

Abstract
Background:
Sport specialization and movement asymmetry have been separately discussed as potential risk factors for lower extremity injury. Early specialization may lead to the development of movement asymmetries that can predispose an athlete to injury, but this has not been thoroughly examined.
Hypothesis:
Athletes rated as specialized would exhibit greater between-limb anterior reach asymmetry and decreased anterior reach distance on the Y-balance test (YBT) as compared with nonspecialized high school athletes, and these differences would not be dependent on sex.
Study Design:
Cross-sectional study.
Level of Evidence:
Level 3.
Methods:
Two hundred ninety-five athletes (117 male, 178 female; mean age, 15.6 ± 1.2 years) from 2 local high schools participating in basketball, soccer, volleyball, and tennis responded to a questionnaire regarding sport specialization status and performed trials of the YBT during preseason testing. Specialization was categorized according to 3 previously utilized specialization classification methods (single/multisport, 3-point scale, and 6-point scale), and interactions between specialization and sex with Y-balance performance were calculated using 2-way analyses of variance.
Results:
Single-sport male athletes displayed greater anterior reach asymmetry than other interaction groups. A consistent main effect was observed for sex, with men displaying greater anterior asymmetry and decreased anterior reach distance than women. However, the interaction effects of specialization and sex on anterior Y-balance performance varied based on the classification method used.
Conclusion:
Single-sport male athletes displayed greater anterior reach asymmetry on the YBT than multisport and female athletes. Specialization classification method is important because the 6- and 3-point scales may not accurately identify balance abnormalities. Male athletes performed worse than female athletes on both of the Y-balance tasks.
Clinical Relevance:
Clinicians should be aware that single-sport male athletes may display deficits in dynamic balance, potentially increasing their risk of injury.
Keywords: specialization, Y-balance, movement screen, youth sports, high school
Nearly 29 million school-aged youth are members of at least 1 organized youth sports team.21 With the explosive growth in youth sports participation, there is increasing concern about the risk of injury in youth sports. Certain sports, such as basketball, soccer, and volleyball, place participants at increased risk of lower extremity injury.26,27,30 Additionally, youth female athletes appear to be at increased risk of certain lower extremity injuries, such as anterior cruciate ligament tears and overuse knee injuries.1,3,12,30 One potential mechanism for the differences seen in injury risk between sports and sex may be the increasing trend toward sport specialization at an early age.15 Sport specialization is commonly defined as “year-round intensive training in a single sport at the exclusion of other sports” and can lead to burnout and put athletes at a greater risk for injury.2,14,20 Additionally, by specializing early, young athletes may miss out on some of the benefits provided by sports diversification, such as the positive transfer of skills and development of a variety of motor skills.20
Approximately 1 in 5 injuries in persons aged 5 to 24 years are related to sports or physical activity. 5 Jayanthi et al14 found that specialization posed an independent risk for both injury and serious overuse injury, with athletes who presented with a serious overuse injury having 1.90 times greater odds of being classified as highly specialized. Furthermore, this study found the risk for injury, overuse injury, and serious overuse injury to have a dose-dependent relationship with specialization level.14 One potential mechanism for the association between specialization and injury is the high volume of repetition and lack of variety in movement patterns.21 Theoretically, these patterns can result in muscle imbalance and alter tissue stress, which results in poor performance or injury (Figure 1).21 Significant research has been performed examining the connection between dynamic balance performance and injury risk.4,7,9,24,28 Poor performance on the Star Excursion Balance Test (SEBT), which measures single-limb reach distance in 8 different directions, is associated with an increased risk of a variety of lower extremity injuries.4,9,24 The Y-balance test (YBT) is a reliable and valid test that was developed as a 3-direction modification of the SEBT to eliminate SEBT redundancies and improve testing efficiency (Figure 2).23 The YBT assesses dynamic stability and balance, requiring a range of skills including neuromuscular control, flexibility, and strength.10,23,24 Poor performance on certain aspects of the YBT, such as movement in the anterior direction (total reach direction and asymmetry), has the most consistent relationship with increased injury risk.7,28 While the relationship between performance on the YBT and injury has been studied, the relationship between the YBT and other aspects of sport has also recently become a topic of interest.
