

Administration of doses of technetium 99m mertiatide in the range of 300–370 MBq (approximately 8–10 mCi) does not improve imaging interpretation and results in excess radiation to the patient; the results of this study support limiting the administered doses to 37–185 MBq (1.0–5.0 mCi) as recommended by expert and existing guidelines.
Abstract
Purpose
To determine if commonly administered doses of technetium 99m (99mTc) mertiatide (MAG3) in the range of 300–370 MBq (approximately 8–10 mCi) contribute to image interpretation and justify the resulting radiation exposure.
Materials and Methods
The respective institutional review boards approved this HIPAA-compliant study and waived informed consent. Baseline and furosemide 99mTc-MAG3 imaging examinations in 50 patients suspected of having renal obstruction and 48 patients suspected of having renovascular hypertension (RVH) were randomly selected from archived databases and were independently scored by three experienced readers without access to 2-second flow images. Readers were blinded to their original scores, and then they rescored each examination with access to high-activity 2-second flow images. Relative renal function was determined after a low activity (62.9 MBq ± 40.7) baseline acquisition for RVH and a high activity (303.4 MBq ± 48.1) acquisition after administration of enalaprilat. Data were analyzed by using random effects analysis of variance and mean and standard error of the mean for the difference between sets of scores and the difference between relative function measurements.
Results
There was no significant difference in the scores without flow images compared with blinded scores with high-activity flow images for patients suspected of having obstruction (P = .80) or RVH (P = .24). Moreover, there was no significant difference in the relative uptake measurements after administration of low and high activities (P > .99).
Conclusion
Administered doses of 99mTc-MAG3 in the range of 300–370 MBq (approximately 8–10 mCi) do not affect the relative function measurements or contribute to interpretation of images in patients suspected of having RVH or obstruction compared with administration of lower doses; unnecessary radiation exposure can be avoided by administering doses in the range of 37–185 MBq as recommended incurrent guidelines.
© RSNA, 2017
Introduction
Technetium 99m (99mTc) mertiatide (MAG3; Technescan MAG3; Mallinckrodt, St Louis, Mo) is used widely for routine dynamic renal imaging and is the radiopharmaceutical of choice for the evaluation of both children and adults suspected of having an obstruction (1–4). The package insert for 99mTc-MAG3 suggests an administered dose range of 185 MBq (5 mCi) to 370 MBq (10 mCi) for the average adult patient who weighs 70 kg (5). Currently available nuclear medicine textbooks recommend doses for renal examinations ranging from 37 to 370 MBq (1–10 mCi), 92.5 to 185 MBq (2.5–5 mCi), and 370 to 720 MBq (10–20 mCi) (6–8). The administered activity is adjusted for infants and children but rarely ever adjusted for adults. We recommend reducing the typical adult dose by 50% to 90%. Current guidelines indicate that an administered dose of 370 MBq is unnecessarily high for almost all applications, and that a range of 37–185 MBq is much more appropriate for the adult patient (1,4,9,10). Nevertheless, 370 MBq appears to be the most commonly administered dose. One of the authors (R.H.) contacted representatives from three nuclear pharmacies in Atlanta, Ga: Triad Isotopes reported that more than 90% of its 99mTc-MAG3 unit doses were 370 MBq, Cardinal Health stated that the majority of unit doses it dispensed were 370 MBq, and GE Healthcare stated that 54.5% were from 296 to 370 MBq (8–10 mCi) and 40.8% were from 148 to 185 MBq (5–6 mCi); although GE Healthcare had no breakdown between adult and pediatric doses.
The primary rationale for the administration of doses in the range of 370–740 MBq appears to be the need to obtain sufficient counts to visualize the initial bolus in 1–3-second frames as the bolus transits the aorta and kidneys and/or to calculate quantitative flow indexes on the basis of these initial 1–3-second frames (11–13). Although there are data to suggest that the flow study may be useful in the evaluation of renal transplants, neither 1–3-second flow images nor quantitative flow calculations obtained in the first few seconds after injection have been demonstrated clearly to contribute to the evaluation of suspected collecting system obstruction or renovascular hypertension (RVH) (1,4,11–14). If administered doses of 99mTc-MAG3 in the 300–370 MBq range fail to provide additional diagnostic information, radiologists and nuclear medicine physicians would have the opportunity to reduce the radiation exposure to their patients by substantially reducing the administered dose. The purpose of this study was to determine if commonly administered doses of 99mTc-MAG3 in the range of 300–370-MBq (approximately 8–10 mCi) contribute to imaging interpretation and justify the resulting level of radiation exposure.
