

Abstract
Objectives
The aim of this study was to assess the socioeconomic inequality in malnutrition in under-5 children in Iran in order to help policymakers reduce such inequality.
Methods
Data on 8443 under-5 children were extracted from the Iran Multiple Indicator Demographic and Health Survey. The wealth index was used as proxy for socioeconomic status. Socioeconomic inequality in stunting, underweight, and wasting was calculated using the concentration index. The concentration index was calculated for the whole sample, as well as for subcategories defined in terms of categories such as area of residence (urban and rural) and the sex of children.
Results
Stunting was observed to be more prevalent than underweight or wasting. The results of the concentration index at the national level, as well as in rural and urban areas and in terms of children’s sex, showed that inequality in stunting and underweight was statistically significant and that children in the lower quintiles were more malnourished. The wasting index was not sensitive to socioeconomic status, and its concentration index value was not statistically significant.
Conclusions
This study showed that it can be misleading to assess the mean levels of malnutrition at the national level without knowledge of the distribution of malnutrition among socioeconomic groups. Significant socioeconomic inequalities in stunting and underweight were observed at the national level and in both urban and rural areas. Regarding the influence of nutrition on the health and economic well-being of preschool-aged children, it is necessary for the government to focus on taking targeted measures to reduce malnutrition and to focus on poorer groups within society who bear a greater burden of malnutrition.
Keywords: Malnutrition, Child, Sex, Socioeconomic factors, Iran
INTRODUCTION
Adequate nutrition in the early stages of children’s lives is essential to ensure the proper development of organs and their optimal performance, the development of a strong immune system, and adequate mental growth and development [1]. Economic growth and social development require a well-nourished population so that individuals are capable of learning new skills and contributing to society [2]. Malnutrition in children occurs when their bodies do not receive adequate amounts of calories, proteins, carbohydrates, fat, vitamins, minerals, and other micronutrients necessary for the health of their organs and their proper functioning [3]. Malnutrition has long-term consequences on children’s intellectual abilities, economic productivity, and vulnerability to heart and metabolic diseases. It directly or indirectly accounts for more than one-third of all deaths and 21% of disability-adjusted life years in children [1-4].
The prevalence of malnutrition in the world has generally declined; from 2000 to 2013, the prevalence of stunting diminished from 33 to 25%, and the prevalence of underweight decreased from 25 to 15% from 1990 to 2013. However, according to the World Health Organization (WHO), the World Bank, and the United Nations Children’s Fund in 2013, approximately 161 million children in the world suffered from chronic stunting and 99 million children suffered from underweight [5]. Malnutrition is also a major challenge for the health sector and is the main factor contributing to child mortality in the Eastern Mediterranean Region, as defined by the WHO, to the extent that it causes 50% of deaths in children under 5 years of age in this region [6].
As in other countries, the prevalence of malnutrition in Iran has declined and the average indices of stunting and underweight have dropped from 19% to around 7% and from 17 to 6%, respectively [7,8]. Over the past 3 decades, improved diets and public health policies such as the establishment of health centers have increased vaccination coverage, and access to safe water and improved sanitation facilities have caused the prevalence of child malnutrition in Iran to decline [9-11]. Nonetheless, according to recent provincial studies, chronic malnutrition remains a health problem in Iran. For example, 11% of the under-5 children in Kerman and 16% in Sistan and Baluchestan suffer from stunting [12-15]. Additionally, according to the United Nation International Children Emergency Fund, the presence of multiple causes of malnutrition and several unknown aspects of malnutrition are the reasons that it has been neglected in Iran, and inequality in the malnutrition burden in the provinces of the country is considered to be a challenge [11]. In this regard, the WHO reported that Iran was among the countries with major differences between socioeconomic groups in terms of chronic malnutrition [6].
However, a common characteristic of all recent studies conducted in Iran on malnutrition among under-5 children is that they have all studied the prevalence of malnutrition in a particular period or its trend over time [12-14]. Since malnutrition is a complicated phenomenon, for which socioeconomic factors such as the educational level of the parents as well as household income are relevant [16-18], it shows large disparities among socioeconomic groups [19-21]. Therefore, it seems necessary to have a clear picture of the nutritional status of children among various socioeconomic groups in Iran in order to identify the patterns of inequality and to determine the vulnerable groups that should be targeted for interventions, with the goal of developing suggestions for policymakers about how to reduce this inequality.
