

Supplemental Digital Content is available in the text
Keywords: cardiovascular disease, epidemiology, immune-mediated inflammatory diseases
Abstract
To analyze in several immune-mediated inflammatory diseases (IMIDs) the influence of demographic and clinical-related variables on the prevalence of cardiovascular disease (CVD), and compare their standardized prevalences.
Cross-sectional study, including consecutive patients diagnosed with rheumatoid arthritis, psoriatic arthritis, psoriasis, systemic lupus erythematosus, Crohn disease, or ulcerative colitis, from rheumatology, gastroenterology, and dermatology tertiary care outpatient clinics located throughout Spain, between 2007 and 2010. Our main outcome was defined as previous diagnosis of angina, myocardial infarction, peripheral vascular disease, and/or stroke. Bivariate and multivariate logistic and mixed-effects logistic regression models were performed for each condition and the overall cohort, respectively. Standardized prevalences (in subjects per 100 patients, with 95% confidence intervals) were calculated using marginal analysis.
We included 9951 patients. For each IMID, traditional cardiovascular risk factors had a different contribution to CVD. Overall, older age, longer disease duration, presence of traditional cardiovascular risk factors, and male sex were independently associated with a higher CVD prevalence. After adjusting for demographic and traditional cardiovascular risk factors, systemic lupus erythematosus exhibited the highest CVD standardized prevalence, followed by rheumatoid arthritis, psoriasis, Crohn disease, psoriatic arthritis, and ulcerative colitis (4.5 [95% confidence interval (CI): 2.2, 6.8], 1.3 [95% CI: 0.8, 1.8], 0.9 [95% CI: 0.5, 1.2], 0.8 [95% CI: 0.2, 1.3], 0.6 [95% CI: 0.2, 1.0], and 0.5 [95% CI: 0.1, 0.8], respectively).
Systemic lupus erythematosus, rheumatoid arthritis, and psoriasis are associated with higher prevalence of CVD compared with other IMIDs. Specific prevention programs should be established in subjects affected with these conditions to prevent CVD.
1. Introduction
Cardiovascular diseases (CVDs) include numerous conditions associated with a high and growing worldwide global burden, representing the most common cause of death.[1] Atherosclerosis is the most common cause of CVD, and several factors, both nonmodifiable (such as genetic factors) and modifiable (including traditional and nontraditional cardiovascular risk factors), are involved in its development. Moreover, atherosclerosis is considered an immune system–mediated process[2]: the accumulation and interplay in the subendothelial region of the arterial wall of several blood-borne inflammatory and immune cells (including autoreactive lymphocytes), as well as resident cells, such as endothelial, smooth muscle and dendritic cells, and other components of the immune system, such as cytokines, chemokines, and antibodies, results in the formation of atherosclerotic plaques, leading to a narrowing of the arterial lumen and, following plaque rupture, to thrombosis.
Considering the underlying mechanisms of this process, it is not surprising that immune-mediated and inflammatory diseases (IMIDs), such as rheumatoid arthritis, systemic lupus erythematosus, psoriasis, psoriatic arthritis, and inflammatory bowel disease, are associated with higher rates of cardiovascular morbidity and mortality, primarily due to accelerated atherosclerosis.[3] Although IMIDs can be associated with a higher prevalence of well-known cardiovascular risk factors, such as metabolic syndrome, smoking, type 2 diabetes, and obesity, these factors do not fully account for the greater prevalence and incidence of CVDs observed in patients with IMIDs when compared to that of the general population.[4] Therefore, IMID-associated factors, such as chronic systemic inflammation,[5] a predisposing genetic background, or the treatment used in these conditions, must contribute to the higher cardiovascular risk.
The objective of this study was to analyze the contribution of different demographic and disease-related variables and traditional cardiovascular risk factors in the prevalence of CVD in subjects affected with rheumatoid arthritis, psoriatic arthritis, psoriasis, systemic lupus erythematosus, or inflammatory bowel disease. Furthermore, we compared the prevalence of CVD among these conditions while adjusting for demographic and traditional cardiovascular risk factors.
2. Patients and methods
2.1. Setting and subjects
The data on patients included in this study were collected between June 2007 and December 2010 as part of the immune-mediated inflammatory disease consortium (IMIDC), a network of Spanish researchers working on the genomic basis of IMIDs[6] that includes patients diagnosed with rheumatoid arthritis, psoriatic arthritis, psoriasis, systemic lupus erythematosus, Crohn disease, and ulcerative colitis. Because the aim of IMIDC is to uncover the common genomic background of IMIDs, we included diseases with a known or suspected genetic overlap.[7] In addition, we selected conditions with a mayor associated burden, in terms of prevalence, disability, and mortality.[8–10] Subjects were enrolled after giving informed consent, from rheumatology, gastroenterology, and dermatology outpatient clinics belonging to tertiary centers and located in several cities throughout Spain (Fig. S1).
All of the patients with rheumatoid arthritis fulfilled the 1987 American College of Rheumatolgy (ACR) diagnosis criteria,[11] all psoriatic arthritis patients fulfilled the CASPAR criteria,[12] all psoriasis patients fulfilled clinical criteria of plaque psoriasis, all systemic lupus erythematosus patients fulfilled the 1997 ACR criteria,[13] and all ulcerative colitis and Crohn disease patients fulfilled the standard Lennard-Jones diagnostic criteria.[14]
At the time of inclusion, demographic and clinical data were collected and recorded following a standard protocol of questionnaires, completed after a clinical interview with closed questions and a review of medical records. Some items on the questionnaires were common to all diseases (including those regarding demographic data, traditional cardiovascular risk factors, and cardiovascular events), whereas other items were specific for each IMID. In addition, informed consent was obtained from all participants, and a blood sample was withdrawn for genomic, proteomic, and metabolomic studies.
Protocols and questionnaires were reviewed and approved by the local institutional review boards. This study was conducted in accordance with the Declaration of Helsinki.
