

Abstract
Chronic total occlusions (CTOs) of coronary arteries represent a common and significant challenge to interventional cardiology. Medical therapy is often regarded as an adequate long term strategy in the management of these lesions with surgical intervention for refractory symptoms. Extensive collateralisation is used as a marker of distal coronary perfusion, further reinforcing non-invasive strategies. This together with relatively low percutaneous success rates outside of specialised centres has meant that rates of percutaneous intervention have remained low. Increasing evidence suggests that CTOs are not a benign entity. Further, symptom control and quality of life improve significantly with successful percutaneous revascularisation. Both factors have reignited interest in percutaneous modalities. The Japanese have been pioneers in the field of CTO intervention although their success rates have been difficult to replicate. New techniques and equipment developed in North America offer an alternative to the Japanese approach. These techniques focus on time, radiation and contrast minimisation. This review will assess the histopathology of CTO and shifting paradigms in CTO treatment strategies.
Keywords: Chronic total occlusion, Techniques, Antegrade, Retrograde, CrossBoss, Stingray balloon, Reverse CART, Knuckle wire
Highlights
-
•
Chronic total occlusions are common and prognostically important.
-
•
Strategies for chronic occlusions are pioneered by Japanese, adapted by North American operators.
-
•
Japanese and North American strategies appear divergent, both add considerable expertise.
1. Introduction
A chronic total occlusion (CTO) is usually defined as a total obstruction of a coronary artery of greater than three months duration. The duration of occlusion has implications for the histopathological characteristics and the success rates associated with intervention. It can occasionally be determined from previous angiography. However, often a combination of clinical history and angiographic features is required to support the diagnosis.
Among patients diagnosed with coronary disease on angiography, CTO’s are common, occurring in 20 to 30% of patients [1]. The presence of a CTO often influences treatment recommendations and is the strongest predictor of referral for coronary artery bypass surgery (CABG) [2]. Revascularisation remains challenging irrespective of the modality selected. For example, in the SYNTAX trial [3], percutaneous coronary intervention (PCI) of CTO lesions was successful in 49% percent of patients. The surgical success rates were only marginally better at 68%. Currently, PCI success rates of greater than 80% are being reported in specialist Japanese, American and European Centres [4]. Despite this, referral for PCI remains low in many countries and the reasons are likely multifactorial. Firstly, the historically poor success rates that characterised early interventional experience continue to affect referral behaviour. While there is a large volume of retrospective data, there is a lack of randomised data supporting the benefit of CTO revascularisation on morbidity and mortality. This review will focus on the development of new techniques for CTO PCI with an emphasis on procedurally relevant histopathology and the differing methodologies that have emerged from sites in Japan and the United States of America. A discussion of the prognostic importance of CTOs and the rationale for revascularisation is beyond the scope of this review and has been published elsewhere [5], [6], [7], [8], [9], [10], [11], [12], [13], [14], [15], [16], [17], [18], [19], [20], [21], [22], [23], [24], [25], [26], [27].
2. Histopathology of CTO lesions
CTOs consist of a proximal and a distal cap with an intervening occluded segment. In one histological study the proximal cap was more likely to be fibro-calcific than the distal cap. This has implications for the particular percutaneous approach selected and explains the rationale behind retrograde strategies. Despite complete occlusion on angiography, CTOs have vascular channels that span the occluded segment [28], [29]. These channels help to protect the vessel wall against the flow limiting effects of intimal plaque progression. There are two types of histological vascular channels within the occluded segment of the CTO: [28], [29]
-
1.
Endothelialised microchannels (160 to 230 μm) generated via neovascularisation that span the CTO from proximal to distal cap. These are termed histologically recanalised segments.
-
2.
Micro capillaries (< 100 μm) that pass into small side branches or into the vaso vasorum. The vaso vasorum is a network of vessels that arise in adventitial layers and provide nutrients to the vessel wall. These micro capillaries are termed non-recanalised segments, as they do not connect the proximal and distal caps.
Histologically recanalised segments may allow coronary wires to pass through the lumen of the CTO within endothelialised microchannels and across the occlusion. Non-recanalised segments are predisposed to subintimal wire passage. Short occlusions with a tapered stump are more likely to have histologically recanalised segments than longer occlusions. All CTOs with a non-tapered (ambiguous) entry point examined histologically had non-recanalised micro capillaries [28].
The precise composition of the intervening occluded segment is influenced by the age of the occlusion. In younger CTO lesions there is softer cholesterol laden material between the proximal and distal caps that typically consists of organised thrombus, extracellular matrix, smooth muscle cells and lipid deposits (so called loose tissue) [28], [29]. This soft material contains endothelialised microchannels. Dense fibro-calcific areas and micro capillary formation characterise older occlusions. These histopathological characteristics provide the theoretical basis for many of the CTO PCI techniques discussed later.
The CTO has traditionally been divided into “luminal” vs “subintimal spaces”. The luminal space is defined as the space containing blood when the artery was patent and is encircled by the intimal (endothelial) layer. The subintimal space refers to that space external to the intimal layer but within the vessel architecture. This includes the media (smooth muscle) and adventitial layers. The internal elastic membrane (IEM) surrounds the intimal layer and the external elastic membrane (EEM) surrounds the media and is bounded by adventitia. During CTO PCI, subintimal wire passage is within the media between the IEM and the EEM following the path of least resistance. This theoretical distinction is relevant when discussing the various percutaneous techniques.
For the myocardium to remain viable in an area subtended by a CTO there must be collateral circulation. This can occur via antegrade bridging collaterals from the culprit vessel or retrograde collaterals from a contralateral vessel. The ability of collateral vessels to provide sufficient flow to maintain coronary perfusion under rest and stress can be difficult to assess. Angiographic size may not predict the functionality of collaterals. Collateral flow distal to the CTO can further be compromised by epicardial or microvascular disease in a contralateral vessel supplying collaterals. The traditional teaching regarding the concept of “adequacy of collateralisation” in preventing ischaemia in CTOs is now challenged by physiological evidence. One study assessed 62 patients undergoing CTO PCI. Sixty-one patients had physiologically significant ischaemia across the occlusion using FFR, irrespective of the angiographic appearance of collaterals. In addition, preserved left ventricular systolic function (present in 39 patients) did not predict adequacy of collaterals [30].
2.1. Clinical and procedural considerations
Clinical indications for CTO revascularisation are the initial consideration and include the severity of symptoms, level of medical therapy, age and comorbid disease. In particular the presence of renal impairment, cognitive impairment and medication non-concordance may influence whether to proceed with PCI or CABG compared with medical therapy. If an evaluation of ischaemia is required then the preferred method depends upon local availability and expertise. Following informed consent, patient preference may alter the options considered. When it has been concluded that revascularisation with PCI is indicated, the procedure requires thorough planning. Procedural success depends upon careful review of the angiogram including stump morphology, length of occlusion, calcification and presence and extent of collaterals.
Traditional factors that predict a lower PCI procedural success rate include length of occlusion greater than (>) 20 mm, presence of calcification within the lesion and/or artery, native vessel CTO after CABG and the presence of bridging collaterals [31], [32], [33]. A tapered tip occlusion is more favourable than a blunt “cut-off”, as is the absence of side branches in close proximity to the occlusion [31], [32], [33].
The J-CTO score was developed to classify lesion complexity [32] (Fig. 1). A number of the lesion characteristics are included in the J-CTO score, which has also been proposed as a predictor of procedural success. This is a numerical score with higher values indicating greater procedure complexity (Fig. 1). Its predictive capability with regard to procedural success has been inconsistent. However, it has been shown to correlate with the duration required for successful intimal wire crossing [32]. (Fig. 2)
Fig. 1.

The J-CTO score is used to characterise lesion complexity in a standardised way. Reproduced with permission from Morino et al. [32].
Fig. 2.

The J-CTO score predicts the ability to cross the lesion antegrade in less than 30 min. This underpins the algorithm and rapid shifts in strategy advocated in the hybrid approach (see below) Reproduced with permission from Morino et al. [32].
An ‘ad hoc’ approach to PCI is widely discouraged to allow appropriate angiographic review and informed consent. Outcomes with PCI have also been linked with the following factors: [34], [35]
-
1.
Operator experience [36]
-
2.
Dual interventional cardiologist approach
-
3.
‘Quarantined’ laboratory time to prevent time constraints
-
4.
Pre procedure laboratory inventory review to ensure necessary equipment is available
-
5.
Radiographer assistance and implementation of radiation minimisation techniques [37], [38].
In selected cases CT coronary angiography may assist in pre-planning by providing additional morphological features of the CTO; in particular vessel course, tortuosity and calcification [39], [40], [41].