METHODS
Data
The study data were extracted from a national survey of households entitled the Iran Multiple Indicator Demographic and Health Survey (IrMIDHS). This survey was conducted by the National Institute Health Research and Ministry of Health in 2010. The IrMIDHS aimed to produce valid nation-wide data on health and population indices in order to assess the impact of social indicators on the health of children and women and to help policymakers develop effective strategies to improve health outcomes and reduce inequalities [8]. In this cross-sectional survey, multi-stage stratified cluster sampling was used. Due to significant differences in the population size across different provinces of Iran and the districts within provinces, each province’s share in the total sample size as well as each region’s share in the provinces was first specified. Subsequently, random samples of clusters in each district were weighted based on the rural and urban populations within each region. Each cluster consisted of 10 households.
In order to obtain a clear picture of the social indicators within each province, the minimum number of clusters in each province was increased to 40, and ultimately 3096 clusters (30 960 households), including 909 rural clusters and 2187 urban clusters, were selected as the sample of the IrMIDHS. The IrMIDHS included a household questionnaire (107 questions), a questionnaire for women aged 15-54 (145 questions) and a questionnaire about under-5 children (88 questions), which were completed by conducting face-to-face interviews with household members. A total of 29 609 household questionnaires (response rate, 95%) and 9298 under-5 children questionnaires (response rate, 99%) were completed [22].
To assess the socioeconomic inequalities in child malnutrition, we included 8443 children in this study, from whom data on height, weight, age, and sex as well as data related to their socioeconomic status had been collected accurately and completely.
The Persian versions of the IrMIDHS questionnaires are available at http://nihr.tums.ac.ir.
Measurements of Socioeconomic Status
No information about household income or expenditures was collected in the IrMIDHS. In general, in the absence of income or expenditure data, proxies such as the asset-based wealth index can be used to assess households’ socioeconomic status. Hence, we used the wealth index created through the principal component analysis statistical method, which has already been used successfully in previous studies to measure socioeconomic inequalities and is especially recommended for low-income and middle-income countries [23,24].
Two major categories of variables, including household assets (such as TV sets, refrigerators, freezers, radios, cell phones, wristwatches, computers, laptops, microwaves, washing machines, vacuum cleaners, washing machines, and cars) and household features (such as heating and cooling systems, types of fuel in the kitchen, access to the internet, sources of drinking water, bathrooms, number of rooms, toilets, and home ownership) were used to construct the wealth index. The wealth index was divided into 5 quintiles (poorest, poor, middle, rich, and richest) for use in the subsequent analysis.
Measurements of Malnutrition
It is common to use anthropometric indicators to assess the nutritional status of under-5 children [25]. The anthropometric indicators height-for-age, weight-for-age, and weight-for-height were calculated using the data collected in surveys on the height, weight, and age of the children. To assess the nutritional status of the children, the anthropometric indicators, calculated as the Z-score, were used to compare the weight and height of the children with the weight and height of the same children in the reference population in terms of age and sex.
If the Z-score value for each anthropometric indicator for a child was more than 2 standard deviations (SDs) below the corresponding value for the reference population, the child was considered to be malnourished. In this study, the child growth standard introduced by the WHO in 2006 was used to calculate the Z-score [26].
According to the measurements of the abovementioned indicators, the following 3 forms of malnutrition can be defined: stunting (if the Z-score value for height-for-age is more than 2 SDs below the corresponding value of the reference population), wasting (if the Z-score value for weight-for-height is more than 2 SDs below the corresponding value of the reference population) and underweight (if the Z-score value for weight-for-age is more than 2 SDs below the corresponding value of the reference population). The outlier values of height-for-age Z-scores (lower than -5 and higher than +3), weight-for-age Z-scores (lower than -5 and higher than +5) and weight-for-height Z-scores (lower than -5 and higher than +4) were excluded from the analyses, according to WHO guidelines [27].
Malnutrition Inequality Analysis
Inequalities in stunting, underweight, and wasting were analyzed using the concentration curve and concentration index.
