

Supplemental Digital Content is available in the text
Keywords: cognition disorders, comprehensive geriatric care, delirium, geriatric ward, hip fractures, interdisciplinary, multidisciplinary
Abstract
Background:
The aim of the current meta-analysis was to assess the treatment effect of comprehensive geriatric care in reducing acute perioperative delirium in older patients with hip fractures, compared with the effect of a routine orthopedic treatment protocol.
Methods:
We conducted a search of multiple databases to identify randomized controlled trials (RCTs) and quasi-RCTs comparing comprehensive geriatric care and routine orthopedic treatment regarding the following outcomes: incidence of delirium, assessment of cognitive status, and duration of delirium. Odds ratios (ORs) and mean differences (MDs) were pooled using either a fixed-effects or a random-effects model, depending on the heterogeneity of the trials included in the analysis.
Results:
Six RCTs and 1 quasi-RCT provided data from 1840 patients. These data revealed that comprehensive geriatric care may reduce the incidence of perioperative delirium (OR = 0.71; 95% confidence interval [CI], 0.57–0.89; P = .003) and that it was associated with higher cognitive status during hospitalization or at 1 month postoperatively (MD = 1.03; 95% CI, 0.93–1.13; P ≤ .00001). There was no significant difference in duration of perioperative delirium between the 2 treatment groups (MD = −2.48; 95% CI, −7.36 to 2.40; P = .32).
Conclusion:
Based on the quality of evidence provided, comprehensive geriatric care may reduce the incidence of perioperative delirium. To obtain evidence regarding the merits of comprehensive geriatric care in reducing severity of delirium and shortening the duration of delirium, there is a need for multicenter RCTs with high methodological quality.
1. Introduction
Femoral neck fractures and intertrochanteric fractures are frequently sustained by geriatric patients.[1,2] To reduce complications, such as decubitus ulcer and hypostatic pneumonia, surgical treatment is mandatory in these fragile patients.[3–5] With the development of knowledge of biomechanics of osteoporotic proximal femur fractures, expertise of surgical skills, and anesthesia monitoring during surgery, most fragile patients could survive the operation and acquire walking ability.[6–9] However, quality of life in these patients is deteriorated in comparison with their preinjury level.[10–13] Acute perioperative delirium, a neuropsychiatric syndrome characterized by disturbance in consciousness, change in cognition, or perceptual disturbance,[14] is a common complication in geriatric hip-fracture patients;[14–17] accordingly, patients with delirium require around-the-clock surveillance to prevent accidents. Perioperative delirium is also a predictive risk factor for postoperative mortality, morbidity, poor functional outcomes, and long hospital stay.[16–19]
Although there has been significant improvement in surgical techniques and skills, perioperative delirium is still high due to orthopedic surgeons’ lack of knowledge and experience in managing fragile older patients.[20] It is presumed that there are several underlying causes that could predispose older patients with hip fractures to perioperative delirium, such as perioperative hypotension, hypoxemia, and anemia.[21–23] Timely and effective management of these risk facts and geriatric patients’ comorbidities may reduce acute perioperative delirium in elderly patients with hip fractures. Comprehensive geriatric care is an established good practice for older trauma patients and incorporates multidisciplinary medical specialists.[24,25] Notwithstanding, several meta-analyses reported contradictory results regarding the treatment effect of comprehensive geriatric care on functional outcomes, length of hospital stay, and mortality rate in older patients with hip fractures.[20,26–28] However, none of these meta-analyses reported outcomes concerning perioperative delirium. Accordingly, we performed this meta-analysis to compare the treatment effect of comprehensive geriatric care in reducing acute perioperative delirium in older patients with hip fractures with that of routine orthopedic treatment.
