

Abstract
Background
In Mexico, the Northern States are highly impacted by alcohol consumption and associated problems. Little is known about the association between contextual social disadvantage and alcohol use disorder in this region.
Methods
Information from 1,265 current drinkers surveyed in the U.S.-Mexico Study on Alcohol and Related Conditions (UMSARC) was combined with official data on neighborhood disadvantage (index of urban marginalization, a composite of ten indicators of area-level social disadvantage) for 302 neighborhoods. Using statistical marginal models, we estimated the association of neighborhood disadvantage with alcohol use disorder (AUD; based on DSM-5 criteria), alone and with adjustment for individual and contextual covariates. We also tested for moderation of neighborhood disadvantage effects by sex, education, internal migration and border area.
Results
There was a statistically significant increase in the odds of AUD of 59% (AOR=1.59; 95%CI=1.03, 2.46) for every one-point increase on the neighborhood disadvantage scale, after adjustment for covariates. A significant interaction between sex and neighborhood disadvantage was indicated by two measures of additive interaction (AP=0.55; p<0.001 and S=2.55; p<0.001), with higher neighborhood disadvantage related to higher prevalence of AUD for men but not for women. No moderation effects were observed for education, internal migration or border area.
Conclusions
Neighborhood disadvantage is a risk factor for AUD independent of other variables, specifically in men. Studies of contextual variables offer the possibility for understanding the role of collective circumstances on individuals in society. Future studies of alcohol use in this geographic area should consider effects of contextual determinants such as disadvantage.
Keywords: Alcohol Use Disorder, Mexico, Epidemiology, Border Area, Neighborhood characteristics
1. Introduction
According to the Global Burden of Disease Study, in Mexico, alcohol use disorder (AUD) is one of the principal causes of years lived with disability (Lozano et al., 2013). In the population aged 15–49, AUD is one of the leading mental and behavioral disorders contributing to disability-adjusted life years (IHME, 2016). Some of the highest prevalence estimates of substance use disorders (SUD) have been reported in northern Mexico, with 5% of the population aged 18–65 meeting International Classification of Diseases (ICD-10) diagnostic criteria for past-year SUD (Medina-Mora et al., 2003). Results from the U.S.-Mexico Study on Alcohol and Related Conditions (UMSARC), a population-based survey conducted in the U.S.-Mexico border region, estimated that 11.3% of current drinkers in three border cities in the State of Tamaulipas and 18.7% in the non-border city of Monterrey (State of Nuevo León) met DSM-5 criteria for past-year AUD (Cherpitel et al., 2015).
Six states of Northern Mexico share border with the U.S., and approximately 15 million people live in cities along the Mexican side of the border (PAHO, 2007). Each of the border cities includes a significant proportion of its population who arrived by distinct migratory flows from other states in the country. For example, while most people who migrated to Tijuana, in the state of Baja California Norte, arrived from states in the south-west of Mexico, those who migrated to Reynosa, in the State of Tamaulipas, arrived from its neighbor State of Veracruz (El Colef, 2011).
In the current study of AUD in Northern Mexico, we take a social epidemiological approach (Kaufman, 2008), considering social, economic, and cultural factors at the individual and community levels (Galea et al., 2004) that contribute to AUD. Although individual and family-level predictors of AUD in Mexico have been well documented (Ortiz-Hernández et al., 2007), community factors have received less attention. However, in other countries, like the U.S., the relationship between neighborhood socioeconomic level and alcohol use has been the subject of study for many years.
It has been proposed that living in an urban environment may influence the behavior of individual residents through determinants at several levels of aggregation. Galea et al. have proposed a framework that lists a set of urban features most proximal to the individual, that is, the urban living conditions with which an individual regularly interacts. These are the surrounding population structure (i.e., demographic composition), the physical environment (including housing quality, population density, infrastructure), the social environment (including social networks, social support and social capital), and formal and informal health and social services (Galea et al., 2005). Since inequality may arise from any or all of these urban features (Galea and Vlahov, 2005), it is necessary to assess the role of living conditions as a potential determinant of health and, in particular, of mental health and addictions, through analyzing the environmental systems that shape human development (Bonfenbrenner, 1988).
In general, and as summarized by Karriker-Jaffe (2011), hypotheses related to neighborhood disadvantage assert that disadvantaged neighborhoods often have less-protective social environments that fail to control antisocial or illegal behaviors of the residents. These areas also have diminished physical environments, manifested through signs of decay such as vacant housing, litter, and graffiti (which also may result from lower social control of deviance). These stressful social and physical environments can exert a negative impact on mental health (Latkin and Curry, 2003), as well as on health risk behaviors such as unsafe injection practices of drug users (Latkin et al., 2005). Moreover, there are likely psychosocial mechanisms at work in disadvantaged neighborhoods, such as perceived lack of control or feelings of hopelessness, which also may contribute to substance use. These processes may vary according to individuals’ relative position in society, as indicated by different aspects of SES such as education, occupation or income (Kaufman, 2008); theories of “differential vulnerability” (McLeod and Kessler, 1990) propose that people with lower SES have fewer resources such as social support and general resilience to cope with exposure to chronic stressors, such as those that accompany life in disadvantaged urban areas.
Two recent reviews of studies examining the relationship between neighborhood socioeconomic status (SES) and alcohol use in individuals (Bryden et al., 2013; Karriker-Jaffe, 2011) showed mixed support for the hypothesis that area-level disadvantage is associated with alcohol outcomes; nevertheless, there are fairly consistent evidence of neighborhood effects in substance use outcomes, especially for alcohol problem measures (rather than general consumption measures) and for adults (Karriker-Jaffe, 2011). To date, studies of alcohol and neighborhood disadvantage have had three important limitations: 1) a lack of consistency in the definition of neighborhood socioeconomic status; 2) limitations in the geographic areas available for analysis; and 3) varied criteria for measurement of alcohol outcomes (e.g., use, risky use, hazardous use, psychiatric diagnosis of AUD). Only five known studies have examined AUD according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders (DSM) in what are known as “small areas” such as census tracts or zip codes (Buu et al., 2007; Karriker-Jaffe et al., 2012; Molina et al., 2012; Mulia and Karriker-Jaffe, 2012; Silveira et al., 2014), and another two have studied DSM-IV AUD in combination with other drugs (Karriker-Jaffe, 2011; Savage and Mezuk, 2014).