Figure 1.

Theoretical model of the potential mechanisms through which sport specialization may increase the risk of injury.
Figure 2.
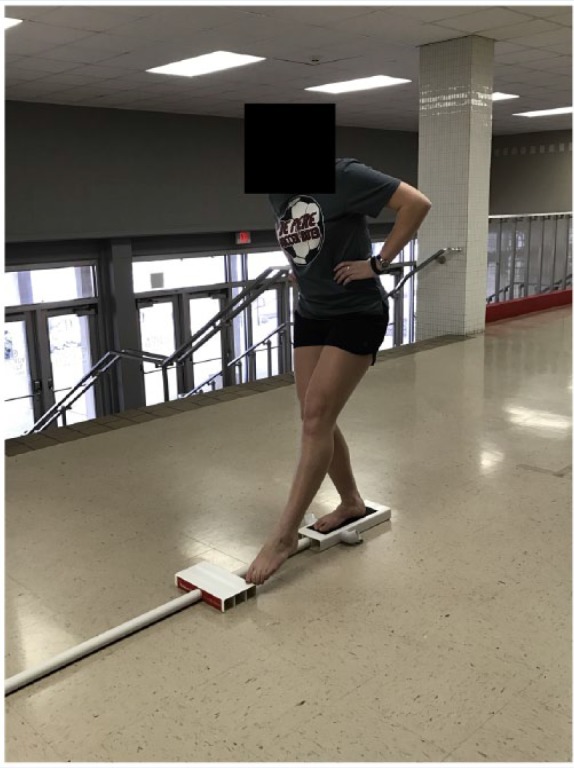
Example of Y-balance test anterior reach performance.
The YBT has recently been investigated with respect to sport specialization and sex. Gorman et al8 observed no differences between single- and multisport high school athletes in reach distance or asymmetry on the YBT. However, specialization is more accurately classified along a continuum as opposed to classifying based on the number of sports played.15 With this in mind, a sport specialization scale has been developed, originally as a 6-point scale and then later as a 3-point scale.14,16 These scales were developed in a sample of youth athletes reporting to a sports medicine clinic for either an injury or a physical.14,16 The scales are based on a previously established and accepted definition of sport specialization and attempt to classify the degree of specialization of an athlete based on their responses to a variety of questions that aim to gauge how closely participants match that definition of specialization.14 However, there is no consensus on the best measure of specialization, and all 3 measures (number of sports played, 6-point scale, 3-point scale) have been utilized in previous studies.12,14,16 Bell et al2 observed that the prevalence of specialization and association of specialization with injury history differed depending on the classification method utilized. This finding indicated that the various methods of measuring specialization may differ in their ability to assess various outcome measures related to sport specialization.2
A literature review performed by Gribble et al9 concluded that with proper normalization, there were no sex-based differences in performance on the SEBT in healthy, nonfatigued populations. However, Gorman et al8 observed that male high school athletes displayed significantly greater anterior reach asymmetry compared with female athletes on the YBT. There also appear to be sex differences in the prevalence of specialization among youth athletes, but these differences may be driven by the method of classification used.2 No differences were found in the prevalence of specialization between sexes when using the 3-point scale to classify specialization.2 However, when classifying specialization using the number of sports played, women were more likely than men to be single-sport athletes.2 Therefore, further analysis of the effects of sex on YBT reach and specialization is warranted.
The purpose of this study was to examine the effect of specialization and sex on performance on the anterior reach portion of the YBT in high school athletes. We hypothesized that athletes rated as specialized (using either the 6-point scale, 3-point scale, or single-/multisport classification) would exhibit greater between-limb anterior reach asymmetry and decreased anterior reach distance on the YBT as compared with nonspecialized high school athletes and that these differences would not be dependent on sex.