2.2. Variables
The dependent variable in our analysis was the presence of CVD, which was defined as a previous diagnosis (given by any physician), of at least one of the following: angina, myocardial infarction, peripheral vascular disease, and/or stroke. To be classified as a case, all cardiovascular events had to have occurred after the diagnosis of the IMID, except for psoriasis, in which we considered as cases those diagnosed with CVD after disease onset. Subjects diagnosed with CVD before the diagnosis of the IMID were excluded from the analysis.
The presence or absence of traditional cardiovascular risk factors (arterial hypertension, type 2 diabetes, obesity, dyslipidemia, and history of smoking) was assessed in all the cohorts (except for the presence of arterial hypertension in psoriatic arthritis patients; due to an informatics error, that information was lost when recorded in our Web-based questionnaires). Other variables common to all cohorts were sex; age at inclusion in the study; elapsed time from IMID diagnosis (disease onset in the case of psoriasis) to inclusion in the study (in years); number of disease-modifying drugs used (categorized in tertiles), such as methotrexate, antimalarials, leflunomide, sulfasalazine, cyclophosphamide, cyclosporine, and acitretin; and use of biological therapy (such as anti-Tumor Necrosis Factors, rituximab, abatacept, efalizumab, and ustekinumab).
In each IMID cohort, several disease-related variables were also analyzed: in the rheumatoid arthritis patients, the presence of rheumatoid factor, the presence and levels of anti-citrullinated peptide antibodies, and previous diagnoses of extra-articular manifestations (such as subcutaneous nodules, pulmonary fibrosis [defined as any interstitial lung disease diagnosed between the diagnosis of the rheumatoid arthritis and the inclusion in the study], and serositis) were included in the study. In the psoriatic arthritis cohort, the presence of axial/peripheral involvement and the severity of the skin disease were included (using the Psoriasis Area Severity Index). The latter was also analyzed in the psoriasis patients, as was the presence of associated arthritis. In systemic lupus erythematosus patients, the presence of vitiligo, family history of other IMIDs, and different disease-related variables, such as the presence of severe central nervous system manifestations, serositis, arthritis, antiphospholipids syndrome, or antiphospholipids antibodies, were included. In the Crohn disease and ulcerative colitis cohorts, the presence of extraintestinal manifestations was also assessed.
2.3. Statistical analysis
Continuous variables were described using the median and interquartile range. Categorical variables were described using proportions.
Comparison of continuous and categorical demographic and CVD-related variables among IMIDs was performed using analysis of variance or χ2 test, respectively. Post-hoc comparisons were adjusted using the Bonferroni correction.
First, we analyzed separately in each IMID cohort the association between the demographic and clinical-related variables and CVD using bivariate and multivariate logistic regression models. Model selection was performed using the Bayesian information criterion.[15] Multicollinearity was assessed by calculating the variance inflation factors (VIFs) of the dependent variables included in the final multivariate regression models.
Second, to assess the association between common demographic and clinical-related variables and CVD in the overall IMIDC, we performed bivariate and multivariate mixed-effects logistic regression models nested by IMID, due to the structure of our sample, integrated by independent cohorts of patients affected by different conditions.
Finally, to compare the prevalence of CVD among the different IMIDs, we performed logistic regression models adjusted for disease, demographic, traditional cardiovascular risk factors, and common disease-related variables. From those models, the standardized prevalence of each IMID was calculated using marginal analysis. Analyses were performed using STATA 12 statistical software (STATA Corp, College Station, TX).
3. Results
We included 9951 patients in the analysis. The demographic characteristics and the prevalence of CVD and traditional cardiovascular risk factors are shown in Table 1. Patients with Crohn disease were the youngest (median age 47), whereas patients with rheumatoid arthritis were the oldest (median age 61). Similarly, Crohn disease had the highest prevalence of secondary or higher education (55.5%) and rheumatoid arthritis had the lowest (33.7%). Systemic lupus erythematosus and rheumatoid arthritis involved the highest proportion of women (93.2% and 77.7%, respectively). The psoriasis and psoriatic arthritis cohorts had the highest prevalence of type 2 diabetes (8.1% and 8.0%, respectively) and obesity (25.8% and 24.6%, respectively). The rheumatoid arthritis and systemic lupus erythematosus cohorts had the highest prevalence of arterial hypertension (29.7% and 23.4%, respectively). Rheumatoid arthritis, systemic lupus erythematosus, and psoriasis had the highest prevalence of dyslipidemia (20.1%, 16.5%, and 17.5%, respectively). Crohn disease, psoriasis, ulcerous colitis, and systemic lupus erythematosus had the highest prevalence of current/past smoking (74.6%, 69.7%, 62.1%, and 62.0%, respectively). Finally, rheumatoid arthritis patients were treated with the highest number of disease-modifying drugs (median number 2) and biological therapy (42.5%). The unadjusted prevalence of CVD for rheumatoid arthritis, psoriatic arthritis, psoriasis, systemic lupus erythematosus, Crohn disease, and ulcerative colitis were 4.2%, 2.1%, 3.8%, 3.2%, 0.7%, and 1.5%, respectively.
Table 1.
Demographic characteristics and prevalence of cardiovascular disease and traditional cardiovascular risk factors of the patients included in this study.