2. Materials and methods
2.1. Search strategy
Ethical approval was not necessary for this meta-analysis study. A search of PubMed, Cochrane databases, Database of Promoting Health Effectiveness Review, EPPI-Centre database of health promotion research, Physiotherapy Evidence Database, DissOnline, the European Association for Grey Literature Exploitation, and China National Knowledge Infrastructure was performed from their inception to July 2016, without limitations to the study designs, using the following Medical Subject Heading terms and text words in different combinations (Supplemental file 1): geriatrics, geriatric nursing, geriatric psychiatry, health services for the aged, multidisciplinary, comanagement, co-management, interdisciplinary, comprehensive care, geriatr∗, geriatr∗-orthop∗, orthopaedic-geriatr∗, ortho∗-geriatr∗, orthogeriatr∗, team approach, protocol driven, integrated care, multi-factorial, hip fracture∗, femur∗ neck fracture∗, femoral∗ neck fracture, proximal femur∗ fracture∗, proximal femoral∗ fracture∗, intracapsular∗ femur∗ neck fracture∗, intracapsular∗ femoral∗ neck fracture∗, intracapsular∗ hip∗ fracture∗, trochant∗ fracture∗, pertrochant∗ fracture∗, intertrochant∗ fracture∗, subtrochant∗ fracture∗, and extracapsular∗ fracture∗. These subject-specific terms were combined with the Cochrane Highly Sensitive Search Strategy, sensitivity- and precision-maximizing version,[29] to identify randomized controlled trials (RCTs) and quasi-RCTs. The search was supplemented by a manual citation search of the reference lists of relevant studies identified.
2.2. Inclusion criteria/exclusion criteria
Only RCTs and quasi-RCTs were included in our meta-analysis, with nonrandomized trials excluded. All RCTs and quasi-RCTs comparing comprehensive geriatric care to routine orthopedic treatment protocol for hip fracture patients treated in an acute setting were eligible. The patients in the comprehensive geriatric care group needed to be treated by a specialist medical team specializing in geriatric orthopedic patients, with staff providing comprehensive medical assessment, management, and initiation of rehabilitation, and orthopedic surgeons performing the operations. Patients in the routine orthopedic treatment group needed to be cared for by orthopedic surgeons, with geriatric consultation as required. Comprehensive geriatric care treatment needed to be initiated preoperatively or within 24 hours postoperatively.
2.3. Outcomes of interest
The following perioperative outcomes of interest were included in the analysis: incidence of delirium, assessment of cognitive status, and duration of delirium. Delirium was defined as neuropsychiatric syndrome characterized by disturbance in consciousness (impaired ability to focus, sustain, or shift attention) and change in cognition (memory impairment, disorientation, or language disturbance) or perceptual disturbance (misinterpretations, illusions, or hallucinations); the disturbance needed to occur over a short period and fluctuate during the course of the day.[16] All outcomes were determined during hospitalization and/or 1 month postoperatively.
2.4. Study selection and data extraction
Two reviewers independently assessed the eligibility of identified trials in an unblinded, standardized manner. Data were collected independently by the 2 reviewers, and disagreements were resolved by discussion with a senior author. The following information was extracted from the included trials: research method; characteristics of trial participants, including age, sex, and fracture type; inclusion and exclusion criteria; intervention characteristics; postoperative outcomes of interest; and risk of bias. When information was missing, we attempted to contact the primary author by email to seek clarification.
2.5. Quality assessment
The risk of bias was evaluated independently by 2 of the review authors using the domain-based evaluation described in the Cochrane Handbook for Systematic Reviews of Interventions.[30] The following domains were assessed: random sequence generation; allocation concealment; blinding of participants, research personnel, and outcome assessors; incomplete outcome data; and selective outcome reporting. Each of these criteria were assessed as “low risk of bias”, “high risk of bias”, or “unclear risk of bias”, when there was lack of information or uncertainty over the potential for bias. The quality of the evidence was quantified using the Grades of Recommendation, Assessment, Development, and Evaluation approach,[31] with disagreements between the review authors regarding the risk of bias for the identified domains resolved by consensus.