Methods
Participants
This study was approved by the Institutional Review Board of the University of Wisconsin–Madison, and informed written assent/consent was obtained from the participant and parent or guardian prior to participation. Participants were recruited in person from 2 local high schools during preseason parent/athlete team meetings and tested at their respective schools prior to the start of their athletic competition season. School administrators, involved coaches, and athletic trainers from both schools all agreed to participate. Subjects were recruited from 4 different sports: soccer, basketball, tennis, and volleyball (women only). These sports were chosen due to their elevated risk of sustaining a lower extremity injury.2 It was required that study participants were between 13 and 18 years of age; a current participant on freshman, junior varsity, or varsity level athletics at 1 of the included schools; and not suffering from a lower extremity injury at the time of testing. Participants who had suffered a previous lower extremity injury were included if they were fully recovered from their injury and participating in sport at the time of testing. A total of 295 healthy athletes (178 females, 117 males; mean age, 15.6 ± 1.2 years; mean height, 171.4 ± 9.3 cm; mean weight, 65.7 ± 11.3 kg) completed the full testing, including YBT, during the 2014-2015 academic year. Two participants with incomplete information were excluded from the study. Testing was performed in a rotating, station-based testing format, during which each subject also individually completed a written questionnaire.
Questionnaire
Participants completed a sport specialization and injury history questionnaire that has been detailed previously.2 In short, sport specialization was assessed using 3 separate measures. The first method entailed asking athletes whether they classified themselves as a single- or multisport athlete. The other 2 classification methods were determined using the responses to a 6-question sports specialization set developed by Jayanthi et al16 to assess and categorize early sports specialization. The questions that comprised these scales are presented in Table 1. Using the 6-point scale, sports specialization was dichotomized using all 6 of these questions (yes to 4 or more questions = specialized, yes to 3 or fewer questions = nonspecialized).16 Finally, sport specialization was classified using the 3-point scale based on the participant’s responses to the final 3 questions (quit other sports, primary sport more important, train more than 8 months). A categorical classification system was used (yes = 1, no = 0), with a score of 3 considered high specialization, 2 considered moderate specialization, and 0 or 1 considered low specialization.2,14 Responses were reviewed with each subject by a certified athletic trainer to ensure completeness of data.
Table 1.
Six-point and 3-point specialization scale questionnaire a
| 1. Do you train more than 75% of the time in your primary sport? | Yes / No |
| 2. Do you train to improve skill and miss time with friends as a result? | Yes / No |
| 3. Do you regularly travel out of state for your primary sport? | Yes / No |
| 4. Have you quit other sports to focus on 1 sport? | Yes / No |
| 5. Do you consider your primary sport more important than other sports? | Yes / No |
| 6. Do you train or participate in your primary sport more than 8 months out of the year? | Yes / No |
Responses to all questions were used to determine 6-point scale score. Responses to questions 4, 5, and 6 were used to determine 3-point scale score.
Y-Balance
The YBT was used to assess dynamic balance. The apparatus involves a centralized platform connected to 3 cylindrical plastic bars. Each plastic bar is attached to a sliding measurement box to be pushed by the subject’s foot. Subjects performed the YBT during a station-based testing session. Subjects were instructed to remove shoes to perform the test while either wearing socks or barefoot and stand on 1 leg (evaluated limb) on the centralized platform, with toes just behind a red indicator line. Subjects were instructed to place their hands on hips and push the measurement box with the nonstance leg as far as possible in the anterior direction. Four practice trials were allowed, followed by 3 recorded trials.7 Trials were repeated if the subjects committed an error during the trial, which included lifting the heel or toe, shifting weight onto the indicator box, loss of balance resulting in falling or stepping off the apparatus, or kicking the sliding measurement box. Maximum distance achieved in the anterior direction was recorded for all 3 trials, and the average of the 3 trials for each limb was used for analysis.7 This procedure was then repeated with the subject standing on the opposite leg. Each participant’s dominant leg was determined prior to testing by asking which leg the participants would choose to kick a soccer ball for maximal distance, and participants were allowed to select which leg would be tested first. Prior to the YBT, leg length of each participant was measured from anterior superior iliac spine to medial malleolus using a tape measure and recorded in centimeters. Research assistants underwent a standardized training program to properly instruct subjects in using the YBT, determine errors, and assess maximum distances. Research assistants were required to demonstrate intra- and interrater reliability values greater than 0.85 before participating in data collection. Anterior reach distance was normalized to limb length (%LL).