Initiation of the procedure requires meticulous attention to arterial access. Bilateral femoral artery access is often performed due to the requirement for dual injection and larger guide catheters. At least 7F-guiding catheters are suggested for CTO intervention. Anchor balloon techniques require a 7F system. Techniques that require the use of a microcatheter simultaneously with IVUS, or the CrossBoss dissection system (Boston Scientific, Marlbourough, Massachusetts) require an 8F system. PCI for CTO is also feasible using radial access [42], [43]. A radial approach can be used for either the interventional or the donor guide catheter. The availability of sheathless Eau catheters (Asahi Intecc, Nagoya, Japan) allows a 7F and an 8F interventional lumen for device delivery. Based upon this there is increasing frequency of a combined femoral and radial access approach.
Simultaneous dual injection is critical for determining characteristics of the CTO including lesion length, proximal and distal cap morphology, site of side branches and extent of collaterals. Furthermore, single catheter antegrade injection should be avoided once dissection occurs in the antegrade space with subintimal entry as it may result in hydraulic enlargement of the dissection plane and resulting haematoma expansion [44].
Drug eluting stents (DES) are used almost exclusively to minimise the risk of restenosis [45]. In the GISSOC II-GISE study, DES usage resulted in a lower proportion of patients with recurrent ischaemia at 24 months after CTO PCI compared with bare metal stents (15.1% vs 32.1%, respectively; p = .01) [46].
3. Current PCI techniques
Recent years have seen the development of specialist operators, techniques and equipment that have improved success rates in CTO PCI. Since its inception, the Japanese have been at the forefront of CTO PCI pioneering the retrograde approach. This was in part driven by historically low rates of CABG and therefore the necessity to progress alternative treatments. Adaptations to the Japanese approach have more recently been published from high volume operators in the United States with similarly high rates of success. Both methods require the pre-procedural planning and set-up specified above.
3.1. The Japanese methodology [44], [47]
Japanese CTO specialists have propagated the traditional approach to CTO PCI. This technique usually begins with an antegrade (proximal to distal) approach. They have pioneered multiple strategies to cross the CTO antegrade. These include:
-
1.
Single wire manipulation with wire escalation.
-
2.
Parallel wiring.
-
3.
Seesaw wiring.
-
4.
Balloon anchoring.
-
5.
IVUS guided wiring.
The aim is for a luminal cross of the occluded segment and a significant amount of time may be spent in achieving this. If the subintimal space is entered, the Japanese emphasise limiting the distance of antegrade dissection by attempting to re-enter quickly or switching to a retrograde strategy.
3.1.1. Antegrade approach
3.1.1.1. Single wire manipulation with wire escalation
Initially a soft hydrophilic wire (e.g. Fielder XT-A, Asahi Intecc) is chosen with the aim of seeking out microchannels to traverse the CTO in the intimal space (soft probing). Non-hydrophilic wires with increasing penetration force are used as needed in fibrous CTO segments for loose tissue tracking or intimal plaque tracking [47]. Gradual escalation of wire tip load aims to traverse the CTO with the safest wire, reducing the chance of perforation — the “wire escalation strategy” [47]. Increasingly, the Japanese are using the Gaia wire (Asahi Intecc) during wire escalation. This is a novel CTO wire utilising composite core technology that theoretically allows greater directional control within the body of the CTO without compromising penetration power. Consequently, manipulation via redirection and penetration is required. They have begun to incorporate this wire early during wire escalation for loose tissue and intimal plaque tracking, as well as retrograde distal cap penetration. Protocol based wire escalation cannot be compiled due to variability among Japanese operators.
An overview of available CTO wires is shown above (Table 1). Higher tip load/penetration force wires (particularly if hydrophilic or polymer jacketed e.g. Pilot 200, Abbott) increase the chance of subintimal tracking or passage outside of the vessel architecture. Traditional high penetration force CTO wires (e.g. Conquest Pro, Asahi Intecc) are hydrophobic at the tip and are difficult to redirect, with an associated risk of perforation in tortuous vessels and over long segments.
Table 1.
An overview of currently available wires used in CTO.
| Wire | Manufacturer | Design/Lengths | Coating | Tip load (g) | Penetration force kg/in.2 |
|---|---|---|---|---|---|
| Fielder FC | Asahi | Non-tapered tip. 0.014 in., 180 and 300 cm lengths. | Hydrophilic, polymer jacket | 0.8 | N/A |
| Fielder XT | Asahi | Tapered tip 0.009 in. Shaft 0.014 in., 180 and 300 cm lengths | Hydrophilic, polymer jacket | 0.8 | N/A |
| Fielder XT — A (A for antegrade) |
Asahi | Tapered tip 0.009 in. Shaft 0.014 in., 180 and 300 cm lengths | Hydrophilic, polymer jacket | 1.0 | N/A |
| Fielder XT — R (R for retrograde collateral cross) |
Asahi | Tapered tip 0.009 in. Shaft 0.014 in., 180 and 300 cm lengths | Hydrophilic, polymer jacket | 0.6 | N/A |
| Pilot 50 | Abbott | Non-tapered tip. 0.014 in., 190 and 300 cm lengths | Hydrophilic, polymer jacket | 1.5 | N/A |
| Sion For retrograde collateral cross |
Asahi | Non-Tapered tip. 0.014 in., 180 and 300 cm lengths | Hydrophilic, non-jacketed over spring coil and tip. | 0.7 | N/A |
| Sion Blue Workhorse wire for procedure completion |
Asahi | Non-Tapered tip. 0.014 in., 180 and 300 cm lengths | Hydrophilic, non-jacketed over spring coil. Hydrophobic tip. | 0.5 | N/A |
| Gaia First | Asahi | Tapered tip 0.010 in. Shaft 0.014 in., 190 cm | Hydrophilic, non-jacketed. Tip hydrophilic | 1.5 | Penetration efficiency rather than power. On par with miracle 6 |
| Gaia Second | Asahi | Tapered tip 0.011 in. Shaft 0.014 in., 190 cm | Hydrophilic, non-jacketed. Tip hydrophilic | 3.5 | Penetration efficiency rather than power. On par with miracle 12 |
| Gaia Third | Asahi | Tapered tip 0.011 in. Shaft 0.014 in., 190 cm | Hydrophilic, non-jacketed. Tip hydrophilic | 4.5 | Penetration efficiency rather than power. On par with Conquest Pro 12 |
| Miracle 3/MIRACLEbros 3 | Asahi | Non-tapered tip. 0.014 in., 180 cm length | Hydrophobic (silicone) | 3.0 | 20 |
| Miracle 4.5/MIRACLEbros 4.5 | Asahi | Non-tapered tip. 0.014 in., 180 cm length | Hydrophobic (silicone) | 4.5 | 30 |
| Miracle 6/MIRACLEbros 6 | Asahi | Non-tapered tip. 0.014 in., 180 cm length | Hydrophobic (silicone) | 6.0 | 39 |
| Miracle 12/MIRACLEbros 12 | Asahi | Non-tapered tip. 0.014 in., 180 cm length | Hydrophobic (silicone) | 12.0 | 78 |
| Ultimate Bros 3 | Asahi | Non-tapered tip. 0.014 in., 180 and 300 cm lengths | Hydrophilic, non-jacketed | 3 | 20 |
| Pilot 150 | Abbott | Non-tapered tip. 0.014 in., 190 and 300 cm length | Hydrophilic, polymer jacketed | 2.7 | N/A |
| Pilot 200 | Abbott | Non-tapered tip. 0.014 in., 190 and 300 cm length | Hydrophilic, polymer jacketed | 4.1 | N/A |
| Conquest/Confianza | Asahi | Tapered tip 0.009 in. Shaft 0.014 in. 180 cm length. Spring coil length 20 cm | Hydrophobic (silicone) | 9.0 | 142 |
| Conquest Pro/Confianza Pro | Asahi | Tapered tip 0.009 in. Shaft 0.014 in., 180 cm length. Spring coil length 20 cm | Hydrophilic non-jacketed over spring coil. Hydrophobic tip and shaft | 9.0 | 142 |
| Conquest Pro 12/Confianza Pro 12 | Asahi | Tapered tip 0.009 in. Shaft 0.014 in., 180 cm length. Spring coil length 20 cm | Hydrophilic non-jacketed over spring coil. Hydrophobic tip and shaft | 12.0 | 189 |
| Conquest Pro 8-20/Confianza Pro 8–20 | Asahi | Tapered tip 0.009 in. Shaft 0.014 in., 180 cm length. Spring coil length 17 cm | Hydrophilic non-jacketed over spring coil. Hydrophobic tip and shaft | 20.0 | 315 |