2.6. Statistical analysis
The meta-analyses were performed using Review Manager software (RevMan Version 5.3; The Nordic Cochrane Center, Copenhagen, Denmark). In addition, tests for funnel plot asymmetry were performed with Stata software (StataSE 12.0; StataCorp LP, College Station, TX). Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for dichotomous outcomes. Continuous outcomes were expressed as mean differences (MDs) with corresponding 95% CIs. Heterogeneity across trials was tested by using chi-squared analysis, with the I2 statistic used to assess the impact of identified heterogeneity on the meta-analysis. Substantial heterogeneity was defined as I2 > 50%. If substantial heterogeneity between trials included in an analysis was identified, estimates of pooled data were evaluated using a random-effect model; otherwise, a fixed-effect model was chosen. Funnel plot asymmetry was assessed using Begg and Egger tests.
3. Results
3.1. Literature search
The details of our search strategy and exclusion criteria are presented in the flow diagram in Figure 1. A total of 1055 titles and abstracts were preliminarily screened, with 7 trials eventually satisfying our eligibility criteria.[32–38] We further manually searched the references of the included studies, but identified no more RCTs or quasi-RCTs satisfying our eligibility criteria. We also further investigated the trials not reporting the outcomes of interest; several studies evaluated cognitive status or mental disability using the Mini Mental State Examination (MMSE), Confusion Assessment Method (CAM), Delirium Index, Short Mental Status Questionnaire score, Clinical Dementia Rating Scale, or Red Cross Hospital Scale at the initial admission as participant baseline characteristics.[25,39–48] Further, we found that 2 studies evaluated general mental health using the Medical Outcomes study 36-item short form Taiwan version shortly after operative treatment of hip fractures, and 1 study evaluated depressive symptoms using the Chinese version of the Geriatric Depression Scale, short form.[49–51] Nonetheless, none of the aforementioned studies addressed outcomes of acute perioperative delirium during hospitalization or 1 month postoperatively. After thorough discussion with each other and in consultation with a neurology specialist, we decided to exclude these trials to ensure that the definition of acute perioperative delirium strictly adhered to our eligibility criteria and consistent throughout our included trials. Six of the included trials were RCTs,[32–37] and 1 was a quasi-RCT.[38] Each study reported the outcome of treatment effect of comprehensive geriatric care in reducing acute perioperative delirium in older patients with hip fractures, compared with that of routine orthopedic treatment.
Figure 1.
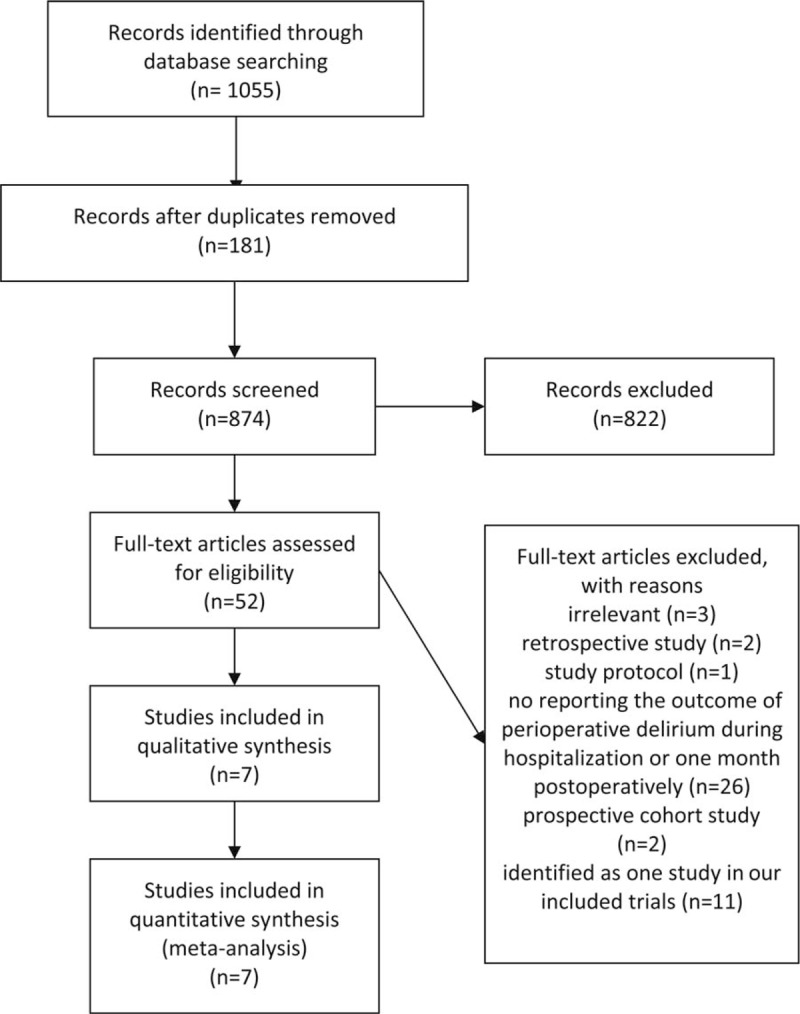
Flow diagram of literature search.