Statistical Analysis
Anterior reach asymmetry was calculated as the absolute value of the difference between the mean dominant and nondominant limb reach distances. Separate 2-way analyses of variance were used to investigate between-group effects (sex [male vs female] and specialization category). History of lower extremity injury was utilized as a covariate in each analysis to control for the influence of previous lower extremity injury on dynamic balance. Post hoc Tukey honestly significant difference (HSD) tests were used when appropriate. All analyses were performed using SPSS statistical software (IBM Corp), with an a priori P value set to <0.05.
Results
Data from 178 (60.3%) women and 117 (39.7%) men were included in our sample, with data from 1 subject not used due to an incomplete specialization questionnaire. Specialization prevalence varied based on the classification method used, with 28.4% (n = 84) of athletes classified as single-sport athletes, 36.2% (n = 107) considered highly specialized using the 3-point scale, and 54.9% (n = 162) classified as specialized using the 6-point scale.
With regard to the single-/multisport classification, we observed a significant interaction between specialization and sex (Table 2). Post hoc testing using Tukey HSD tests revealed that single-sport male athletes displayed significantly greater anterior reach asymmetry compared with all other groups (P < 0.05), with no significant differences between any of the other groups. No significant interaction was observed between sex and sport specialization classification using the 6-point scale (P = 0.06) or the 3-point scale (P = 0.67) for anterior reach asymmetry. Additionally, no interactions were observed between specialization classification methods and sex for anterior reach distance (P > 0.05) (Table 3).
Table 2.
Anterior reach asymmetry interaction effects a
| Anterior Reach Asymmetry (cm) | P Value | |
|---|---|---|
| Single-/Multi-interaction | 0.015 | |
| Multisport male athletes | 3.10 ± 0.26 | |
| Single-sport male athletes | 4.63 ± 0.50 | |
| Multisport female athletes | 2.91 ± 0.23 | |
| Single-sport female athletes | 2.75 ± 0.32 | |
| 3-point scale interaction | 0.670 | |
| Low male athletes | 2.89 ± 0.39 | |
| Moderate male athletes | 4.30 ± 0.44 | |
| High male athletes | 3.28 ± 0.38 | |
| Low female athletes | 2.40 ± 0.32 | |
| Moderate female athletes | 3.30 ± 0.34 | |
| High female athletes | 2.93 ± 0.31 | |
| 6-point scale interaction | 0.056 | |
| Nonspecialized male athletes | 2.69 ± 0.32 | |
| Specialized male athletes | 4.17 ± 0.33 | |
| Nonspecialized female athletes | 2.65 ± 0.29 | |
| Specialized female athletes | 3.00 ± 0.24 |
Boldfaced value indicates statistical significance (P < 0.05). Previous lower extremity injury utilized as a covariate.
Table 3.