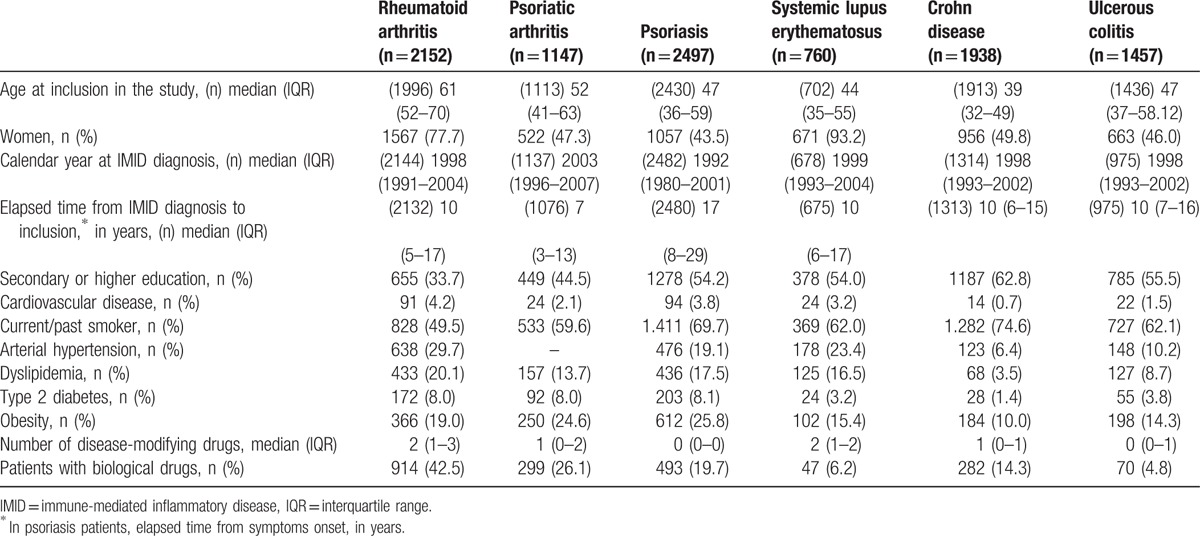
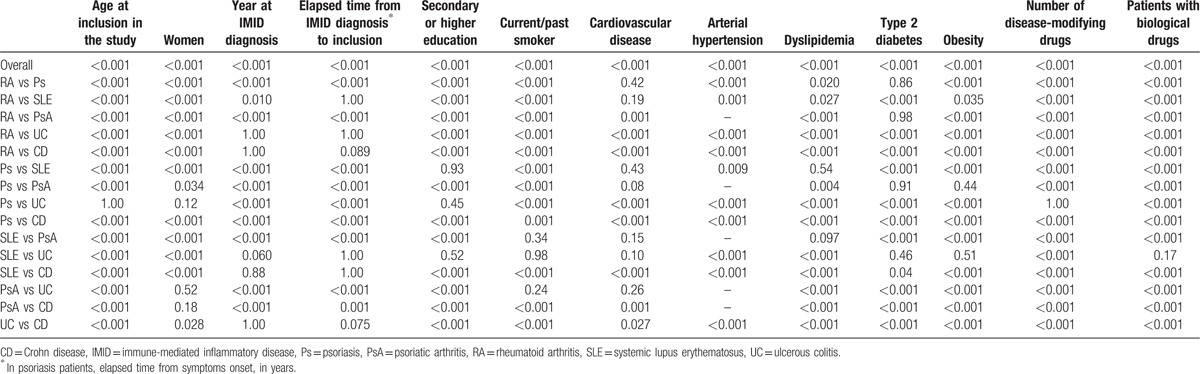
Table 2 shows the results from the comparisons among IMIDs regarding demographic and CVD-related variables. The disease-specific clinical data from each IMID are shown in S1 Table.
Table 2.
Comparison of demographic and cardiovascular disease–related variables among the immune-mediated inflammatory diseases included in this study.
3.1. Influence of demographic and clinical variables in CVD in each IMID
Bivariate (S2 to S6 Tables) and multivariate (Table 3) logistic regression models were used to analyze the association between demographic, traditional cardiovascular risk factors, and disease-specific clinical variables and CVD in each IMID.
Table 3.
Multivariate logistic regression models to analyze the association between demographic and clinical characteristics and cardiovascular disease in rheumatoid arthritis, psoriatic arthritis, psoriasis patients, systemic lupus erythematosus, Crohn disease, and ulcerative colitis patients.
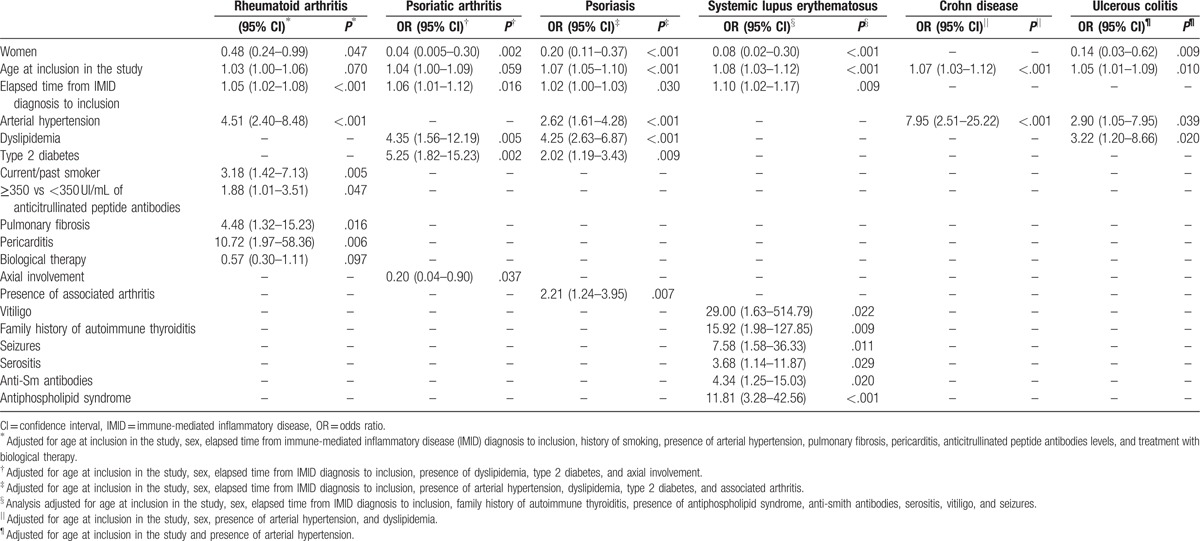
In the best fitting multivariate models, older age at inclusion in the study was associated with a higher risk of CVD in all cohorts except for psoriatic arthritis and rheumatoid arthritis. Women were associated with a lower risk in all conditions except for Crohn disease. In addition, a longer elapsed time from IMID diagnosis to inclusion in the study was associated with a higher cardiovascular risk except for inflammatory bowel disease. Regarding traditional risk factors, dyslipidemia was associated with a higher risk of CVD in psoriatic arthritis, psoriasis, and ulcerative colitis; arterial hypertension in inflammatory bowel disease, rheumatoid arthritis, and psoriasis; type 2 diabetes in psoriatic arthritis and psoriasis; and current/past smoking in rheumatoid arthritis. With regard to the disease-specific variables, in psoriatic arthritis, axial involvement was associated with lower cardiovascular risk; in rheumatoid arthritis, the presence of pulmonary fibrosis, pericarditis, and high anticitrullinated peptide antibodies levels were associated with higher risk; in systemic lupus erythematosus, family history of autoimmune thyroiditis and the presence of antiphospholipid syndrome, anti-Sm antibodies, serositis, vitiligo, and seizures were associated with higher risk; and in psoriasis, the presence of arthritis was also associated with higher risk of CVD. With regard to treatment, neither the use of a greater number of disease-modifying drugs nor the use of biological therapies was associated with CVD in any cohort. No significant multicollinearity was observed among the variables introduced in the final models (mean VIFs 1.15, 1.07, 1.17, 1.04, 1.12, and 1.10, for rheumatoid arthritis, psoriatic arthritis, psoriasis, systemic lupus erythematosus, Crohn disease, and ulcerative colitis, respectively).