3.2. Quality assessment
Six included studies had methodological flaws that put them at either unclear or high risk of bias for at least 1 domain,[32–35,37,38] with 1 trial of high methodological quality[36] (Figs. 2 and 3). Adequate randomization was reported in 4 RCTs; these RCTs used a random number table,[36] computer-generated number,[32,35] or throw of dice[34] as randomization methods. The method of randomization was not reported in the other 2 RCTs[33,37]. The quasi-RCT reported that group assignment was based on bed availability.[38]
Figure 2.
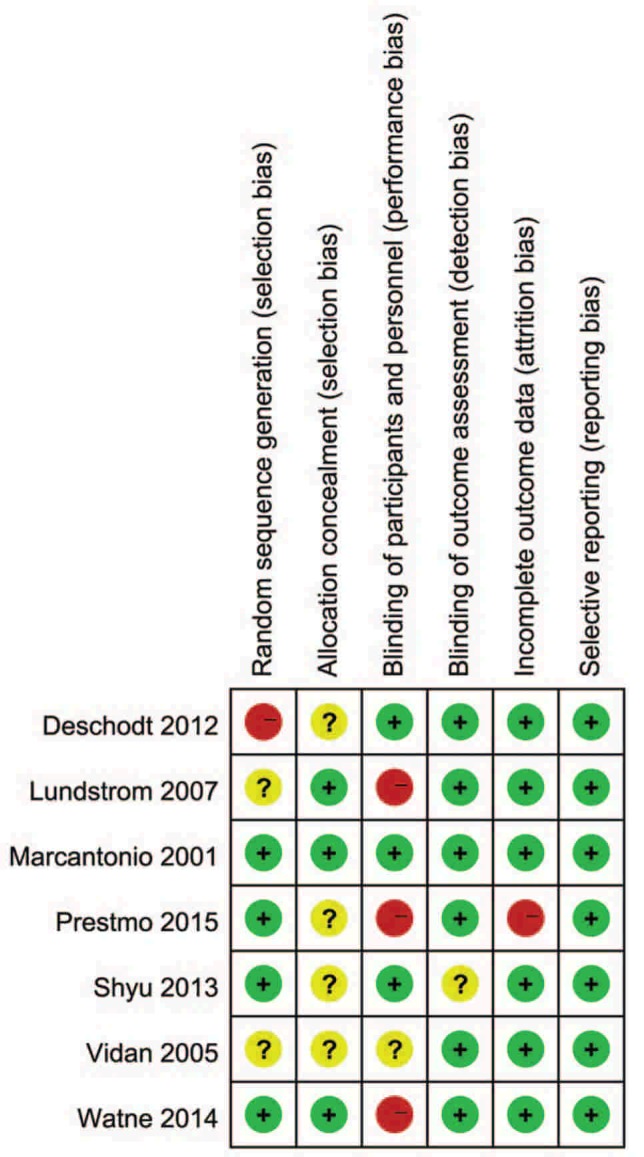
Summary of risk bias assessment. Note: Reviewers’ assessment of each risk of bias item; “+”, low risk of bias; “?”, unclear risk of bias; and “−”, high risk of bias.
