

Abstract
We describe a 48-year-old man with cholecystolithiasis whose preoperative magnetic resonance cholangiopancreatography (MRCP) scan showed that the right accessory hepatic duct branching from the cystic duct dominated an anterior segment of the right hepatic lobe. We observed the right accessory hepatic duct using intraoperative cholangiography, and we were able to perform laparoscopic cholecystectomy without injuring it. He had no complication after discharge, and a drip-infusion cholangiography-computed tomography (DIC-CT) scan demonstrated that the right accessory hepatic duct was intact, and it dominated an anterior segment of the right hepatic lobe. During laparoscopic cholecystectomy, a bile duct injury is the most challenging perioperative complication. We selected MRCP preoperatively; however, if it is necessary for us to observe an anomalous biliary tract more precisely, we recommend selecting DIC-CT endoscopic retrograde cholangiopancreatography. Additionally, we think a bile duct injury can be avoided with intraoperative cholangiography, even if there is an anomalous biliary tract.
INTRODUCTION
A right accessory hepatic duct is a type of anomalous biliary tract, and its incidence rate is 1.02% [1]. Most anomalous biliary tracts include a posterior segment of the right hepatic branch; a right accessory hepatic duct that dominates an anterior segment of the right hepatic lobe is relatively rare. We herein describe a case of laparoscopic cholecystectomy (LC) in a man with cholecystolithiasis whose right accessory hepatic duct branching from the cystic duct dominated an anterior segment of the right hepatic lobe.
CASE REPORT
A 48-year-old Japanese man experienced abdominal pain after dinner. He underwent computed tomography (CT), and we observed stones in his cystic duct (Fig. 1). Hematological findings showed no liver dysfunction. A magnetic resonance cholangiopancreatography (MRCP) scan demonstrated that the right accessory hepatic duct branching from the cystic duct dominated an anterior segment of the right hepatic lobe (Fig. 2). Therefore, we diagnosed him as cholelithiasis with an anomalous biliary tract, and LC was planned.
Figure 1:
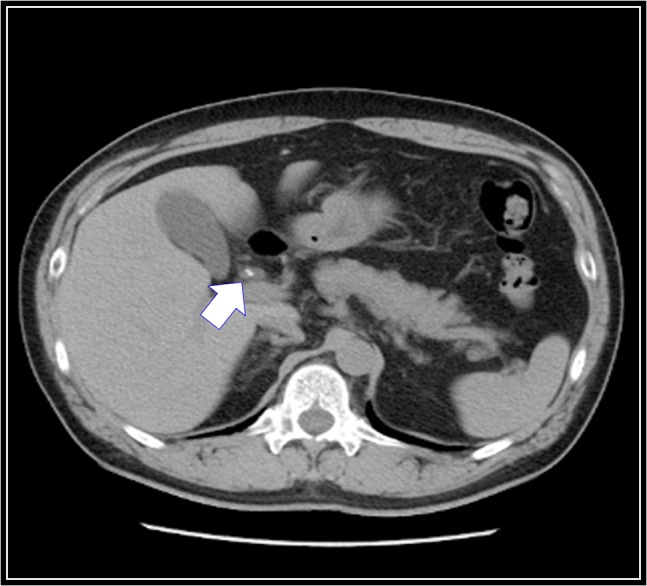
Preoperative abdominal computed tomography scan. There are stones in his cystic duct (white arrow).
Figure 2:
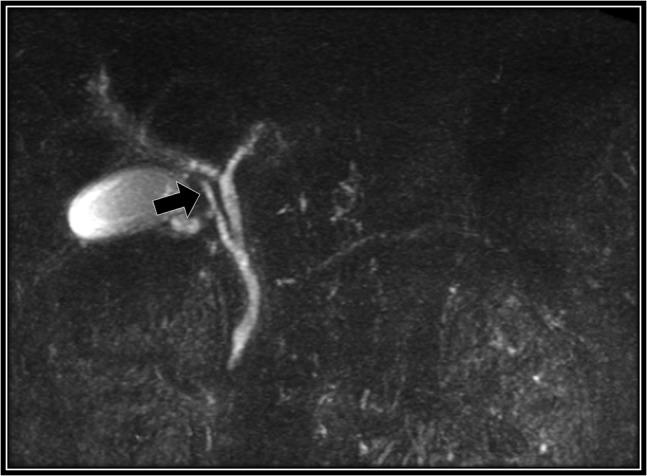
Preoperative magnetic resonance cholangiopancreatography scan. The right accessory hepatic duct branching from the cystic duct (black arrow) dominates an anterior segment of the right hepatic lobe.