3.2. Influence of the demographic and clinical-related variables in CVD risk on the overall IMIDC, and standardized prevalence of CVD
Next, we studied the cardiovascular risk of the variables collected in all the cohorts in the entire IMIDC (S7 Table). We observed that male sex, older age at inclusion in the study, longer elapsed time from IMID diagnosis to the inclusion in the study, and the presence of traditional cardiovascular risk factors were independently associated with a higher risk of CVD. Although in the bivariate analysis, higher education and current/past smoking were significantly associated with lower and higher risk of CVD, respectively, in the multivariate analysis, no significant association was observed.
Finally, we compared the risk of CVD among the different IMIDs, adjusting for the demographic and common clinical variables (Table 4). We observed that before adjustment and using rheumatoid arthritis as the reference IMID for comparison, psoriasis and systemic lupus erythematosus had a lower, although not significantly lower risk of CVD, whereas inflammatory bowel disease and psoriatic arthritis had a significantly lower risk. After adjustment for demographic variables, psoriasis continued to have a lower although not significant risk of CVD, whereas systemic lupus erythematosus exhibited a significantly higher risk of CVD. Inflammatory bowel disease and psoriatic arthritis both had a significantly lower risk. Similar results were observed after adjusting for demographic variables, traditional cardiovascular risk factors, and educational level, except for Crohn disease, which showed a nonsignificantly lower risk of CVD. When systemic lupus erythematosus was used as the reference comparison, all IMIDs showed a significantly lower CVD risk. The standardized prevalence and 95% confidence interval (95% CI) for systemic lupus erythematosus, rheumatoid arthritis, psoriasis, Crohn disease, psoriatic arthritis, and ulcerative colitis were 4.5 (95% CI: 2.2, 6.8), 1.3 (95% CI: 0.8, 1.8), 0.9 (95% CI: 0.5, 1.2), 0.8 (95% CI: 0.2, 1.3), 0.6 (95% CI: 0.2, 1.0), and 0.5 (95% CI: 0.1, 0.8), respectively (Fig. 1).
Table 4.
Bivariate and multivariate logistic regression models to compare the risk of cardiovascular disease among the different immune-mediated inflammatory diseases.
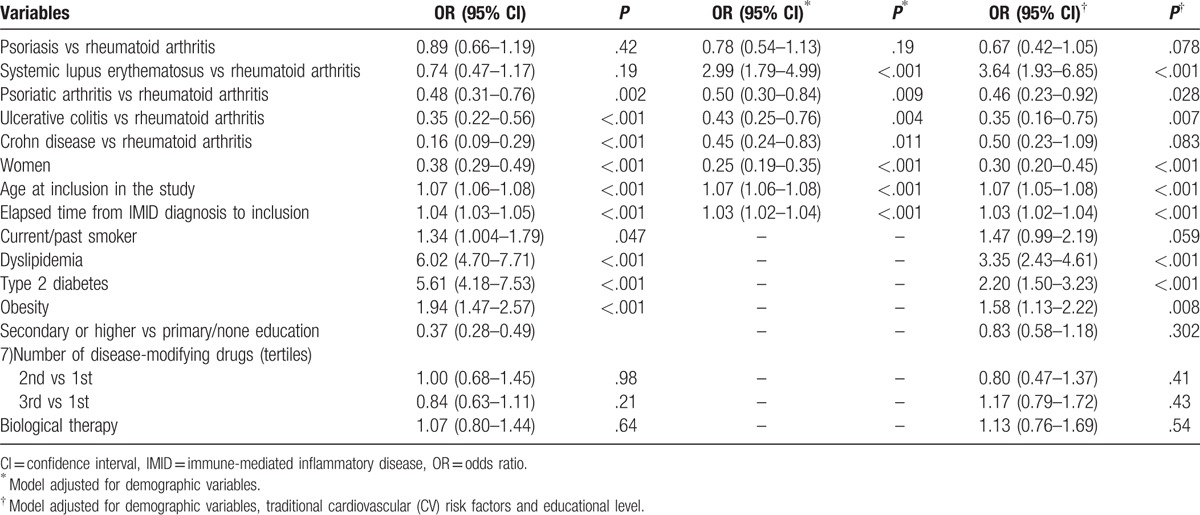
Figure 1.