Figure 3.
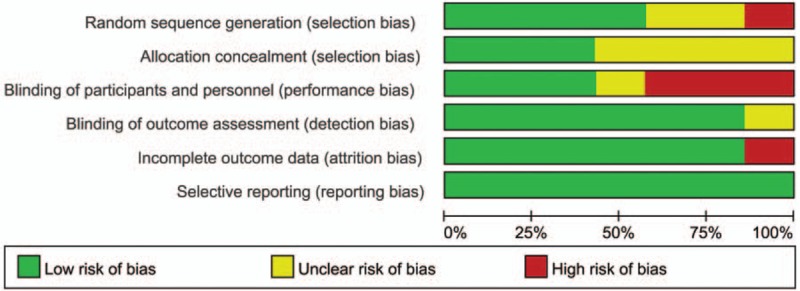
Risk of bias graph. Note: Reviewers’ assessment of each risk bias item, presented as a percent across all included randomized controlled trials.
Three trials described the method of allocation concealment.[32,36,37] Two studies used blinding of participants, personnel and outcome assessment,[36,38] 1 trial used blinding of participants and personnel,[34] and 4 trials used blinding of outcome assessment.[32,33,35,37] One study was at high risk of bias from incomplete outcome data, this was due to a high attrition rate (19.40%); furthermore, the authors did not report the derivation of missing data, nor did they describe the distribution of patients lost to follow-up between the 2 treatment groups. Moreover, that particular study reported the cognitive status evaluated by MMSE, without the outcomes of incidence of delirium or duration of delirium.[35]
3.3. Descriptive characteristics
The descriptive characteristics of the included studies are listed in Table 1, with relevant characteristics summarized here. All the included trials were reported in English and were single-center trials; 5 trials were conducted in Europe,[32,33,35,37,38] 1 in North America,[36] and 1 in China.[34] Six studies were parallel RCTs[32–37] and 1 was a quasi-RCT.[38] In 4 of the included studies, the patients in the comprehensive geriatric care group were actively cared for by a geriatric team daily[33,34,36,38]; in the other 3 trials, the patients in the comprehensive geriatric care group were cared for in the geriatric ward.[32,35,37] Five studies initiated the comprehensive geriatric care treatment preoperatively,[32–35,38] 1 study initiated the treatment within 24 hours postoperatively,[37] and 1 study initiated the treatment either preoperatively or within 24 hours postoperatively.[36] Six studies reported no significant difference in preoperative cognitive status between treatment groups,[32,33,35–38] with 1 study excluding cognitively impaired participants.[34]
Table 1.
Descriptive characteristics of included trials.
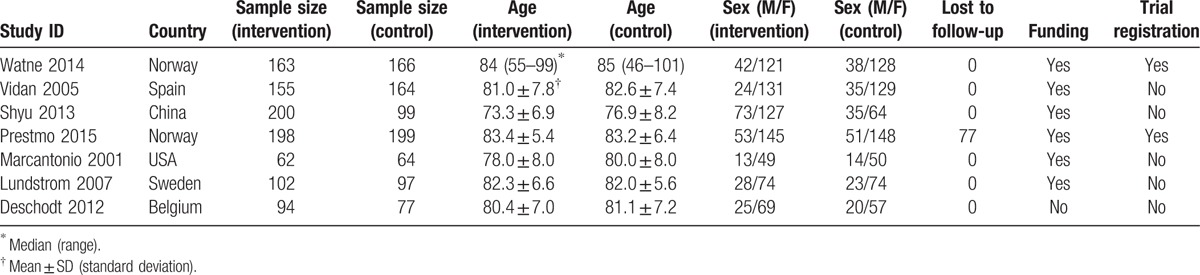
Together, the included trials enrolled a total of 1840 patients; after accounting for participants lost to follow-up, data from 1763 participants were entered in our meta-analysis. Six trials included hip fractures (extra- and intracapsular),[32–36,38] and 1 trial included only femoral neck fractures.[37]
3.4. Effects of interventions
Four trials coincidentally and strictly followed the CAM criteria to diagnose perioperative delirium.[32,33,36,38] One trial used the Organic Brain Syndrome Scale (OBS-Scale) to screen the patients for perioperative deliriums; the authors stated that the OBS-Scale showed 100% agreement regarding the diagnosis of delirium when compared with the CAM.[37] One trial did not directly screen the participants for delirium, but detected perioperative delirium using the MMSE.[34] Six trials reported the incidence of perioperative delirium during hospitalization or at 1 month postoperatively,[32–34,36–38] with a calculated OR of 0.71 (95% CI, 0.57–0.89; P = .003; Fig. 4). Four trials reported the number of days of perioperative delirium,[32,36–38] but we were only able to extract data from 2 trials,[36,37] with a calculated MD of −2.48 (95% CI, −7.36 to 2.40; P = .32; Fig. 5). The other 2 trials reported the median duration of delirium,[32,38] with no significant differences between groups.