In the study by Karriker-Jaffe et al. (2012), it was suggested that the association between neighborhood disadvantage and alcohol use in small areas may be moderated by gender, whereby men could have elevated heavy drinking in stressful situations or environments due to relaxed social norms, while women could be more negatively affected by worsened conditions of their neighborhoods because they may be more “place-bound” due to their lack of resources. The study reported a small moderation effect (p<0.10) of neighborhood disadvantage on DSM-IV alcohol dependence among Hispanic men who were current drinkers.
When considering moderation of neighborhood effects, one of the most important individual characteristics that has been studied is SES, and several theoretical explanations of how individual SES may moderate the association between neighborhood disadvantage and alcohol use have been proposed. Mulia and Karriker-Jaffe (2012) explicitly tested three of these, analyzing the U.S. National Alcohol Survey: double jeopardy (i.e., living in a disadvantaged neighborhood has a worse effect among those with low individual SES); status inconsistency (i.e., people with low SES living in neighborhoods with high SES may experience higher stress due to not meeting others’ expectations or due to being unfamiliar with social norms), and relative deprivation (i.e., people with low SES in any given neighborhood may experience frustration and stress compared to those better off in the same neighborhood). Results from this study found that among both male and female drinkers, the odds for alcohol problems (which included DSM-IV AUD) were greater in areas of low SES compared to those of medium level, and that the effect was independent of individual SES. Although current drinkers with low SES had higher rates of alcohol problems at each level of neighborhood disadvantage, they did not find statistical evidence supporting any of the three theories in relation to alcohol problems.
In addition to sex and individual SES as possible moderators of the association between neighborhood disadvantage and AUD, there are two features of Northern Mexico that are also likely to affect how the neighborhood environment is related to alcohol use. First, due to job opportunities in maquilas (large manufacturing factories), there is internal migration to border cities from inner states of Mexico, where lower prevalences of alcohol dependence and binge drinking have been reported (Medina-Mora et al., 2012). Second, proximity of the border cities to the U.S. affects urban environmental conditions and social norms. Some specific characteristics of the border area that are likely to be relevant to AUD are the high prevalence of drug trafficking and associated violence, a relatively young population, and stress related to unemployment and poverty (Wallisch and Spence, 2006; Zemore et al., 2016).
The objective of the present study is to examine, for the first time, the relationship between neighborhood disadvantage and AUD in the population living in Northern Mexico, and to test whether this association is moderated by sex, SES, internal migration history or border proximity. We use a secondary analysis of a four-city, representative survey combined with Mexican government data. Unlike most studies published to date, the DSM- 5 definition of AUD is used (APA, 2013), which no longer makes a distinction between abuse and dependence and incorporates the criterion of craving (an intense desire to consume alcohol) in place of legal problems (Hasin et al., 2013). This last point is especially relevant to the present study, as a positive diagnosis for alcohol abuse using earlier diagnostic criteria could be inflated due to the relationship of social or cultural factors (such as discrimination) with alcohol-related legal problems (Babor and Caetano, 2008). Based on prior studies conducted in the U.S. and elsewhere, our hypothesis is that neighborhood disadvantage is an independent risk factor for AUD in this urban Mexican population, and that this association is moderated by sex (where we expect higher rates among males in disadvantaged neighborhoods), individual SES (higher rates among the population with lower SES living in disadvantaged neighborhoods), internal migration (lower rates among internal migrants in disadvantaged neighborhoods) and border proximity (higher rates in disadvantaged neighborhoods in border areas).
2. Methods
2.1. Target Population
The target population consists of approximately 1.5 million Mexicans aged 18–65 living in private homes in four cities in northern Mexico. Cities were selected based on their closeness to Texas, the largest border state in the U.S.
2.2. Procedure
2.2.1. Individual-Level Information
The methodology of the U.S.-Mexico Study on Alcohol and Related Conditions (UMSARC) has been described in detail elsewhere (Cherpitel et al., 2015). Briefly stated, the study, which was carried out from May 2011 to June 2013, used multistage probability sampling to select residents of private homes, aged 18–65, from Nuevo Laredo (n=828), Reynosa and Matamoros (n=821), in the border state of Tamaulipas, and Monterrey (n=811), in the state of Nuevo León (not on the border).
The first sampling stage selected Basic Geostatistical Areas (Areas Geoestadísticas Básicas, AGEBs), which are similar to U.S. census tracts (INEGI, 2010), with probability proportional to size. Given the incidence of robbery, threats, and extortion related to organized crime in some areas, 41 primary sampling units (out of 306) considered by survey administrators to present a high level of risk were randomly replaced. The next sampling stages selected random blocks, then three residences per block, and finally, after administering a brief household census, a resident aged 18–65 was randomly selected from each residence, using a method that allowed for oversampling of men ages 18–34.
Each selected residence was visited at least three times on different days and at different times of day by trained study interviewers to attempt to recruit an occupant and administer a household questionnaire. Once a household member was selected, three additional attempts were made to recruit and administer a face-to-face interview using a computerized individual questionnaire that included 21 sections, with validated scales used in previous studies to measure alcohol consumption and risk factors. When respondents declined to participate or were not at home on any visit, the residence was randomly replaced with another from the same block. The process was repeated until eight surveys were completed in each AGEB. The final cooperation rate was 71.4% (with a response rate of 63.3%) (AAPOR, 2011).
As in previous reports of the UMSARC focusing on AUD (Cherpitel et al., 2015), all analyses reported here are based on the 52% of current drinkers in the sample (i.e., those who reported drinking any kind of beverage containing alcohol in the past 12 months), and with valid information for all variables used in the analysis (n=1,265 in 302 neighborhoods, with a mean number of 4.2 current drinkers per neighborhood).
2.2.1.1. Ethical Approval
All persons surveyed gave written consent to participate in the study. The survey procedures, informed consent process and questionnaire were approved by the ethics committee of the Mexican National Institute of Psychiatry.
2.2.2. Aggregate-Level Data
The individual-level data from the UMSARC were combined with data on neighborhood disadvantage (Index of Urban Marginalization, defined below) compiled at the AGEB level by the National Council on Population (CONAPO), a Mexican government agency. This allowed us to include data from two levels: an aggregated (i.e. contextual) level, in which AGEBs define neighborhood boundaries, and an individual level of selected persons within each neighborhood.
