

Abstract
The aim of this study was to introduce a novel method of mesiodens extraction using a vascularized pedicled bone flap by piezosurgery and to compare the differences between a computer-aided design surgical guide template and free-hand operation.
A total of 8 patients with mesiodens, 4 with a surgical guide (group I), and 4 without it (group II) were included in the study. The surgical design was to construct a trapdoor pedicle on the superior mucoperiosteal attachment with application of piezosurgery. The bone lid was repositioned after mesiodens extraction. Group I patients underwent surgeries based on the preoperative planning with surgical guide templates, while group II patients underwent free-hand operation. The outcome variables were success rate, intraoperative time, anterior nasal spine (ANS) position, changes of nasolabial angle (NLA), and major complications. Data from the 2 groups were compared by SPSS 17.0, using Wilcoxon test.
The operative time was significantly shorter in group I patients. All the mesiodentes were extracted successfully and no obvious differences of preoperative and postoperative ANS position and NLA value were found in both groups. The patients were all recovered uneventfully.
Surgical guide templates can enhance clinical accuracy and reduce operative time by facilitating accurate osteotomies.
Keywords: mesiodens, pedicled bone flap, piezosurgery, surgical template
1. Introduction
Hyperdontia or supernumerary teeth are those that exceed the normal dental formula and can be found in almost any region of the dental arch, which are encountered more frequently in maxilla than in mandible, and anteriorly than posteriorly, with a predilection for the maxillary incisor region.[1–4] Mesiodens, defined as a supernumerary tooth located between the 2 central incisors, is the most commonly impacted tooth and frequently found in the maxilla and in the permanent dentition with a prevalence of 0.15% to 1.9% in the general population.[5–7]
Supernumerary teeth can may result in crowding, diastema, cyst formation, resorption, displacement, or rotation of adjacent teeth, or it may delay or prevent permanent teeth eruption.[8] When a supernumerary tooth causes symptoms or clinical signs, or disturbs orthodontic treatment, it becomes necessary to extract the tooth. High-situated mesiodens in premaxilla is comparatively deep and adjacent to anatomical structures like apex of permanent teeth, nasal cavity and anterior nasal spine (ANS). Conventional approach for the removal of a deeply impacted mesiodens is accompanied with complications such as permanent teeth injury, supernumerary tooth entering nasal cavity, or maxillary deformity because of mass bone removal.[1,6] Moreover, ANS plays an important role as a bony structure supporting the columella and nasal tip while maintaining the individual nasolabial angle (NLA).[9] Piezosurgery, as a promising, meticulous and soft tissue-sparing system, has proven to be an effective tool for cutting bone without encountering necrosis from overheating and damaging soft tissues. Its atraumatic manipulation of tissues and precision in surgery are widely accepted by oral and maxillofacial surgeons.[10] Thus, we modified the conventional approach under the help of piezosurgery, which used a bone flap with mucoperiosteal pedicle—“trapdoor” method—to restore premaxilla integrity.
The techniques providing three-dimensional (3D) digital information using computed tomography (CT). With the advances in computer-aided design/computer-assisted manufacturing (CAD/CAM) technique, the surgical guide template has drawn more and more attention in the clinic, as it can be designed to fit an individual's anatomy and assist in transferring the treatment plan to the surgical procedure and simplify the surgical steps.[11,12] Therefore, it would decrease the operation time and improve the accuracy of osteotomy.
In the present study, we aimed to evaluate the operation time and effectiveness of the trapdoor method, comparing surgical template with free-hand operation and to analyze the advantages of the method and the surgical template.
2. Materials and methods
2.1. Study design
A retrospective study was designed and implemented which included 8 patients with supernumerary teeth in the premaxilla at our department from January 2012 to December 2015. The study was approved by the Ethics Committee of Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine. All the patients provided signed informed consent.
All the patients have been treated with mesiodentes extraction using “trapdoor” method with or without a surgical template and all the surgeries were performed by same senior surgeon. Patients with any of the following were excluded from the study: acute infections; systemic diseases such as diabetes, blood dyscrasias; history of alcoholism, drug abuse or heavy smoking; and serious psychiatric disease.