Anterior reach distance interaction effects a
| Anterior Reach Distance (% Limb Length) | P Value | |
|---|---|---|
| Single-/Multi-interaction | 0.412 | |
| Multisport male athletes | 62.3 ± 0.7 | |
| Single-sport male athletes | 63.6 ± 1.3 | |
| Multisport female athletes | 67.2 ± 0.6 | |
| Single-sport female athletes | 67.0 ± 0.8 | |
| 3-point scale interaction | 0.812 | |
| Low male athletes | 61.5 ± 1.0 | |
| Moderate male athletes | 62.3 ± 1.1 | |
| High male athletes | 63.8 ± 1.0 | |
| Low female athletes | 66.7 ± 0.8 | |
| Moderate female athletes | 66.3 ± 0.9 | |
| High female athletes | 68.1 ± 0.8 | |
| 6-point scale interaction | 0.537 | |
| Nonspecialized male athletes | 61.8 ± 0.8 | |
| Specialized male athletes | 63.4 ± 0.8 | |
| Nonspecialized female athletes | 66.8 ± 0.7 | |
| Specialized female athletes | 67.4 ± 0.6 |
Previous lower extremity injury utilized as a covariate.
A consistent main effect was observed for sex and anterior reach asymmetry, with men displaying more anterior asymmetry than women across all 3 specialization classification methods (single-/multisport: men, 3.86 ± 0.28 cm vs women, 2.83 ± 0.20 cm [P = 0.003]; 3-point scale: men, 3.49 ± 0.23 cm vs women, 2.88 ± 0.19 cm [P = 0.040]; 6-point scale: men, 3.43 ± 0.23 cm vs women, 2.83 ± 0.19 cm [P = 0.044]). Similarly, a consistent main effect was observed for sex and anterior reach distance, with women exhibiting increased anterior reach distance compared with men across all 3 specialization methods (men, 62.6% ± 0.6% LL; women, 67.1 ± 0.5% LL; P < 0.001).
The main effect for specialization on anterior YBT performance varied based on the specialization scale used. Athletes categorized as specialized using the 6-point scale displayed greater anterior reach asymmetry compared with nonspecialized athletes (specialized, 3.59 ± 0.20 cm; nonspecialized, 2.67 ± 0.22 cm; P = 0.002). However, moderately specialized athletes exhibited greater anterior reach asymmetry compared with low or highly specialized athletes (low specialization, 2.64 ± 0.25 cm; moderate specialization, 3.80 ± 0.28 cm; high specialization, 3.11 ± 0.25 cm; P = 0.009) when the 3-point scale was utilized. No difference was observed in anterior reach distance using any of the 3 specialization classification methods (P > 0.05).
Discussion
The most important finding of this study was that single-sport male athletes displayed greater anterior asymmetry than other groups. Additionally, our findings differed based on the method of classification of specialization. We were only able to identify differences with the single-/multisport classification method and were unable to detect any differences using the 6- and 3-point scales. It is possible that these methods may not be able to detect sex by specialization differences. However, the 6-point scale was able to detect differences between specialized and nonspecialized athletes. Finally, male athletes had greater asymmetry and smaller normalized reach distances than female athletes.
The overall trend in youth sports toward early specialization is driven by many factors, including competition for collegiate scholarships, the desire to achieve elite or professional status, pressure from parents who want to give their children a competitive advantage, and influence of businesses and advertising.18 While certain people and institutions may value specialization, current research demonstrates that specialization is associated with adverse outcomes such as psychological burnout and injury.2,12,14,18 One of the mechanisms through which specialization may increase the risk of injury is by hindering proper motor skill development in youth athletes when those athletes only focus on the movement skills necessary for their sport.21
However, there is disagreement regarding the most accurate method for classifying specialization.15 Using the single-/multisport classification method, Hall et al12 observed that single-sport adolescent female athletes had a 1.5 times greater incidence of patellofemoral pain. Following the idea that specialization occurs along a spectrum and that the single-/multisport classification is too simple to detect this spectrum, 2 sport specialization scales were developed. The original scale was a 6-point scale,16 which was later condensed into a 3-point scale,14 and specialization classified using either of these scales has been associated with injury.2,14,16 Jayanthi et al14 found that sports specialization was associated with increased risk for injury, independent of training volume and age. The participants in that study who were categorized as highly specialized were 2.25 times more likely than their unspecialized counterparts to present with an overuse injury. Finally, Bell et al2 observed that high school athletes who competed in their sport year-round were more likely to report a previous history of hip and overuse knee injuries. Therefore, it is important for researchers in this area to consider all current methods of classifying specialization until an optimal measure can be determined.