2.3. Measurements
2.3.1. Outcome
Alcohol Use Disorder
This was defined according to the DSM-5 (APA, 2013), using a version of the Composite International Diagnostic Interview (CIDI) (WHO, 1999). The diagnosis is based on eleven symptoms: drinking in larger amounts or over a longer period than originally intended; repeated unsuccessful attempts to cut down or control drinking; spending significant time obtaining alcohol, drinking, or recuperating from the effects of drinking; craving alcohol; failing to meet obligations at work, in school, or at home as a result of drinking; continuing or recurrent social or interpersonal problems caused or exacerbated by the effects of alcohol; cutting back or giving up social, occupational, or recreational activities as a result of drinking; repeated drinking in situations where doing so is physically dangerous; continued drinking despite knowing that alcohol use is producing persistent physical or psychological problems; alcohol tolerance; and withdrawal symptoms. Participants with two or more symptoms in the previous 12 months were classified as having symptoms consistent with a clinical diagnosis of AUD (NIAAA, 2013).
2.3.2. Exposure
Neighborhood Disadvantage
The Index of Urban Marginalization (IUM) is a summary measure of ten indicators from the 2010 Mexican Census related to urban deprivation in four domains: 1) lack of access to education (percent of the population ages 6–14 not attending school and percent of the population ages 15 and over without a complete primary education); 2) lack of access to health services (percent of the population eligible for public health services and percent of women ages 15–49 with children who have died); 3) lack of access to adequate housing (percent of private homes with no connection to a sewage system or septic tank, without a toilet or connection to a water supply, without indoor plumbing, with a dirt floor, or in a condition of overcrowding); and 4) lack of basic appliances (percent of private homes without a refrigerator). The IUM represents relative disparities that exist between urban neighborhoods within cities and between urban zones, and it is measured on a continuous scale on which negative values represent a lesser degree of marginalization and positive values a greater degree. It has been used in previous research on alcohol use (Urquieta et al., 2006). For descriptive purposes, we used the categorical version of this indicator (very low, low, medium, high, or very high disadvantage) calculated by CONAPO using the optimal stratification technique of Dalenius and Hodge (CONAPO, 2015).
2.3.3. Covariates
Covariates were drawn from a review of the international literature on the relation between neighborhood socioeconomic status and alcohol consumption, in addition to other variables relevant to the region under study. The individual socio-demographic variables included sex, age (for descriptive analysis we grouped age into five groups: 18–24, 25–34, 35–44, 45–54 and 55–65), internal migration (whether participants had always lived in the city where they were surveyed vs. not), and three indicators of SES: educational level (less than university or university and above), employment (employed during the last 30 days, unemployed, or other status such as student, homemaker, or retired) and financial hardship (based on three questions on current and expected financial difficulties given current household income, where a higher score on a 1 to 4 scale represents a greater degree of economic hardship) (Vinokur et al., 1996). As in previous studies, education was used as the main indicator of individual SES, while controlling for employment and financial hardship (Lahelma et al., 2006; Mulia and Karriker-Jaffe, 2012). We also considered the type of city where the survey took place (border or non-border city) as a contextual variable. Sex, education, internal migration and border area were treated as effect modifiers.
2.4. Statistical Analysis
Associations between AUD and IUM were estimated with logistic marginal models using generalized estimating equations (GEE). This technique models the dichotomous outcome (AUD) considering the correlation among subjects within neighborhoods, by modelling this correlation in the estimation of regression coefficients and their standard errors (Diez Roux, 2002; Hubbard et al., 2010). The marginal models were fitted specifying an exchangeable working correlation structure. Data analysis was carried out in SUDAAN version 11.0.1 (Research Triangle Institute, 2012).
First, we fitted bivariate models of AUD with neighborhood disadvantage and each covariate. Then we fitted a full model, without interaction terms, controlling for all covariates. After fitting this model, we added an interaction term for neighborhood disadvantage with sex. Using this model, we computed three indices to assess effect modification on an additive scale: relative excess risk due to interaction (RERI), attributable proportion (AP) and synergy index (S) (Knol et al., 2011). These indices with their 95% CIs were computed based on model coefficients and the variance-covariance matrix, using the delta method for the latter (Knol and VanderWeele, 2012). Values of RERI=0, AP=0 or S=1 indicate no interaction, while greater values indicate positive interaction (i.e., more than an additive relationship). For graphical purposes, we computed the conditional predicted probability (Bieler et al., 2010) of AUD for females and males, evaluated at values of low (IUM=−1.0) and high (IUM=0.2) neighborhood disadvantage. The same process was used to separately assess additive interaction for educational level, internal migration and border area. Finally, if an additive interaction was present for a given moderator, stratified models were computed for each level of the moderator to facilitate interpretation.
2.5. Sample Weighting
The sample was weighted to be representative of the target population. Weights were first calculated by city to reflect the multistage design of the survey. Then, the iterative algorithm of raking (Deville et al., 1993; Izrael et al., 2004) was used to fit the census marginal distribution on education and the combination of age and sex. This weight was used in all analyses.
3. Results
About two-thirds of the current drinkers in the study were males (64%). Approximately half were younger than 35, only 18% had studied at the university level, 76% had had some type of employment in the past 30 days, and 70% were natives of the city in which the survey was conducted (Table 1). With respect to the principal exposure, where positive values represent greater disadvantage, the average score on neighborhood disadvantage was −0.61 [range: −1.47, 2.12], which is slightly better off than the Mexican national average, which is zero.
Table 1.
