

Abstract
Good to excellent results at long-term follow-up have been published for bone–patellar tendon–bone (BTB) graft anterior cruciate ligament reconstruction. Fixation using screws historically has been the most common choice for femoral and tibial bone blocks, but screws present several disadvantages, which include the risk of blowout (for which prevention implies having to shift the position of the tunnel anteriorly), as well as lesions of the bone blocks and tendons. This article describes a technique using Pullup BTB adjustable–loop length suspensory fixation (SBM, Lourdes, France) on the femoral and tibial sides. The graft is harvested and prepared classically. This device combines the advantages of suspensory fixation (precise position of the tunnel, high tensile strength), with the advantages of the adjustable loop (control of bone block position within the femoral tunnel, possibility of retightening the graft) and allows for double passage of the loop through each bone block for increased safety. So, it could represent an interesting and secure option for anatomic reconstruction of the anterior cruciate ligament when a BTB graft is chosen.
Initially described by Jones,1 anterior cruciate ligament (ACL) reconstruction using a bone–patellar tendon–bone (BTB) graft provides good long-term results. Even though it is not the main relevant factor in the case of failure, fixation of the graft is an important element of the surgical technique.2 ACL reconstruction with a BTB graft has mostly been described with an interference screw as femoral fixation.3 Cortical suspensory fixation has mainly been studied for hamstring tendon grafts. However, cortical fixation with suspensory fixation increases the area of contact between the graft and the bone4, 5 and decreases the risk of posterior wall blowout.6 Miyatake et al.7 described cortical fixation for a BTB graft but used a fixed-length device. Adjustable suspensory fixation could be a valuable option for BTB graft femoral fixation, but it needs to be adapted for use with a bone block. This article describes an ACL reconstruction technique with a BTB graft using Pullup BTB adjustable–loop length suspensory fixation (SBM, Lourdes, France) with femoral and tibial bone blocks.
Surgical Technique
The standard procedure is followed for harvesting the central one-third of the patellar tendon. The patient is placed in the supine position with the knee flexed to 90°. A tourniquet is usually used. A longitudinal incision is made between the patella and the tibial tuberosity. A 10-mm-wide part of the patellar tendon is isolated with a No. 15 scalpel blade, and 2 bone blocks, measuring 15 mm in length and 9 mm in width, are separated using a saw with a blade width of 10 mm. A narrower 5-mm saw blade is used to control the thickness of the bone block to be harvested to avoid cutting too much bone, which could cause a patellar fracture. Once the graft is completely detached from the knee, the bone defects are filled with bone wax to achieve local hemostasis. The 2 bone blocks are reshaped and calibrated. Usually, the patellar bone block is dedicated to the femoral tunnel and calibrated a half millimeter less than the tibial bone block to facilitate graft insertion. Moreover, the free extremity of the patellar bone block is remodeled in the shape of a cone to facilitate insertion of the block through the femoral socket. Next, the 2 blocks are drilled, each twice, by use of a 1.5-mm drill (Fig 1). One hole is placed in the middle of the block and the other at the bone-tendon junction.
Fig 1.

Position of holes in bone plugs: aspect of graft bone block with 2 different passages of loop. One should note that the first hole is drilled at the bone and tendon limit to respect a minimum distance of 1 cm between the 2 holes and to place the braid on strong cortical bone, reducing the risk of bone block breakage. The minimum bone block length must be 1.5 cm.
The next step is to attach the Pullup BTB adjustable suspensory fixation devices to the 2 bone blocks. First, the Pullup BTB is placed on the GraftTech table (SBM) (Fig 2). The bone block is secured on the movable end of the GraftTech device (Fig 3A). A needled suture loop is used to pull the Pullup white braided suture through the hole in the bone block (Fig 3 B and C, Video 1). This white braided suture is then passed through the opposite temporary black loop emerging from the white braid (Fig 3D). Two operators are required: The surgeon grabs the free white braided suture with one hand and the white braided suture previously folded through the black loop with the other hand, while his or her assistant grabs the thread ends of the temporary black loop opposite the white braided suture with one hand while firmly holding the Pullup button plate with the other hand. The assistant slowly pulls on the thread ends of the temporary black loop, while the surgeon gently resists by keeping slight tension on the suture braid (Fig 3E). The suture progresses through the braid until it finally emerges from the opposite end. This process is repeated with the second white braided suture. The lengths of the 2 Pullup loops are shortened to obtain 3 cm between the bone block extremity and the button plate (Fig 3F). The same steps are repeated at the tibial bone block extremity, but on this side, a Pullup XL (SBM) is used instead (Fig 4). The Pullup XL and the bone block are secured on the GraftTech table, the white braids are passed through the bone block using black loops in the same way described previously, and finally, the length of the loop is adjusted.
Fig 2.