Figure 4.
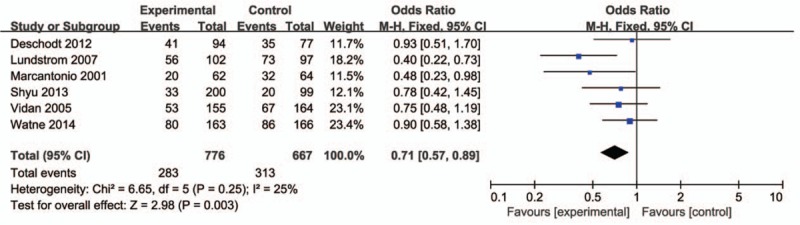
Forest plot of odds ratios and associated confidence intervals for the incidence of perioperative delirium during hospitalization or 1 month postoperatively.
Figure 5.

Forest plot of mean differences and associated confidence intervals for number of days of perioperative delirium during hospitalization or 1 month postoperatively.
Three trials assessed cognitive status during hospitalization or at 1 month postoperatively using the MMSE[35,37,38]; we were only able to extract data from 2 trials,[35,37] with a calculated MD of 1.03 (95% CI, 0.93–1.13; P ≤ .00001; Fig. 6). The remaining trial[38] reported that control participants had lower MMSE scores than those in intervention participants.
Figure 6.

Forest plot of mean differences and associated confidence intervals for cognitive status based on Mini–Mental State Examination Scores during hospitalization or 1 month postoperatively.
3.5. Sensitivity analysis
As 1 study used the MMSE to diagnose delirium indirectly[34] and 5 trials used a more sophisticated screening method,[32,33,36–38] we performed the sensitivity analysis by excluding the study using the MMSE. The result was in accordance with general pooled data, with a calculated OR of 0.71 (95% CI, 0.56–0.89; P = .004).
3.6. Publication bias
An assessment of publication bias was conducted for incidence of perioperative delirium; the funnel plot is presented as Supplemental file 2. The analysis did not identify any potential publication bias (Egger test, P = .250; Begg test, P = .260).
4. Discussion
The current meta-analysis indicated that being in the comprehensive geriatric care group was associated with a lower incidence of perioperative delirium and higher cognitive status during hospitalization or at 1 month postoperatively. There was no significant difference in duration of perioperative delirium between the 2 groups. Although we could not extract outcome data from 3 trials which reported cognitive status and duration of perioperative delirium, the results of these 3 trials were in accordance with our pooled results.
Delirium is the frequently encountered complication in elderly hip fracture patients by orthopedic surgeons, but it received much less attention compared with other complications, such as deep vein thrombosis, pulmonary embolism, and infections. The pathogenesis of delirium has not been thoroughly studied and fully understood. It has been reported that there are several underlying causes which predisposing geriatric hip fracture patients to perioperative delirium. Timely and corrective management of these underlying causes and patient comorbidities may reduce perioperative delirium in elderly hip fracture patients. Although multiple meta-analyses reported the treatment effect of comprehensive geriatric care compared with routine orthopedic treatment, the result of perioperative delirium has not been reported yet. Our meta-analysis exclusively focuses on the treatment effect of comprehensive geriatric care on perioperative delirium to complement existing meta-analyses.