Individual Sociodemographic and Contextual Characteristics. Mexican Sample of Current Drinkers (n=1,265) from the U.S.-Mexico Study on Alcohol and Related Conditions (UMSARC), 2011–2013.
| n | Percent/Mean (s.d.) | |
|---|---|---|
|
|
||
| Individual characteristics | ||
| Sex | ||
| Female | 359 | 35.76 |
| Male | 906 | 64.24 |
| Age | ||
| 18–24 | 266 | 19. 42 |
| 25–34 | 429 | 31.09 |
| 35–44 | 292 | 27.40 |
| 45–54 | 162 | 15.67 |
| 55–65 | 116 | 6.41 |
| Educational Level | ||
| Below university | 999 | 81. 64 |
| Some university or more | 266 | 18.36 |
| Employment | ||
| Employed | 970 | 75. 85 |
| Unemployed | 66 | 4.86 |
| Other (student, homemaker, retired, etc.) | 229 | 19.29 |
| Lived entire life in survey city | ||
| No | 366 | 29. 58 |
| Yes | 899 | 70.42 |
| Financial hardship index (continuous)a | 1,265 | 2.12 (0.79) |
| Contextual variables | ||
| Neighborhood disadvantage (continuous)b | 1,265 | −0.61 (0.44) |
| Neighborhood disadvantage (categorical) | ||
| Very low | 295 | 20. 60 |
| Low | 343 | 30.41 |
| Medium | 555 | 44.29 |
| High/very high | 72 | 4.70 |
| Border city | ||
| No | 406 | 31.1 |
| Yes | 859 | 68.9 |
Note: Frequencies not weighted; percentages weighted. s.d. - standard deviation
Range: 1 to 4
Principal exposure of interest
Table 2 shows the prevalence of AUD in the previous 12 months. There was an AUD diagnosis in 13.5% of current drinkers, with a greater prevalence in men (17%) than in women (7%). The prevalence of AUD in less disadvantaged neighborhoods was 10%, with a monotonic increase to 16% in those areas with high or very high disadvantage. Other high prevalences were observed in persons without university education, the unemployed, and those not living in the border cities.
Table 2.
Prevalence of DSM-5 Alcohol Use Disorder in Previous Year Among Current Drinkers (n=1,265), Total and by Individual Sociodemographic and Contextual Characteristics.
| AUD Prevalence (%)
|
|
|---|---|
| Total | 13.54 |
| Individual characteristics | |
| Sex | |
| Female | 7.02 |
| Male | 17.18 |
| Age | |
| 18–24 | 14. 33 |
| 25–34 | 13.50 |
| 35–44 | 11.93 |
| 45–54 | 16.19 |
| 55–65 | 11.82 |
| Educational level | |
| Below university | 15. 09 |
| Some university or more | 6.65 |
| Employment | |
| Employed | 14. 10 |
| Unemployed | 28.19 |
| Other (student, homemaker, retired, etc.) | 7.67 |
| Lived entire life in survey city | |
| No | 13. 50 |
| Yes | 13.56 |
| Contextual variables | |
| Neighborhood disadvantage (categorical) | |
| Very low | 10. 01 |
| Low | 12.21 |
| Medium | 15.81 |
| High/very high | 16.38 |
| Border city | |
| No | 18. 63 |
| Yes | 11.25 |
Note: percentages are weighted
Table 3 shows the bivariate and multivariate associations between AUD and the covariates, estimated with marginal models. Statistically significant associations were observed for all variables except internal migration. In the bivariate associations, the odds for AUD increased 71% for each point on the neighborhood disadvantage scale (95%CI=1.14, 2.57). After controlling all variables simultaneously, the multivariate model shows that a one-unit increase in neighborhood disadvantage is associated with a statistically significant increase of 59% in the odds of AUD, adjusting for the rest of the variables (95%CI=1.03, 2.46). To understand which of the components of neighborhood disadvantage were most strongly associated with AUD, we replaced the composite measure with each of its components, one at a time. In these models, only the percent living in a house with a dirt floor (in increments of 5%) was significantly related to AUD (OR=1.48; 95%CI=1.03, 2.12). Conditions of overcrowding and the proportion of the population eligible for public services were at the limit of statistical significance (p=0.05), with ORs of 1.09 (95%CI=1.00, 1.18) and 1.16 (95%CI=1.00, 1.34), respectively.
Table 3.
Association of DSM-5 Alcohol Use Disorder in Previous Year with Individual Sociodemographic and Contextual Characteristics, Among Current Drinkers (n=1,265), Unadjusted and Adjusted Estimates.
| Unadjusteda | Adjusted | |||||
|---|---|---|---|---|---|---|
| OR | 95%CI | AOR | 95%CI | |||
|
|
|
|||||
| Neighborhood disadvantage (continuous) | 1.71 | (1.14, 2.57) | * | 1.59 | (1.03, 2.46) | * |
| Sex (ref: female) | 1.00 | – | 1.00 | – | ||
| Male | 2.66 | (1.41, 5.02) | ** | 2.55 | (1.37, 4.74) | ** |
| Age (continuous) | 1.00 | (0.98, 1.01) | 0.99 | (0.97, 1.00) | ||
| Educational level (ref: Some university or more) | 1.00 | – | 1.00 | – | ||
| Below university | 2.55 | (1.44, 4.51) | ** | 2.22 | (1.17, 4.21) | * |
| Current employment (ref: employed) | 1.00 | – | 1.00 | – | ||
| Unemployed | 2.29 | (1.27, 4.15) | ** | 1.57 | (0.85, 2.90) | |
| Other (student, homemaker, retired, etc.) | 0.45 | (0.21, 0.95) | * | 0.66 | (0.30, 1.46) | |
| Lived entire life in survey city (ref: yes) | 1.00 | – | 1.00 | – | ||
| No | 0.96 | (0.64, 1.44) | 1.05 | (0.68, 1.63) | ||
| Index of financial hardship (continuous) | 1.53 | (1.17, 2.00) | ** | 1.47 | (1.12, 1.94) | ** |
| Border city (ref: yes) | 1.00 | – | 1.00 | – | ||
| No | 1.74 | (1.13, 2.67) | * | 2.14 | (1.34, 3.43) | ** |
Note: OR-Odds ratio; AOR-Adjusted Odds Ratio; Cl-Confidence Interval
Unadjusted estimates by bivariate logistic marginal models, with AUD as dependent variable and each predictor as sole independent variable.
p < 0.05;
p < 0.01;
p < 0.001
Per the AP and S indices, a moderation effect on the additive scale was observed between neighborhood disadvantage and sex, but there was no interaction with education, internal migration or border area (table 4). Inspection of point estimates and 95% CIs in Figure 1 shows the interaction effect is due to a higher prevalence of AUD among male drinkers in neighborhoods with high disadvantage, compared to those in neighborhoods with low disadvantage, without differences among females. The stratified model for males, adjusted for all covariates, indicates a significant association of neighborhood disadvantage with AUD (OR=2.23; 95%CI=1.40, 3.56), while the estimate for females is not statistically significant (OR=0.40; 95%CI=0.10, 1.58). Additional sensitivity analyses testing for additive interaction with two other indicators of individual SES (financial hardship and household income) did not show additive interaction in the full model.
