

Abstract
Background:
A case report of Hashimoto's thyroiditis-associated ophthalmopathy that masqueraded as double elevator palsy in 1 eye.
Case presentation:
A 54-year-old woman presented to our strabismus clinic with diplopia for 1 year. She was diagnosed with double elevator palsy in the left eye. The forced duction test yielded positive findings for the inferior rectus of the left eye; hence, computed tomography of the orbit and thyroid-associated blood tests were performed; surprisingly, the thyroid function test results were consistent with hypothyroidism and the antibody results such as antithyroglobulin and antithyroid peroxidase were markedly elevated, and the patient was diagnosed with Hashimoto's thyroiditis and treated with corticosteroids. Unfortunately, her diplopia was not relieved with medical management. Subsequently, a 9-mm left inferior rectus recession was performed.
Conclusion:
Clinicians should be aware of the atypical signs of Hashimoto's thyroiditis for its proper diagnosis and management.
Keywords: Hashimoto's thyroiditis, paralytic strabismus, thyroid-associated ophthalmopathy
1. Introduction
Acquired strabismus is usually attributed to thyroid-associated ophthalmopathy (TAO), cranial nerve palsies (cranial nerves III, IV, and VI), orbital fractures, intracranial bleeding or infections, and intracranial/intraorbital/intraocular masses. TAO is characterized by autoimmune inflammation of the extraocular muscles, surrounding connective tissue, and adipose tissue. Typical signs include upper eyelid retraction (UER), proptosis, periorbital edema, and eyeball motility defects. It is commonly related to Graves’ disease, but rarely to Hashimoto's thyroiditis or a euthyroid state. Hashimoto's thyroiditis is a common autoimmune disease that usually presents with a spectrum of altered thyroid function. It is characterized by a diffuse goiter, lymphocytic infiltration, and autoantibodies to thyroglobulin and thyroid peroxidase. We report a case of Hashimoto's thyroiditis-associated ophthalmopathy that masqueraded as a unilateral double elevator palsy (DEP) at its initial presentation.
2. Case description
A 54-year-old nondiabetic woman was referred to our hospital with a 1-year history of severe diplopia. The preliminary diagnosis was a DEP in the left eye. She had previously used a pair of pressing triple prisms to partially correct her diplopia for 6 months. Her past medical history was unremarkable. She did not have chemosis, conjunctival hyperemia, proptosis, or the typical symptoms of hypothyreosis or hyperthyreosis since the onset of symptoms. On ophthalmologic examination, her visual acuity and intraocular pressures were normal; she had a limitation of upward gaze in her left eye (Fig. 1). The degree of hypotropia in the primary position of the eye was 40 prism diopters, and the forced duction test (FDT) was positive for the inferior rectus (IR) of the left eye. Subsequently, the patient underwent computed tomography (CT) of the orbit and thyroid-associated blood tests. The belly of the left IR showed slight enlargement on the CT orbit scans (Fig. 2). Her blood analysis revealed the following: free triiodothyronine (FT3), 2.67 pg/mL (normal range, 1.8–4.6 pg/mL); free thyroxine (FT4), 11.84 pmol/L (normal range, 12–22 pmol/L); thyroid-stimulating hormone (TSH), 5.020 μIU/mL (normal range, 0.27–4.2 μIU/mL); antithyroglobulin (A-TG), 1785.00 IU/mL (normal range, 0–115 IU/mL); and antithyroid peroxidase (A-TPO), more than 600.00 IU/mL (normal range, 0–34 IU/mL). Additionally, the patient's thyrotropin receptor antibody (TRAb) levels were 12 IU/mL (normal range, 0.01–30 IU/mL). Ultrasonography showed a thyroid gland with heterogeneous echogenicity and a nodule in the left lobe (Fig. 3). The patient was referred for an endocrinology consultation, following which she was diagnosed with Hashimoto's thyroiditis. Subsequently, we rectified the preliminary ophthalmic diagnosis of DEP to TAO based on her history and clinical features and findings. She was treated with 80 mg of prednisolone daily for a week. However, her diplopia failed to improve and a left IR recession (9 mm) was performed (Fig. 4).
Figure 1.
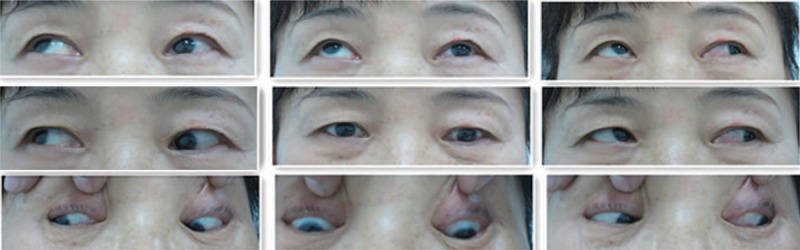
Nine positions of ocular movement examination. The left eye was lower than the right eye at primary position, and there was a limitation of upward gaze in her left eye.
Figure 2.