Materials and Methods
Patient Selection
This retrospective study was performed under the purview and approval of both the institutional review board and the Veterans Affairs Research and Development Committee and was compliant with the Health Insurance Portability and Accountability Act, or HIPAA; the requirement for informed consent was waived, because archived data were used in the study. A power calculation was performed to determine the number of kidneys needed for the study (see the statistical section of this article). The population suspected of having obstruction consisted of 50 patients with ages ranging from 18 to 82 years (mean age ± standard deviation, 52.1 years ± 17.3); there were 22 men with ages ranging from 28 to 82 years (mean age, 55.5 years ± 15.7) and 28 women with ages ranging from 18 to 80 years (mean age, 49.4 years ± 18.3) who were randomly selected from our archived database. This database currently contains the raw data of 578 archived renal examinations dating from January 5, 1994, to the present. Of these 578 examinations, 216 are categorized as showing suspected obstruction with the use of furosemide. The 50 studies were sequentially selected from the archived studies categorized as suspicious for obstruction with the use of furosemide beginning on March 24, 1998, and ending on April 10, 2010. Two patients had only one kidney; consequently, the imaging data of 98 kidneys were evaluable for patients suspected of having obstruction.
Our standard protocol for patients suspected of having obstruction is to perform a 24-minute baseline acquisition; if the baseline renal study results are within the normal range, obstruction is excluded and furosemide is not administered. If the baseline renal study shows either kidney to be abnormal or equivocal for obstruction after the postvoid image, furosemide is administered and an additional 20-minute acquisition is performed. The subset of patients included in our study was restricted to those who received furosemide, and, consequently consisted of patients more likely to have equivocal or abnormal results; this subset was chosen to allow the flow images the greatest opportunity of affecting the interpretation, because flow images are unlikely to affect the diagnosis of obstruction in a patient with a baseline study with completely normal results.
We also evaluated the images of 50 patients (48 men and two women) aged 37–84 years (mean age, 63.5 years ± 10.2); there were 48 men aged 37–84 years (mean age, 63.8 years ± 10.2), and two women, aged 52 and 62, who were randomly selected from a Veterans Affairs database. The database contains the processed and unprocessed data of patients referred for a renal imaging examination because of suspicion of RVH. The preponderance of male subjects was due to the fact that the patient population came from a Veterans Administration Hospital. Entry criteria consisted of all patients referred and archived for possible RVH beginning February 6, 2012, and we chose 50 studies by working backward sequentially. Two of the patients suspected of having RVH had incomplete datasets and were excluded from further analysis, and four had a single kidney; consequently, 48 patients (92 kidneys) were available for evaluation.
Acquisition Protocol
All patients were hydrated with 500 mL of water and positioned supine with the scintillation camera detector placed under the table.
Patients suspected of having obstruction.—Studies were performed by using separate baseline and furosemide (Hospira, San Diego, Calif) acquisitions, which represented a minor modification of the single-acquisition protocol recommended in the 1996 Santa Fe Consensus Report on diuresis renography, in which furosemide was administered 20 minutes after injection of a tracer (1). A three-phase dynamic acquisition (baseline examination) was begun after the injection of 374.1 MBq ± 29.6 of 99mTc-MAG3. Phase 1 consisted of 24 2-second frames, phase 2 consisted of 16 15-second frames, and phase 3 consisted of 40 30-second frames. At the end of the baseline acquisition, an additional postvoid 2-minute image was obtained of the kidneys with the patient in the supine position; 1-minute anterior prevoid and postvoid bladder images also were obtained to determine residual urine volume. For all the patients suspected of having obstruction, the baseline examination demonstrated one or both kidneys to have abnormal or equivocal uptake and/or drainage; consequently, each patient received a subsequent intravenous injection of furosemide followed immediately by a second 20-minute dynamic acquisition consisting of 40 frames of 30-second images. The majority of patients (76%) received 40 mg of furosemide as recommended in consensus reports (1,4); one patient received 20 mg and 22% received a higher dose of furosemide because of poor baseline renal function (14).
Patients suspected of having RVH.—We used the 1-day imaging protocol and followed published guidelines for baseline and angiotensin converting enzyme inhibition studies obtained on the same day (15,16). A baseline acquisition was obtained after a low-dose injection of 99mTc-MAG3 (62.9 MBq ± 40.7). Patients then received an intravenous injection of 0.04 mg/kg (a maximum of 2.5 mg) of the angiotensin converting enzyme inhibitor enalaprilat (Teva Parenteral Medicines, Irvine, Calif). At least 15 minutes after administration of enalaprilat, the patient received a high-dose injection of 99mTc-MAG3 (303.4 MBq ± 48.1) followed by a second acquisition with the identical baseline acquisition protocol.