2.2. Clinical procedure
The patients’ preoperative CT or cone beam CT (CBCT) scans were stored on a disc as Digital Imaging Communications in Medicine (DICOM) files and then 3D reconstruction were performed using Mimics, version 18.0 (Materialise, Leuven, Belgium), software. The preoperative planning included verifying the position of supernumerary teeth, determining osteotomy lines and avoiding vital anatomical structures. For patients in group I, optical scanning on tooth plaster models was performed to make 3D digital models after image examination, being registered with CT or CBCT to form 3D reconstructive jaw models. Therefore, the characteristics of teeth, especially the occlusal surfaces, could be clearly presented.[13] The surgical guide template was designed according to the image registration and preoperative planning, which used upper teeth as a retainer and demonstrated accurate directions of osteotomy lines, then output in STL (Standard Template Library) format. The STL data were input into rapid prototyping (RP) software (Geomagic, version 10.0; Geomagic, Research Triangle Park, NC) to make the surgical guide template (Fig. 1). Surgeries based on the guide template were performed in group I patients. Group II patients underwent surgeries without guide template, based on preoperative planning only and by the same surgeon.
Figure 1.
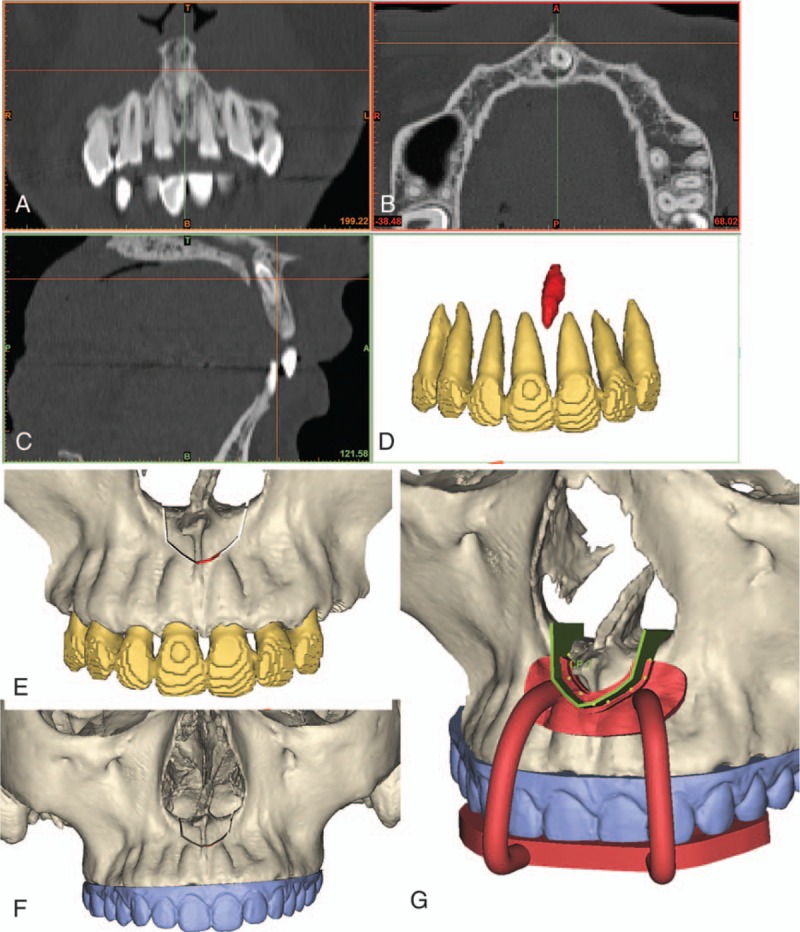
Surgical guide template design. (A–D) Computed tomography scans and three-dimensional construction of the mesiodens and permanent teeth; (E) preoperative osteotomy design; (F) image registration tooth plaster model; (G) digital design of surgical guide template.
2.3. Surgical techniques
Patients underwent local infiltration in labial and palatal mucosa of upper anterior teeth and submucosa of nasal bottom with 2% lidocaine. The surgical design was to make a trapezoid or a pentagon trapdoor using 3 or 4 consecutive cuts, fracture the upper margin and lift the bone lid upward. An incision was made in the upper vestibule down to the periosteum. The osteotomy sites on the inferior, medial, and lateral sides of the bone lid were exposed subperiosteally, whereas the mucoperiosteal attachments on the superior and central areas of the bone lid were remained. The osteotomy lines were made on the buccal surface of premaxilla using piezosurgery with or without a surgical guide template (Fig. 2A and D). Afterward, following fracture of the upper bone margin, the bone flap pedicle on the mucoperiosteum was lifted upward, exposing the impacted teeth (Fig. 2B). The supernumerary tooth was gently removed from its socket by an elevator. Then the bone flap was repositioned (Fig. 2C) and the mucosal incision was sutured using 4 to 0 nylon suture.