Concentration curve
The concentration curve shows how a health or disease outcome is distributed among different socioeconomic groups. On its horizontal axis, the cumulative percentage of the samples is arranged according to socioeconomic status, from poor to rich, while on the vertical axis, the cumulative percentage of the health or disease outcome is shown. If the disease occurs unequally among poorer socioeconomic groups, the concentration curve will be above the equality line. On the contrary, if the disease or health variable is concentrated among the rich, the concentration curve will be below the equality line; and finally, the concentration curve will coincide with the equality line if the health or disease variable is equally distributed among socioeconomic groups. In the present study, also we used the dominance test presented by O’Donnell et al. [28] to examine the significance of the concentration curve of the stunting, underweight, and wasting indices with regard to the equality line (45°) at the 5% level.
Concentration index
The concentration index is obtained from the enclosed space between the concentration curve and the equality line. If the concentration curve is above the equality line, the index will be negative, showing that the condition is concentrated among the poor. However, if the concentration curve is below the equality line, the index will be positive, indicating that the focus of the condition is among the rich. The concentration index can be expressed in different ways, but one of the most widely used methods, proposed by Kakwani [29], is as follows:
| (1) |
In this equation yi shows the health outcome of interest (e.g., malnutrition) of the ith individual, μ indicates its mean, and Ri represents the fractional rank of the ith individual in the distribution of socioeconomic status. The concentration index ranges from -1 to +1, where -1 indicates the full concentration of the disease in the poorest quintile and +1 indicates the full concentration of the disease in the richest quintile. If the disease or health condition is equally distributed among the quintiles, the concentration index will be equal to zero.
In this study, the concentration indices for stunting, underweight, and wasting at the national level and according to various subcategories, including place of residence (rural or urban) and the sex of the children, were estimated separately. The bootstrap resampling technique with 500 bootstrap samples was used to calculate the concentration index and standard error. All analyses were done using Stata version 14.1 (StataCorp, College Station, TX, USA).
Ethics
All analyses in this study were based on the data contained in the survey, and for ethical reasons, information on the identity of individuals and households was removed. Furthermore, a consent form was signed by the heads of the households and mothers at the time that the initial data were collected by the IrMIDHS team.
RESULTS
Table 1 shows the descriptive statistics of the under-5 children in the present study. The average values of the height-for-age, weight-for-age, and weight-for-height Z-scores were 0.60, 0.62, and 0.44, respectively. There were somewhat more male children than female children (51.10% vs. 48.90%). A significant majority of the children (63.34%) lived in urban areas, while 36.66% lived in rural areas. The average number of people in each family was 4.4, and the distribution of the children in the study was almost the same across the socioeconomic quintiles.
Table 1.
Summary statistics for under-5 children based on data from the Iran Multiple Indicator Demographic Health Survey, 2010
| Variable | n | % | Mean | Standard deviation |
|---|---|---|---|---|
| Z-score | ||||
| Height-for-age | 0.60 | 1.12 | ||
| Weight-for-age | 0.62 | 0.72 | ||
| Weight-for-height | 0.44 | 0.64 | ||
| Sex of child | ||||
| Male | 4314 | 51.10 | ||
| Female | 4129 | 48.90 | ||
| Age of child (mo) | ||||
| <6 | 782 | 9.26 | ||
| 6-12 | 837 | 9.91 | ||
| >12 | 6824 | 80.82 | ||
| Area of residence | ||||
| Rural | 3095 | 36.66 | ||
| Urban | 5348 | 63.34 | ||
| Breastfeeding duration (y) | 1.04 | 0.19 | ||
| No. of under-5 children in household | 1.26 | 0.50 | ||
| Size of household | 4.38 | 1.60 | ||
| Socioeconomic status | ||||
| Poorest | 1689 | 20.00 | ||
| Poor | 1700 | 20.14 | ||
| Middle | 1694 | 20.06 | ||
| Rich | 1690 | 20.02 | ||
| Richest | 1670 | 19.78 |
Table 2 shows the rates of stunting, underweight, and wasting at the national level, by area of residence, and by the sex of the child. The overall rate of stunting was higher than that of underweight or wasting, and its frequency at the national level was almost twice and three times as high as those of underweight and wasting, respectively.
Table 2.