| High Torque CROSS IT 100 XT | Abbott | Tapered tip 0.010 in. Shaft 0.014 in. 190 and 300 cm length. | Hydrophilic including tip, non-jacketed | 1.7 | 22 |
| High Torque CROSS IT 200 XT | Abbott | Tapered tip 0.010 in. Shaft 0.014 in. 190 and 300 cm length. | Hydrophilic including tip, non-jacketed | 4.7 | 60 |
| High Torque CROSS IT 300 XT | Abbott | Tapered tip 0.010 in. Shaft 0.014 in. 190 and 300 cm length. | Hydrophilic including tip, non-jacketed | 6.2 | 79 |
| High Torque CROSS IT 400 XT | Abbott | Tapered tip 0.010 in. Shaft 0.014 in. 190 and 300 cm length. | Hydrophilic including tip, non-jacketed | 8.7 | 110 |
| High Torque Progress 40 | Abbott | Non-Tapered tip 0.014 in. 190 and 300 cm length. | Hydrophilic, non-jacketed. | 4.8 | 30 |
| High Torque Progress 80 | Abbott | Non-Tapered tip 0.014 in. 190 and 300 cm length. | Hydrophilic, non-jacketed. | 9.7 | 63 |
| High Torque Progress 120 | Abbott | Non-Tapered tip 0.014 in. 190 and 300 cm length. | Hydrophilic, non-jacketed. | 13.9 | 90 |
| High Torque Progress 140T | Abbott | Tapered tip 0.0105 in. Shaft 0.014 in. 190 and 300 cm length. | Hydrophilic, non-jacketed. | 12.5 | 144 |
| High Torque Progress 200T | Abbott | Tapered tip 0.009 in. Shaft 0.014 in. 190 and 300 cm length. | Hydrophilic, non-jacketed. | 13.3 | 209 |
| Galeo Hydro S | BIOTRONIK | Non-tapered tip. 0.014 in. 175 cm length. | Hydrophilic 12 cm including tip. Hydrophobic shaft. Non-jacketed | 3.1 | N/A |
| Galeo Hydro F | BIOTRONIK | Non-tapered tip. 0.014 in. 175 cm length. | Hydrophilic 12 cm including tip. Hydrophobic shaft. Non-jacketed | 6 | N/A |
| Galeo Hydro M | BIOTRONIK | Non-tapered tip. 0.014 in. 175 cm length. | Hydrophilic 12 cm including tip. Hydrophobic shaft. Non-jacketed | 4.5 | N/A |
| PT Graphix | Boston | Non-Tapered tip. 0.014 in.. 182 and 300 cm lengths | Hydrophilic, non-jacketed. | 4.0 | 26 |
| Shinobi | CORDIS | Non-tapered tip. 0.014 in. 180 and 300 cm lengths | Hydrophillic. Teflon coated. | 2.0 | 13 |
| Shinobi Plus | CORDIS | Non-tapered tip. 0.014 in. 180 and 300 cm lengths | Hydrophilic Teflon coated. | 4.0 | 26 |
| Persuader 3 | MEDTRONIC | Non-tapered tip. 0.014 in. 190 and 300 cm lengths. | Available in hydrophilic (non-jacketed) and hydrophobic forms. Tip hydrophobic in all variants | 5.1 | 33 |
| Persuader 6 | MEDTRONIC | Non-tapered tip. 0.014 in. 190 and 300 cm lengths. | Available in hydrophilic (non-jacketed) and hydrophobic forms. Tip hydrophobic in all variants | 8 | 52 |
| Persuader 9 | MEDTRONIC | Tapered tip. 0.010 in., Shaft 0.014 in. 190 and 300 cm lengths. | Available in hydrophilic (non-jacketed) and hydrophobic forms. Tip hydrophobic in all variants | 9.1 | 96 |
| Provia 3 | MEDTRONIC | Non-tapered tip. 0.014 in. 180 and 300 cm lengths. | Available in hydrophilic (non-jacketed) and hydrophobic forms. Tip hydrophobic in all variants | 3 | 19 |
| Provia 6 | MEDTRONIC | Non-tapered tip. 0.014 in. 180 and 300 cm lengths. | Available in hydrophilic (non-jacketed) and hydrophobic forms. Tip hydrophobic in all variants | 6 | 39 |
| Provia 9 | MEDTRONIC | Tapered tip. 0.009 in., Shaft 0.014 in. 190 and 300 cm lengths. | Available in hydrophilic (non-jacketed) and hydrophobic forms. Tip hydrophobic in all variants | 9 | 142 |
| Provia 12 | MEDTRONIC | Tapered tip. 0.009 in., Shaft 0.014 in. 190 and 300 cm lengths. | Available in hydrophilic (non-jacketed) and hydrophobic forms. Tip hydrophobic in all variants | 12 | 189 |
| Provia 15 | MEDTRONIC | Tapered tip. 0.009 in., Shaft 0.014 in. 190 and 300 cm lengths. | Available in hydrophilic (non-jacketed) and hydrophobic forms. Tip hydrophobic in all variants | 15 | 236 |
| Muskie | Vascular Solutions, Inc. |
Non-Tapered tip. 0.014 in. 195 and 300 cm lengths. | Hydrophillic, non-jacketed | 3 | 20 |
| Muskie | Vascular Solutions, Inc | Non-tapered tip. 0.014 in. 195 and 300 cm lengths. | Hydrophillic, non-jacketed | 4.5 | 30 |
| Muskie | Vascular Solutions, Inc | Non-tapered tip. 0.014 in. 195 and 300 cm lengths. | Hydrophillic, non-jacketed | 6 | 39 |
| Muskie | Vascular Solutions, Inc | Non-tapered tip. 0.014 in. 195 and 300 cm lengths. | Hydrophillic, non-jacketed | 9 | 58 |
| Muskie | Vascular Solutions, Inc | Non-tapered tip. 0.014 in. 195 and 300 cm lengths. | Hydrophillic, non-jacketed | 12 | 78 |
| High Torque floppy extra support | Abbott | Soft tip, high shaft support | Hydrophobic | 0.6 | N/A |
| Grand slam | Asahi | Soft tip, high shaft support | Hydrophobic | 0.7 | N/A |
| Stabiliser | CORDIS | Soft tip, high shaft support | Hydrophobic | Very soft tip | N/A |
| Stabiliser Plus | CORDIS | Soft tip, very high shaft support | Hydrophobic | Very soft tip | N/A |
| RG 3 | Asahi | Non-tapered tip. Tip 0.014 in., Shaft 0.010 in. 330 cm length | Hydrophilic, non-jacketed over the shaft | 3.0 | N/A |
| Rotawire | Boston Scientific | Monofilament wire. Tip 0.014 in. Shaft 0.009 in. 325 cm | Hydrophobic | N/A | N/A |
| ViperWire Advance | Cardiovascular systems | Non-tapered tip. 0.014 in. 330 cm | Hydrophobic | N/A | N/A |
N.B. Penetration power is the tip load or tip stiffness (in kg) divided by the area of the wire tip (square inches). It is a better representation of wire penetration ability. Shaft stiffness is a different measure that assesses delivery of equipment along the wire shaft. Penetration efficiency is a new concept in relation to the Gaia wire (Asahi Intecc), which describes the coexistence of high penetration force with maintained steerability and torque response within the CTO segment. Tip load and tip diameter data obtained from the respective manufacturer.
Wire escalation is performed with an over the wire (OTW) microcatheter (Table 2). OTW balloons are rarely used, as they induce wire bias and have a profile that may make it difficult to cross the occluded segment after successful wiring.
Table 2.
Overview of available microcatheters (data from manufacturer).
| Microcatheter | Length | Material | Size | Comments | Maker |
|---|---|---|---|---|---|
| Corsair | 135 cm (antegrade) 150 cm (retrograde) |
10 wires of tungsten braiding to form a metallic tube. Tapered soft tip and hydrophilic polymer coating |
1.3F distal 2.8F proximal |
Tapered tip allows progress through occluded segment. Caution in calcified segments as over-rotation may lead to entrapment and unravelling. Mainstay device in CTO intervention. |
Asahi |
| Tornus Tornus 88 Flex |
135 cm 135 cm |
0.12 mm × 8 wires 0.18 mm × 8 wires Intertwined wires make up the shaft |
2.1F proximal 1.8F distal 3.0F proximal to 2.1F distal |
Corkscrew motion to forward advance Advance (counterclockwise rotation) Withdraw (clockwise rotation) After 20 turns of rotation open haemostatic valve to released kinetic energy. Always rotate clockwise to exit lesion. Tornus 88 Flex has twice the penetration ability |
Asahi |
| Stride | 105 cm, 125 cm, 130 cm |
Stainless steel braiding | 2.2 and 2.6F versions | Soft tip. Unlikely to traverse the CTO segment. Reduced wire bias compared to OTW balloon. | Asahi |
| Fine cross | 135 cm 150 cm |
Hydrophilic coating | 1.8F distal 2.6F proximal |
May allow passage due to small distal diameter. Highly deliverable. | Terumo |
| Venture OTW and monorail versions |
140 cm OTW 145 cm monorail |
Deflectable catheter up to 90° | 1.24 mm proximal 0.56 mm distal |
Steerable catheter for wiring tortuous and angulated branches | Vascular Solutions Inc |
| Crusade | 140 cm | 2.2F distal diameter | Double lumen with monorail and OTW component. Ideal for parallel wiring and bifurcation strategies | Kaneka |
The microcatheter offers several advantages. Firstly it provides added support to the wire and increases penetration force. Secondly it allows maintaining position once the lesion is crossed and for wire exchange or wire reshaping. The Corsair catheter (Asahi Intecc) is an OTW hybrid catheter that has features of a microcatheter and a support catheter [48]. It has become the initial microcatheter of choice for most CTO interventions and is usually able to traverse occluded segments once wiring has occurred.