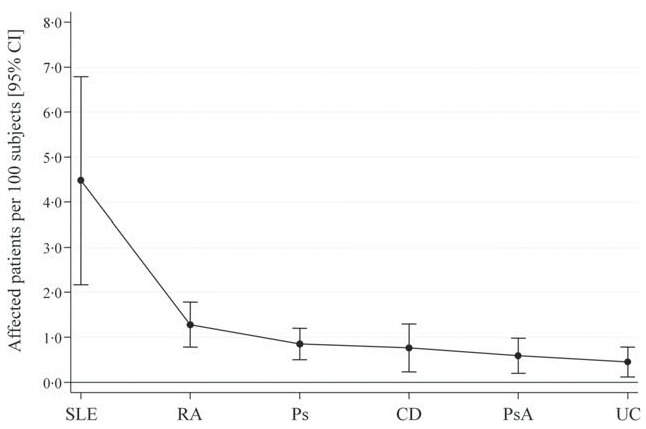
Adjusted prevalence of cardiovascular disease, with 95% confidence intervals, for each immune-mediated inflammatory disease. CD = Crohn disease, CI = confidence interval, Ps = psoriasis, PsA = psoriatic arthritis, RA = rheumatoid arthritis, SLE = systemic lupus erythematosus, UC = ulcerous colitis.
4. Discussion
In this study, we have analyzed, in 6 different IMIDs including almost 10,000 patients, the association of several demographic and clinical-related variables in the CVD risk. To our knowledge, this is the first time such an analysis has been conducted in patients affected by rheumatoid arthritis, psoriasis, psoriatic arthritis, systemic lupus erythematosus, ulcerative colitis, or Crohn disease, recruited in the same time frame, with similar follow-up times, using the same inclusion/exclusion criteria, with data collected using the same protocols and questionnaires. This particular setting allowed us to compare the CVD risk among different conditions and to perform a pooled analysis to identify common risk factors.
4.1. Risk factors of CVD in IMIDs
The analysis of CVD risk factors in different IMIDs was conducted in several previous studies (S Discussion and References). With regard to rheumatoid arthritis,[16–19] psoriatic arthritis,[20–22] psoriasis,[20,23] systemic lupus erythematosus,[24–26] and inflammatory bowel disease[27,28] similar findings were observed in our cohort. However, some differences have also been observed: in psoriasis and psoriatic arthritis, the severity of the skin disease was previously associated with CVD,[21,23] but no significant association was observed in our cohorts. Different definitions of severity were used, which may explain the different findings. In addition, in our psoriasis cohort, no association between younger age at disease onset and CVD was observed.[23]
In systemic lupus erythematosus, we described for the first time 2 new independent associations of CVD with vitiligo (which in turn has been associated with a lower prevalence of abdominal obesity and dyslipidemia)[29] and with a family history of autoimmune thyroiditis (which in turn has been associated with a higher risk of stroke).[30] In addition, comparing with a Spanish systemic lupus erythematosus registry,[31] we observed a lower prevalence of CVD and a lack of influence of traditional cardiovascular risk factors. However, surrogate markers of disease severity were independent risk factors in both studies. The fact that our patients came from systemic lupus erythematosus specialized units with a tighter management of both disease and CVD risk factors might explain these differences.
Finally, regarding inflammatory bowel disease, shorter disease duration was previously described as a risk factor for CVD in Crohn disease patients.[32] However, in our cohort, this influence was not observed.
4.2. Comparison of CVD risk among IMIDs
Several studies have compared the risk of CVD among different IMIDs, although none of them included the 6 we analyzed. Zöller et al[30] studied the risk of ischemic and hemorrhagic stroke in 32 different IMIDs (including psoriasis, rheumatoid arthritis, ulcerative colitis, Crohn disease, and systemic lupus erythematosus) using data from the entire Swedish population. An overall higher risk was observed for these 5 conditions compared with the general population, and although no direct comparisons were performed, systemic lupus erythematosus exhibited a higher standardized incidence rate, followed by rheumatoid arthritis and Crohn disease or psoriasis. Ulcerative colitis patients had the lowest risk for both ischemic and hemorrhagic stroke. In our study, although our dependent variable included all cardiovascular events, similar results were observed.
Regarding psoriasis and psoriatic arthritis, the latter was associated with a higher cardiovascular risk, regardless of whether the psoriatic arthritis patients were selected among those with psoriasis[20] or the psoriatic arthritis and psoriasis patients were selected separately in population-based studies.[23] When considering only our psoriasis cohort, similar results were observed: the presence of arthritis was independently associated with a higher risk of CVD. However, when we compared the psoriasis and the psoriatic arthritis cohorts, we observed the opposite result: a lower risk of CVD, albeit not significant, among the psoriatic arthritis cohort. To address this discrepancy, we compared the subjects from the psoriasis cohort with psoriatic arthritis, without psoriatic arthritis, and the patients from the psoriatic arthritis cohort (S8 and S9 Tables). In general, patients from the psoriasis cohort had a higher prevalence of traditional cardiovascular risk factors and higher skin disease severity, which could explain their higher prevalence of CVD. Taking into account that the patients from the psoriasis cohort were recruited from tertiary care outpatient clinics, it is likely that we selected patients with a more severe disease.
Few studies compared the risk of CVD between rheumatoid arthritis and psoriatic arthritis, observing a lower, although not significant, cardiovascular risk among the latter, regardless of whether the patients from both conditions were enrolled from different[22] or similar[33] settings. In our study, psoriatic arthritis patients had a significantly lower cardiovascular risk before and after adjusting for demographic and traditional risk factors. This observation may be related to the characteristics of the psoriatic arthritis cohort. A recent population-based study performed by Ogdie et al[34] showed that rheumatoid arthritis and psoriasis had similar standardized CVD hazard ratios, which were higher than that of psoriatic arthritis (although no direct comparison was performed).
Rheumatoid arthritis has also been compared with systemic lupus erythematosus. The latter was associated with a higher rate (compared with the general population) of first-time acute myocardial infarction than rheumatoid arthritis (although no direct comparison was performed).[35] In our sample, although rheumatoid arthritis showed a higher CVD prevalence in the bivariate analysis, after adjusting for age and sex, systemic lupus erythematosus showed a higher risk of CVD.