Estimated rates (%) of stunting, underweight, and wasting in under-5 children at the national level, by area of residence, and by sex, Iran, 2010
| Stunting |
Underweight |
Wasting |
||||
|---|---|---|---|---|---|---|
| Rate (%) | p-value | Rate (%) | p-value | Rate (%) | p-value | |
| National | 10.13 | 5.70 | 3.29 | |||
| Area | ||||||
| Urban | 8.47 | <0.001 | 4.94 | <0.001 | 3.46 | 0.26 |
| Rural | 12.99 | 7.01 | 3.00 | |||
| Sex | ||||||
| Male | 10.38 | 0.42 | 5.70 | 0.98 | 3.34 | 0.81 |
| Female | 9.86 | 5.69 | 3.25 | |||
The rates of stunting and underweight were significantly higher in rural areas than in urban areas, although there was no significant relationship between wasting and place of residence. Although the rates of stunting, underweight, and wasting were slightly higher in males than in females, no significant relationships were found between any of the three malnutrition indices and the sex of the children (Table 2).
Table 3 shows the frequency of stunting, underweight, and wasting among under-5 children across socioeconomic quintiles at a national level. The rate of stunting, compared to underweight and wasting, was generally higher in all socioeconomic groups. The number of the children who suffered from malnutrition in the lowest socioeconomic quintile was higher than in other quintiles, and a decline in the frequency of stunting, underweight, and wasting could be seen as the socioeconomic quintiles increased. Table 3 also shows the odds ratios (ORs) of stunting, underweight, and wasting in children of other quintiles compared to the richest quintile. The OR for stunting in children of the four other quintiles showed a significant relationship in comparison to the baseline group, and the children in the lowest quintile had the highest OR. Regarding the underweight index, the OR at the 5% level was significant only for the poorest two groups compared to the richest quintile, and no significant ORs for the wasting index were found in a comparison between the other quintiles and the reference quintile using the chi-square test.
Table 3.
Frequency, estimated ORs, and 95% CIs of stunting, underweight, and wasting in under-5 children across socioeconomic quintiles, Iran, 2010
| Poorest | Poor | Middle | Rich | Richest | |
|---|---|---|---|---|---|
| Stunting | |||||
| Frequency (%) | 17.4 | 10.0 | 8.3 | 8.3 | 6.4 |
| OR (95% CI) | 3.04 (2.40, 3.80)* | 1.60 (1.24, 2.08)* | 1.32 (1.01, 1.73)* | 1.31 (1.00, 1.72)* | Reference |
| Underweight | |||||
| Frequency (%) | 9.7 | 5.0 | 5.3 | 4.5 | 3.8 |
| OR (95% CI) | 2.68 (1.98, 3.67)* | 1.40 (1.00, 1.98)* | 1.32 (0.93, 1.86) | 1.19 (0.84, 1.70) | Reference |
| Wasting | |||||
| Frequency (%) | 3.8 | 3.4 | 3.1 | 3.0 | 2.9 |
| OR (95% CI) | 1.29 (0.87, 1.92) | 1.20 (0.80, 1.79) | 1.01 (0.66, 1.53) | 1.00 (0.66, 1.52) | Reference |
OR, odds ratio; CI, confidence interval.
p<0.05 by the chi-square test.
Figure 1 shows the concentration curve of the stunting, underweight, and wasting indices of the under-5 children. The concentration curves for all three malnutrition indices were above the equality line. This implies that all three types of malnutrition were concentrated among children in poorer groups and that this group of children suffered more from malnutrition. To measure the significance of the concentration curve for each index (stunting, underweight, and wasting) with regard to the equality line, we used the stochastic dominance test. Using the dominance test at the significance level of 5%, the concentration curves for stunting and underweight indices statistically dominated the equality line; in other words, this result suggests that the concentration curves for the stunting and underweight indices were above the equality line to a statistically significant extent, but the concentration curve for the wasting index was not significantly above the equality line, lying almost tangent to it.
Figure. 1.
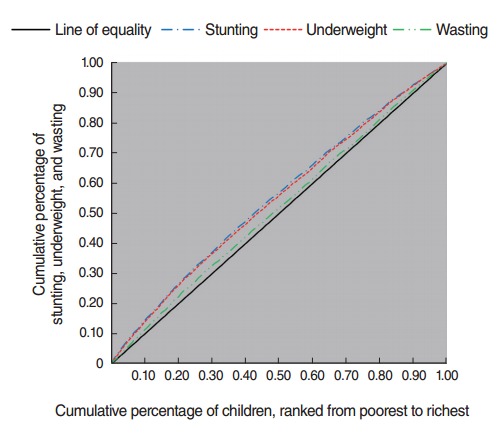
Concentration curve for child malnutrition in Iran, 2010.