Data Processing
All patient studies were processed by using an updated in-house version of the QuantEM renal quantification program (GE Healthcare, Milwaukee, Wis) that was introduced in the mid-1990s. The current in-house software incorporates several quality control procedures to improve reproducibility and to detect patient motion automatically. The software also generates a series of common quantitative parameters to assist imaging interpretation, including the relative uptake, time-to-peak counts, and the 20-minute-to-maximum count ratio for the whole kidney and parenchymal regions of interest, as well as the T one-half for the whole kidney and pelvic regions of interest; the software also generates voiding indexes (postvoid-to-prevoid and postvoid-to-maximum count ratios) and a camera-based 99mTc-MAG3 clearance (4,17–19). The 99mTc-MAG3 clearance method has been validated previously in a multicenter trial (20). To process the studies, static image data were summed from frames obtained 2–3 minutes after injection. By using a filtered version of this image, whole kidney, parenchymal (cortical), and background regions of interest were automatically defined. The user had the option to override any of these automatic regions of interest and replace them with manual regions of interest. Background-subtracted curves were generated for the whole kidney for automatic calculation of multiple quantitative parameters (4,16,18,19). Relative uptake was calculated by using the software on the basis of the integral of counts in the kidney region of interest 60–150 seconds after the bolus reaches the kidneys (17). The imaging display included sequential 2-minute images, which were smoothed by using a three-pixel boxcar average in the x and y directions (Figs 1–3). The display also included patient demographics (height, weight, age, sex, and body surface area).
Figure 1a:

Planar 99mTc-MAG3 images of the kidneys in an 84-year-old man with hypertension, mild bilateral renal artery stenosis, diabetes with proteinuria level of 3 or more, and a serum creatinine level of 2.8 mg/dL. (a) Sequential 2-minute images after administration of low-dose (43.3 MBq,1.17 mCi) 99mTc-MAG3. (b) Sequential 2-minute images after administration of high-dose (203.5 MBq, 5.5 mCi) 99mTc-MAG3.
Figure 3a:

Planar 99mTc-MAG3 images of the kidneys in a 76-year-old man with hypertension, chronic renal failure, creatinine level of 1.3 mg/dL, and history of prostate cancer with pelvic radiation. (a) Sequential 2-minute images after administration of low-dose (40.7 MBq 1.1 mCi) 99mTc-MAG3. (b) Sequential 2-minute images after administration of high-dose (347.8 MBq, 9.4 mCi) 99mTc-MAG3.
Figure 1b:

Planar 99mTc-MAG3 images of the kidneys in an 84-year-old man with hypertension, mild bilateral renal artery stenosis, diabetes with proteinuria level of 3 or more, and a serum creatinine level of 2.8 mg/dL. (a) Sequential 2-minute images after administration of low-dose (43.3 MBq,1.17 mCi) 99mTc-MAG3. (b) Sequential 2-minute images after administration of high-dose (203.5 MBq, 5.5 mCi) 99mTc-MAG3.
Figure 2a:

Planar 99mTc-MAG3 images of the kidneys in a 52-year-old woman suspected of having RVH and serum creatinine level of 0.7 mg/dL. (a) Sequential 2-minute images after administration of low-dose (74 MBq, 2.0 mCi) 99mTc-MAG3. (b) Sequential 2-minute images after administration of high-dose (370MBq, 10.0 mCi ) 99mTc-MAG3.
Figure 2b:

Planar 99mTc-MAG3 images of the kidneys in a 52-year-old woman suspected of having RVH and serum creatinine level of 0.7 mg/dL. (a) Sequential 2-minute images after administration of low-dose (74 MBq, 2.0 mCi) 99mTc-MAG3. (b) Sequential 2-minute images after administration of high-dose (370MBq, 10.0 mCi ) 99mTc-MAG3.
Figure 3b:

Planar 99mTc-MAG3 images of the kidneys in a 76-year-old man with hypertension, chronic renal failure, creatinine level of 1.3 mg/dL, and history of prostate cancer with pelvic radiation. (a) Sequential 2-minute images after administration of low-dose (40.7 MBq 1.1 mCi) 99mTc-MAG3. (b) Sequential 2-minute images after administration of high-dose (347.8 MBq, 9.4 mCi) 99mTc-MAG3.
Imaging Interpretation
Three nuclear medicine physicians (A.T.T., E.V.D., R.H., each with 30 years or more of experience in nuclear medicine) independently interpreted each examination. All three physicians had access to a FileMaker Pro database containing abstracted clinical information for each patient (21).
Patients suspected of having obstruction.—Two separate comparisons were performed. Initially, the baseline and diuretic acquisitions were interpreted without the flow images; readers scored each kidney on a scale from 1.0 to −1.0; scores greater than or equal to 0.20 indicated a diagnosis of obstruction, with higher scores approaching 1.0, indicating greater confidence in the diagnosis of obstruction. Scores from 0.19 to −0.19 were indeterminate, and scores of less than or equal to −0.2 indicated nonobstructed kidneys, with lower scores (those approaching −1.0) indicating greater confidence in the absence of obstruction. After scoring each kidney, the readers were shown 2-second flow images (Fig 4) and asked to score each kidney again for the presence or absence of obstruction on the basis of the additional information provided by the flow images.