Preparation of graft on GraftTech table. The button is locked on the fixed end of the GraftTech device, by use of the flip threads (green and white or blue) or directly with a clamp. The bone block is secured on the mobile end of the GraftTech device; it is inserted between the 2 hooks to facilitate the insertion of the Pullup braids. We can see the temporary black loop emerging from the braid, well exposed with this setting. A Polysorb No. 1 suture (reference 1CL-936 GS 12; Syneture) is used as a suture relay to insert the braid through the bone block.
Fig 3.

Different steps of graft-Pullup setting. (A) The Pullup device is placed on the fixed end of the GraftTech device as described in Figure 2, and the bone plug is inserted in the movable end. (B) A needle suture loop is inserted through the bone block in the 1.5-mm bone hole. (C) The white Pullup braid is passed into the suture loop and pulled through the bone block. (D) The white Pullup braid is passed through the opposite black loop. (E) The scrub nurse pulls the black loop, while the surgeon gently tightens the opposite white braid. (F) The Pullup braid is inserted within the opposite braid, and the Pullup loop thus formed can be reduced to the appropriate length. This process is repeated with the second loop. BTB, bone–patellar tendon–bone.
Fig 4.

Final aspect of graft with femoral bone block on left. The plug is harvested from the patella. The bone block is cone shaped to facilitate its introduction into the femoral tunnel. For this reason, the distal hole is placed more proximally to avoid bone block breakage. The end is equipped with the standard Pullup device. The tibial bone block on the right is equipped with the Pullup XL device. It should be a half millimeter wider than the femoral bone block to allow for a better introduction of the graft. BTB, bone–patellar tendon–bone.
Once the complete system is assembled, the entire construct (graft plus attached Pullup and Pullup XL BTB devices) is placed on the GraftTech device for manual pre-tensioning. The surgical process continues with arthroscopic exploration and tunnel drilling. A complete tibial tunnel is drilled to match the diameter of the tibial bone block and is placed in the anteromedial native ACL fibers. An inside-out socket is drilled on the femoral side at an adapted length ranging between 25 and 35 mm depending on the length of the patellar tendon. Next, the graft is pulled from the tibia to the femur until it is lodged at the bottom of the femoral socket. To achieve this, the surgeon has to pull on the blue thread of the Pullup device, having in his or her hand the green thread too but with gentle tension. The Pullup button plate is flipped out of the femoral tunnel by pulling on the green flip thread to make sure that the button plate is outside of the femoral cortex. The length of the Pullup loop is reduced by alternately pulling on the white braided sutures to lock the graft into place in the femoral tunnel. The tibial Pullup XL device is then pulled and the knee is cycled to completely apply the femoral button plate against the femoral cortex. Then, the knee is flexed to 20°, and a black plastic plug is inserted in the tunnel external aperture (Fig 5) to guide the Pullup XL button plate perpendicular to the top of the tibial tunnel and to avoid having the button plate go into the tibial aperture. The tibial Pullup XL device is tightened to secure and lock the graft into place (Table 1).
Fig 5.

Black plastic plug inserted in tunnel external aperture. To guide the Pullup XL button plate, a plastic cone-shaped plug is inserted in the tibial tunnel just before tightening the Pullup XL braid. In this situation, the plate is perfectly positioned at the upper part of the external aperture. This avoids flipping of the button plate inside the tibial tunnel.
Table 1.
Surgical Steps, Pitfalls, and Pearls
| Surgical Steps | Pitfalls | Pearls |
|---|---|---|
| Characteristics of patient | When the tourniquet is placed on the middle of the thigh, it limits knee flexion in the case of a patient with a large thigh; this may present an issue in correctly placing the femoral tunnel. | The tourniquet must be placed as proximally as possible on the thigh. This will avoid the knee flexion limitation and facilitate the inside–out femoral tunnel drilling. |
| Long patellar tendon | When the patellar tendon is too long, especially with a tendon length up to 5 cm, as the femoral bone plug extends out of the femoral socket, the tibial bone plug extends out of the tibial tunnel. In this case, it is impossible to tighten the tibial Pullup device because the plate is not leaning on the tibial cortex. | In such a case, there are 2 possibilities:
|
| Bone plug too short | When the bone plug length is too short (<1.5 cm), there is a risk of plug breakage when tensioning the Pullup device because the 2 holes are very close, weakening the plug. The bone plug could be split into 2. | The ideal bone plug length for such a technique is between 1.5 and 2 cm. It is recommended to save a minimum bone bridge of 1 cm between the 2 holes. For this reason, the proximal hole must be at the limit of the tendon and the bone. |
| Femoral bone plug introduction | In the classic bone–patellar tendon–bone graft technique, the end of the bone plug is square. In the procedure described in this article, it may be difficult to insert the plug inside the femoral tunnel. | A cone-shaped bony extremity can be very helpful. The plug should be oriented using a probe or clamp during pulling on the femoral Pullup device. |
| Graft fixation and knee flexion angle | When the 2 Pullup devices are tightened in flexion close to 90°, there is a risk of over-tensioning the graft, leading either to bone plug breakage or to a lack of extension. | The recommended process is to tighten the graft close to extension, cycle the knee, and then retighten the graft. |
Discussion
The use of adjustable suspensory fixation for BTB graft fixation represents an alternative to interference screw fixation, which remains the gold standard for this type of graft. This option should be helpful especially when there is difficulty in preserving enough bone stock in the femoral tunnel or when there is a risk of posterior wall blowout, which consequently weakens the graft fixation. In revision cases with tunnel enlargement, graft fixation using an interference screw can be difficult and cortical fixation with this system can be a solution. If the tunnel enlargement is very important, a 2-step procedure should be planned to first fill the tunnel with bone. When using the all-inside technique with an interference screw for femoral graft fixation, it is sometimes difficult to correctly drive the screw in the right position, and during this step, the screw can damage the patellar tendon, which rolls up around the screw; another advantage of the Pullup fixation is that it allows one to preserve the bone block and the patellar tendon. However, the Pullup BTB technique is more technically demanding than interference screw fixation, and it is important to first understand its limitations and risks, as well as some tips and tricks:
-
•
If the graft is too long, the tibial bone block will emerge from the tibial tunnel. In this case, two options are available: Either the tibial bone block is secured using an interference screw, or a staple is placed at the distal tibial site bridging the Pullup suture, after which the Pullup XL device is tightened (Fig 6). In this latter case, the staple must not be equipped with teeth because this could damage the Pullup braided suture.
-
•
In our technique, 2 separate holes are drilled through the bone block on either side of the graft. So, it is necessary to have sufficiently long bone blocks because if the 2 holes are too close, there is a risk of fracture. However, this also offers two advantages: First, reducing the diameter of the hole to 1.5 mm decreases the risk of bone fracture; second, to better secure the link between the bone block and the fixation, 2 different passages through the bone block provide 2 chances of fixation in case 1 should fail.
-
•
With small knees, it is important to pay attention to the length of the 2 loops on the femoral side and reduce the distance between the Pullup button plate and the bone block to 2 cm to avoid the risk of button-plate migration through the iliotibial band.
-
•
If the Pullup XL device on the tibial side is tightened with a flip in the tunnel, the loop can no longer be extended; this is why it is important to put the black plastic plug in the tibial tunnel aperture, allowing good contact of the button plate on the tibial cortex. Advantages and disadvantages of the technique are listed in Table 2.
Fig 6.
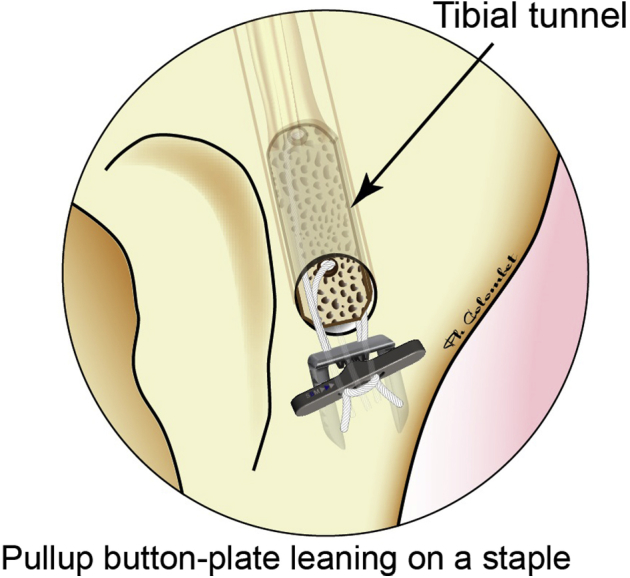
Rescue option when patellar tendon length is up to 5 cm. In this situation, there is a risk of not being able to tighten the Pullup XL device, even though the Pullup loops are reduced to a minimum. The Pullup XL device should be tightened on a 6-mm-wide staple inserted in the tibial epiphysis, 1.5 cm away from the tibial tunnel external aperture. It should be helpful to drill the longest femoral tunnel as is acceptable to increase the length of the graft inside the femoral tunnel.
Table 2.