As can be seen in Table 4, the concentration indices for stunting, underweight, and wasting at the national level were -0.177, -0.092, and -0.031, respectively. The results of the concentration index at the national level showed that the inequality in stunting and underweight was statistically significant and the children in lower quintiles suffered more from malnutrition. The negative value of the concentration indices for stunting and underweight in urban and rural areas also implies the existence of inequality, with these conditions concentrated among the lower quintiles. Our results also showed a significant difference between urban and rural areas in terms of inequality, and the lower quintile in urban areas bore a greater burden of stunting than in rural areas (Table 4). The stunting and underweight inequality pattern in terms of children’s sex likewise indicated a tendency for children in the lower quintiles to suffer more from malnutrition. The wasting index at the national level in terms of place of residence and sex of the children was not generally sensitive to socioeconomic status, and its concentration index value was not statistically significant.
Table 4.
Concentration indices (CIs) of stunting, underweight, and wasting among under-5 children at the national level, by area of residence, and by sex, Iran, 2010
| Stunting |
Underweight |
Wasting |
||||
|---|---|---|---|---|---|---|
| CI | p-value1 | CI | p-value1 | CI | p-value1 | |
| National | -0.177 | <0.001 | -0.092 | <0.001 | -0.031 | 0.37 |
| Area | ||||||
| Urban | -0.176 | <0.001 | - 0.073 | <0.001 | -0.031 | 0.43 |
| Rural | -0.107 | <0.001 | -0.094 | <0.001 | -0.053 | 0.13 |
| Diff 1 | 0.069 | 0.02 | -0.021 | 0.15 | -0.021 | 0.40 |
| Sex | ||||||
| Male | -0.176 | <0.001 | - 0.090 | <0.001 | -0.031 | 0.36 |
| Female | -0.178 | <0.001 | -0.095 | <0.001 | -0.031 | 0.51 |
| Diff 2 | -0.002 | 0.94 | -0.005 | 0.76 | 0.000 | 0.99 |
Diff 1, difference in the CI of under-5 child malnutrition between urban and rural; Diff 2, difference in the CI of under-5 child malnutrition between males and females.
Independent 2-tailed t-test to compare the values with 0.
DISCUSSION
Previous studies concerning child malnutrition in Iran have mainly focused on absolute levels of malnutrition and relative trends. Using IrMIDHS data, this study first investigated the prevalence of malnutrition at the national level and in urban and rural areas in Iran, and then measured the socioeconomic inequality in malnutrition among under-5 children.
The prevalence of child malnutrition was calculated using stunting, underweight, and wasting indices. Additionally, the rate of inequality in the malnutrition indices was measured through the concentration index. According to the present study, the rates of stunting, underweight, and wasting at the national level were found to be 10.13, 5.70, and 3.29%, respectively, and the values of the malnutrition indices in rural areas were slightly higher than in urban areas (Table 2). A comparison between the results of this study with those of previous surveys in Iran, such as Multiple Indicator Cluster Survey (1995) and Anthropometric Nutritional Indicators Survey (1999) reveals that in accordance with the global trend of malnutrition prevalence [5], there was a downward trend in the stunting, underweight, and wasting indices both nationally and in urban and rural areas.
Increased access to health services and the development of healthcare centers, as well as the promotion of public health indicators after the implementation of a primary health care network across the country on the one hand, and the establishment of the Multidisciplinary Program for Improvement of Nutritional Status of Children in Iran on the other hand, may be the main reasons that the prevalence of malnutrition has decreased in recent years in Iran [30].
An overall reduction of malnutrition can occur by neglecting the nutritional status of children in poor families and improving the nutrition of children in rich families. Moreover, the average reports of malnutrition indices at the national level can be misleading and may hide useful and vital subnational information that can be used for better and more appropriate policymaking [31,32]. Therefore, obtaining a clear picture of malnutrition in children across socioeconomic groups, especially the stunting index, which has a well-proven relationship with the socioeconomic status of children [18,20,33] seems essential for policymakers.