Our meta-analysis included 7 studies which reported outcomes of interest concerning perioperative delirium. Because the outcome of interest was delirium during hospitalization or at 1 month postoperatively, attrition bias was low in 6 included studies due to the short-term follow-up period, with only 1 trial high attrition bias. Due to lack of allocation concealment and blinding of participants and personnel, we concluded the quality of evidence for incidence of perioperative delirium to be moderate. With regard to cognitive status, owing to the lack of blinding of participants and personnel in combination with the low sample size and high attrition bias, we concluded the quality of evidence for perioperative cognitive status was very low. Due to high heterogeneity and low sample size, we concluded the quality of data regarding duration of delirium to be low.
The current meta-analysis firmly followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines for systematic reviews and meta-analyses (Supplemental file 3). However, there are several limitations, so the outcomes should be interpreted with caution. First, all the included studies were small, single-center trials. Second, the included studies used 3 diagnosis and assessment criteria to screen participants for acute perioperative delirium; of these, the CAM and OBS-Scale are validated in the literature in assessing and diagnosing delirium with high sensitivity and specificity,[52,53] whereas MMSE has been used but is not frequently used in diagnosing delirium.[54] Accordingly, we performed the sensitivity analysis by excluding the study of Shyu et al,[34] in which delirium was diagnosed using MMSE and in which the incidence of acute of perioperative delirium was much lower than other included studies. The result was in accordance with general pooled data. Third, although comprehensive geriatric care in our identified trials coincidentally included treatment provided by a specialist medical team specializing in geriatric orthopedic patients, the specific intervention, surgical technique, staff member experience, and anesthetic method would differ between studies. Fourth, the inclusion and exclusion criteria were different across included trials, and the differences in included/excluded comorbidities may affect our outcome of interest. Fifth, because of a language barrier, we excluded studies written in languages other than English and Chinese. We acknowledge that failure to include studies in other languages resulted in missing data.
5. Conclusion
The present meta-analysis is the first to assess the treatment effect of comprehensive geriatric care in reducing perioperative delirium in older patients with hip fractures compared with the effect of a routine orthopedic treatment protocol. Based on the quality of evidence provided, comprehensive geriatric care can reduce the incidence of perioperative delirium during hospitalization or at 1 month postoperatively. To obtain evidence regarding the merits of comprehensive geriatric care in reducing severity of delirium and shortening the duration of delirium, there is a need for multicenter RCTs with high methodological quality.
Acknowledgments
We would like to thank Editage [www.editage.com] for English language editing.
Supplementary Material
Footnotes
Abbreviations: CAM = Confusion Assessment Method, CI = confidence interval, MD = mean difference, MMSE = Mini Mental State Examination, OBS-Scale = Organic Brain Syndrome Scale, OR = odds ratio, RCT = randomized controlled trial.
Each author certifies that no benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Funding/support: The study was supported by the Wenzhou Municipal Science and Technology Bureau (CN) (Y20160389).
The authors have no funding and conflicts of interest to disclose.
Supplemental Digital Content is available for this article.