The patient was placed in supine position. Initially, intracorporeal procedures were performed in the laparoscopic view through four trocars (one 12-mm port and three 5-mm ports). We considered using intraoperative cholangiography to explore the right accessory hepatic duct. We incised the serosa by the neck of the gallbladder, used the Rouviere sulcus as a landmark, and peeled off the Calot triangle near the gallbladder. Subsequently, we identified the cystic artery and isolated it. Then we identified the cystic duct, and we inserted a cholangiography tube into it. The intraoperative cholangiography image showed that the right accessory hepatic duct branching from the cystic duct dominated an anterior segment of the right hepatic lobe (Fig. 3). Next, we isolated the cystic duct while preserving the right accessory hepatic duct. We resected the gallbladder. The total operating time was 125 min, and the intraoperative blood loss was minimal. Since the patient's postoperative course was uneventful, he was discharged 4 days later. We performed drip-infusion cholangiography-CT (DIC-CT) 48 days postoperatively. The DIC-CT scan demonstrated that the right accessory hepatic duct was intact, and it dominated an anterior segment of the right hepatic lobe (Fig. 4).
Figure 3:
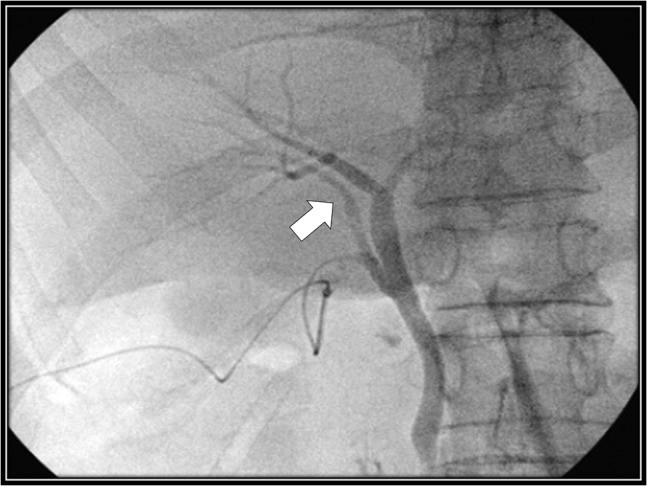
Intraoperative cholangiography image. The right accessory hepatic duct branching from the cystic duct (white arrow) dominates an anterior segment of the right hepatic lobe.
Figure 4:
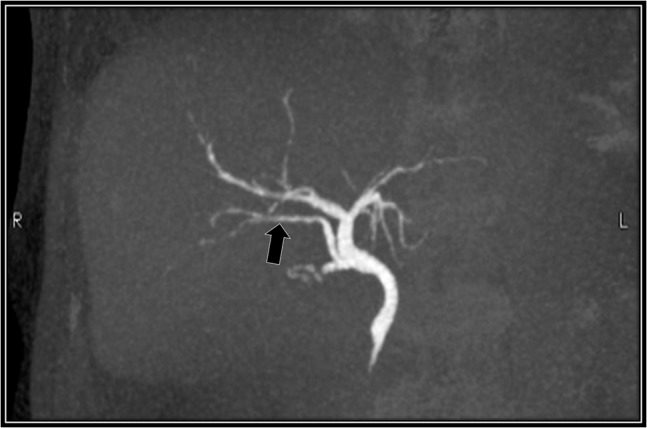
Drip-infusion cholangiography-computed tomography scan. Forty-eight days postoperatively, the right accessory hepatic duct is intact (black arrow), and it dominates an anterior segment of the right hepatic lobe, as indicated by the intraoperative cholangiography scan.