Figure 4:

Sequential 2-second planar flow images of the intial 99mTc-MAG3 bolus (373.7 MBq [10.1 mCi]) as it transits abdominal aorta and kidneys in 44-year-old man with creatinine level of 1.05 mg/dL and moderate left hydronephrosis.
This study design incorporated the possibility of bias because the readers knew their initial scores when they rescored the examinations with the addition of the flow images. To avoid the recall bias that may have been introduced by the study design, readers were blinded to their original scores and independently reinterpreted all 50 examinations (98 kidneys) with access to the flow images approximately 2 years after their initial interpretations.
Patients suspected of having RVH.—As in the patients suspected of having obstruction, two separate analyses were performed. Initially, the baseline and enalaprilat 99mTc-MAG3 acquisitions were interpreted without flow images; readers scored each kidney for the presence of RVH on the 1.0 to −1.0 scale. After scoring each kidney, the readers were immediately given access to the 2-second flow images and were asked to score each kidney again on the basis of the additional information. To avoid recall bias, readers were blinded to their original scores and independently reinterpreted all 48 examinations (92 kidneys) with access to the flow images approximately 2 years after their initial interpretations.
Statistical Analysis
Power calculations were performed for two outcomes: score and relative uptake measurements. By using a standard deviation of 0.25 obtained from interrater variability of a separate study (22), a sample size of 50 kidneys provided 80% power to detect a minimum difference of 0.10 between scores at a significance level of .05 (if a difference existed). With a standard deviation of 4.0 percentage units obtained from the standard deviation of relative uptake measurements in a normal population (23), a sample size of 50 kidneys provided power of 0.98 to detect a difference of 3.0 percentage units at a significance level of .05 (if a difference existed). Our study consisted of 98 kidneys suspected of obstruction and 92 kidneys for RVH studies, which provided considerably high power for detection of even very small differences (<0.10 for the score and 3.0 percentage units for the relative uptake) if they existed.
The difference between scores (with and without the flow images) was analyzed by using a random effects analysis of variance, which accounted for possible correlations among raters and for the correlation from the left and right kidneys of the same patient. Adjusted means and standard errors of the means from analysis of variance were presented for the left kidney, right kidney, and both kidneys combined. Relative uptake data were analyzed by using a paired t test; a plot with a regression line was presented to provide the relationship between the high- and low-dose relative uptake values.
Results
Patients Suspected of Having Obstruction
When readers scored each initial examination and then immediately rescored each examination with access to the flow images and their original scores, two of the three readers had no changes in their initial scores, while the third reader changed the scores of only two of the 98 kidneys evaluated, one from −0.7 to −0.3 and another from −0.6 to −0.5. In neither case did the change in score change the diagnosis of nonobstruction. One of these patients had a urinary diversion partially overlying the kidney, and the other had a possible urinoma; the reader used the flow study to help evaluate the renal parenchyma before any urine was excreted. Moreover, there was no significant difference in the scores before and after the addition of the flow images; the mean of the differences was −0.0017; standard error, 0.0017 (95% confidence interval: −0.0089, 0.0056; P = .42).
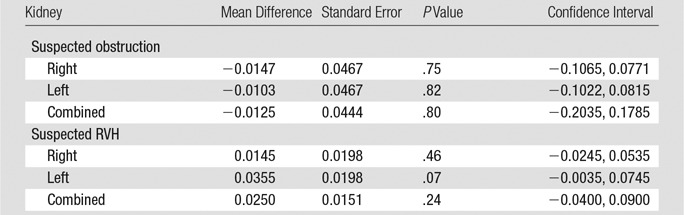
The study design mirrored clinical practice, in which a radiologist may form an impression on the basis of the initial analysis of an image but then may modify that impression as additional images or clinical data become available. This design, however, had the potential to bias the readers, since they had knowledge of their initial scores when they were given access to the flow images. To avoid this bias, the three readers were blinded to their initial scores and independently rescored the studies with the flow images approximately 2 years after the initial interpretation. Again, there was no significant difference between the initial scores without the flow images and the later scores with the flow images; the mean difference in these scores, standard error of the mean, 95% confidence interval, and P value for the right and left kidneys and both kidneys combined are provided in the Table.
Mean Difference in Blinded Reader Scores
Patients Suspected of Having RVH
For the initial comparison, readers interpreted each examination and then reinterpreted it with access to the flow images and their original scores. Two of the three readers had no change in their initial scores with the addition of the flow images; the third reader changed the score of only one of the 92 kidneys evaluated; the change in score was from 0 to 0.1, which did not affect the indeterminate diagnosis of RVH. Moreover, there was no significant difference in the scores before and after the addition of the flow images; the mean of the difference in the scores was −0.0004; standard error, 0.0004 (95% confidence interval: −0.0019, 0.0012; P = .42).