Microchannel navigation and loose tissue tracking utilise the traditional wire manipulation techniques used in conventional angioplasty. Intimal plaque tracking requires two CTO specific wire techniques during wire escalation [47]. Firstly controlled drilling, where the wire is spun through 360-degree rotations and very gently advanced forward such that the wire seeks its own path through the CTO (Fig. 3).
Fig. 3.

Controlled drilling vs penetration for intimal plaque tracking.
Secondly, penetration involves pushing the wire with gentle rotation for penetration of calcified or fibrotic CTO segments. This is also useful for focused reentry to the true lumen from the subintimal space. The wire technique and shape required for these techniques are shown below (Fig. 4, Fig. 5).
Fig. 4.

A 30 to 60 degree distal bend 1 to 2 mm from the tip should be placed on the wire for controlled drilling or penetration. Reentry into the true lumen requires a high penetration force wire with a more acute bend. Reproduced with permission from Thach N et al. Practical Handbook of Advanced Interventional Cardiology: Tips and Tricks, 4th Edition Wiley and Sons [49].
Fig. 5.

Secondary bend 3 to 6 mm from the tip is useful if the proximal vessel is tortuous.
3.1.1.2. Parallel and seesaw wiring technique
In the parallel wire strategy, a wire that enters the subintimal space is left in position to seal that tract and act as a marker. Continued advancement of this wire close to the distal cap should be avoided as it can collapse the distal true lumen and make reentry difficult. A second penetrating wire is therefore introduced using a microcatheter and attempt made at redirection into the true lumen (Fig. 6). The Crusade Catheter (Kaneka, Osaka, Japan) is a double lumen microcatheter that contains both a monorail and an OTW port. It is ideally suited to parallel wiring by allowing the introduction of multiple wires without removal of the catheter from an optimal position.
Fig. 6.

Parallel wire technique.
Seesaw wiring (Fig. 7) involves the use of two microcatheters and wires. It has the advantage of avoiding the need for complex exchange of OTW microcatheters. Also wires can be reshaped and their roles switched promptly.
Fig. 7.

Seesaw wiring technique.
3.1.1.3. Anchor wire or anchor balloon technique
This involves placing a second support wire in a side branch proximal to the occlusion to increase support from the guiding catheter. The balloon anchoring technique involves inflating an appropriately sized balloon in the side branch to stabilise the guide and increase guide support. The disadvantages with these methods include the risk of injury to the side branch and ischaemia if the side branch supplies a large myocardial territory.
3.1.1.4. Intravascular ultrasound guided wiring technique
Intravascular ultrasound (IVUS) features heavily in the Japanese strategy.
IVUS guided proximal cap penetration may be used when an occlusion may be flush with a large side branch. An IVUS catheter can be placed in the proximal side branch for interrogation of the CTO lesion in the main lumen (Fig. 8). IVUS investigation also helps to examine the composition of the plaque and its consistency at the entry site.
Fig. 8.

Flush occlusion with a side branch. Entry into the CTO from the side branch can be facilitated with IVUS placed in the side branch.
If the wire enters a false lumen after the distal cap, the IVUS can be advanced over this wire to investigate the distal true lumen and to assess a favourable reentry location (Fig. 9).
Fig. 9.

IVUS placed in the subintimal space can help guide reentry to the true lumen.
3.1.2. Retrograde approach
Japanese CTO operators pioneered the retrograde CTO approach [44], [47], [50]. The retrograde approach refers to CTO access of the distal cap via collateral vessels. It is usually reserved as a second line strategy for failed intimal antegrade crossing. Failure occurs where the antegrade wire fails to make forward intimal progress or enters the subintimal space and prompt reentry to the true lumen is not possible. The overall aim is to connect antegrade and retrograde channels to allow successful CTO PCI. Reconnecting to the true lumen as close as possible to the proximal or distal cap of the CTO within normal vessel is ideal.
The retrograde approach requires the presence of useable collaterals from the opposing circulation and allows access to the CTO, via the softer distal cap. Angiographic collaterals can be divided into septal and epicardial channels which have different characteristics. Septal channels are safer for wire crossing, as they are less prone to rupture. Successful crossing is not always predictable based on angiographic appearance. In addition, small side branches and tortuosity are often underappreciated on angiography. The Japanese advocate careful progress with repeat injections through the microcatheter to confirm position in the correct channel. If perforation occurs, bleeding is normally contained and rarely results in catastrophic outcomes. Epicardial collaterals on the other hand are fragile and associated with high mortality if rupture occurs and is untreated (usually via cardiac tamponade).
In contrast to the antegrade strategy, subintimal tracking is not considered a failure as it facilitates procedural success using various strategies such as the reverse CART manoeuvre (see below).
The retrograde wire escalation strategy is initially used with a microcatheter to cross the body of the CTO. If the CTO is crossed in the intimal space, the wire is then externalised and angioplasty commences — termed retrograde wire cross. IVUS may be used over the antegrade wire to confirm that the retrograde wire is luminal prior to advancement through the proximal vessel.
Failure of luminal retrograde wire cross (either subintimal wire passage or failure to advance the wire within intima) increases procedural complexity. The Japanese will then introduce an antegrade wire (if not already present) — this is termed antegrade preparation. Subsequently, there are four possible fates for the antegrade and retrograde wires that require different strategies for successful retrograde CTO crossing. The possibilities are listed below (Table 3).
Table 3.
An overview of connecting antegrade and retrograde channels for successful retrograde cross.
| Wire position | Strategy |
|---|---|
| Antegrade intimalRetrograde intimal |
|
| Antegrade subintimal Retrograde subintimal (Ideal situation) |
(Reverse CART) using an adequately size antegrade balloon |
| Antegrade intimal Retrograde subintimal (least favourable) |
|
| Antegrade subintimal Retrograde intimal |
|
Firstly both antegrade and retrograde wires are in the intimal space. In this case the objective is either to advance the antegrade or retrograde wire with the opposing wire as a landmark toward the opposing channel — so called “kissing wire cross”. Antegrade balloon dilatation is the next strategy. This expands the antegrade channel to increase the chance of the retrograde wire finding the antegrade channel and advancing in the intima toward the antegrade guiding catheter. If this fails, intentionally penetrating the subintimal space with the antegrade wire followed by balloon inflation may increase success in connecting the channels.
The most favourable scenario is that both antegrade and retrograde wires are in the subintimal space. The two sides are usually connected when the antegrade space is enlarged via balloon dilatation. This is known as reverse controlled antegrade and retrograde subintimal-tracking (reverse CART) manoeuver (Fig. 10).
Fig. 10.
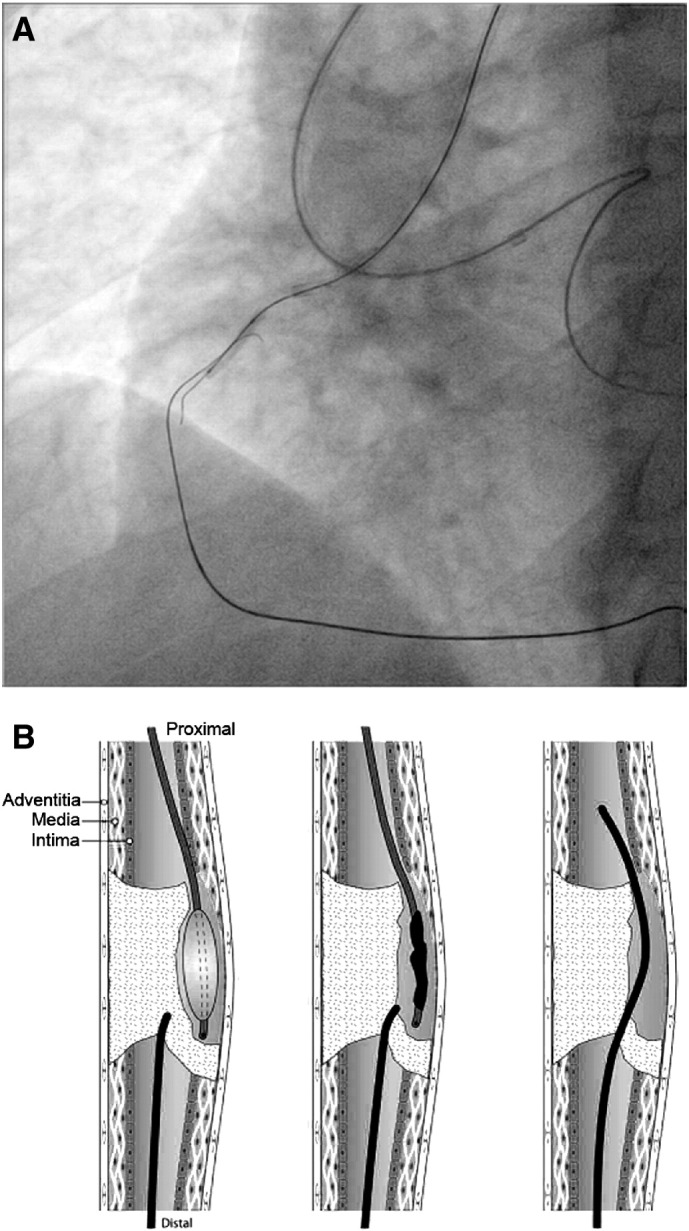
Reverse CART technique. A. Angiographic depiction of the technique. B. A balloon is inflated over the antegrade wire within the subintimal (subluminal) space that is connected proximally to the true lumen. The retrograde wire is advanced toward the newly created space. Imaged reproduced with permission from Joyal et al. [50].