Regarding inflammatory bowel disease, similar normalized rates of ischemic heart disease and higher normalized rates of stroke were described in Crohn disease compared with ulcerative colitis, although no direct comparisons were performed.[27] In our sample, considering all CVDs, no significant differences were observed, although Crohn disease was associated with a higher standardized prevalence of CVD.
4.3. Limitations
There are several limitations to our study. First, because the study is cross-sectional, the directionality of the associations could not be determined. In addition, the presence of CVD, traditional cardiovascular risk factors, and disease-related variables was based either on the previous existence of a diagnosis of such conditions or manifestations, or on the indication by the patient of their existence during the clinical interview. We did not perform any complementary tests; therefore, the prevalence may be underestimated, especially for arterial hypertension, dyslipidemia, and type 2 diabetes.
Patients were recruited from rheumatology (rheumatoid arthritis, systemic lupus erythematosus, and psoriatic arthritis), dermatology (psoriasis), and gastroenterology (ulcerative colitis and Crohn disease) tertiary care outpatient clinics. Therefore, for some IMIDs, especially psoriasis, the generalization of our results to the whole population must be undertaken with caution because it is likely that only patients with a more severe disease were included. Moreover, patients were consecutively recruited, favoring the inclusion of subjects with a more severe disease, who tend to seek care more frequently. Because patients were recruited from practices throughout the country, these cohorts may be representative of the subpopulation of patients affected with severe disease in Spain.
No replication cohorts were included in this study, and therefore the newly described risk factors (such as vitiligo or a familiar history of autoimmune thyroiditis) need to be assessed in other cohorts.
This analysis was also limited by the inclusion of living patients, that is to say, subjects who survived long enough to be included in this study. Therefore, our sample may be biased toward patients with milder CVD and IMID. Moreover, the variables identified as associated with CVD may be predictors of survival following a CVD event rather than its occurrence. These conditions are important to consider when generalizing our results.
No direct disease activity measure, either at diagnosis or encompassing the whole disease duration, was available. However, treatment with disease-modifying drugs and biological therapy was used as a surrogate marker. Unfortunately, we lacked data regarding corticosteroid use throughout the disease.
Finally, there has been a delay between the inclusion of patients in this study and the presentation of the data used in this article. It is important to consider that due to the large amount of patients and centers that participated, it is expected logistic difficulties in the collection, ensemble, and quality control of the data that defer its use and dissemination.
5. Conclusions
We reported a direct comparison of CVD and cardiovascular risk factors prevalence among 6 IMIDs. We observed that different sets of demographic and clinical-related variables contribute to the risk of CVD in the different conditions studied. Furthermore, we compared the standardized CVD prevalence among those diseases, observing that systemic lupus erythematosus exhibited the highest prevalence, followed by rheumatoid arthritis and psoriasis. Our evidence provides a compelling argument to prioritize the institution of specific prevention programs in subjects affected with systemic lupus erythematosus, rheumatoid arthritis, and psoriasis to reduce the burden of CVD associated with these conditions.
Acknowledgments
The authors would like to thank all the physicians and health professionals who participated in the IMID Consortium: Pilar Nos (Hospital Universitari La Fe, Valencia, and CIBERehd, Instituto de Salud Carlos III, Madrid, Spain), Lluís Puig (Hospital de la Santa Creu i Sant Pau, Barcelona, and Universitat Autònoma de Barcelona, Barcelona, Spain), Isidoro González-Álvaro (Hospital Universitario de la Princesa and IIS-IP, Madrid, Spain), José A. Pinto-Tasende (Rheumatology Department, Complejo Hospitalario Universitario A Coruña, INIBIC, A Coruña, Spain), Ricardo Blanco (Hospital Universitario Marqués de Valdecilla and Facultad de Medicina. Universidad de Cantabria, Santander, Spain), Ana Gutiérrez Casbas (Gastroenterology Department, Hospital General Universitario de Alicante, Alicante, and CIBERehd, Instituto de Salud Carlos III, Madrid, Spain), Emilia Fernández (Hospital Universitario de Salamanca, Salamanca, Spain), Raimon Sanmartí (Hospital Clínic de Barcelona and IDIBAPS, Barcelona, Spain), Jordi Gratacós (Hospital Parc Taulí, Sabadell, Spain), Víctor