Again, because readers may have been biased in the initial reading by knowledge of their scores without the flow images, the three readers were blinded to their initial scores, and they independently rescored the studies with the flow images approximately 2 years later. Again there was no significant difference between the initial scores without the flow images and the later scores with the flow images; the mean difference in these scores, standard error, 95% confidence interval, and P value for the right and left kidneys and both kidneys combined are provided in the Table.
Measurement of Relative Uptake
The relative uptake of the right and left kidneys calculated after the low-dose (62.9 MBq ± 40.7 ) acquisition was compared with the relative uptake of the right and left kidneys calculated after a high-dose (303.4 MBq ± 48.1) acquisition after administration of enalaprilat. There was no significant difference in the relative uptake of 99mTc-MAG3 at high and low levels of activity for the left kidney (P = .32); the mean difference ± standard error of the mean was 0.75 ± 0.747 (95% confidence interval: −0.734, 2.234). Similarly, there was no significant difference in the relative uptake of 99mTc-MAG3 at high and low levels of activity for the right kidney (P = .32); the mean difference was −0.75 ± 0.747 (95% confidence interval: −2.234, 0.734).
The relationship of relative uptake with low and high doses for the left kidney is shown in Figure 5; the slope of the regression line was 1.02 (95% confidence interval: 0.94, 1.10), the correlation coefficient was 0.96 (95% confidence interval: 0.94, 0.98), and the intercept was −0.23 (95% confidence interval, −4.84, 4.37). For the right kidney, the slope of the regression line was 1.02 (95% confidence interval: 94, 1.10), the correlation coefficient was 0.96 (95% confidence interval: 0.94, 0.98), and the intercept was −1.65 (95% confidence interval: −5.91, 2.61). For both left and right kidneys, the slopes of the regression lines were not significantly different from 1, and intercepts were not significantly different from zero. These results show that relative uptake values are not affected by the amount of the dose.
Figure 5:

Scatterplot shows relative uptake of left kidney after low-dose (62.9 MBq ± 40.7) acquisition and high-dose (303.4 ± 48.1 MBq) acquisition after administration of enalaprilat. Mean slope of regression line ± standard error of the mean for respective relative uptake values was 1.02 ± 0.04, not significantly different from unity (P = .65). Correlation coefficient was 0.96 and mean intercept ± standard error of the mean was −0.23 ± 2.29, not significantly different from zero (P = .92). CI = confidence interval.
Discussion
Our major finding is that visual inspection of the radionuclide angiogram had no effect on the interpretation of 99mTc-MAG3 examinations obtained in patients suspected of having obstruction or RVH. Consequently, for these indications, administration of doses in the range of 300–370 MBq or higher to adequately visualize the bolus as it transits the aorta and kidneys cannot be justified on the basis of more accurate imaging interpretation. Our study had more than adequate power (greater than 0.8) to detect a small difference of 0.1, which represents a 5% difference on our scale and, unless that change was on the decision cusp of 0.2 or −0.2, a 5% change would not be clinically meaningful. Another important finding of our study was the observation that there was no significant difference in relative uptake measurements obtained after administration of doses in the range of 37–74 mBq (1–2 mCi) compared with administration of much higher doses in the range of 300–370 MBq (8–10 mCi). Power analysis confirmed that the test had adequate power; we could detect any difference greater than three percentage units at a significance level of .05 with a power of 0.98. Although determination of relative renal function is another common indication for a renal examination, there is no need to administer high doses to increase the accuracy of the relative renal function determination.
A major past indication for a renal imaging examination was for evaluation of transplants (11,13). Visual and quantitative evaluation of the radionuclide angiogram helped to distinguish between acute tubular necrosis and rejection with the use of administered doses in the 444–740 MBq (12–20 mCi) range (11,24). When 99mTc-MAG3 was introduced in the late 1980s, evaluation of renal transplants was still an important indication, and many institutions, including our own, adopted a protocol for using 370 MBq (10 mCi) of 99mTc-MAG3, the upper level of activity suggested by the 99mTc-MAG3 package insert (5). As the number of examinations for transplant evaluation became progressively less frequent and almost disappeared, the 370 MBq (10 mCi) protocol and the perceived importance of the radionuclide angiogram for optimal imaging interpretation persisted. Once a specific protocol is established and adopted by clinicians and technologists, it may tend to remain in textbook recommendations and clinical practice even when the rationale for the protocol no longer exists. The persistence of high administered doses of 99mTc-MAG3 is supported by results of recent publications (8,25,26) and the fact that most unit doses dispensed by the three major nuclear pharmacies in the Atlanta metropolitan market are still in the 300–370 MBq range. Atlanta is a large metropolitan market and is likely representative of radiopharmaceutical practices of similar centers throughout the United States.