Table 4.
Assessment of Effect Modification
| Effect modifier | Indexa
|
|||||||
|---|---|---|---|---|---|---|---|---|
| RERI
|
AP
|
S
|
||||||
| Estimate | 95%CI | Estimate | 95%CI | Estimate | 95%CI | |||
|
|
|
|
||||||
| Sex | 5.63 | (−3.48, 14.75) | 0.55 | (0.33, 0.77) |
** * |
2.55 | (1.55, 4.19) |
** * |
| Educational level | 1.39 | (−3.30, 6.08) | 0.32 | (−0.28, 0.91) | 1.69 | (0.61, 4.70) | ||
| Lived entire life in survey city | 0.31 | (−1.93, 2.54) | 0.16 | (−0.77, 1.08) | 1.47 | (0.17, 12.58) | ||
| Border city | −0.51 | (−2.40, 1.37) | −0.26 | (−1.54, 1.01) | 0.65 | (0.08, 5.57) | ||
Note: RERI = relative excess risk due to interaction; AP = attributable proportion; S = synergy index
Null values for each index are: RERI = 0; AP = 0; S = 1
p < 0.05;
p < 0.01;
p < 0.001
Fig. 1.
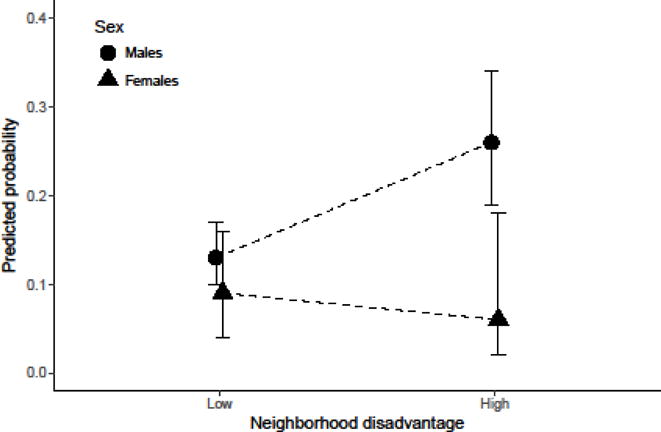
Predicted probability (with 95% bars) of AUD by sex and neighborhood disadvantage among current drinkers.
4. Discussion
For these cities in Northern Mexico, higher neighborhood disadvantage is associated with higher odds of AUD, even after controlling for socio-demographic covariates. We only found evidence of a moderation effect by sex (with neighborhood effects limited to males). There was no moderation by individual SES (measured by education, financial hardship or income), internal migration or border area.
Consistent with previous studies, our results showed the prevalence of AUD increased monotonically with higher levels of neighborhood disadvantage. One U.S. study documented that the prevalence of AUD among the drinking population increased from 3.3% in neighborhoods of high socioeconomic status to 7.7% in those of low socioeconomic status (Mulia and Karriker-Jaffe, 2012). Our estimates also showed an increase in AUD from 10% in less disadvantaged neighborhoods to 16% in those that are most disadvantaged.
The interaction between neighborhood disadvantage and sex indicates that men evidence higher prevalence of AUD at higher levels of disadvantage, while there is no evidence of higher prevalence of AUD for females at higher levels of disadvantage. This result is consistent with that of Karriker-Jaffe (2012), where a three-way interaction between disadvantage, Hispanic ethnicity and male sex indicated a small moderation effect, but it is in contrast with that of Mulia and Karriker-Jaffe (2012), who found that, in a nationally-representative sample of the U.S. population, low neighborhood SES was significantly associated -after controlling for covariates including race/ethnicity- with increased alcohol problems for women, but not for men. It has been suggested that social norms in the neighborhood related to alcohol consumption may apply differently to males and females in different contexts. Our results suggest there may be more liberal norms for males, especially in more disadvantaged neighborhoods, but more restrictive norms for females across all kinds of neighborhoods. It also is likely that males in more disadvantaged neighborhoods have greater access to drinking opportunities outside the house (such as bars and cantinas or in the streets), as is common in Mexico, whereas females in these neighborhoods may be less likely to spend time in public drinking places.
Violence and criminal activities, especially those related to organized crime in border cities such as those included in this survey, for which the U.S. Department of State has issued Travel Warnings to U.S. citizens (U.S.Department of State, 2016), are likely to affect both alcohol use occasions and places of drinking differentially for men and women. Furthermore, since violence concentrates in neighborhoods of low SES in some border cities (Fuentes and Hernández, 2013), the border may be associated with a degraded urban living environment in several ways. For example, people and families leaving a border city may weaken social networks, social support and social capital, while leaving behind uninhabited homes, businesses, and dilapidated urban environments (Fuentes, 2015). Future studies should delve into the relationship between gender, neighborhood violence and alcohol problems in these communities, which have suffered from worsening social conditions in recent years.
We did not find evidence of moderation of neighborhood disadvantage by individual SES as measured by education, which is in contrast with the study by Mulia and Karriker-Jaffe (2012), nor as measured by two other indicators of individual SES, financial hardship and income. In this study we focused only on AUD, but it is possible that individual SES may moderate the effect of neighborhood disadvantage for other alcohol outcomes such as heavy drinking (Chuang et al., 2007). We did not find evidence of moderation by internal migration or by border area either. Since there is substantial internal migration to border cities, where people look for job opportunities at the maquilas, we expected some differential effect of AUD by internal migration.