The most challenging scenario occurs where the retrograde wire is subintimal and the antegrade wire is in the true lumen. The difficulty arises because of a large layer of tissue between the two wires. Inflation with an adequately sized balloon in the antegrade space is vital to disturb the body of the CTO and open a passage into the subintimal space. This will allow the retrograde wire to engage the newly created space and hence the antegrade true lumen.
Finally the retrograde wire is intimal and the antegrade wire is subintimal. A CART procedure has been advocated to deal with this scenario. This involves dilating the tract retrograde — the opposite of the reverse CART. The routine use of the CART procedure in this scenario should be avoided, as there is inherent risk in delivering bulky devices along fragile collaterals. Advancing the wire retrograde until it reaches an adjacent subintimal space as the antegrade wire and finishing with a reverse CART to connect the spaces is a more efficient and safe method.
3.1.3. Equipment and wire management following successful CTO crossing
A number of procedural issues require specific attention once the spaces are united:
-
1.
After retrograde crossing and during PCI, the retrograde microcatheter should remain in the distal portion of the native artery covering the collateral bed. Removal prior to PCI completion may result in wire induced collateral transection with resulting rupture.
-
2.
After retrograde luminal connection the wire should be externalised (retrieved out the contralateral sheath). This is performed via wiring of the antegrade guiding catheter or by snaring and retrieving the wire. The retrograde wire used to cross the occlusion is too short for externalisation and is replaced with a long 300 to 325 cm wire.
-
3.
Inability to perform balloon dilatation is an important problem particularly in highly calcified vessels. While rotational atherectomy through a dissection plane is generally contraindicated, the Japanese are confident in using this modality with small to medium burr sizing and in the absence of angiographic staining. If significant staining precludes rotational atherectomy, the procedure may need to be aborted to allow healing and the procedure rescheduled.
-
4.
Removal of OTW equipment while maintaining distal wire position, or exchanging high tip load wires for softer workhorse wires can be achieved via three methods: doc wire, balloon trapping and the aqua plane technique. Regardless of the method used, reliable maintenance of distal wire position is pivotal to procedural success.
3.1.4. Limitations of disseminating the Japanese approach
There are barriers limiting dissemination of some aspects of the Japanese technique to other countries. Firstly the success of Japanese CTO specialists likely reflects a high case volume that allows development of superior wire technique and skill. Unique to Japan is the situation where patient preference results in low rates of CABG and this results in preferential treatment with PCI. Second, health systems outside of Japan may have greater financial and laboratory time limitations. Long case duration may not be feasible when laboratory time is limited. Finally, the Japanese approach is highly individualised making it difficult to teach and disseminate. Concerns have been raised over radiation and contrast volume during protracted cases.
3.1.5. The American methodology [34], [35], [49], [50]
In response to these limitations, the North American total occlusion group has developed an alternate strategy to CTO PCI — the “hybrid” approach. The stated aims of this strategy are to create a systematic approach to CTO intervention with the following goals:
-
1.
Maximise success, while minimising radiation dose, contrast and procedural time.
-
2.
Enhance the teaching and dissemination of CTO techniques and to reduce interoperator variability in CTO success rates via an algorithmic approach.
-
3.
Focus on using workhorse equipment available in most interventional laboratories. Hence a small number of wires are suggested for routine inventory. It proposes easier integration into busy catheter laboratories with minimal interruption to work flow.
-
4.
Clinical factors decide whether revascularisation is needed and precise dual injection angiography to delineate anatomy defines the appropriate technique.
Definite time limits are set for a given strategy with a rapid shift to an alternate approach if no headway is made at the specified time limit. Limitations are set on contrast volume and radiation dose and the procedure is aborted if unsuccessful despite multiple strategies. Failure does not preclude repeat intervention.
The proposed methodology is shown below (Fig. 11).
Fig. 11.

The American methodology — “hybrid approach”. Anatomy defines the strategy [34], [35]. A minimal number of wire choices are available to simplify methodology, minimise cost and allow adoption of the technique in a variety of catheter laboratory environments.
The approach is dictated by 4 major anatomical factors — proximal cap anatomy, length of occlusion, the presence of a landing zone in the distal vessel, and the presence of usable septal or epicardial collaterals. As with the Japanese approach, procedural preparation is critical to success.
3.1.6. Antegrade approach
The antegrade approach requires defined proximal cap anatomy ideally with a tapered stump or defined entry point. The antegrade approach is technically demanding when the entry point is ambiguous or at a bifurcation.
3.1.6.1. Short lesion (< 20 mm)
The approach for short lesions is similar to the Japanese strategy. Wire escalation is chosen as the initial modality, as a successful luminal cross is more likely with short occlusions. The major differences are that specified time limits are set for a change in strategy if successful crossing is not achieved. Also, the technique proposes the use of only a few workhorse wires (likely present in most interventional labs) with rapid wire escalation to wires with a very high tip load if the lesion is not crossed. Intermediate tip load (3.0 to 6.0 g) wires are not present in this algorithm as these wires are felt to be more likely to enter the subintimal space. This is known as the “stiffer is safer” principle [34], [35].
CTO crossing is initially attempted with a soft tipped polymer jacketed wire to seek out microchannels — “probing” (e.g. Fielder FC/XT, Sion [Asahi Intecc], Pilot 50 [Abbott Vascular, Abbott Park, Illinois]). If this fails the next step is rapid escalation to stiffer wires such as the Conquest Pro 12 (Asahi Intecc) if there is a clear distal target. The Pilot 200 (Abbott Vascular) is suggested if the path is unclear or the vessel is tortuous.
Passage into the subintimal space requires an adaptation in strategy. The goal now shifts to traversing the CTO in the subintimal space utilising the safest possible method that minimises the risk of perforation. The algorithm advocates the use of a dedicated dissection/reentry device — the CrossBoss/Stingray reentry system (Boston Scientific). The CrossBoss (Fig. 12) [34], [35], [51] is a metal OTW microcatheter with a rounded tip to minimise the risk of perforation compared with advancing high tip load wires. It is designed to traverse the occluded segment through the subintimal space until it is adjacent to normal true lumen where reentry can occur. This device is rotated rapidly in either direction and advanced without a wire.
Fig. 12.

CrossBoss dissection system (Boston Scientific) [51].
The Stingray device (Fig. 13) is then proposed to facilitate reentry to the true lumen [34], [35], [51]. It consists of a balloon that assumes a flat shape when inflated and allows orientation of the wire toward the adjacent true lumen. The balloon has 2 exit ports opposite one another with a radio-opaque marker distal to each port for orientation toward the true lumen. It includes a high penetration force wire with an extreme tapered distal tip (Stingray wire, Boston Scientific). The Stingray wire is advanced through the exit port into the true lumen to create a communicating channel with the subintimal space. It is then removed and a Pilot 200 used to find this newly created channel for entry into the true lumen and distal wire passage. The wire is then exchanged for a workhorse wire and stenting is performed distal to proximal in the routine fashion. In the absence of usable retrograde channels, inability to re-enter the true lumen antegrade represents a procedural failure and the procedure is terminated.
Fig. 13.

The Stingray reentry system (Boston Scientific) [51].
3.1.6.2. Long lesions (> 20 mm)
The algorithm suggests subintimal tracking as an initial strategy for long segment (> 20 mm) lesions. The rationale is that for long lesions, intimal crossing is unlikely even in the hands of expert operators [32]. Early use of the CrossBoss/Stingray system is advocated to reduce procedural duration.
If antegrade dissection/reentry fails, retrograde bailout via the reverse CART strategy is recommended if useable collaterals exist.
3.1.7. Retrograde approach
The retrograde approach is proposed as a first line strategy where the proximal stump is ambiguous. Wire escalation retrograde through the distal cap is reserved for short lesions (< 20 mm). If the lesion is crossed into the proximal true lumen the wire can then be externalised.