Figure 2.
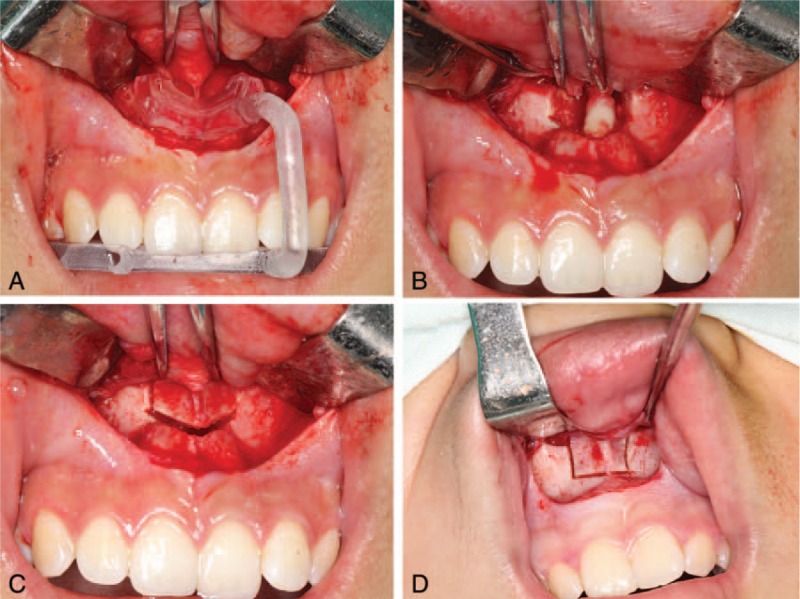
Intraoperative imaging. (A) Surgical guide template positioning; (B) mesiodens exposure after lifting the bone lid upward; (C) pedicled bone flap repositioning; (D) osteotomy lines cut by free-hand manipulation.
All the patients were prescribed an oral medication of 0.25 g amoxicillin 4 times a day for 3 days, with a 0.02% compound chlorhexidine solution as mouth wash. One week following extraction, the stitches were removed.
2.4. Outcome variables
The predictor variable was computer-designed surgical guide template (group I) compared with free-hand operation (group II) for premaxillary supernumerary teeth extraction. The outcome variables were success rate, intraoperative time (from the first incision to the last suture), ANS position, changes of NLA value, and major complications (injury of the root of permanent teeth, nerve damage, supernumerary teeth entering nasal cavity, etc.).
2.4.1. Postoperative assessments
Four parameters were applied to assess the clinical efficacy of using digital templates to guide supernumerary tooth extraction. The first referred to applicability: Could the template be smoothly positioned and fitted to the bone? The second involved accuracy: Could the supernumerary teeth be extracted successfully, without changing the position of ANS? The third involved expedience: Would the surgical time be cut down by use of template? The fourth related to safety: Would the template sufficiently protect the vital anatomical structures?
The DICOM data from postoperative CT or CBCT was input into Mimics 18.0 software and a 3D maxilla was then reconstructed in STL format. Based on specific markers, image registration was carried out between postoperative STL data and preoperative data. The markers included bilateral infraorbital points (OrL, OrR), porions (PoL, PoR), nasion (N), and sella (S). The horizontal plane (HP) was determined by OrL, OrR, PoL, and PoR; the medial sagittal plane (SP) was perpendicular to HP, passing through N and S; and the coronal plane (CP) was perpendicular to both HP and SP through S.
The position of ANS was evaluated by distances from preoperative and postoperative acanthion to HP, SP, and CP (Fig. 3). The NLA values were measured on the medial sagittal scans of preoperative and postoperative CT or CBCT.
Figure 3.