The concept of restricting administration to lower doses of 99mTc-MAG3 (37–185 MBq) is supported by expert recommendations and recent guidelines (4,9,10,27–29). Of note, guidelines for suspected RVH recommend administering 37 MBq (1 mCi) for the baseline component of the 1-day protocol (15,16). An important implication of the 1-day protocol is that that both image quality and quantitative assessment of the baseline imaging examination are considered to be acceptable after a very low dose administration of 37–74 MBq (1–2 mCi). More senior radiologists and nuclear medicine physicians will remember when renal imaging examinations were performed with only 11.1 MBq (300 μCi) of iodine 131-hippuran.
There were several limitations to our study. First, our results do not apply to patients referred for evaluation of renal transplants. Second, relative uptake was calculated on the basis of the integral of counts in the kidney from 1 to 2.5 minutes; there are other approaches to calculating relative uptake, and it is possible that one of these approaches may give different results for low and high levels of activities (30,31). Moreover, our conclusions were based on visual inspection of the radionuclide angiogram; it is conceivable that quantitative flow indexes generated after high administered doses might provide information that would affect the diagnosis of obstruction or RVH; however, support for this hypothesis would have to be demonstrated in well-designed studies before the routine administration of higher doses could be justified.
The as low as reasonably achievable, or ALARA, principle advocates minimizing risk by using the lowest radiation dose possible to achieve an acceptable diagnostic image. This principle has been incorporated in the Image Gently and Image Wisely campaigns and is clearly stated in the Image Wisely pledge, “to put my patient’s safety, health, and welfare first by optimizing imaging examinations to use only the radiation necessary to produce diagnostic quality images” (32,33). For radiologists and nuclear medicine physicians who still administer 99mTc-MAG3 doses in the 300–370 MBq range, our results offer the rationale and opportunity to substantially reduce the administered dose and effect a proportional reduction in the radiation dose to their patients.
Administered doses in the 300–370 MBq (approximately 8–10 mCi) range are required to obtain 2-second flow images of the initial bolus as it transits the kidneys, but these high administered doses do not improve the measurement of relative renal function, and 2-second flow images do not contribute to interpretation of renal examinations obtained in patients suspected of having obstruction or RVH. In conclusion, administration of doses of 99mTc-MAG3 in the range of 300–370 MBq (approximately 8–10 mCi) does not improve imaging interpretation and results in excess radiation to the patient; the results of our study support limiting the administered activity to 37–185 MBq (1.0–5.0 mCi) as advocated by expert recommendations and existing guidelines (1,4,9,10,27–29).
Advances in Knowledge
■ There was no statistically significant difference in the interpretation of renal images in patients suspected of having obstruction when readers had access to the radionuclide angiogram (2-seconds per frame images of the administered bolus of technetium 99m [99mTc] mertiatide [MAG3], because it transits the abdominal aorta and kidneys) compared with their interpretation without access to the radionuclide angiogram; examinations were scored on a scale of −1.0 to 1.0, and the mean difference in scores was −0.0125 (95% confidence interval: −0.2035, 0.1785; P = .80).
■ There was no statistically significant difference in the interpretation of renal images in patients suspected of having renovascular hypertension when readers had access to the radionuclide angiogram compared with their interpretations without access to the radionuclide angiogram; the mean difference in scores was 0.0250 (95% confidence interval: −0.040, 0.090; P = .24).
■ There was no significant difference in the measurement of relative uptake after administration of a low dose of 99mTc-MAG3 (mean ± standard deviation, 62.9 MBq ± 40.7) compared with a high-dose administration (mean, 303.4 MBq ± 48.1); the mean difference in relative uptake for the left kidney was 0.75 percentage units (95% confidence interval: −0.734, 2.34; P = .32).
Implications for Patient Care
■ There is no need to administer 300–370 MBq (approximately 8–10 mCi) of 99mTc MAG3 to achieve a count rate sufficient to obtain a radionuclide angiogram (2-second flow images of the bolus as it first transits the kidneys), because the radionuclide angiogram does not contribute to interpretation of imaging in patients referred for suspicion of obstruction or renovascular hypertension.
■ For most 99mTc-MAG3 renal imaging examinations, administration of doses as high as 300–370 MBq (approximately 8–10 mCi) fails to have a diagnostic effect and results in unnecessary radiation to the patient; our results support administration of doses for routine studies in the range of 37–185 MBq (1–5 mCi) as recommended by most experts and existing consensus guidelines.
Received October 20, 2015; revision requested December 5; revision received November 16, 2016; accepted December 8; final version accepted June 20.
Study supported by National Institute of Diabetes and Digestive and Kidney Diseases (R01DK108070-01A1, R37DK038842).