Although we did not find evidence of synergy between individual and contextual SES, our fully adjusted model indicates that the contextual and individual disadvantage effects are independent of each other. Similar conclusions have been reported in several studies that examine other health outcomes, like mortality or physical and mental health (Pickett and Pearl, 2001). Thus, in this population, effects of neighborhood disadvantage may be mediated by factors at the contextual level (such as diminished social control) and at the individual level (such as lack of resources to deal with stressful situations). In fact, individual financial hardship had a significant association with AUD, independent of neighborhood conditions. Although we might expect financial difficulties to be associated with an overall decrease in alcohol use (Alcohol and Public Policy Group, 2010), our result among past-year drinkers could reflect an increase in drinking (and alcohol problems) in order to cope with financial and other difficulties, or a change in preference for cheaper alcoholic beverages, whose questionable quality might make them more dangerous (WHO, 2000).
A fundamental difference between this and previous studies is the operational definition of neighborhood socioeconomic status. Although most studies base their measurement on a combination of indicators (such as the percentage of the population with a particular educational level or the percentage of the population that is unemployed), it is possible that each study is measuring different constructs. When analyzing each indicator that comprised the measure of neighborhood disadvantage, we found that the strongest predictor of AUD is living in a house with a dirt floor, which is an indicator of very low resources in the community and is correlated to extreme household monetary poverty (López and Ortiz, 2009). Molina, by contrast, analyzed two indicators of neighborhood socioeconomic level that appear to be complementary: “affluence” (percentage of persons with annual income over 75,000 pesos, in management positions, and with high educational level) and “disadvantage” (which included, among other indicators, lack of home ownership, unemployment, and a need for public assistance). However, in that U.S. sample after adjusting for multiple covariates, disadvantage was not associated with AUD, but greater affluence conferred lower risk of AUD (Molina et al., 2012). Future studies should consider exploring carefully how the inclusion of different indicators of economic well-being interact with (possibly potentiating or cancelling out) indicators of disadvantage as predictors of AUD.
Our study has several strengths: it uses the DSM-5 definition of AUD and one of the commonly used indicators of neighborhood disadvantage in Mexico (the Index of Urban Marginalization) which includes several of aspects of urban living conditions described by Galea et al. (2005), namely characteristics of the population, physical environment, social environment and health and social services. Our models also control simultaneously for several possible confounders. The inclusion of aspects of individual socioeconomic status such as educational level, financial difficulties, and employment as control variables allows us to isolate the effect of neighborhood disadvantage more clearly. Finally, the use of marginal models correctly calculates the standard errors for covariate effects in the models.
There are, however, limitations to the interpretation of these results. Our analyses do not include effects for other contextual factors, either to test moderation (Galea et al., 2005) or mediation (Gephart, 1997), by variables such as social capital (community participation or closeness, support, and unity in a community) (Bryden et al., 2013) or neighborhood cohesion (Savage and Mezuk, 2014). Our results do support the conclusions from a longitudinal study following alcoholic men (Buu et al., 2007), which found that neighborhood disadvantage predicted later alcohol problems, but also that a greater number of alcohol-related problems predicted remaining in or migrating to a more disadvantaged neighborhood over time. Given the cross-sectional nature of our study, it is possible that the AUD estimates obtained from drinkers are at least in part a consequence of this downward social migration process. Finally, our results may not generalize to all of northern Mexico, as the cities in our sample may not be representative of the urban regions of the north as a whole.
5. Conclusion
Neighborhood disadvantage is a risk factor for AUD independent of other variables, specifically in men. Given that the border population keeps growing, in part because of internal migration of young men, an increase in demand for services, housing, and employment would be expected (Tuirán and Ávila, 2002). For this reason, it is necessary to understand the relationship between urban disadvantage and problems related to alcohol use in order to implement preventive measures at the neighborhood level. From a more academic point of view, studies of contextual variables offer the possibility of understanding the role of collective circumstances on individuals in society and using this knowledge to assess the extent to which substance use disorders arise from these factors. Future studies on alcohol use in this geographic area should consider the effect of such contextual determinants.
Highlights.
Higher neighborhood disadvantage is related to higher DSM-5 alcohol use disorder (AUD) prevalence
This association is moderated by sex
Financial hardship is related to AUD after adjusting for neighborhood disadvantage
Acknowledgments
Role of Funding Source
Research reported in this publication was supported by the National Institute on Alcohol Abuse and Alcoholism of the National Institutes of Health under award number R01AA018365 (C.C., PI). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funding source had no role in the study design or analysis.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributors
Authors Orozco and Borges designed the study. Orozco conducted the statistical analysis with advice from Ruiz-Velasco, Benjet, Karriker-Jaffe and Zemore. Orozco wrote the first draft of the manuscript and subsequent versions contained input from Moreno, Karriker-Jaffe, Zemore, Cherpitel, and all the other authors. All authors contributed to and have approved the final manuscript.