DISCUSSION
A right accessory hepatic duct is one of the intrahepatic bile ducts that dominates the hepatic segment, and it merges into a common hepatic duct, common bile duct, cystic duct or gallbladder. Kune et al. [2] defined an accessory hepatic duct in patients without a right hepatic duct, and they emphasized that in these cases, the ducts should not be called an accessory hepatic duct since the anterior and posterior segments of the right hepatic branch directly merge into a common hepatic duct. Thus, the definition of a right accessory hepatic duct is obscure, and the incidence rates of a right accessory hepatic duct have been reported as 0.8 [3] to 1.02% [1], 18 [4] and 38% [5]. Flint et al. [6] classified three types, Matsunaga et al. [7] classified four types, Hayes et al. [4] classified five types and Hisatsugu et al. [2] classified six types (types 0–V) of right accessory hepatic ducts according to its opening site using several modalities. Hisatsugu reported that the incidence rates of a types I and V were 16.8% (34 cases) and 6.9% (14 cases), respectively, in 202 patients with an anomalous biliary tract [8]. Additionally, patients with types I or V have the greatest risk of injury during cholecystectomy [8]. Similar to other hospitals, we examined patients planned to undergo LC, because we had to determine whether there were stones in the common bile duct and whether they had an anomalous biliary tract. We performed MRCP in these patients. However, if we unable to observe stones and an anomalous biliary tract, we selected DIC-CT as a secondary examination, and if there were stones in the common bile duct, we performed endoscopic retrograde cholangiopancreatography (ERCP). According to Kumon et al. [9], most right accessory hepatic ducts are an infraportal duct [9], and they dominate the posterior segment of the right hepatic lobe. Generally, a posterior segment of the hepatic lobe merges into the common hepatic duct through the cranial side of the hilar plate. On the other side, an infraportal duct short circuits the caudal side of the right branch of the portal vein, and it merges into the common hepatic duct. Therefore, an infraportal duct is often observed near the Rouviere sulcus after a surgeon peels off the Calot triangle between the Hartmann pouch and Rouviere sulcus during LC. As our case was not equivalent to Hisatsugu's classification, we considered that our case was rarer than patients in whom the right accessory hepatic duct dominates a posterior segment of the right hepatic lobe. A search in Pub-Med using the keywords ‘right accessory hepatic duct’, ‘anterior segment’, generated five items, including conference proceedings. However, there were no specific descriptions of the right accessory hepatic duct dominating an anterior segment of the right hepatic lobe. Conversely, a search in Ichushi’ (from April 2003 to November 2015) using the keywords along with ‘right accessory hepatic duct’, ‘anterior segment’, resulted in three cases, including ours. However, one article was a conference proceeding, and the other cases included patients with a communicating accessory bile duct. During LC, a bile duct injury is the most difficult perioperative complication. Although the frequency of a bile duct injury has been reduced, its incidence is 0.57%. In a previous report [10], a bile duct injury occurred in 201 (0.65%) of 31 000 patients, and an accessory hepatic duct injury occurred in 8 (4%) of the 201 patients. Such as aforementioned, in addition to the CT, we should use MRCP in patients planned to undergo LC, and should select DIC-CT or ERCP in certain situations. On the basis of these examinations, we performed LC. In patients with an anomalous biliary tract, physicians should prevent a biliary tract injury by using MRCP, DIC-CT and ERCP during the preoperative examination to confirm the route of the biliary tract.
ACKNOWLEDGMENTS
None.
FUNDING
None.
CONFLICTS OF INTEREST STATEMENT
None of the authors has any conflict of interest to declare.
REFERENCES
- 1. Hisatsugu T, Yamamoto H, Igimi H, Konomi K, Hurusawa T, Jimi M, et al. . Anomaly of bile duct including aberrant right hepatic duct with cholecystolithiasis. Rinshou Seijinbyou (J Adult Dis) 1974;4:581–6. [article in Japanese]. [Google Scholar]
- 2. Kune GA, Sali A. The Practice of Biliary Surgery. 2nd edn Oxford: Blackwell, 1980;1–31. [Google Scholar]
- 3. Okada K, Tamio T, Sakuramoto K, Saigusa T, Okajima K. Studies with ERCP in cases with anomalies of biliary tract, with special references of variation of cystic duct. J Gastroenterol Surg 1981;14:1197–203. [article in Japanese]. [Google Scholar]
- 4. Hayes MA, Goldenberg I, Bioshop CC. The developmental basis for bile duct anomalies. Surg Gynecol Obstet 1958;107:447–56. [PubMed] [Google Scholar]
- 5. Michels NA. The hepatic, cystic and retroduodenal arteries and their relations to the biliary ducts with samples of the entire celiacal blood supply. Ann Surg 1951;133:503–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Flint ER. Abnormalities of the right hepatic, cystic, and gastroduodenal arteries, and of the bile ducts. Br J Surg 1922;1:509–19. [Google Scholar]
- 7. Matsunaga A, Tokunaga S, Takeuchi M, Kuwahara Y, Ohba S, Arita T, et al. . A clinical study on the accessory hepatic duct. J Gastroenterol Surg 1989;22:65–71. [article in Japanese]. [Google Scholar]
- 8. Hisatsugu T. Japanese Society of Biliary Surgery SI-1 Variations of extrahepatic bile duct and surgery. 1993:22:1–8 [article in Japanese].
- 9. Kumon M, Matsushima M, Itahara T, Mori W, Araki K, Kawasaki H, et al. . A dissection of hepatic portal portion and caudate lobe by the liver casts. J Biliary Tract Pancreas 1989;10:1417–22. [article in Japanese]. [Google Scholar]
- 10. Urakami A, Tsunoda T, Ensako T, Muta Y, Aoyama Y, Murakami H, et al. . Bile duct injury during laparoscopic cholecystectomy, 1997–2002: a multicenter study of 201 bile duct injuries in 31,000 operations in Japan. Kawasaki Med J 2012;38:107–18. [article in Japanese]. [Google Scholar]