Advantages and Disadvantages
| Advantages |
| Cortical fixation with resistance to pull |
| Preservation of bone blocks |
| Decreased risk of blowout for femoral fixation |
| No damage to tendon during fixation |
| No risk of discomfort due to fixation device |
| Disadvantages |
| Risk of fracture of graft as 2 holes are necessary in each bone block |
| Technically demanding |
| Risk of having graft that is too long if patellar tendon is long |
| Risk of migration of femoral button plate through iliotibial band |
| Inability to extend loop of device when it is tightened on bone |
Regarding knee flexion, for graft fixation, it is recommended to fix the graft with the knee flexed to 20° because the Pullup suspensory fixation is a rigid fixation and does not allow for any slippage; in addition, in the case of isometric tunnel positioning, eccentric placement could lead to bone block fracture. The Pullup BTB suspensory fixation is adjustable, a feature that gives this graft fixation the very useful option of retightening the graft if needed. After cycling the graft from extension to full flexion several times, the graft should be tightened again on the femoral and/or tibial end. No other graft fixation offers this possibility.
Adjustable suspensory fixation represents a useful additional option for BTB grafts. It is particularly indicated in the case of an inside-out femoral tunnel approach or in ACL revision surgery. However, the patellar tendon graft is not very flexible, especially when considering its length. A rigorous technique is mandatory to prevent pitfalls and difficulties. The graft must be fixed with the knee flexed to 20° to avoid bone block fracture or knee extension deficit.
Footnotes
The authors report the following potential conflict of interest or source of funding: P.C. receives support from Amplitude Surgical. SBM. Royalties for being designer of the Pullup system.
Supplementary Data
Surgical technique presenting all the technical details (in a left knee), especially how to set the Pullup braids through the 2 bone blocks. The use of the GraftTech table as a support for the Pullup device and the bone block is very helpful. One should note that using a Polysorb No. 1 suture as a suture relay is very tricky. The needle is grabbed at its tip end with the needle holder and passed through the bone block to form a loop through which the Pullup braid is introduced. For the second hole, it is sometimes difficult to find the bone hole through the tendon fibers, so an intermediary loop is used. The Pullup braid is then inserted through the temporary black loop. Two persons are required to proceed with braid passage because slight countertraction is mandatory to facilitate braid insertion.
References
- 1.Jones K.G. Reconstruction of the anterior cruciate ligament. A technique using the central one-third of the patellar ligament. J Bone Joint Surg Am. 1963;45:925–932. [PubMed] [Google Scholar]
- 2.Trojani C., Sbihi A., Djian P. Causes for failure of ACL reconstruction and influence of meniscectomies after revision. Knee Surg Sports Traumatol Arthrosc. 2011;19:196–201. doi: 10.1007/s00167-010-1201-6. [DOI] [PubMed] [Google Scholar]
- 3.Kurosaka M., Yoshiya S., Andrish J.T. A biomechanical comparison of different surgical techniques of graft fixation in anterior cruciate ligament reconstruction. Am J Sports Med. 1987;15:225–229. doi: 10.1177/036354658701500306. [DOI] [PubMed] [Google Scholar]
- 4.Colombet P., Graveleau N., Jambou S. Incorporation of hamstring graft within the tibial tunnel after anterior cruciate ligament reconstruction: magnetic resonance imaging of suspensory fixation versus interference screws. Am J Sports Med. 2016;44:2838–2845. doi: 10.1177/0363546516656181. [DOI] [PubMed] [Google Scholar]
- 5.Smith P.A., Stannard J.P., Pfeiffer F.M., Kuroki K., Bozynski C.C., Cook J.L. Suspensory versus interference screw fixation for arthroscopic anterior cruciate ligament reconstruction in a translational large-animal model. Arthroscopy. 2016;32:1086–1097. doi: 10.1016/j.arthro.2015.11.026. [DOI] [PubMed] [Google Scholar]
- 6.Robin B.N., Jani S.S., Marvil S.C., Reid J.B., Schillhammer C.K., Lubowitz J.H. Advantages and disadvantages of transtibial, anteromedial portal, and outside-in femoral tunnel drilling in single-bundle anterior cruciate ligament reconstruction: A systematic review. Arthroscopy. 2015;31:1412–1417. doi: 10.1016/j.arthro.2015.01.018. [DOI] [PubMed] [Google Scholar]
- 7.Miyatake S., Kondo E., Tohyama H., Kitamura N., Yasuda K. Biomechanical evaluation of a novel application of a fixation device for bone-tendon-bone graft (EndoButton CL BTB) to soft-tissue grafts in anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2010;26:1226–1232. doi: 10.1016/j.arthro.2010.01.007. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Surgical technique presenting all the technical details (in a left knee), especially how to set the Pullup braids through the 2 bone blocks. The use of the GraftTech table as a support for the Pullup device and the bone block is very helpful. One should note that using a Polysorb No. 1 suture as a suture relay is very tricky. The needle is grabbed at its tip end with the needle holder and passed through the bone block to form a loop through which the Pullup braid is introduced. For the second hole, it is sometimes difficult to find the bone hole through the tendon fibers, so an intermediary loop is used. The Pullup braid is then inserted through the temporary black loop. Two persons are required to proceed with braid passage because slight countertraction is mandatory to facilitate braid insertion.