Conflict of Interest
No conflict declared
References
- AAPOR. Standard Definitions: Final Dispositions of Case Codes and Outcome Rates for Surveys. 7. The American Association for Public Opinion Research; 2011. [Google Scholar]
- Alcohol and Public Policy Group. Alcohol: no ordinary commodity–a summary of the second edition. Addiction. 2010;105:769–779. doi: 10.1111/j.1360-0443.2010.02945.x. [DOI] [PubMed] [Google Scholar]
- APA. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 1. American Psychiatric Association; Arlington, VA: 2013. [Google Scholar]
- Babor TF, Caetano R. The trouble with alcohol abuse: What are we trying to measure, diagnose, count and prevent? Addiction. 2008;103:1057–1059. doi: 10.1111/j.1360-0443.2008.02263.x. [DOI] [PubMed] [Google Scholar]
- Bieler GS, Brown GG, Williams RL, Brogan DJ. Estimating model-adjusted risks, risk differences, and risk ratios from complex survey data. Am J Epidemiol. 2010;171:618–623. doi: 10.1093/aje/kwp440. [DOI] [PubMed] [Google Scholar]
- Bonfenbrenner U. Interacting systems in human development. Research paradigms: Present and future. In: Bolger N, Caspi A, Downey G, Moorehouse M, editors. Persons in Context: Developmental Process. Cambridge University Press; New York: 1988. pp. 25–49. [Google Scholar]
- Bryden A, Roberts B, Petticrew M, McKee M. A systematic review of the influence of community level social factors on alcohol use. Health Place. 2013;21:70–85. doi: 10.1016/j.healthplace.2013.01.012. [DOI] [PubMed] [Google Scholar]
- Buu A, Mansour M, Wang J, Refior SK, Fitzgerald HE, Zucker RA. Alcoholism effects on social migration and neighborhood effects on alcoholism over the course of 12 years. Alcohol Clin Exp Res. 2007;31:1545–1551. doi: 10.1111/j.1530-0277.2007.00449.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cherpitel CJ, Ye Y, Bond J, Zemore SE, Borges G, Greenfield TK. Border effects on DSM-5 alcohol use disorders on both sides of the U.S.-Mexico border. Drug Alcohol Depend. 2015;148:172–179. doi: 10.1016/j.drugalcdep.2015.01.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chuang YC, Li YS, Wu YH, Chao HJ. A multilevel analysis of neighborhood and individual effects on individual smoking and drinking in Taiwan. BMC Public Health. 2007;7:151. doi: 10.1186/1471-2458-7-151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- CONAPO. #x000CD;ndice de marginación urbana 2010. Consejo Nacional de Población; 2015. http://www.conapo.gob.mx/en/CONAPO/Indice_de_marginacion_urbana_2010 (accessed February 2016) [Google Scholar]
- Deville JC, Sarndal CE, Sautory O. Generalized raking procedures in survey sampling. J Am Stat Assoc. 1993;88:1013–1020. [Google Scholar]
- Diez Roux AV. A glossary for multilevel analysis. J Epidemiol Community Health. 2002;56:588–594. doi: 10.1136/jech.56.8.588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Colef El. Movimientos Migratorios En La Frontera De México. 1. El Colegio de la Frontera Norte, El colegio de San Luis; Tijuana, BC: 2011. Ires y Venires. [Google Scholar]
- Fuentes CM. El impacto de las viviendas deshabitadas en el incremento de delitos (robo a casa habitación y homicidios) en Ciudad Juárez, Chihuahua, 2010. Frontera Norte. 2015;27:171–196. [Google Scholar]
- Fuentes CM, Hernández V. Assessing spatial pattern of crime in Ciudad Juárez, Chihuahua, Mexico (2009): The macrolevel, mesolevel and microlevel approaches. Int J Crim Soc Theory. 2013;6:242–259. [Google Scholar]
- Galea S, Freudenberg N, Vlahov D. Cities and population health. Soc Sci Med. 2005;60:1017–1033. doi: 10.1016/j.socscimed.2004.06.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galea S, Nandi A, Vlahov D. The social epidemiology of substance use. Epidemiol Rev. 2004;26:36–52. doi: 10.1093/epirev/mxh007. [DOI] [PubMed] [Google Scholar]
- Galea S, Vlahov D. Urban health: Evidence, challenges, and directions. Annu Rev Public Health. 2005;26:341–365. doi: 10.1146/annurev.publhealth.26.021304.144708. [DOI] [PubMed] [Google Scholar]
- Gephart MA. Neighborhoods and communities as contexts for development. In: Brooks-Gunn J, Duncan GJ, Aber JL, editors. Neighborhood Poverty, Volume 1: Context and Consequences for Children. Russell Sage Foundation; New York: 1997. pp. 1–43. [Google Scholar]
- Hasin DS, O’Brien CP, Auriacombe M, Borges G, Bucholz K, Budney A, Compton WM, Crowley T, Ling W, Petry NM, Schuckit M, Grant BF. DSM-5 criteria for substance use disorders: Recommendations and rationale. Am J Psychiatry. 2013;170:834–851. doi: 10.1176/appi.ajp.2013.12060782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hubbard AE, Ahern J, Fleischer NL, Van der Laan M, Lippman SA, Jewell N, Bruckner T, Satariano WA. To GEE or not to GEE: Comparing population average and mixed models for estimating the associations between neighborhood risk factors and health. Epidemiol. 2010;21:467–474. doi: 10.1097/EDE.0b013e3181caeb90. [DOI] [PubMed] [Google Scholar]
- IHME. Data Visualizations. GBD Compare. 2016 http://ihmeuw.org/3z9r (accessed December 2016)
- INEGI. Compendio De Criterios y Especificaciones Técnicas Para La Generación De Datos e Información De Caracter Fundamental. Instituto Nacional de Estadística y Geografía; Aguascalientes, México: 2010. [Google Scholar]
- Izrael D, Hoaglin DC, Battaglia MP. To rake or not to rake is not the question anymore with the enhanced raking macro. 2004 www2.sas.com/proceedings/sugi29/207-29.pdf (accessed February 2016)
- Karriker-Jaffe KJ. Areas of disadvantage: A systematic review of effects of area-level socioeconomic status on substance use outcomes. Drug Alcohol Rev. 2011;30:84–95. doi: 10.1111/j.1465-3362.2010.00191.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karriker-Jaffe KJ, Zemore SE, Mulia N, Jones-Webb R, Bond J, Greenfield TK. Neighborhood disadvantage and adult alcohol outcomes: Differential risk by race and gender. J Stud Alcohol Drugs. 2012;73:865–873. doi: 10.15288/jsad.2012.73.865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaufman JS. Social epidemiology. In: Rothman KJ, Greenland S, Lash TL, editors. Modern Epidemiology. Lippincott Williams and Wilkins; Philadelphia, PA: 2008. pp. 532–548. [Google Scholar]