Purposeful dissection retrograde from the outset is reserved for long lesions (> 20 mm). The knuckle wire technique is used as the dissection strategy of choice (Fig. 14). It has little risk of perforation due to the lack of wire tip contact with the subintimal space — hence it is more likely to remain in the vessel architecture. To perform this technique the stiff wire is removed and replaced with a broadly curved softer jacketed wire that is pushed (never rotated) and advanced through the subintimal space. A wire is then advanced from the antegrade direction and the spaces connected via the reverse CART as occurs with the Japanese strategy.
Fig. 14.
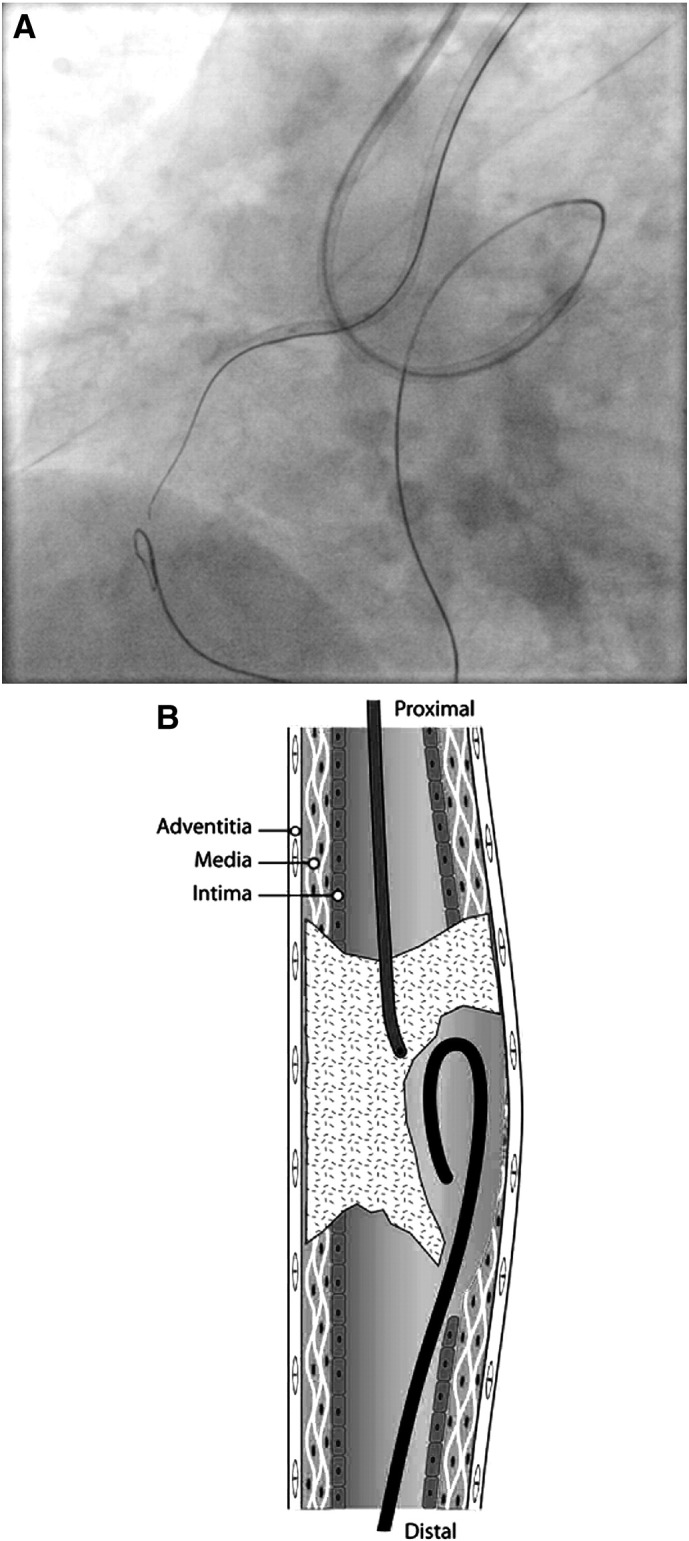
A knuckle is formed on the retrograde wire by first fashioning a broad curve and then advancing forward. A soft polymer jacketed wire (e.g. Fielder XT, Pilot 50) is ideal. Image reproduced with permission from Joyal et al. [50].
3.1.8. Controversies of the North American approach
There are limitations with this strategy. A possible disadvantage with this approach is that purposeful subintimal tracking with a knuckle wire or CrossBoss may make it difficult to salvage large side branches. Many favour exhausting all attempts at true lumen cross when large side branches need to be preserved. In the absence of a dedicated reentry method (such as the Stingray balloon), or retrograde bailout (absence of usable collaterals or expertise), the procedure will terminate with subintimal wire passage if wire reentry is not possible. Purposeful dissection strategies increase the risk of haematoma formation in the subintimal space. Uncontrolled haematoma may rapidly compress the true lumen to the point where reentry is impossible. Haematoma management strategies include controlling knuckle size and the STRAW technique [34], [35].
The importance of minimising the distance of subintimal tracking is uncertain. The approach of creating long segments of antegrade dissection followed by reentry (the STAR technique) has been associated with significant restenosis in long term follow-up and is not widely practiced [52]. Subintimal tracking with the CrossBoss and Stingray system mimics the STAR technique in principle. Long term stent patency and clinical outcomes associated with stenting across large false channels created by these devices has not been assessed in controlled trials. In particular, the effects on stent endothelialisation, late acquired stent malapposition and duration of dual antiplatelet therapy are uncertain.
4. Management of complications
The risk of coronary perforation from the antegrade and retrograde approach was 0.4% in the J-CTO registry [32]. Management includes prolonged balloon inflation and covered stent implantation. Reversal of anticoagulation should be performed judiciously to prevent guide thrombosis. Pericardiocentesis is occasionally required and should be considered when rapid haemodynamic compromise occurs.
Collateral channel rupture is potentially fatal. Septal collateral rupture usually results in self-limiting septal haematoma and may be managed conservatively. Epicardial collateral rupture is more serious and often requires pericardial drainage followed by antegrade and retrograde coiling to complete haemostasis. Coils should be available and operators should be familiar with their use. Reversal of anticoagulation may be life saving but carries a risk of guide thrombosis, that may compromise non-occluded vessels.
Guide thrombosis is a potential complication during prolonged procedures. Regular activated clotting time (ACT) checks should be performed with a target ACT of > 300 s.
Contrast volume is closely monitored and should be minimised at all times.
Routine radiation minimisation techniques are particularly important with prolonged procedures. This involves monitoring patient skin dose, reducing fluoroscopy frame rates and angulation change of the image intensifier at regular intervals to prevent intensified skin doses. Intraprocedural blood loss should be minimised by careful attention to Y-adapter haemostasis.
Over treatment of distal disease should be avoided. Chronic under filling makes it difficult to assess true vessel size. With time, vasodilation and remodelling may result in significant improvements.
5. Conclusion
CTOs are a common and prognostically important finding during coronary angiography. Percutaneous intervention of chronic occlusions pioneered by the Japanese and adapted by North American operators now offers a feasible management strategy for patients. With mentorship, patient selection and specialised equipment PCI success rates are improving worldwide. While the Japanese and North American strategies appear divergent, both add considerable expertise to CTO strategies.
Conflict of interest statement
The authors report no relationships that could be construed as a conflict of interest.