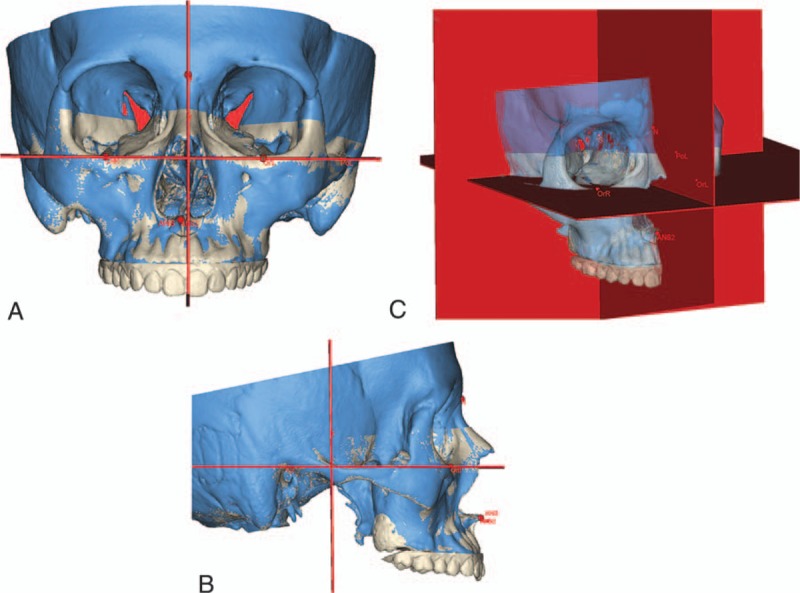
Three-dimensional measurement and image registration of preoperative (white) and postoperative (blue) computed tomography scans. (A) Frontal view; (B) sagittal view; (C) horizontal plane, sagittal plane, and coronal plane defined by the markers. ANS = preoperative anterior nasalspine, ANS2 = postoperative anterior nasalspine, S = sella, N = nasion, OrL = orbitale left, OrR = orbitale right, PoL = porion left, PoR = porion right.
All the image registrations and measurements were performed separately by 2 attending doctors who were blind to the surgical methods, and remeasured at a 2-week interval. Intraexaminer and interexaminer reliability were estimated. The mean value of measurements was used to perform statistical analysis.
2.5. Statistical analysis
All the data were analyzed by Statistical Package for Social Sciences software package, version 17.0 (SPSS, Chicago, IL). A P value of less than .05 was accepted as statistically significant.
The operative time of the 2 groups was compared using Wilcoxon rank-sum test. ANS positions and NLA values before and after surgery were analyzed by Wilcoxon signed rank-sum test. Intragroup and intergroup differences were analyzed using intraclass correlation coefficients (ICCs).
3. Results
Six out of the 8 patients were females and 2 were males. The mean of their ages was 19.13 years (range 14–28), with a mean follow-up period of 13.25 months (range 6–21). Of the 8 patients, 4 underwent surgeries using templates to guide osteotomy and 4 had free-hand surgeries.
During the operations, all guide templates were positioned smoothly and fitted to the bone surfaces. The templates precisely transferred the treatment plan to the surgical procedure, and all the supernumerary teeth in group I were extracted uneventfully. Although the supernumerary teeth were removed successfully in group II as well, there was 1 case that needed extra osteotomy due to insufficient exposure of the tooth after lifting the pedicled bone flap.
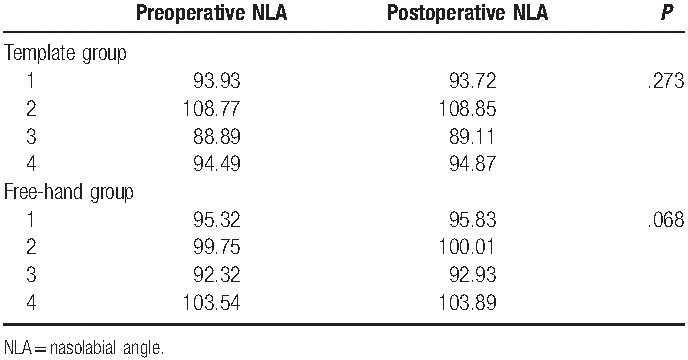
Wilcoxon rank-sum test showed that the operative time of group I was significantly shorter than group II (P = .021) (Table 1). ICCs for interobserver agreement was ranged between 0.88 and 0.90, and intraobserver agreement was ranged between 0.95 and 0.98, showing excellent reliabilities. There were no obvious differences of preoperative and postoperative ANS position and NLA value in both groups (Tables 2 and 3).
Table 1.
Comparison of operative time of the 2 groups.

Table 2.
Preoperative and postoperative positions of ANS.