Disclosures of Conflicts of Interest: A.T.T. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: royalty payments for QuantEm software licensed by Emory University to GE Healthcare. Other relationships: disclosed no relevant relationships.R.D.F. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: royalty payments for QuantEm software licensed by Emory University to GE Healthcareroyalties and stock from Syntermed. Other relationships: disclosed no relevant relationships. A.K.M.F.R. disclosed no relevant relationships. A.P. disclosed no relevant relationships. E.V.D. disclosed no relevant relationships. R.H. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: royalty payments for QuantEm software licensed by Emory University to GE Healthcare royalties from Elgems and fees as an inspector for Intersocietal Accreditation Commission. Other relationships: disclosed no relevant relationships. A.M. disclosed no relevant relationships.
Abbreviations:
- MAG3
- mertiatide
- RVH
- renovascular hypertension
References
- 1.O’Reilly P, Aurell M, Britton K, Kletter K, Rosenthal L, Testa T. Consensus on diuresis renography for investigating the dilated upper urinary tract. Radionuclides in Nephrourology Group. Consensus Committee on Diuresis Renography. J Nucl Med 1996;37(11):1872–1876. [PubMed] [Google Scholar]
- 2.Shulkin BL, Mandell GA, Cooper JA, et al. Procedure guideline for diuretic renography in children 3.0. J Nucl Med Technol 2008;36(3):162–168. [DOI] [PubMed] [Google Scholar]
- 3.Gordon I, Piepsz A, Sixt R; Auspices of Paediatric Committee of European Association of Nuclear Medicine . Guidelines for standard and diuretic renogram in children. Eur J Nucl Med Mol Imaging 2011;38(6):1175–1188. [DOI] [PubMed] [Google Scholar]
- 4.Taylor AT, Blaufox MD, De Palma D, et al. Guidance document for structured reporting of diuresis renography. Semin Nucl Med 2012;42(1):41–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mallinckrodt Website . Technescan MAG3 Kit for the Preparation of Technetium Tc 99m Mertiatide. http://www.mallinckrodt.com/WorkArea/DownloadAsset.aspx?id=616. Accessed July 2, 2014.
- 6.Taylor A, Schuster DM, Alazraki N. A clinician’s guide to nuclear medicine. 2nd ed. Reston, Va: Society of Nuclear Medicine, 2006; 50. [Google Scholar]
- 7.Ziessman HA, O’Malley JP, Thrall JH, Fahey FH. Genitourinary system. In: The requisites: nuclear medicine. 4th ed. Philadelphia, Pa: Elsevier Saunders, 2014; 175. [Google Scholar]
- 8.Mettler FA, Jr, Giuiberteau MJ. Genitourinary system and adrenal glands. In: Essentials of nuclear medicine imaging. 6th ed. Philadelphia, Pa: Elsevier Saunders, 2012; 316. [Google Scholar]
- 9.Blaufox MD, Aurell M, Bubeck B, et al. Report of the Radionuclides in Nephrourology Committee on renal clearance. J Nucl Med 1996;37(11):1883–1890. [PubMed] [Google Scholar]
- 10.Prigent A, Cosgriff P, Gates GF, et al. Consensus report on quality control of quantitative measurements of renal function obtained from the renogram: International Consensus Committee from the Scientific Committee of Radionuclides in Nephrourology. Semin Nucl Med 1999;29(2):146–159. [DOI] [PubMed] [Google Scholar]
- 11.Hilson AJ, Maisey MN, Brown CB, Ogg CS, Bewick MS. Dynamic renal transplant imaging with Tc-99m DTPA (Sn) supplemented by a transplant perfusion index in the management of renal transplants. J Nucl Med 1978;19(9):994–1000. [PubMed] [Google Scholar]
- 12.Peters AM, Brown J, Crossman D, et al. Noninvasive measurement of renal blood flow with technetium-99m-DTPA in the evaluation of patients with suspected renovascular hypertension. J Nucl Med 1990;31(12):1980–1985. [PubMed] [Google Scholar]
- 13.el Maghraby TA, van Eck-Smit BL, de Fijter JW, Pauwels EK. Quantitative scintigraphic parameters for the assessment of renal transplant patients. Eur J Radiol 1998;28(3):256–269. [DOI] [PubMed] [Google Scholar]
- 14.Taylor AT. Radionuclides in nephrourology, Part 2: pitfalls and diagnostic applications. J Nucl Med 2014;55(5):786–798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Taylor A, Nally J, Aurell M, et al. Consensus report on ACE inhibitor renography for detecting renovascular hypertension. Radionuclides in Nephrourology Group. Consensus Group on ACEI Renography. J Nucl Med 1996;37(11):1876–1882. [PubMed] [Google Scholar]