References
- 1.Fefer P., Knudtson M.L., Cheema A.N., Galbraith P.D., Osherov A.B., Yalonetsky S. The Canadian Multicenter Chronic Total Occlusions Registry. Current perspectives on coronary chronic total occlusions. J Am Coll Cardiol. Mar 13 2012;59(11):991–997. doi: 10.1016/j.jacc.2011.12.007. [DOI] [PubMed] [Google Scholar]
- 2.Christofferson R.D., Lehmann K.G., Martin G.V., Every N., Caldwell J.H., Kapadia S.R. Effect of chronic total coronary occlusion on treatment strategy. Am J Cardiol. May 1 2005;95(9):1088–1091. doi: 10.1016/j.amjcard.2004.12.065. [DOI] [PubMed] [Google Scholar]
- 3.Mohr F.W., Morice M.C., Kappetein A.P., Feldman T.E., Stahle E., Colombo A. Coronary artery bypass surgery versus percutaneous coronary intervention in patients with three vessel disease and left main coronary disease: 5 year follow up of the randomised, clinical SYNTAX trial. Lancet. Feb 23 2013;381(9867):629–638. doi: 10.1016/S0140-6736(13)60141-5. [DOI] [PubMed] [Google Scholar]
- 4.Bufe A., Haltern G., Dinh W., Wolfertz J., Schleiting H., Guelkar H. Recanalisation of coronary chronic total occlusions with new techniques including the retrograde approach via collaterals. Neth Heart J. Apr 2011;19(4):162–167. doi: 10.1007/s12471-011-0091-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Claessen B.E., Dangas G.D., Weisz G., Witzenbichler B., Guagliumi G., Mockel M. Prognostic impact of a chronic total occlusion in a non-infarct-related artery in patients with ST-segment elevation myocardial infarction: 3-year results from the HORIZONS-AMI trial. Eur Heart J. Mar 2012;33(6):768–775. doi: 10.1093/eurheartj/ehr471. [DOI] [PubMed] [Google Scholar]
- 6.Lexis C.P., Van der Horst I., Rahel B.M., Lexis M.A., Kampinga M.A., Gu Y.L. Impact of chronic total occlusions on markers of reperfusion, infarct size, and long-term mortality: a substudy from the TAPAS-trial. Catheter Cardiovasc Interv. Mar 1 2011;77(4):484–491. doi: 10.1002/ccd.22664. [DOI] [PubMed] [Google Scholar]
- 7.Van der Schaaf R.J., Vis M.M., Sjauw K.D., Koch K.T., Baan J., Jr., Tijssen J.G. Impact of multivessel coronary disease on long-term mortality in patients with ST-elevation myocardial infarction is due to the presence of a chronic total occlusion. Am J Cardiol. Nov 1 2006;98(9):1165–1169. doi: 10.1016/j.amjcard.2006.06.010. [DOI] [PubMed] [Google Scholar]
- 8.Claessen B.E., Hoebers L.P., Van der Schaaf R.J., Kikkert W.J., Engstrom A.E., Vis M.M. Prevalence and impact of a chronic total occlusion in a non-infarct-related artery on long-term mortality in diabetic patients with ST elevation myocardial infarction. Heart. Dec 2010;96(24):1968–1972. doi: 10.1136/hrt.2010.197673. [DOI] [PubMed] [Google Scholar]
- 9.Claessen B.E., Van der Schaaf R.J., Verouden N.J., Stegenga N.K., Engstrom A.E., Sjauw K.D. Evaluation of the effect of a concurrent chronic total occlusion on long-term mortality and left ventricular function in patients after primary percutaneous coronary intervention. JACC Cardiovasc Interv. Nov 2009;2(11):1128–1134. doi: 10.1016/j.jcin.2009.08.024. [DOI] [PubMed] [Google Scholar]
- 10.Hoebers L.P., Vis M.M., Claessen B.E., der Schaaf RJ Van, Kikkert W.J., Bean J., Jr. The impact of multivessel disease with and without a co-existing chronic total occlusion on short- and long-term mortality in ST-elevation myocardial infarction patients with and without cardiogenic shock. Eur J Heart Fail. Apr 2013;15(4):425–432. doi: 10.1093/eurjhf/hfs182. [DOI] [PubMed] [Google Scholar]
- 11.Jones D.A., Weerackody R., Rathod K., Behar J., Gallagher S., Knight C. Successful recanalization of chronic total occlusions is associated with improved long-term survival. JACC Cardiovasc Interv. April 2012;5(4):380–388. doi: 10.1016/j.jcin.2012.01.012. [DOI] [PubMed] [Google Scholar]
- 12.Joyal D., Afilalo J., Rinfret S. Effectiveness of recanalization of chronic total occlusions: a systematic review and meta-analysis. Am Heart J. Jul 2010;160(1):179–187. doi: 10.1016/j.ahj.2010.04.015. [DOI] [PubMed] [Google Scholar]
- 13.Khan M.F., Wendel C.S., Thai H.M., Mouvahed M.R. Effects of percutaneous revascularization of chronic total occlusions on clinical outcomes: a meta-analysis comparing successful versus failed percutaneous intervention for chronic total occlusion. Catheter Cardiovasc Interv. Jul 1 2013;82(1):95–107. doi: 10.1002/ccd.24863. [DOI] [PubMed] [Google Scholar]
- 14.Hoebers L.P., Claessen B.E., Dangas G.D., Park S.J., Colombo A., Moses J.W. Multinational CTO Registry. Long-term clinical outcomes after percutaneous coronary intervention for chronic total occlusions in elderly patients (≥ 75 years): five-year outcomes from a 1,791 patient multi-national registry. Catheter Cardiovasc Interv. Jul 1 2013;82(1):85–92. doi: 10.1002/ccd.24731. [DOI] [PubMed] [Google Scholar]
- 15.Takagi K., Lelasi A., Chieffo A., Basavarajaiah S., Latib A., Montorfano M. Impact of residual chronic total occlusion of right coronary artery on the long-term outcome in patients treated for unprotected left main disease: the Milan and New-Tokyo registry. Circ Cardiovasc Interv. Apr 2013;6(2):154–160. doi: 10.1161/CIRCINTERVENTIONS.112.000079. [DOI] [PubMed] [Google Scholar]
- 16.Grantham J.A., Jones P.G., Cannon L., Spertus J.A. Quantifying the early health status benefits of successful chronic total occlusion recanalization results from the FlowCardia's approach to chronic total occlusion recanalization (FACTOR) trial. Circ Cardiovasc Qual Outcomes. May 2010;3(3):284–290. doi: 10.1161/CIRCOUTCOMES.108.825760. [DOI] [PubMed] [Google Scholar]
- 17.Hachamovitch R., Rozanski A., Shaw L.J., Stone G.W., Thomson L.E.J., Friedman J.D. Impact of ischaemia and scar on the therapeutic benefit derived from myocardial revascularization vs. medical therapy among patients undergoing stress-rest myocardial perfusion scintigraphy. Eur Heart J. Jul 27 2011;32(8):1012–1024. doi: 10.1093/eurheartj/ehq500. [DOI] [PubMed] [Google Scholar]
- 18.Shaw L.J., Berman D.S., Maron D.J., Mancini G.B., Hayes S.W., Hartigan P.M. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation. Mar 11 2008;117(10):1283–1291. doi: 10.1161/CIRCULATIONAHA.107.743963. [DOI] [PubMed] [Google Scholar]
- 19.Safley D.M., Koshy S., Grantham J.A., Bybee K.A., House J.A., Kennedy K.F. Changes in myocardial ischemic burden following percutaneous coronary intervention of chronic total occlusions. Catheter Cardiovasc Interv. Sep 1 2011;78(3):337–343. doi: 10.1002/ccd.23002. [DOI] [PubMed] [Google Scholar]
- 20.Claessen B.E., Dangas G.D., Godino C., Henriques J.P., Leon M.B., Park S.J. Multinational CTO Registry. Impact of target vessel on long-term survival after percutaneous coronary intervention for chronic total occlusions. Catheter Cardiovasc Interv. Jul 1 2013;82(1):76–82. doi: 10.1002/ccd.24579. [DOI] [PubMed] [Google Scholar]
- 21.Kirschbaum S.W., Baks T., Van den Ent M., Sianos G., Krestin G.P., Serruys P.W. Evaluation of left ventricular function three years after percutaneous recanalization of chronic total coronary occlusions. Am J Cardiol. Jan 15 2008;101(2):179–185. doi: 10.1016/j.amjcard.2007.07.060. [DOI] [PubMed] [Google Scholar]
- 22.Baks T., Van Geuns R.J., Duncker D.J., Cademartiri F., Mollet N.R., Krestin G.P. Prediction of left ventricular function after drug-eluting stent implantation for chronic total coronary occlusions. J Am Coll Cardiol. Feb 21 2006;47(4):721–725. doi: 10.1016/j.jacc.2005.10.042. [DOI] [PubMed] [Google Scholar]
- 23.Dzavik V., Carere R.G., Mancini G.B., Cohen E.A., Catellier D., Anderson T.E. Predictors of improvement in left ventricular function after percutaneous revascularization of occluded coronary arteries: a report from the Total Occlusion Study of Canada (TOSCA). Total Occlusion Study of Canada Investigators. Am Heart J. Aug 2001;142(2):301–308. doi: 10.1067/mhj.2001.116960. [DOI] [PubMed] [Google Scholar]
- 24.Chung C.M., Nakamura S., Tanaka K., Tanigawa J., Kitano K., Akiyama T. Effect of recanalization of chronic total occlusions on global and regional left ventricular function in patients with or without previous myocardial infarction. Catheter Cardiovasc Interv. Nov 2003;60(3):368–374. doi: 10.1002/ccd.10641. [DOI] [PubMed] [Google Scholar]
