholar]
- 59.Abdel-Wahab M, Bourque JM, Pynda Y, et al. Status of radiotherapy resources in Africa: An International Atomic Energy Agency analysis. Lancet Oncol. 2013;14:e168–e175. doi: 10.1016/S1470-2045(12)70532-6. [DOI] [PubMed] [Google Scholar]
- 60.Fisher BJ, Daugherty LC, Einck JP, et al. Radiation oncology in Africa: improving access to cancer care on the African continent. Int J Radiat Oncol Biol Phys. 2014;89:458–461. doi: 10.1016/j.ijrobp.2013.12.032. [DOI] [PubMed] [Google Scholar]
- 61.Friedlander M, Grogan M, US Preventative Services Task Force Guidelines for the treatment of recurrent and metastatic cervical cancer. Oncologist. 2002;7:342–347. [PubMed] [Google Scholar]
- 62.The World Bank GNI per capita, Atlas method (current US$). http://data.worldbank.org/indicator/NY.GNP.PCAP.CD?page=1.
- 63.Sachs JD. Macroeconomics and Health: Investing in Health for Economic Development. Geneva, Switzerland: World Health Organization; 2001. [Google Scholar]