- 16.Taylor A, Blaufox MD, Dubovsky EV, et al. Society of Nuclear Medicine procedure guideline for diagnosis of renovascular hypertension 3.0. Procedure guidelines, Policy and Practice. http://www.snm.org. Published 2003. Accessed February 3, 2017. [PubMed]
- 17.Taylor A, Jr, Corrigan PL, Galt J, et al. Measuring technetium-99m-MAG3 clearance with an improved camera-based method. J Nucl Med 1995;36(9):1689–1695. [PubMed] [Google Scholar]
- 18.Folks RD, Manatunga D, Garcia EV, Taylor AT. Automated patient motion detection and correction in dynamic renal scintigraphy. J Nucl Med Technol 2011;39(2):131–139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bao J, Manatunga A, Binongo JN, Taylor AT. Key variables for interpreting 99mTc-mercaptoacetyltriglycine diuretic scans: development and validation of a predictive model. AJR Am J Roentgenol 2011;197(2):325–333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Taylor A, Jr, Manatunga A, Morton K, et al. Multicenter trial validation of a camera-based method to measure Tc-99m mercaptoacetyltriglycine, or Tc-99m MAG3, clearance. Radiology 1997;204(1):47–54. [DOI] [PubMed] [Google Scholar]
- 21.Folks RD, Savir-Baruch B, Garcia EV, Verdes L, Taylor AT. Development of a relational database to capture and merge clinical history with the quantitative results of radionuclide renography. J Nucl Med Technol 2012;40(4):236–243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Taylor A, Shenvi N, Folks R, et al. Tc-99m MAG3 diuretic renography: Impact of a decision support system (iRENEX) on resident interpretations. J Nucl Med 2013;54(Suppl 2):562. [Google Scholar]
- 23.Esteves FP, Taylor A, Manatunga A, Folks RD, Krishnan M, Garcia EV. 99mTc-MAG3 renography: normal values for MAG3 clearance and curve parameters, excretory parameters, and residual urine volume. AJR Am J Roentgenol 2006;187(6):W610–W617. [DOI] [PubMed] [Google Scholar]
- 24.Kirchner PT, Rosenthall L. Renal transplant evaluation. Semin Nucl Med 1982;12(4):370–378. [DOI] [PubMed] [Google Scholar]
- 25.Parikh KR, Davenport MS, Viglianti BL, Hubers D, Brown RK. Cost-savings analysis of renal scintigraphy, stratified by renal function thresholds: mercaptoacetyltriglycine versus diethylene triamine penta-acetic acid. J Am Coll Radiol 2016;13(7):801–811. [DOI] [PubMed] [Google Scholar]
- 26.Takahara N, Saga T, Inubushi M, et al. Drugs interacting with organic anion transporter-1 affect uptake of Tc-99m-mercaptoacetyl-triglycine (MAG3) in the human kidney: therapeutic drug interaction in Tc-99m-MAG3 diagnosis of renal function and possible application of Tc-99m-MAG3 for drug development. Nucl Med Biol 2013;40(5):643–650. [DOI] [PubMed] [Google Scholar]
- 27.Muller-Suur R, Prigent A. Radiopharmaceuticals: their intrarenal handling and localization. In: Ell PJ, Gambhir SS, eds. Nuclear medicine in clinical diagnosis and treatment. 3rd ed. London, England: Churchill Livingstone/Elsevier, 2004; 1501–1515. [Google Scholar]
- 28.Brown SCW. Nuclear medicine in the clinical diagnosis and treatment of obstructive uropathy. In: Ell PJ, Gambhir SS, eds. Nuclear medicine in clinical diagnosis and treatment. 3rd ed. London, England: Churchill Livingstone/Elsevier, 2004; 1581–1602. [Google Scholar]
- 29.Oei H, Oei Y. Dynamic and static renal imaging. In: Ell PJ, Gambhir SS, eds. Nuclear medicine in clinical diagnosis and treatment. 3rd ed. London, England: Churchill Livingstone/Elsevier, 2004; 1517–1535. [Google Scholar]
- 30.Lythgoe MF, Gordon I, Khader Z, Smith T, Anderson PJ. Assessment of various parameters in the estimation of differential renal function using technetium-99m mercaptoacetyltriglycine. Eur J Nucl Med 1999;26(2):155–162. [DOI] [PubMed] [Google Scholar]
- 31.Wesolowski MJ, Conrad GR, Šámal M, et al. A simple method for determining split renal function from dynamic (99m)Tc-MAG3 scintigraphic data. Eur J Nucl Med Mol Imaging 2016;43(3):550–558. [DOI] [PubMed] [Google Scholar]
- 32.Jafari ME, Daus AM. Applying Image Gently SM and Image Wisely SM in nuclear medicine. Health Phys 2013;104(2 Suppl 1):S31–S36. [DOI] [PubMed] [Google Scholar]
- 33.Brink JA, Amis ES, Jr. Image Wisely: a campaign to increase awareness about adult radiation protection. Radiology 2010;257(3):601–602. [DOI] [PubMed] [Google Scholar]