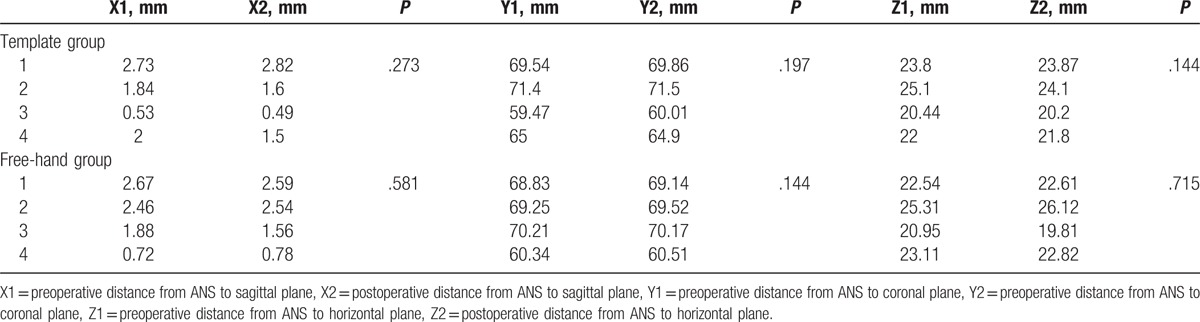
Table 3.
Preoperative and postoperative values of NLA.
Clinical examinations showed that the upper incisors and molars were in good condition, no crown surface discoloration, no loss of pulp vitality and no loosen teeth. Image examination revealed morphologically normal ANS, no adjacent roots resorption (Fig. 4).
Figure 4.
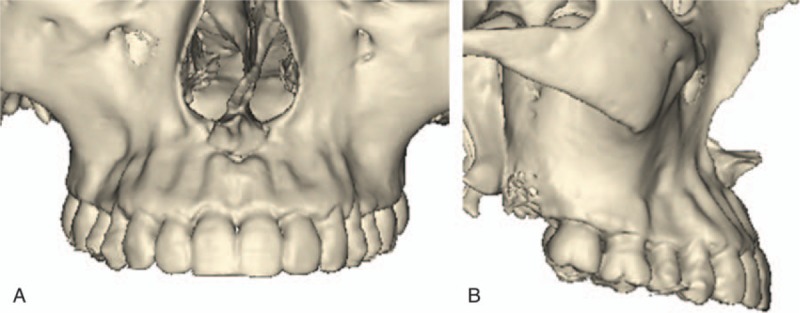
Postoperative three-dimensional reconstruction of computed tomography imaging, showing normal morphology of preoperative anterior nasalspine and good healing of the bone flap.
4. Discussion
For a deeply or high-suited mesiodens, conventional labial approach requires excessive bone removal. Besides, traditional rotating burs are not selective for bone cutting and thus can cause significant harm to the surrounding soft tissues. Nowadays, with the development of CAD/CAM technique, the surgical guide template has been widely used in the clinic. In this study, with assistance of piezosurgery, we performed the mesiodens extraction using vascularized pedicled bone flap, namely trapdoor method, as a minimally invasive and safe approach to maintain the normal contour of premaxilla and reduce bone loss. Also, we compared effects of surgical guide templates with free-hand surgeries. The results revealed that the contour of ANS was well preserved by trapdoor method in both groups and surgical guide template shortens the operative time and minimize invasiveness.
To accurately locate supernumerary teeth and their relationship with neighboring structures, imaging examinations are of great importance. Traditionally, 2-dimensional radiographs only show the location of impacted teeth in general, but is impossible to determine their exact relationship with surrounding structures due to superposition and magnification or reduction in size.[14–16] While spiral CT and CBCT can provide the ability to perform 3D reconstructions and clearly manifest the intraosseous location, inclination, and morphology of impacted supernumerary teeth, as well as their distances from adjacent roots, teeth, and the cortical bone, avoiding superposition of bony and dental structures, which helps in making surgical approaches.[16–19] Therefore, we suggest that for a deeply impacted supernumerary tooth in the anterior maxilla, all adjacent structures should be assessed by 3D imaging examination preoperatively while determining the optimal osteotomy.
Nevertheless, CT or CBCT is less accurate for reflecting the specific features of the teeth compared with the plaster model, especially characteristics of occlusal surfaces. The teeth outline on the imaging scans are usually not clear and often magnified with some artifacts. Besides, it can often be impossible to segment the upper and lower teeth due to the compact occlusal bite. Thus, a combination of the data using a laser scan of the teeth would significantly improve the accuracy of the surgical guide template, leading to smoothly positioning, and excellent stability intraoperatively.
