

Key Clinical Message
We report a case of Noonan syndrome with loose anagen hair (NS/LAH), a rare variant of Noonan syndrome, with associated trichorrhexis nodosa and trichoptilosis. The SHOC2 mutation may be responsible for these additional hair shaft defects, revealing the importance of microscopic examination of hairs in these patients.
Keywords: Noonan syndrome with loose anagen hair, trichoptilosis, trichorrhexis nodosa
Case Report
A 6‐year‐old Haitian female was seen in the Genodermatoses Clinic for abnormal hair. She had a history of sparse, slow‐growing hair since birth, reaching a maximum length of 3 inches, and never needing a haircut. There had been minimal hair grooming and braiding. Her past medical history revealed failure to thrive, short stature, macrocephaly, dysmorphic facial features, multiple dental caries, learning disability, and recent behavioral issues. There was no personal history of eczema and no family history of genetic disorders.
Her height and weight were at the 1st percentile for her age. She had a prominent forehead and epicanthal folds. Her hair was coarse, brittle, and sparse (Fig. 1). There was no scalp erythema or scarring. Approximately 20 hairs were easily and painlessly plucked with a hemostat. Under microscopic examination, 15 anagen hairs were visible with misshapen hair bulbs and ruffled cuticles, consistent with the diagnosis of loose anagen hair. Several hair shafts showed trichoptilosis and trichorrhexis nodosa (Fig. 2). The remainder of her examination revealed hairless skin without ichthyosis or eczematous dermatitis.
Figure 1.

Sparse, coarse, short hair accentuated in temporal and occipital regions with longer hair on vertex.
Figure 2.
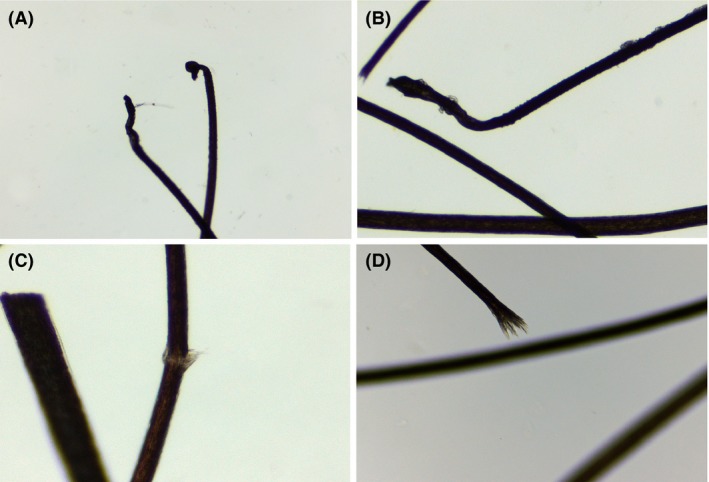
Light microscopy view of extracted hairs. Loose anagen hairs (A) and (B) displaying ruffled cuticles and misshapen hair bulbs positioned at an acute angle to hair shaft. Trichorrhexis nodosa (C) represented as focal longitudinal fractures of inner fibers with outer fibers bulging out causing segmental increase in hair diameter. Trichoptilosis (D) represented as longitudinal splitting of distal hair shaft.
Genetic testing revealed a heterozygous, missense mutation, c.4A>G (p.Ser2Gly) in SHOC2 and confirmed the diagnosis of Noonan syndrome with loose anagen hair (NS/LAH). Growth hormone studies revealed a normal serum insulin‐like growth factor (IGF1) level, but given her short stature, recombinant human growth hormone therapy was initiated.
Discussion
Noonan syndrome is an autosomal dominant, multisystem disorder characterized by dysmorphic features, short stature, cardiac and brain anomalies, predisposition to certain malignancies, and developmental delay 1. Patients with NS/LAH have these typical features plus growth hormone deficiency, distinctive hyperactive behavior, more significant cognitive defects, hoarse or hypernasal voice, darkly pigmented and hairless skin with eczema or ichthyosis and loose anagen hair 1, 2. They are part of a group of clinically related disorders caused by mutations in genes encoding molecules in the RAS/MAPK pathway, which is vital for cell differentiation and proliferation 1, 2.
Studies have demonstrated the EGFR‐Ras‐Raf pathway is required for hair cycle progression and maintenance of follicular integrity 3. The SHOC2 mutation encodes a scaffold protein that becomes aberrantly localized in the cell membrane after stimulation with epidermal growth factor leading to increased MAPK activation. This likely causes a disruption in the proliferation, survival, or differentiation of epithelial stem cells residing in the hair follicle during anagen phase, resulting in loose anagen hair 2. The hairs are predominantly in anagen phase and are easily pluckable, sparse, and slow growing. The diagnosis can be confirmed by microscopic examination of extracted hairs from hair pull test or hair‐pluck trichogram, revealing >50% anagen hairs with misshapen bulbs, ruffled cuticles, and absent inner and outer root sheaths 4.
Both trichorrhexis nodosa and trichoptilosis are hair shaft abnormalities that result in fractures and splitting due to defects in the underlying structure of the hair shaft, or damage to the protective cuticle layer. These can be congenital or acquired secondary to excessive hair manipulation 5. It is possible that the SHOC2 mutation in NS/LAH may also lead to structural defects in the hair shaft resulting in increased hair fragility.
This case expands upon the hair features seen in NS/LAH and suggests these patients may have an increased susceptibility to hair shaft fragility. Both the diagnostic features of loose anagen hair and hair shaft abnormalities can be detected using light microscopy of extracted hairs. Additional preventative counseling on minimizing hair manipulation may be beneficial for these patients.
Authorship
JK: wrote the original draft and revisions of the manuscript. KB: edited the manuscript and cared for the patient. RM: took the clinical photographs and edited the manuscript. SP: took the hair shaft photographs and edited the manuscript. BH: was the geneticist who made the diagnosis of Noonan syndrome and cared for the patient. MM: was the initial geneticist who saw the patient. KW: was the senior author and pediatric dermatologist who diagnosed the hair shaft abnormalities.
Conflict of Interest
None declared.
References
- 1. Gripp, K. W. , Zand D. J., Demmer L., Anderson C. E., Dobyns W. B., Zackai E. H., et al. 2013. Expanding the SHOC2 mutation associated phenotype of Noonan syndrome with loose anagen hair: structural brain anomalies and myelofibrosis. Am. J. Med. Genet. 161A:2420–2430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Cordeddu, V. , Di Schiavi E., Pennacchio L. A., Ma'ayan A., Sarkozy A., Fodale V., et al. 2009. Mutation of SHOC2 promotes aberrant protein N‐myristoylation and causes Noonan‐like syndrome with loose anagen hair. Nat. Genet. 41:1022–1026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Doma, E. , Rupp C., and Baccarini M.. 2009. EGFR‐Ras‐Raf signaling in epidermal stem cells: roles in hair follicle development, regeneration, tissue remodeling and epidermal cancers. Int. J. Mol. Sci. 14:19361–19384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Dhurat, R. P. , and Deshpande D. J.. 2010. Loose anagen hair syndrome. Int. J. Trichology. 2:96–100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Rudnicka, L. , Rakowska A., Kerzeja M., and Olszewska M.. 2013. Hair shaft in trichoscopy: clues for diagnosis of hair and scalp diseases. Dermatol. Clin. 31:695–708. [DOI] [PubMed] [Google Scholar]