Balance and neuromuscular control of the lower extremity have been proposed by researchers as potential factors related to injury risk.17,19 One standard of “poor performance” on the YBT is an asymmetry in anterior reach distance between limbs.28 Athletes across various sports with significant reach asymmetries on the YBT and SEBT are more likely to sustain noncontact injuries.4,28 For example, professional and amateur athletes who demonstrated a between-limb reach deficit were more likely to sustain lower body soft tissue injuries.7 Anterior reach distance asymmetries greater than 4 cm are associated with a 2.3- to 2.5-times greater risk of lower extremity injury.24,28 In our study, the single-sport male athletes had a mean anterior reach asymmetry of 4.63 cm, which is greater than this threshold. This may indicate that the single-sport male athletes in our study are at an increased risk of sustaining a lower extremity injury. Stiffler et al29 found that mean normalized anterior reach distances in a sample of college athletes ranged between 62% and 69%,29 similar to the values found in this study. They also found that female soccer players exhibited increased anterior reach distance compared with male soccer athletes,29 which matches the findings in this study of increased anterior reach distance among female athletes.
Impairments in dynamic balance due to the repetition of a small profile of movement patterns may be 1 potential mechanism for the increased risk of lower extremity injury seen in highly specialized athletes.14,21,25 No significant differences were found in reach asymmetry between athletes who played a single sport compared with those who reported playing multiple sports in a sample of 92 high school athletes.8 While this differed from the results of our study, the use of multiple methods of classifying specialization and a much larger sample may have better detected differences in YBT performance. Additionally, specialization scales may allow for more accurate classification of specialized and nonspecialized athletes beyond just the number of sports in which an athlete participates. It is possible to imagine a single-sport athlete who plays their sport casually to socialize with friends and an athlete who plays multiple sports but focuses in 1 of those sports year-round.20
A main effect for specialization was observed when utilizing the 6-point specialization scale, with specialized athletes displaying increased anterior asymmetry compared with female athletes. Interestingly, when using the 3-point specialization scale, moderately specialized athletes demonstrated the greatest anterior asymmetry. While high specialization classified on the 3-point scale appears to be linked with injury,2,14 it is possible that this scale is not able to discriminate changes in movement patterns on the YBT as effectively as the 6-point scale. Ideally, clinicians could utilize the 6-point scale to identify specialized athletes who may be at risk of impaired movement patterns and then use the YBT to assess progress after providing an intervention aimed at improving neuromuscular control.
Contrary to our hypothesis, we observed a consistent main effect for sex, with men displaying increased anterior reach asymmetry and decreased anterior reach distance compared with women. Similarly, female athletes have demonstrated increased reach distances in 3 separate directions on the SEBT, and these differences were magnified after a fatigue protocol.11 In single- and multisport athletes, male athletes exhibited significantly greater anterior reach asymmetry on the YBT, similar to the findings of this study.8 These findings would suggest that male athletes would be at increased risk of injury in the sports we examined. However, female athletes have an increased risk of knee injury in sex-equivalent sports such as soccer, volleyball, and basketball.30 Additionally, previous research has indicated that specific biomechanical strategies such as increased hip adduction and decreased knee and hip flexion are associated with decreased anterior reach distance and knee injury.6,13,22 The strategies that led to men having shorter reach distances and greater asymmetry than women are unknown; however, it is possible that they differ from the movement patterns and strategies that contribute to increased rates of knee injury in female athletes. It is important to consider the sex of the athlete when utilizing the YBT as part of a preseason physical examination or as a movement assessment.