As a part of the piriform aperture, the ANS plays an important role as a bony structure supporting the columella and nasal tip while maintaining the individual NLA. In cases where the underlying bony support is atrophied, widening of nose width and collapsing of nasal tip could be secondarily manifested.[9] In this article, the mesiodens in premaxilla was under the ANS whose morphology would be damaged when removing the mass bone quantity, while less bone quantity reduction may not expose the tooth. Using the trapdoor method could not only preserve the appearance of ANS, but also could assure the vascularity and viability of the bony window, which promoted quick recovery and decrease possibility of infection due to blood supply.[20] Operation of the superior margin fracture was controllable and the bone lid lifting was easy because of strong attachment of the mucoperiosteum.
Because of the close relationship between the mesiodens and lateral incisors, the transversal osteotomy line should place 2 mm away from the apexes of upper incisors to protect the root of adjacent teeth. Moreover, owing to exact repositioning of the bone flap, extra fixation was not required.
With CAD/CAM technique, the ideal osteotomy lines could be simulated and determined accurately before surgery. By fabricating digital templates, the design could be transferred into the operation accurately.[21] In the present study, we evaluated the efficiencies of mesiodens extraction by preoperative CAD planning with and without a surgical guide template. The results revealed that both groups could obtain satisfactory clinical effect. But the use of surgical template decreased operative time significantly. The reasons might be that the template guaranteed precise osteotomy and sufficient exposure of the mesiodens, while free-hand manipulation might need multiple osteotomies or tooth splitting caused by inaccurate trapdoor position.
There are several advantages of surgical guide template. The first is safety. Despite no significant structural damage in both groups in the present study, sufficient preoperative planning and application of guide template can ensure the safety and reduce the incidence of complications, especially for young surgeons. A second advantage is high efficiency. Surgical template simplifies the operation steps, helps the surgeon reduce complications and unnecessary osteotomy, resulting in less operative time. Although only 4 minutes was saved for the senior surgeon, it would be much more time saving for young and inexperienced surgeons. Another advantage is the minimal bone loss. The pedicled bone flap can be repositioned easily owing to mucoperiosteal attachment. But if extra osteotomy is required, the removed bone plate would be difficult to reposition. Thus, the use of surgical guide template can avoid extra osteotomy to preserve alveolar bone as much as possible. However, the use of template might add extra expense and specific equipment, which limits its expansion. But it is still worth using for deeply embedded tooth extraction.
There were some limitations to this study. First, clinical symptoms like pain and swelling were not investigated due to the research type. Next, the sample size was small and the test power was not performed. Besides, further research may be warranted to compare the efficiency of piezosurgery and chisel.
5. Conclusion
In conclusion, digital surgical templates can enhance clinical accuracy and reduce operative time by facilitating accurate osteotomies. Trapdoor method can preserve anatomic form of ANS and reduce bone quantity loss. The method presented in our study has a broad application prospect for clinical application.
Footnotes
Abbreviations: 3D = three-dimensional, ANS = anterior nasal spine, CAD/CAM = computer-aided design/computer-assisted manufacturing, CBCT = cone beam CT, CT = computed tomography, DICOM = Digital Imaging Communications in Medicine, NLA = nasolabial angle.
YKH and QYX have contributed equally to the article and share first authorship.
Author contributions: YKH and QYX participated in the study design, acquisition of data, analysis and interpretation of data, drafting, and revising the manuscript for important intellectual content. CY conceptualized and designed the study, critically reviewed and revised the manuscript, and approved the final manuscript as submitted. GZX critically reviewed and revised the manuscript, also helped with statistical analysis. JG participated in the acquisition of data and revising the manuscript critically. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
The study was supported by Science and Technology Commission of Shanghai Funding/support: Municipality Science Research Project (14DZ2294300), and Shanghai Summit & Plateau Disciplines.
The authors have no conflicts of interest to disclose.