The concentration indices at the national level for stunting, underweight, and wasting were found to be -0.177, -0.092, and -0.031, respectively. Considering these values and the concentration curve (Figure 1), it is clear that, in general, poorer children suffer more from malnutrition. This is consistent with findings of previous studies on socioeconomic inequality in malnutrition, which have reported socioeconomic inequality in malnutrition to the detriment of lower socioeconomic groups. The concentration index of childhood malnutrition was reported to be -0.147 in Nigeria [34]. In the study conducted by Chen et al. [35] of childhood malnutrition in China, they found the concentration index, indicating socioeconomic inequality of under-5 childhood malnutrition, was −0.366. Using Demographic and Health Survey and Multiple Indicator Cluster Survey data in 80 countries, Bredenkamp et al. [36] showed that generally, the decrease in the prevalence of malnutrition was not accompanied by reduced socioeconomic inequality, and that in all countries malnutrition was concentrated in lower groups, with no exceptions. Furthermore, Van de Poel et al. [20] used Demographic and Health Survey data from 47 developing countries to investigate inequality in stunting and wasting. Their findings indicated that greater inequality in stunting, unlike wasting, occurred to the advantage of higher socioeconomic groups. Other studies in India [24], South Africa [31], China [37] and Ghana [31] confirmed socioeconomic inequality in malnutrition among children.
Investigating the inequality in malnutrition indices in terms of the place of residence can contribute to policymaking and prioritizing the regions where inequality is greater. As at the national level, the inequality when analyzed according to children’s place of residence was distributed to the detriment of poorer groups. While the rate of malnutrition indices in rural areas was higher, the concentration index value for stunting was greater in urban areas. This finding is in line with the results of other studies that have reported more inequality in stunting among children in urban areas [24,31,33]. It seems that a lack of resources and economic opportunities, as well as the rapid population growth in urban areas, may lead to reduced planning potential and increased marginalization; additionally, the diversity and wider range of variables relating to poverty, nutritional status, disease, and death are among the reasons for the increased inequality in urban areas [38-40].
Strengths and Limitations
This study has some advantages and some limitations. Since the data in the present study were extracted from the IrMIDHS survey at the national level with a large randomized sample, our findings can be generalized to the entire country.
One of the most important limitations of surveys such as the IrMIDHS is the absence of directly collected information about household expenditures and income; instead, the wealth index based on assets used in this study does not necessarily show results that correspond to those obtained using income and household variables, although the wealth index has fewer limitations in developing countries.
The data in this study were extracted from a cross-sectional survey. Therefore, interpretations should be made with caution.
In summary, like other studies, this study showed that the mean values of malnutrition indices at the national level, without knowledge of the distribution of malnutrition among different socioeconomic groups, might be misleading, and that evaluating the distribution of malnutrition among children is as important as assessing average malnutrition across the entire population. Significant socioeconomic inequality in malnutrition indices (stunting, underweight, and wasting), especially in stunting, was observed at the national level and in urban and rural areas. Regarding the influence of nutrition on the health and economic well-being of preschool-aged children, it is necessary for the government to focus on taking targeted measures to reduce malnutrition, as well as to focus on the poorer groups of society who bear a greater burden of malnutrition.
Acknowledgments
This study was part of a PhD thesis supported by the Iran University of Medical Sciences (grant no. IUMS/SHMIS_9221 504202). The authors hereby would like to thank Mrs. Sahar Goodarzi and Mr. Sajad Vahedi for their valuable guidance.
Footnotes
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
REFERENCES
- 1.Black RE, Allen LH, Bhutta ZA, Caulfield LE, de Onis M, Ezzati M, et al. Maternal and child undernutrition: global and regional exposures and health consequences. Lancet. 2008;371(9608):243–260. doi: 10.1016/S0140-6736(07)61690-0. [DOI] [PubMed] [Google Scholar]
- 2.Victora CG, Adair L, Fall C, Hallal PC, Martorell R, Richter L, et al. Maternal and child undernutrition: consequences for adult health and human capital. Lancet. 2008;371(9609):340–357. doi: 10.1016/S0140-6736(07)61692-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.United Nations Children’s Fund Facts for life. 2010 [cited 2017 May 1]. Available from: https://www.unicef.org/publications/files/Facts_for_Life_EN_010810.pdf.
- 4.World Health Organization Global nutrition policy review: what does it take to scale up nutrition action? [cited 2017 May 1]. Available from: http://apps.who.int/iris/bitstream/10665/84408/1/9789241505529_eng.pdf.