- Knol MJ, VanderWeele TJ. Recommendations for presenting analyses of effect modification and interaction. Int J Epidemiol. 2012;41:514–520. doi: 10.1093/ije/dyr218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knol MJ, VanderWeele TJ, Groenwold RH, Klungel OH, Rovers MM, Grobbee DE. Estimating measures of interaction on an additive scale for preventive exposures. Eur J Epidemiol. 2011;26:433–438. doi: 10.1007/s10654-011-9554-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahelma E, Laaksonen M, Martikainen P, Rahkonen O, Sarlio-Lahteenkorva S. Multiple measures of socioeconomic circumstances and common mental disorders. Soc Sci Med. 2006;63:1383–1399. doi: 10.1016/j.socscimed.2006.03.027. [DOI] [PubMed] [Google Scholar]
- Latkin CA, Curry AD. Stressful neighborhoods and depression: A prospective study of the impact of neighborhood disorder. J Health Soc Behav. 2003;44:34–44. [PubMed] [Google Scholar]
- Latkin CA, Williams CT, Wang J, Curry AD. Neighborhood social disorder as a determinant of drug injection behaviors: A structural equation modeling approach. Health Psychol. 2005;24:96–100. doi: 10.1037/0278-6133.24.1.96. [DOI] [PubMed] [Google Scholar]
- López LF, Ortiz E. Medición multidimensional de la pobreza en México: Significancia estadística en la inclusión de dimensiones no monetarias. Estud Econ. 2009:3–33. [Google Scholar]
- Lozano R, Gomez-Dantes H, Garrido-Latorre F, Jimenez-Corona A, Campuzano-Rincon JC, Franco-Marina F, Medina-Mora ME, Borges G, Naghavi M, Wang H, Vos T, Lopez AD, Murray CJ. Burden of disease, injuries, risk factors and challenges for the health system in Mexico. Salud Publica Mex. 2013;55:580–594. [PubMed] [Google Scholar]
- McLeod JD, Kessler RC. Socioeconomic status differences in vulnerability to undesirable life events. J Health Soc Behav. 1990;31:162–172. [PubMed] [Google Scholar]
- Medina-Mora ME, Borges G, Lara C, Benjet C, Blanco J, Fleiz C, Villatoro J, Rojas E, Zambrano J, Casanova L, Aguilar-Gaxiola S. Prevalence of mental disorders and use of services: Results from the Mexican Nacional Survey of Psychiatric Epidemiology. Salud Ment. 2003;26:1–16. [Google Scholar]
- Medina-Mora ME, Villatoro J, Fleiz C, Téllez-Rojo MM, Méndoza-Alvarado LR, Romero-Martínez M, Gutiérrez-Reyes JP, Castro-Tinoco M, Hernández-Ávila M, Tena-Tamayo C, Alvear-Sevilla C, Guisa-Cruz V. Encuesta Nacional De Adicciones 2011: Reporte De Alcohol. Instituto Nacional de Psiquiatría Ramón de la Fuente; Instituto Nacional de Salud Pública; Secretaría de Salud; México, D.F: 2012. [Google Scholar]
- Molina KM, Alegria M, Chen CN. Neighborhood context and substance use disorders: a comparative analysis of racial and ethnic groups in the United States. Drug Alcohol Depend. 2012;125(Suppl 1):S35–S43. doi: 10.1016/j.drugalcdep.2012.05.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mulia N, Karriker-Jaffe KJ. Interactive influences of neighborhood and individual socioeconomic status on alcohol consumption and problems. Alcohol Alcohol. 2012;47:178–186. doi: 10.1093/alcalc/agr168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NIAAA. Alcohol Use Disorder: A Comparison Between DSM-IV and DSM-5. National Institute on Alcohol Abuse and Alcoholism; 2013. http://pubs.niaaa.nih.gov/publications/dsmfactsheet/dsmfact.htm (accessed November 2014) [Google Scholar]
- Ortiz-Hernández L, López-Moreno S, Borges G. Socioeconomic inequality and mental health: a Latin American literature review. Cad Saude Publica. 2007;23:1255–1272. doi: 10.1590/s0102-311x2007000600002. [DOI] [PubMed] [Google Scholar]
- PAHO. United States - Mexico Border Area, Health in the Americas 2007. II. Panamerican Health Organization; Washington, DC: 2007. pp. 732–744. [Google Scholar]
- Pickett KE, Pearl M. Multilevel analyses of neighbourhood socioeconomic context and health outcomes: A critical review. J Epidemiol Community Health. 2001;55:111–122. doi: 10.1136/jech.55.2.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Research Triangle Institute. SUDAAN Language Manual. 1 and 2. Research Triangle Park; NC: 2012. Release 11. [Google Scholar]
- Savage JE, Mezuk B. Psychosocial and contextual determinants of alcohol and drug use disorders in the National Latino and Asian American Study. Drug Alcohol Depend. 2014;139:71–78. doi: 10.1016/j.drugalcdep.2014.03.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Silveira CM, Siu ER, Anthony JC, Saito LP, de Andrade AG, Kutschenko A, Viana MC, Wang YP, Martins SS, Andrade LH. Drinking patterns and alcohol use disorders in Sao Paulo, Brazil: The role of neighborhood social deprivation and socioeconomic status. PLoS One. 2014;9:e108355. doi: 10.1371/journal.pone.0108355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tuirán R, Ávila JL. In: Delimitación de la franja fronteriza del norte de México. Consejo Nacional de Población, editor. La Situación Demográfica De México; México, D.F.: 2002. pp. 89–100. [Google Scholar]
- U.S.Department of State. Mexico Travel Warning. Bureau of Consular Affairs. 2016 https://travel.state.gov/content/passports/en/alertswarnings/mexico-travel-warning.html (accessed December 2016)
- Urquieta JE, Hernandez-Avila M, Hernandez B. Tobacco and alcohol consumption among youth in marginalized urban zones in Mexico: analysis of related decisions. Salud Publica Mex. 2006;48(Suppl 1):S30–S40. doi: 10.1590/s0036-36342006000700005. [DOI] [PubMed] [Google Scholar]
- Vinokur AD, Price RH, Caplan RD. Hard times and hurtful partners: How financial strain affects depression and relationship satisfaction of unemployed persons and their spouses. J Pers Soc Psychol. 1996;71:166. doi: 10.1037//0022-3514.71.1.166. [DOI] [PubMed] [Google Scholar]
- Wallisch LS, Spence RT. Alcohol and drug use, abuse, and dependence in urban areas and colonias of the Texas-Mexico border. Hisp J Behav Sci. 2006;28:286–307. [Google Scholar]
- WHO. Composite International Diagnostic Interview (CIDI – Authorize Core Version 1.0) World Health Organization; Geneva: 1999. [Google Scholar]
- WHO. Estimating per capita alcohol consumption, International Guide for Monitoring Alcohol Consumption and Related Harm. World Health Organization; Geneva: 2000. pp. 21–35. [Google Scholar]
- Zemore SE, Cherpitel CJ, Ye Y, Borges G, Li L, Wallisch LS. Factors explaining variation in alcohol use disorder prevalence across border and non-border communities in Texas. Alcohol Clin Exp Res. 2016;40:1707–1716. doi: 10.1111/acer.13124. [DOI] [PMC free article] [PubMed] [Google Scholar]