References
- [1].Thimmegowda U, Kajapuram P, Prasanna M, et al. Interdisciplinary management of impacted supernumerary tooth between roots of permanent teeth—a management dilemma? J Clin Diagn Res 2016;10:ZJ05–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Russell KA, Folwarczna MA. Mesiodens—diagnosis and management of a common supernumerary tooth. J Can Dent Assoc 2003;69:362–6. [PubMed] [Google Scholar]
- [3].Mali S, Karjodkar FR, Sontakke S, et al. Supernumerary teeth in non-syndromic patients. Imaging Sci Dent 2012;42:41–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Hyun HK, Lee SJ, Ahn BD, et al. Nonsyndromic multiple mandibular supernumerary premolars. J Oral Maxillofac Surg 2008;66:1366–9. [DOI] [PubMed] [Google Scholar]
- [5].Van Buggenhout G, Bailleul-Forestier I. Mesiodens. Eur J Med Genet 2008;51:178–81. [DOI] [PubMed] [Google Scholar]
- [6].Mossaz J, Kloukos D, Pandis N, et al. Morphologic characteristics, location, and associated complications of maxillary and mandibular supernumerary teeth as evaluated using cone beam computed tomography. Eur J Orthod 2014;36:708–18. [DOI] [PubMed] [Google Scholar]
- [7].Sukegawa S, Kanno T, Kawakami K, et al. Use of a piezosurgery technique to remove a deeply impacted supernumerary tooth in the anterior maxilla. Case Rep Dent 2015;2015:974169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Mason C, Azam N, Holt RD, et al. A retrospective study of unerupted maxillary incisors associated with supernumerary teeth. Br J Oral Maxillofac Surg 2000;38:62–5. [DOI] [PubMed] [Google Scholar]
- [9].Cho YS, Hwang KG, Park CJ. Postoperative effects of anterior nasal spine bone harvesting on overall nasal shape. Clin Oral Implants Res 2013;24:618–22. [DOI] [PubMed] [Google Scholar]
- [10].Pereira CC, Gealh WC, Meorin-Nogueira L, et al. Piezosurgery applied to implant dentistry: clinical and biological aspects. J Oral Implantol 2014;40:401–8. [DOI] [PubMed] [Google Scholar]
- [11].Zhang Y, Wen L, Zhang J, et al. Three-dimensional printing and computer navigation assisted hemipelvectomy for en bloc resection of osteochondroma: a case report. Medicine (Baltimore) 2017;96:e6414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Hultin M, Svensson KG, Trulsson M. Clinical advantages of computer-guided implant placement: a systematic review. Clin Oral Implants Res 2012;23:124–35. [DOI] [PubMed] [Google Scholar]
- [13].Lin Z, He B, Chen J, et al. Manufacture method and clinical application of minimally invasive dental implant guide template based on registration technology. Hua Xi Kou Qiang Yi Xue Za Zhi 2012;30:402–6. 410. [PubMed] [Google Scholar]
- [14].Sawamura T, Minowa K, Nakamura M. Impacted teeth in the maxilla: usefulness of 3D Dental-CT for preoperative evaluation. Eur J Radiol 2003;47:221–6. [DOI] [PubMed] [Google Scholar]
- [15].Chaushu S, Chaushu G, Becker A. The role of digital volume tomography in the imaging of impacted teeth. World J Orthod 2004;5:120–32. [PubMed] [Google Scholar]
- [16].Kim KD, Ruprecht A, Jeon KJ, et al. Personal computer-based three-dimensional computed tomographic images of the teeth for evaluating supernumerary or ectopically impacted teeth. Angle Orthod 2003;73:614–21. [DOI] [PubMed] [Google Scholar]
- [17].Schulze D, Heiland M, Thurmann H, et al. Radiation exposure during midfacial imaging using 4- and 16-slice computed tomography, cone beam computed tomography systems and conventional radiography. Dentomaxillofac Radiol 2004;33:83–6. [DOI] [PubMed] [Google Scholar]
- [18].Liu DG, Zhang WL, Zhang ZY, et al. Three-dimensional evaluations of supernumerary teeth using cone-beam computed tomography for 487 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103:403–11. [DOI] [PubMed] [Google Scholar]
- [19].Nakajima A, Sameshima GT, Arai Y, et al. Two- and three-dimensional orthodontic imaging using limited cone beam-computed tomography. Angle Orthod 2005;75:895–903. [DOI] [PubMed] [Google Scholar]
- [20].Lazaridis N, Tilaveridis I, Venetis G, et al. Maxillary sinus osteoplasty with vascularized pedicled bone flap. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:828–32. [DOI] [PubMed] [Google Scholar]
- [21].Shen P, Zhao J, Fan L, et al. Accuracy evaluation of computer-designed surgical guide template in oral implantology. J Craniomaxillofac Surg 2015;43:2189–94. [DOI] [PubMed] [Google Scholar]