- 5.United Nations Children’s Fund. World Health Organization. World Bank UNICEFWHO-World Bank joint child malnutrition estimates-levels and trends. 2012 [cited 2017 May 1]. Available from: http://www.who.int/nutgrowthdb/jme_unicef_who_wb.pdf.
- 6.World Health Organization Regional Office for the Eastern Mediterranean Regional strategy on nutrition 2010-2019. 2010 [cited 2017 May 1]. Available from: http://apps.who.int/iris/handle/10665/122919.
- 7.Sheikholeslam R, Naghavi M, Abdollahi Z, Zarati M, Vaseghi S, Sadeghi Ghotbabadi F, et al. Current status and the 10 years trend in the malnutrition indexes of children under 5 years in Iran. Iran J Epidemiol. 2008;4(1):21–28. (Persian) [Google Scholar]
- 8.Rashidian A, Karimi-Shahanjarini A, Khosravi A, Elahi E, Beheshtian M, Shakibazadeh E, et al. Iran’s Multiple Indicator Demographic and Health Survey - 2010: study protocol. Int J Prev Med. 2014;5(5):632–642. [PMC free article] [PubMed] [Google Scholar]
- 9.Mehrdad R. Health system in Iran. Japan Med Assoc J. 2009;52(1):69–73. [Google Scholar]
- 10.Goudarzi S, Kameli ME, Hatami H. Improvement in health indicators of islamic republic of iran in the years 2004 and 2008. Iran Red Crescent Med J. 2011;13(8):574–577. [PMC free article] [PubMed] [Google Scholar]
- 11.Asaei SE, UNICEF Iran’s Specialist for Early Childhood Development Development. Iran’s excellent primary health care system. [cited 2017 May 12]. Available from: https://www.unicef.org/iran/media_4427.html.
- 12.Veghari G. The comparison of under-five-children’s nutrition status among ethnic groups in north of Iran, 1998-2013; results of a three stages cross-sectional study. Iran J Pediatr. 2015;25(4):e2004. doi: 10.5812/ijp.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Akhlaghi M, Sadri Z, Tabatabaee HR. Malnutrition frequency and its family-related factors among infants in Yasuj City in Iran, 2011. J Health Sci Surveill Syst. 2013;1(1):19–26. [Google Scholar]
- 14.Mohammadinia N, Sharifi H, Rezaei M, Heydari N. The prevalence of malnutrition among children under 5 years old referred to health centers in Iranshahr during 2010-2011. J Occup Health Epidemiol. 2012;1(3):139–149. [Google Scholar]
- 15.Gholami M, Dehghan A, Kargar N, Mohammadi P, Moosazadeh M, Hadizadeh H. Prevalence of malnutrition in children 7-12 years old in Kerman, 2013. J Community Health Res. 2014;4(2):261–266. [Google Scholar]
- 16.Wong HJ, Moy FM, Nair S. Risk factors of malnutrition among preschool children in Terengganu, Malaysia: a case control study. BMC Public Health. 2014;14:785. doi: 10.1186/1471-2458-14-785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Salvucci V. Determinants and trends of socioeconomic inequality in child malnutrition: the case of Mozambique, 1996–2011. J Int Dev. 2016;28(6):857–875. [Google Scholar]
- 18.Van de Poel E, Hosseinpoor AR, Jehu-Appiah C, Vega J, Speybroeck N. Malnutrition and the disproportional burden on the poor: the case of Ghana. Int J Equity Health. 2007;6:21. doi: 10.1186/1475-9276-6-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Fotso JC. Child health inequities in developing countries: differences across urban and rural areas. Int J Equity Health. 2006;5:9. doi: 10.1186/1475-9276-5-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Van de Poel E, Hosseinpoor AR, Speybroeck N, Van Ourti T, Vega J. Socioeconomic inequality in malnutrition in developing countries. Bull World Health Organ. 2008;86(4):282–291. doi: 10.2471/BLT.07.044800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kumar A, Singh A. Decomposing the gap in childhood undernutrition between poor and non-poor in urban India, 2005-06. PLoS One. 2013;8(5):e64972. doi: 10.1371/journal.pone.0064972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Rashidian A, Khosravi A, Khabiri R, Khodayari-Moez E, Elahi E, Arab M, et al. Islamic Republic of Iran’s Multiple Indicator Demograpphic and Healh Survey (IrMIDHS) 2010. Tehran: Ministry of Health and Medical Education; 2012. p. 131. (Persian) [Google Scholar]
- 23.Rarani MA, Rashidian A, Arab M, Khosravi A, Abbasian E. Inequality in under-five mortality in Iran: a national and subnational survey data analysis. Glob J Health Sci. 2016;9(3):215. [Google Scholar]
- 24.Chalasani S. Understanding wealth-based inequalities in child health in India: a decomposition approach. Soc Sci Med. 2012;75(12):2160–2169. doi: 10.1016/j.socscimed.2012.08.012. [DOI] [PubMed] [Google Scholar]
- 25.WHO Working Group Use and interpretation of anthropometric indicators of nutritional status. Bull World Health Organ. 1986;64(6):929–941. [PMC free article] [PubMed] [Google Scholar]
- 26.World Health Organization WHO child growth standard: length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. 2006 [cited 2017 May 12]. Available from: http://www.who.int/childgrowth/standards/Technical_report.pdf.