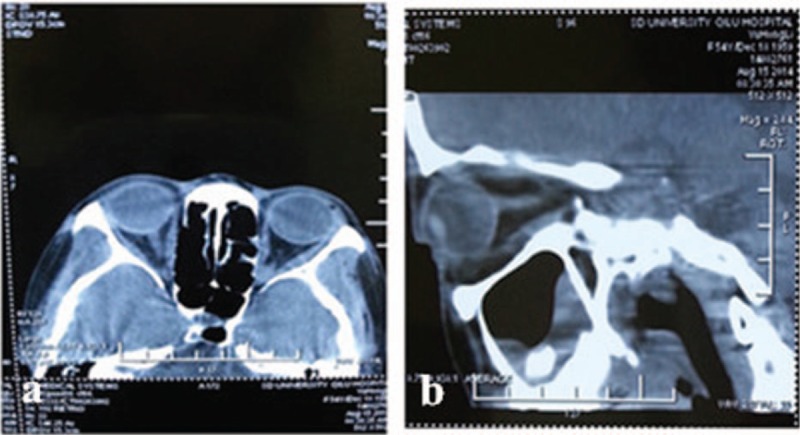
The computed tomography scan of the left orbit. There was slight enlargement of the left inferior rectus belly shown in b.
Figure 3.

Ultrasonography of the thyroid gland. A heterogeneous echogenicity in the left lobe was detected, which implied the possibility of Hashimoto's thyroiditis.
Figure 4.

Nine positions of ocular movement after the surgery. The vertical deviation and the limitation of upward gaze were improved.
3. Discussion
TAO is one of the most common causes of adult ocular myopathy, which often occurs in patients with Graves’ disease, but rarely in patients with Hashimoto's thyroiditis. We confirmed the diagnosis for the patient in this report according to her clinical findings such as slight enlargement of the left inferior rectus belly (shown in Fig. 2), hypothyroidism, negtive TRAb, and positive A-TG and A-TPO results; besides, the effectiveness of simple 9 mm recession of the left inferior rectus is another indirect evidence, since this kind of surgery is usually not enough to correct a vertical deviation of 40 prism diopters which is not caused by TAO. The first study on the prevalence of ophthalmopathy in Hashimoto's thyroiditis was conducted by Tjiang et al,[1] who reported that eye signs were present in 34% of the 91 patients with Hashimoto's thyroiditis included in the study, and symptoms such as UER, chemosis, conjunctival injection, proptosis, or periorbital swelling were observed in one-third of all the subjects with eye signs. Kan et al[2] updated the available data with a larger number of patients (n = 110) and a comparison with healthy subjects. They showed that the eye signs were present in 22.7% of patients with Hashimoto's thyroiditis, and 11.8% had UER, 6.4% had proptosis, and 5.5% had ocular myopathy. Hashimoto's thyroiditis is not usually associated with overt ophthalmopathy, but extraocular muscle involvement is common and has been reported in other studies.[3–5] The present case is quite similar to the one reported by Hiraga et al.[3] Both patients had isolated extraocular muscle involvement and had no other eye signs; however, the patient in the report by Hiraga et al was sensitive to corticosteroid treatment, whereas ours was not. Similarly, the 2 patients reported by Yoshihara et al[5] were also sensitive to corticosteroid treatment, although they had much more severe orbitopathy and involvement of more than 1 extraocular muscle. Since the FDT was positive for the left IR and the muscle enlargement was not as evident as that of their patients, a probable explanation is that the left IR was fibrotic in our patient and acutely inflamed in theirs.
The pathogenesis of TAO and extraocular muscle damage are poorly understood. It is believed that immunologic cross-reactivity of sensitized T-lymphocytes and/or autoantibodies against the thyroid and orbit may trigger the inflammatory process.[6] As the inflammatory reaction becomes chronic, the extraocular muscles and surrounding tissues become fibrotic, causing restricted eye movements. Unlike Graves’ disease, the TRAb hypothesis cannot be used to explain the ocular myopathy in Hashimoto's thyroiditis, because patients with Hashimoto's disease usually test negative for TRAb. However, specific antibodies against eye muscle proteins, such as calsequestrin, collagen XIII flavoprotein (Fp), and G2 s may be responsible for the extraocular muscle involvement in this condition. There is accumulating evidence that calsequestrin and Fp antibodies are the most frequently detected antibodies; hence, some scholars suggest that they may be used as indicator tests to predict muscle involvement at the onset of extraocular muscle inflammation, thereby facilitating early treatment.[7,8] Unfortunately, we were unable to test these antibodies in the present patient. Hashimoto's thyroiditis and Graves’ disease share some immunological features; hence, determining the genetic basis is the key to a better understanding of the differences between these 2 related diseases. Brown et al[9] reported that the major histocompatibility complex class I and II genes, BTNL2, NOTCH4, TNFAIP3, and CXCR4, showed significant association with Graves’ disease. Lombardi et al[10] mapped 3 single-nucleotide polymorphisms at a chromosome 3q locus that conferred susceptibility to Graves’ disease in Italians. Huang et al[11] identified that HLA-B ∗46:01 conferred susceptibility to Hashimoto's thyroiditis in the pediatric Chinese Han population, whereas Wang et al[12] found that TCGGC haplotype and UBE2L3 were associated with Hashimoto's thyroiditis in the adult Chinese Han population. We were unable to obtain the patient's consent for genetic testing, which was another limitation of this study.