Martínez Taboada (Hospital Universitario Marqués de Valdecilla and Facultad de Medicina. Universidad de Cantabria, Santander, Spain), Fernando Gomollón (Hospital Clínico Universitario, Zaragoza, and CIBERehd, Instituto de Salud Carlos III, Madrid, Spain), Esteban Daudén (Hospital Universitario de la Princesa and IIS-IP, Madrid, Spain), Joan Maymó (Hospital del Mar, Barcelona, Spain), Rubén Queiró (Hospital Universitario Central de Asturias, Asturias, Spain), Francisco Javier Lopez Longo (Hospital General Universitario Gregorio Marañón, Madrid, Spain), Esther García-Planella (Hospital de la Santa Creu i Sant Pau, Barcelona, Spain), Jose Luís Sánchez Carazo (Consorcio Hospital General Universitario de Valencia, Spain), Mercedes Alperi-López (Hospital Universitario Central de Asturias, Asturias, Spain), Carlos Montilla (Hospital Universitario de Salamanca, Salamanca, Spain), José Javier Pérez-Venegas (Hospital de Jerez de la Frontera, Cádiz, Spain), Juan L Mendoza (Gastroenterology Department, Hospital Clínico San Carlos, IDISSC, Madrid, Spain), José Luís López Estebaranz (Hospital Universitario Fundación Alcorcón, Madrid, Spain), Àlex Olivé (Hospital Universitari Germans Trias i Pujol, Badalona, Spain), Juan Carlos Torre-Alonso (Hospital Monte Naranco, Oviedo, Spain), Manuel Barreiro-de Acosta (Hospital Clínico Universitario, Santiago de Compostela, Spain), David Moreno Ramírez (Hospital Virgen de la Macarena, Sevilla, Spain), Héctor Coromines (Hospital Moisès Broggi, Barcelona, Spain), Santiago Muñoz-Fernández (Hospital Universitario Infanta Sofía, Madrid, Spain), José Luis Andreu (Hospital Universitario Puerta de Hierro, Madrid, Spain), Fernando Muñoz (Complejo Hospitalario de León, León, Spain), Pablo de la Cueva (Department of Dermatology, Hospital Universitario Infanta Leonor, Madrid, Spain), Alba Erra (Hospital Sant Rafael, Barcelona, Spain), Carlos M González (Hospital General Universitario Gregorio Marañón, Madrid, Spain), María Ángeles Aguirre-Zamorano (Hospital Universitario Reina Sofía, Instituto Maimónides de Investigación Biomédica de Córdoba (IMIBIC), Universidad de Córdoba, Córdoba, Spain), Maribel Vera (Hospital Universitario Puerta de Hierro, Madrid, Spain), Francisco Vanaclocha (Hospital Universitario Doce de Octubre, Madrid, Spain), Daniel Roig (Hospital Moisès Broggi, Barcelona, Spain), Paloma Vela (Rheumatology Department, Hospital General Universitario de Alicante, Alicante, Spain), Cristina Saro (Hospital de Cabueñes, Gijón, Spain), Enrique Herrera (Hospital Virgen de la Victoria, Málaga, Spain), Pedro Zarco (Hospital Universitario Fundación Alcorcón, Madrid, Spain), Joan M. Nolla (Hospital Universitari de Bellvitge, Barcelona, Spain), Maria Esteve (Hospital Universitari Mútua de Terrassa, Barcelona, and CIBERehd, Instituto de Salud Carlos III, Madrid, Spain), José Luis Marenco de la Fuente (Hospital del Valme, Sevilla, Spain), M. Jesus Garcia Villanueva (Hospital Universitario Ramón y Cajal, Madrid, Spain), José María Pego-Reigosa (Hospital do Meixoeiro, Vigo, and Grupo IRIDIS, IBI (Instituto de Investigación Biomédica de Vigo, Pontevedra y Orense), Spain), Laia Codó (LifeSciences, Barcelona Supercomputing Centre, National Institute of Bioinformatics, Barcelona, Spain), Josep Lluís Gelpí (LifeSciences, Barcelona Supercomputing Centre, National Institute of Bioinformatics, Barcelona, Spain), Andrés C. García-Montero (Banco Nacional de ADN Carlos III, University of Salamanca, Salamanca, Spain), Adrià Aterrido (Rheumatology Research Group, Vall d’Hebron Hospital Research Institute, Barcelona, Spain), María López-Lasanta (Rheumatology Research Group, Vall d’Hebron Hospital Research Institute, Barcelona, Spain), Arnald Alonso (Rheumatology Research Group, Vall d’Hebron Hospital Research Institute, Barcelona, Spain), Raül Tortosa (Rheumatology Research Group, Vall d’Hebron Hospital Research Institute, Barcelona, Spain).
Supplementary Material
Footnotes
Abbreviations: CI = confidence interval, CVD = cardiovascular disease, IMIDC = immune-mediated inflammatory disease consortium, IMID = immune-mediated inflammatory disease, VIF = variance inflation factor.
B.F.G., S.M., and L.R.R. share senior authorship on this work.
PSE-010000-2006-6: “Development of a diagnostic kit for immune-mediate inflammatory diseases” (Ministry of Science and Technology, Spain).
F.B. reported receiving consultancy fees from Gebro Pharma, and grant support from Bioiberica, MSD, Glaxo, UCB, Roche, Pfizer, Celltrion, Celgene, Amgen, Grunenthal, Sanofi, and Teded-Meiji; J.P.G. reported receiving speaker's, consultancy or grant support from MSD, Abbvie, Hospira, Kern Pharma, Takeda, Janssen, Pfizer, Ferring, Faes Farma, Shire Pharmaceuticals, Dr. Falk Pharma, Chiesi, Casen Fleet, Gebro Pharma, Otsuka Pharmaceutical, and Vifor Pharma; and the remaining authors have no conflicts of interest to disclose.
Supplemental digital content is available for this article.