- 25.Werner G.S., Surber R., Kuethe F., Emig U., Schwarz G., Bahrmann P. Collaterals and the recovery of left ventricular function after recanalization of a chronic total coronary occlusion. Am Heart J. Jan 2005;149(1):129–137. doi: 10.1016/j.ahj.2004.04.042. [DOI] [PubMed] [Google Scholar]
- 26.Kinoshita I., Katoh O., Nariyama J., Otsuji S., Tateyama H., Kobayashi T. Coronary angioplasty of chronic total occlusions with bridging collateral vessels: immediate and follow-up outcome from a large single-center experience. J Am Coll Cardiol. Aug 1995;26(2):409–415. doi: 10.1016/0735-1097(95)80015-9. [DOI] [PubMed] [Google Scholar]
- 27.Stone G.W., Rutherford B.D., McConahay D.R., Johnson W.L., Jr., Giorgi L.V., Ligon R.W. Procedural outcome of angioplasty for total coronary artery occlusion: an analysis of 971 lesions in 905 patients. J Am Coll Cardiol. Mar 15 1990;15(4):849–856. doi: 10.1016/0735-1097(90)90285-w. [DOI] [PubMed] [Google Scholar]
- 28.Srivasta S.S., Edwards W.D., Boos C.M., Grill D.E., Sangiorgi G.M., Garratt K.N. Histologic correlates of angiographic chronic total coronary artery occlusions. influence of occlusion duration on neovascular channel patterns and intimal plaque composition. J Am Coll Cardiol. April 1997;29(5):955–963. doi: 10.1016/s0735-1097(97)00035-1. [DOI] [PubMed] [Google Scholar]
- 29.Katsuragawa M., Fujiwara H., Miyamae M., Sasayama S. Histologic studies in percutaneous transluminal coronary angioplasty for chronic total occlusion: comparison of tapering and abrupt types of occlusion and short and long occluded segments. J Am Coll Cardiol. Mar 1 1993;21(3):604–611. doi: 10.1016/0735-1097(93)90091-e. [DOI] [PubMed] [Google Scholar]
- 30.Werner G., Surber A., Ferrari M., Fritzenwanger M., Figulla H.R. The functional reserve of collaterals supplying long-term chronic total coronary occlusions in patients without prior myocardial infarction. Eur Heart J. Oct 2006;27(20):2406–2412. doi: 10.1093/eurheartj/ehl270. [DOI] [PubMed] [Google Scholar]
- 31.Maiello L., Colombo A., Gianrossi R., Mutinelli M.R., Bouzon R., Thomas J. Coronary angioplasty of chronic occlusions: factors predictive of procedural success. Am Heart J. Sep 1992;124(3):581–584. doi: 10.1016/0002-8703(92)90262-t. [DOI] [PubMed] [Google Scholar]
- 32.Morino Y., Abe M., Morimoto T., Kimura T., Hayashi Y., Muramatsu T. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. Feb 2011;4(2):213–221. doi: 10.1016/j.jcin.2010.09.024. [DOI] [PubMed] [Google Scholar]
- 33.Noguchi T., Miyazaki S., Morii I., Daikoku S., Goto Y., Nonogi H. Percutaneous transluminal coronary angioplasty of chronic total occlusions. Determinants of primary success and long-term clinical outcome. Catheter Cardiovasc Interv. Mar 2000;49:258–264. doi: 10.1002/(sici)1522-726x(200003)49:3<258::aid-ccd7>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 34.http://www.ctofundamentals.org
- 35.Brilakis E.S., Grantham J.A., Rinfret S., Wyman R.M., Burke M.N., Karmpaliotis D. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv. Apr 2012;5(4):367–379. doi: 10.1016/j.jcin.2012.02.006. [DOI] [PubMed] [Google Scholar]
- 36.Thompson C.A., Jayne J.E., Robb J.F., Friedman B.J., Kaplan A.V., Hettleman B.D. Retrograde techniques and the impact of operator volume on percutaneous intervention for coronary chronic total occlusions: an early U.S. experience. JACC Cardiovasc Interv. Sep 2009;2(9):834–842. doi: 10.1016/j.jcin.2009.05.022. [DOI] [PubMed] [Google Scholar]
- 37.Karmpaliotis D., Lembo N., Kalynych A., Carlson H., Lombardi W,.L., Anderson C.N. Development of a high-volume, multiple-operator program for percutaneous chronic total coronary occlusion revascularization: procedural, clinical, and cost-utilization outcomes. Catheter Cardiovasc Interv. Jul 2013;82(1):1–8. doi: 10.1002/ccd.24387. [DOI] [PubMed] [Google Scholar]
- 38.Preetham K., Levy M.S. Radiation Exposure in the Cardiac Catheterization Lab Shifting the Focus From Low Dose, to “No Dose” Exposure. Catheter Cardiovasc Interv. Jul 2013;82(1):17–18. doi: 10.1002/ccd.25027. [DOI] [PubMed] [Google Scholar]
- 39.Soon K.H., Selvanayagam J.B., Cox N., Kelly A.M., Bell K.W., Lim Y.L. Percutaneous revascularization of chronic total occlusions: review of the role of invasive and non-invasive imaging modalities. Int J Cardiol. Mar 2 2007;116(1):1–6. doi: 10.1016/j.ijcard.2006.03.023. [DOI] [PubMed] [Google Scholar]
- 40.Mollet N.R., Hoye A., Lemos P.A., Cademartiri F., Sianos G., McFadden E.P. Value of pre-procedure multi slice computed tomographic coronary angiography to predict the outcome of percutaneous recanalisation of chronic total occlusions. Am J Cardiol. Jan 15 2005;95(2):240–243. doi: 10.1016/j.amjcard.2004.09.009. [DOI] [PubMed] [Google Scholar]
- 41.Soon K.H., Cox N., Wong A., Chaitowitz I., MaCgregor l, Santos P. CT coronary angiography predicts the outcome of percutaneous coronary intervention of chronic total occlusion. J Interv Cardiol. Oct 2007;20(5):359–366. doi: 10.1111/j.1540-8183.2007.00275.x. [DOI] [PubMed] [Google Scholar]
- 42.Rathore S., Hakeem A., Pauriah M., Roberts E., Beaumont A., Morris J.L. Comparison of the transradial and the transfemoral approach in chronic total occlusion percutaneous coronary intervention. Catheter Cardiovasc Interv. Jun 1 2009;73(7):883–887. doi: 10.1002/ccd.21922. [DOI] [PubMed] [Google Scholar]
- 43.Rinfret S., Joyal D., Nguyen C.M., Bagur R., Hui W., Leung R. Retrograde recanalization of chronic total occlusions from the transradial approach; early Canadian experience. Catheter Cardiovasc Interv. Sep 1 2011;78(3):366–374. doi: 10.1002/ccd.23140. [DOI] [PubMed] [Google Scholar]
- 44.Yamane M. Current percutaneous recanalization of coronary chronic total occlusion. Rev Esp Cardiol. Mar 2012;65(3):265–277. doi: 10.1016/j.recesp.2011.10.026. [DOI] [PubMed] [Google Scholar]
- 45.Saeed B., Kandzari D.E., Agostoni P., Lombardi W.L., Rangan B.V., Banerjee S. Use of drug-eluting stents for chronic total occlusions: a systematic review and meta-analysis. Catheter Cardiovasc Interv. Feb 15 2011;77(3):315–332. doi: 10.1002/ccd.22690. [DOI] [PubMed] [Google Scholar]
- 46.Rubartelli P., Petronio A.S., Guiducci V., Sganzerla P., Bolognese L., Galli M. Gruppo Italiano di Studio sullo Stent nelle Occlusioni Coronariche II GISE Investigators. Comparison of sirolimus-eluting and bare metal stent for treatment of patients with total coronary occlusions: results of the GISSOC II-GISE multicentre randomized trial. Eur Heart J. Aug 2010;31(16):2014–2020. doi: 10.1093/eurheartj/ehq199. [DOI] [PubMed] [Google Scholar]
- 47.Sumitsuji S., Inoue K., Ochiai M., Tsuchikane E., Ikeno F. Fundamental wire technique and current standard strategy of percutaneous intervention for chronic total occlusion with histopathological insights. JACC Cardiovasc Interv. Sep 2011;4(9):941–951. doi: 10.1016/j.jcin.2011.06.011. [DOI] [PubMed] [Google Scholar]
- 48.Tsuchikane E., Katoh O., Kimura M., Nasu K., Kinoshita Y., Suzuki T. The first clinical experience with a novel catheter for collateral channel tracking in retrograde approach for chronic coronary total occlusions. JACC Cardiovasc Interv. Feb 2010;3(2):165–171. doi: 10.1016/j.jcin.2009.10.026. [DOI] [PubMed] [Google Scholar]
- 49.Nguyen T., Hu D., Chen S., Kim M., Saito S., Grines C. 4th ed. John Wiley and Sons; 2012. Practical handbook of interventional cardiology: tips and tricks. [Google Scholar]
- 50.Joyal D., Thompson C.A., Grantham J.A., Buller C.E., Rinfret S. The retrograde technique for recanalization of chronic total occlusions. JACC Cardiovasc Interv. Jan 2012;5(1):1–11. doi: 10.1016/j.jcin.2011.10.011. [DOI] [PubMed] [Google Scholar]
- 51.Werner G.S. The BridgePoint devices to facilitate recanalization of chronic total coronary occlusions through controlled subintimal reentry. Expert Rev Med Devices. Jan 2011;8(1):23–29. doi: 10.1586/erd.10.76. [DOI] [PubMed] [Google Scholar]
- 52.Valenti R., Vergara R., Migliorini A., Parodi G., Carrabba N., Cerisano G. Predictors of reocclusion after successful drug-eluting stent-supported PCI of CTO. J Am Coll Cardiol. Feb 5 2013;61(5):545–550. doi: 10.1016/j.jacc.2012.10.036. [DOI] [PubMed] [Google Scholar]