In this case, a lack of typical signs led to the initial misdiagnosis of DEP in the left eye. DEP can be congenital or acquired, and Ziffer et al[13] classified it into 3 sub-types: primary IR restriction, complete or incomplete paralysis of the superior rectus, and supranuclear palsy. FDT and orbital imaging are sometimes insufficient to differentiate TAO from primary IR restriction, especially when patients have atypical history and clinical features. Thus, a specialist should always consider all the possibilities and perform further investigations, if necessary. Systemic manifestations, such as fatigue, weight gain, pale or puffy face, chills, joint and muscle pains, constipation, dry and thinning hair, heavy menstrual flow or irregular periods, depression, and bradycardia may provide clues, suggesting a diagnosis of Hashimoto's thyroiditis. Besides, Hashimoto's thyroiditis can also be a component of polyglandular autoimmune hypofunction syndrome. Therefore, other autoimmune diseases should be suspected in such patients.[14]
Footnotes
Abbreviations: A-TG = antithyroglobulin, A-TPO = antithyroid peroxidase, CT = computed tomography, DEP = double elevator palsy, FDT = forced duction test, FT3 = free triiodothyronine, FT4 = free thyroxine, IR = inferior rectus, TAO = thyroid-associated ophthalmopathy, TRAb = thyrotropin receptor antibody, TSH = thyroid-stimulating hormone, UER = upper eyelid retraction.
Declaration: A written informed consent was obtained from the patient. The ethical approval was not necessary because there was no ethical issue involved.
The authors have no funding and conflicts of interest to disclose.
References
- [1].Tjiang H, Lahooti H, McCorquodale T, et al. Eye and eyelid abnormalities are common in patients with Hashimoto's thyroiditis. Thyroid 2010;20:287–90. [DOI] [PubMed] [Google Scholar]
- [2].Kan E, Kan EK, Ecemis G, et al. Presence of thyroid-associated ophthalmopathy in Hashimoto's thyroiditis. Int J Ophthalmol 2014;7:644–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Hiraga A, Mimura M, Kamitsukasa I. Isolated inferior rectus muscle myopathy due to Hashimoto's thyroiditis. Intern Med 2008;47:1283–4. [DOI] [PubMed] [Google Scholar]
- [4].Grzesiuk W, Szydlarska D, Pragacz A, et al. Thyroid-associated orbitopathy in patients with Hashimoto's thyroiditis: a case report. Pol Arch Med Wewn 2008;118:318–21. [PubMed] [Google Scholar]
- [5].Yoshihara A, Yoshimura Noh J, Nakachi A, et al. Severe thyroid-associated orbitopathy in Hashimoto's thyroiditis. Report of 2 cases. Endocr J 2011;58:343–8. [DOI] [PubMed] [Google Scholar]
- [6].Iyer S, Bahn R. Immunopathogenesis of Graves’ ophthalmopathy: the role of the TSH receptor. Best Pract Res Clin Endocrinol Meta 2012;26:281–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Gopinath B, Ma G, Wall JR. Eye signs and serum eye muscle and collagen XIII antibodies in patients with transient and progressive thyroiditis. Thyroid 2007;17:1123–9. [DOI] [PubMed] [Google Scholar]
- [8].Miller A, Arthurs B, Boucher A, et al. Significance of antibodies reactive with a 64 kDa eye muscle membrane antigen in patients with thyroid autoimmunity. Thyroid 1992;2:197–202. [DOI] [PubMed] [Google Scholar]
- [9].Brown RS, Lombardi A, Hasham A, et al. Genetic analysis in young-age-of-onset Graves’ disease reveals new susceptibility loci. J Clin Endocrinol Metab 2014;99:1387–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Lombardi A, Menconi F, Greenberg D, et al. Dissecting the genetic susceptibility to Graves’ disease in a cohort of patients of Italian origin. Front Endocrinol (Lausanne) 2016;7:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Huang CY, Chang TY, Chu CC, et al. The HLA-B gene and Hashimoto disease in Han Chinese children: a case-control and family-based study. Tissue Antigens 2012;80:431–6. [DOI] [PubMed] [Google Scholar]
- [12].Wang Y, Zhu YF, Wang Q, et al. The haplotype of UBE2L3 gene is associated with Hashimoto's thyroiditis in a Chinese Han population. BMC Endocr Disord 2016;16:18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Ziffer AJ, Rosenbaum AL, Demer JL, et al. Congenital double elevator palsy: vertical saccadic velocity utilizing the scleral search coil technique. J Pediatr Ophthalmol Strabismus 1992;29:142–9. [DOI] [PubMed] [Google Scholar]
- [14].Dieli-Crimi R, Núñez C, Estrada L, et al. An autoimmune polyglandular syndrome complicated with celiac disease and autoimmune hepatitis. Ann Hepatol 2016;15:588–91. [PubMed] [Google Scholar]