There are several limitations to this study. Subjects included high school athletes from 4 sports: basketball, soccer, volleyball, and tennis. Thus, the conclusions may not be generalizable beyond this population of athletes, especially since dynamic performance differs based on sport.29 Additionally, sport specialization may be more accurately defined by prospectively following a cohort of youth athletes to track their sport participation patterns. This was not done due to the cross-sectional design of this study. We were also unable to determine prospective injury risk in this sample because we did not follow athletes into their sport seasons and only tested them at baseline. Finally, previous lower extremity injury was assessed using self-report, which presents an opportunity for subject recall bias. However, this limitation was well-controlled for by having each questionnaire thoroughly reviewed with the subject by an athletic trainer to ensure proper classification and recall of injuries.
Conclusion
Specialized athletes displayed greater anterior reach asymmetry on the YBT than nonspecialized athletes across multiple methods of classifying specialization. Anterior reach asymmetry was significantly greater in specialized male athletes, which may be an especially at-risk population. Women performed better than men on both aspects of the YBT, exhibiting increased reach distance and decreased reach asymmetry.
Footnotes
The following author declared potential conflicts of interest: M. Alison Brooks, MD, MPH, is a paid consultant for the NBA.
References
- 1. Arendt E, Agel J, Dick R. Anterior cruciate ligament injury patterns among collegiate men and women. J Athl Train. 1999;34:86-92. [PMC free article] [PubMed] [Google Scholar]
- 2. Bell DR, Post EG, Trigsted SM, Hetzel S, McGuine TA, Brooks MA. Prevalence of sport specialization in high school athletics: a 1-year observational study. Am J Sports Med. 2016;44:1469-1474. [DOI] [PubMed] [Google Scholar]
- 3. Beynnon BD, Vacek PM, Newell MK, et al. The effects of level of competition, sport, and sex on the incidence of first-time noncontact anterior cruciate ligament injury. Am J Sports Med. 2014;42:1806-1812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Butler RJ, Lehr ME, Fink ML, Kiesel KB, Plisky PJ. Dynamic balance performance and noncontact lower extremity injury in college football players: an initial study. Sports Health. 2013;5:417-422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Conn JM, Annest JL, Gilchrist J. Sports and recreation related injury episodes in the US population, 1997-99. Inj Prev. 2003;9:117-123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Delahunt E, Chawke M, Kelleher J, et al. Lower limb kinematics and dynamic postural stability in anterior cruciate ligament-reconstructed female athletes. J Athl Train. 2013;48:172-185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Gonell AC, Romero JAP, Soler LM. Relationship between the Y balance test scores and soft tissue injury incidence in a soccer team. Int J Sports Phys Ther. 2015;10:955-966. [PMC free article] [PubMed] [Google Scholar]
- 8. Gorman PP, Butler RJ, Rauh MJ, Kiesel K, Plisky PJ. Differences in dynamic balance scores in one sport versus multiple sport high school athletes. Int J Sports Phys Ther. 2012;7:148-153. [PMC free article] [PubMed] [Google Scholar]
- 9. Gribble P, Hertel J, Plisky P. Using the Star Excursion Balance Test to assess dynamic postural-control deficits and outcomes in lower extremity injury: a literature and systematic review. J Athl Train. 2012;47:339-357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Gribble PA, Kelly SE, Refshauge KM, Hiller CE. Interrater reliability of the Star Excursion Balance Test. J Athl Train. 2013;48:621-626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Gribble PA, Robinson RH, Hertel J, Denegar CR. The effects of gender and fatigue on dynamic postural control. J Sport Rehabil. 2009;18:240-257. [DOI] [PubMed] [Google Scholar]