- 27.World Health Organization Physical status: the use of and interpretation of anthropometry, report of a WHO Expert Committee. 1995 [cited 2017 May 1]. Available from: http://apps.who.int/iris/bitstream/10665/37003/1/WHO_TRS_854.pdf. [PubMed]
- 28.O’Donnell O, van Doorslaer F, Wagstaff A, Lindelow M. Analyzing health equity using household survey data: a guide to techniques and their implementation. 2008 [cited 2017 May 1]. Available from: http://siteresources.worldbank.org/INTPAH/Resources/Publications/459843-1195594469249/HealthEquityFINAL.pdf.
- 29.Kakwani N, Wagstaff A, van Doorslaer E. Socioeconomic inequalities in health: measurement, computation, and statistical inference. J Econom. 1997;77(1):87–103. [Google Scholar]
- 30.Ghassemi H, Harrison G, Mohammad K. An accelerated nutrition transition in Iran. Public Health Nutr. 2002;5(1A):149–55. doi: 10.1079/PHN2001287. [DOI] [PubMed] [Google Scholar]
- 31.Zere E, McIntyre D. Inequities in under-five child malnutrition in South Africa. Int J Equity Health. 2003;2(1):7. doi: 10.1186/1475-9276-2-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Sousa A, Hill K, Dal Poz MR. Sub-national assessment of inequality trends in neonatal and child mortality in Brazil. Int J Equity Health. 2010;9:21. doi: 10.1186/1475-9276-9-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Mussa R. Explaining urban rural malnutrition inequality in Malawi. 2011 [cited 2017 May 19]. Available from: http://www.iariw.org/papers/2011/mussapaper.pdf.
- 34.Uthman OA. Using extended concentration and achievement indices to study socioeconomic inequality in chronic childhood malnutrition: the case of Nigeria. Int J Equity Health. 2009;8:22. doi: 10.1186/1475-9276-8-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Chen L, Wu Y, Coyte PC. Income-related children’s health inequality and health achievement in China. Int J Equity Health. 2014;13:102. doi: 10.1186/s12939-014-0102-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Bredenkamp C, Buisman LR, Van de Poel E. Persistent inequalities in child undernutrition: evidence from 80 countries, from 1990 to today. Int J Epidemiol. 2014;43(4):1328–1335. doi: 10.1093/ije/dyu075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Wu Y, Qi D. Urban-rural and provincial disparities in child malnutrition in China. Soc Work Public Health. 2016;31(6):574–588. doi: 10.1080/19371918.2015.1137524. [DOI] [PubMed] [Google Scholar]
- 38.World Health Organization Urbanization and health: health equity and vulnerable populations: case studies from the Eastern Mediterranean Region. 2010 [cited 2017 May 12]. Available from: http://apps.who.int/iris/bitstream/10665/119914/1/dsa1083.pdf.
- 39.Basta SS. Nutrition and health in low income urban areas of the third world. Ecol Food Nutr. 1997;6(2):113–124. [Google Scholar]
- 40.Bradley DJ, Stephens C, Harpham T, Cairncross S, World Bank . A review of environmental health impacts in developing country cities. Washington, DC: World Bank; 1992. p. 10. [Google Scholar]