References
- [1].Moran AE, Forouzanfar MH, Roth GA, et al. The global burden of ischemic heart disease in 1990 and 2010: the Global Burden of Disease 2010 study. Circulation 2014;129:1493–501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Hansson GK, Hermansson A. The immune system in atherosclerosis. Nat Immunol 2011;12:204–12. [DOI] [PubMed] [Google Scholar]
- [3].Sherer Y, Shoenfeld Y. Mechanisms of disease: atherosclerosis in autoimmune diseases. Nat Clin Pract Rheumatol 2006;2:99–106. [DOI] [PubMed] [Google Scholar]
- [4].Sattar N, McCarey DW, Capell H, et al. Explaining how “high-grade” systemic inflammation accelerates vascular risk in rheumatoid arthritis. Circulation 2003;108:2957–63. [DOI] [PubMed] [Google Scholar]
- [5].Prodanovich S, Shelling ML, Federman DG, et al. Cytokine milieu in psoriasis and cardiovascular disease may explain the epidemiological findings relating these 2 diseases. Arch Dermatol 2008;144:1518–9. [DOI] [PubMed] [Google Scholar]
- [6].Julià A, Domènech E, Chaparro M, et al. A genome-wide association study identifies a novel locus at 6q22.1 associated with ulcerative colitis. Hum Mol Genet 2014;23:6927–34. [DOI] [PubMed] [Google Scholar]
- [7].Richard-Miceli C, Criswell LA. Emerging patterns of genetic overlap across autoimmune disorders. Genome Med 2012;4:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Burisch J, Jess T, Martinato M, et al. The burden of inflammatory bowel disease in Europe. J Crohns Colitis 2013;7:322–37. [DOI] [PubMed] [Google Scholar]
- [9].Rosman Z, Shoenfeld Y, Zandman-Goddard G. Biologic therapy for autoimmune diseases: an update. BMC Med 2013;11:88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Shapira Y, Agmon-Levin N, Shoenfeld Y. Geoepidemiology of autoimmune rheumatic diseases. Nat Rev Rheumatol 2010;6:468–76. [DOI] [PubMed] [Google Scholar]
- [11].Arnett FC, Edworthy SM, Bloch DA, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 1988;31:315–24. [DOI] [PubMed] [Google Scholar]
- [12].Taylor W, Gladman D, Helliwell P, et al. Classification criteria for psoriatic arthritis: development of new criteria from a large international study. Arthritis Rheum 2006;54:2665–73. [DOI] [PubMed] [Google Scholar]
- [13].Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 1997;40:1725. [DOI] [PubMed] [Google Scholar]
- [14].Lennard-Jones JE. Classification of inflammatory bowel disease. Scand J Gastroenterol Suppl 1989;170:2–6. discussion 16–19. [DOI] [PubMed] [Google Scholar]
- [15].Burnham K, Anderson D. Model Selection and Multimodel Inference: A Practical Information—Theoretic Approach. 2nd edNew York: Springer; 2002. [Google Scholar]
- [16].Naranjo A, Sokka T, Descalzo MA, et al. Cardiovascular disease in patients with rheumatoid arthritis: results from the QUEST-RA study. Arthritis Res Ther 2008;10:R30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Amaya-Amaya J, Sarmiento-Monroy JC, Mantilla R-D, et al. Novel risk factors for cardiovascular disease in rheumatoid arthritis. Immunol Res 2013;56:267–86. [DOI] [PubMed] [Google Scholar]
- [18].Turesson C, McClelland RL, Christianson TJH, et al. Severe extra-articular disease manifestations are associated with an increased risk of first ever cardiovascular events in patients with rheumatoid arthritis. Ann Rheum Dis 2007;66:70–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Ajeganova S, Andersson MLE, Frostegård J, et al. Disease factors in early rheumatoid arthritis are associated with differential risks for cardiovascular events and mortality depending on age at onset: a 10-year observational cohort study. J Rheumatol 2013;40:1958–66. [DOI] [PubMed] [Google Scholar]
- [20].Li W-Q, Han J-L, Manson JE, et al. Psoriasis and risk of nonfatal cardiovascular disease in U.S. women: a cohort study. Br J Dermatol 2012;166:811–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Gladman DD, Ang M, Su L, et al. Cardiovascular morbidity in psoriatic arthritis. Ann Rheum Dis 2009;68:1131–5. [DOI] [PubMed] [Google Scholar]
- [22].Jamnitski A, Visman IM, Peters MJL, et al. Prevalence of cardiovascular diseases in psoriatic arthritis resembles that of rheumatoid arthritis. Ann Rheum Dis 2011;70:875–6. [DOI] [PubMed] [Google Scholar]
- [23].Ahlehoff O, Gislason GH, Charlot M, et al. Psoriasis is associated with clinically significant cardiovascular risk: a Danish nationwide cohort study. J Intern Med 2011;270:147–57. [DOI] [PubMed] [Google Scholar]
- [24].Bertoli AM, Vilá LM, Alarcón GS, et al. Factors associated with arterial vascular events in PROFILE: a Multiethnic Lupus Cohort. Lupus 2009;18:958–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Toloza SMA, Uribe AG, McGwin G, et al. Systemic lupus erythematosus in a multiethnic US cohort (LUMINA). XXIII. Baseline predictors of vascular events. Arthritis Rheum 2004;50:3947–57. [DOI] [PubMed] [Google Scholar]
- [26].Pons-Estel GJ, González LA, Zhang J, et al. Predictors of cardiovascular damage in patients with systemic lupus erythematosus: data from LUMINA (LXVIII), a multiethnic US cohort. Rheumatology (Oxford) 2009;48:817–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Bernstein CN, Wajda A, Blanchard JF. The incidence of arterial thromboembolic diseases in inflammatory bowel disease: a population-based study. Clin Gastroenterol Hepatol 2008;6:41–5. [DOI] [PubMed] [Google Scholar]
- [28].Kristensen SL, Ahlehoff O, Lindhardsen J, et al. Disease activity in inflammatory bowel disease is associated with increased risk of myocardial infarction, stroke and cardiovascular death—a Danish nationwide cohort study. PLoS One 2013;8:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Rodríguez-Martín M, de Paz NM, Mehtani P, et al. Patients with vitiligo present fewer cardiovascular risk factors: results from a case-control study. J Eur Acad Dermatol Venereol 2013;27:124–5. [DOI] [PubMed] [Google Scholar]
- [30].Zöller B, Li X, Sundquist J, et al. Risk of subsequent ischemic and hemorrhagic stroke in patients hospitalized for immune-mediated diseases: a nationwide follow-up study from Sweden. BMC Neurol 2012;12:41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Fernández-Nebro A, Rúa-Figueroa Í, López-Longo FJ, et al. Cardiovascular events in systemic lupus erythematosus: a nationwide study in Spain from the RELESSER registry. Medicine (Baltimore) 2015;94:e1183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Osterman MT, Yang Y-X, Brensinger C, et al. No increased risk of myocardial infarction among patients with ulcerative colitis or Crohn's disease. Clin Gastroenterol Hepatol 2011;9:875–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Han C, Robinson DW, Hackett MV, et al. Cardiovascular disease and risk factors in patients with rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis. J Rheumatol 2006;33:2167–72. [PubMed] [Google Scholar]
- [34].Ogdie A, Yu Y, Haynes K, et al. Risk of major cardiovascular events in patients with psoriatic arthritis, psoriasis and rheumatoid arthritis: a population-based cohort study. Ann Rheum Dis 2014;74:326–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Fischer LM, Schlienger RG, Matter C, et al. Effect of rheumatoid arthritis or systemic lupus erythematosus on the risk of first-time acute myocardial infarction. Am J Cardiol 2004;93:198–200. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.