- 12. Hall R, Barber Foss K, Hewett TE, Myer GD. Sport specialization’s association with an increased risk of developing anterior knee pain in adolescent female athletes. J Sport Rehabil. 2015;24:31-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33:492-501. [DOI] [PubMed] [Google Scholar]
- 14. Jayanthi NA, LaBella CR, Fischer D, Pasulka J, Dugas LR. Sports-specialized intensive training and the risk of injury in young athletes: a clinical case-control study. Am J Sports Med. 2015;43:794-801. [DOI] [PubMed] [Google Scholar]
- 15. Jayanthi NA, Pinkham C, Dugas L, Patrick B, LaBella C. Sports specialization in young athletes: evidence-based recommendations. Sports Health. 2013;5:251-257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Jayanthi NA, Pinkham C, Luke A. The risks of sports specialization and rapid growth in young athletes. Clin J Sport Med. 2011;21:153-184. [Google Scholar]
- 17. Lephart SM, Pincivero DM, Rozzi SL. Proprioception of the ankle and knee. Sports Med. 1998;25:149-155. [DOI] [PubMed] [Google Scholar]
- 18. Malina RM. Early sport specialization: roots, effectiveness, risks. Curr Sports Med Rep. 2010;9:364-371. [DOI] [PubMed] [Google Scholar]
- 19. McGuine T, Greene JJ, Best T, Leverson G. Balance as a predictor of ankle injuries in high school basketball players. Clin J Sport Med. 2000;10:239-244. [DOI] [PubMed] [Google Scholar]
- 20. Myer GD, Jayanthi N, Difiori JP, et al. Sport specialization, part I: does early sports specialization increase negative outcomes and reduce the opportunity for success in young athletes? Sports Health. 2015;7:437-442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Myer GD, Jayanthi N, DiFiori JP, et al. Sports specialization, part II: alternative solutions to early sport specialization in youth athletes. Sports Health. 2016;8:65-73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Paterno MV, Schmitt LC, Ford KR, et al. Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med. 2010;38:1968-1978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Plisky PJ, Gorman PP, Butler RJ, Kiesel KB, Underwood FB, Elkins B. The reliability of an instrumented device for measuring components of the star excursion balance test. N Am J Sports Phys Ther. 2009;4:92-99. [PMC free article] [PubMed] [Google Scholar]
- 24. Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star Excursion Balance Test as a predictor of lower extremity injury in high school basketball players. J Orthop Sports Phys Ther. 2006;36:911-919. [DOI] [PubMed] [Google Scholar]
- 25. Post EG, Trigsted SM, Riekena JW, et al. The association of sport specialization and training volume with injury history in youth athletes [published online March 1, 2017]. Am J Sports Med. doi: 10.1177/0363546517690848. [DOI] [PubMed] [Google Scholar]
- 26. Roos KG, Kerr ZY, Mauntel TC, Djoko A, Dompier TP, Wickstrom EA. The epidemiology of lateral ligament complex ankle sprains in National Collegiate Athletic Association sports. Am J Sports Med. 2017;45:201-209. [DOI] [PubMed] [Google Scholar]
- 27. Roos KG, Wasserman EB, Dalton SL, et al. Epidemiology of 3825 injuries sustained in six seasons of National Collegiate Athletic Association men’s and women’s soccer (2009/2010-2014/2015) [published online May 17, 2016]. Br J Sports Med. doi: 10.1136/bjsports-2015-095718. [DOI] [PubMed] [Google Scholar]
- 28. Smith CA, Chimera NJ, Warren M. Association of Y balance test reach asymmetry and injury in Division I athletes. Med Sci Sports Exerc. 2015;47:136-141. [DOI] [PubMed] [Google Scholar]
- 29. Stiffler MR, Sanfilippo JL, Brooks MA, Heiderscheit BC. Star Excursion Balance Test performance varies by sport in healthy Division I collegiate athletes. J Orthop Sports Phys Ther. 2015;45:772-780. [DOI] [PubMed] [Google Scholar]
- 30. Swenson DM, Collins CL, Best TM, Flanigan DC, Fields SK, Comstock RD. Epidemiology of knee injuries among U.S. high school athletes, 2005/2006-2010/2011. Med Sci Sports Exerc. 2013;45:462-469. [DOI] [PMC free article] [PubMed] [Google Scholar]