References
- [1].Cooper C, Campion G, Melton LJ., III Hip fractures in the elderly: a world-wide projection. Osteoporos Int 1992;2:285–9. [DOI] [PubMed] [Google Scholar]
- [2].Hartholt KA, van Beeck EF, Polinder S, et al. Societal consequences of falls in the older population: injuries, healthcare costs, and long-term reduced quality of life. J Trauma 2011;71:748–53. [DOI] [PubMed] [Google Scholar]
- [3].Burge R, Dawson-Hughes B, Solomon DH, et al. Incidence and economic burden of osteoporosisrelated fractures in the United States, 2005–2025. J Bone Miner Res 2007;22:465–75. [DOI] [PubMed] [Google Scholar]
- [4].Osnes EK, Lofthus CM, Meyer HE, et al. Consequences of hip fracture on activities of daily life and residential needs. Osteoporos Int 2004;15:567–74. [DOI] [PubMed] [Google Scholar]
- [5].Ikpeze TC, Mohney S, Elfar JC. Initial preoperative management of geriatric hip fractures. Geriatr Orthop Surg Rehabil 2017;8:64–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Brox WT, Chan PH, Cafri G, et al. Similar mortality with general or regional anesthesia in elderly hip fracture patients. Acta Orthop 2016;87:152–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Kim BG, Lee YK, Park HP, et al. C-reactive protein is an independent predictor for 1-year mortality in elderly patients undergoing hip fracture surgery: A retrospective analysis. Medicine (Baltimore) 2016;95:e5152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Bang S, Chung J, Jeong J, et al. Efficacy of ultrasound-guided fascia iliaca compartment block after hip hemiarthroplasty: a prospective, randomized trial. Medicine (Baltimore) 2016;95:e5018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Tol MC, van den Bekerom MP, Sierevelt IN, et al. Hemiarthroplasty or total hip arthroplasty for the treatment of a displaced intracapsular fracture in active elderly patients: 12-year follow-up of randomised trial. Bone Joint J 2017;99-B:250–4. [DOI] [PubMed] [Google Scholar]
- [10].Chammout G, Muren O, Laurencikas E, et al. More complications with uncemented than cemented femoral stems in total hip replacement for displaced femoral neck fractures in the elderly. Acta Orthop 2017;88:145–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Vergara I, Vrotsou K, Orive M, et al. Factors related to functional prognosis in elderly patients after accidental hip fractures: a prospective cohort study. BMC Geriatr 2014;14:124–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Chiu MH, Hwang HF, Lee HD, et al. Effect of fracture type on health-related quality of life among older women in Taiwan. Arch Phys Med Rehabil 2012;93:512–9. [DOI] [PubMed] [Google Scholar]
- [13].Orive M, Aguirre U, García-Gutiérrez S, et al. Changes in healthrelated quality of life and activities of daily living after hip fracture because of a fall in elderly patients: a prospective cohort study. Int J Clin Pract 2015;69:491–500. [DOI] [PubMed] [Google Scholar]
- [14].Robertson BD, Robertson TJ. Postoperative delirium after hip fracture. J Bone Joint Surg Am 2006;88:2060–8. [DOI] [PubMed] [Google Scholar]
- [15].Mukka S, Knutsson B, Krupic F, et al. The influence of cognitive status on outcome and walking ability after hemiarthroplasty for femoral neck fracture: a prospective cohort study. Eur J Orthop Surg Traumatol 2016;DOI: 10.1007/s00590-016-1873-9. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Edelstein DM, Aharonoff GB, Karp A, et al. Effect of postoperative delirium on outcome after hip fracture. Clin Orthop Relat Res 2004;422:195–200. [DOI] [PubMed] [Google Scholar]
- [17].Oh CS, Rhee KY, Yoon TG, et al. Postoperative delirium in elderly patients undergoing hip fracture surgery in the sugammadex era: a retrospective study. Biomed Res Int 2016;2016:1054597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Marcantonio ER, Flacker JM, Michaels M, et al. Delirium is independently associated with poor functional recovery after hip fracture. J Am Geriatr Soc 2000;48:618–24. [DOI] [PubMed] [Google Scholar]
- [19].Gustafson Y, Berggren D, Brannstrom B, et al. Acute confusional states in elderly patients treated for femoral neck fracture. J Am Geriatr Soc 1988;36:525–30. [DOI] [PubMed] [Google Scholar]
- [20].Grigoryan KV, Javedan H, Rudolph JL. Ortho-geriatric care models and outcomes in hip fracture patients: a systematic review and meta-analysis. J Orthop Trauma 2014;28:e49–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Winawer N. Postoperative delirium. Med Clin North Am 2001;85:1229–39. [DOI] [PubMed] [Google Scholar]
- [22].Trzepacz PT. The neuropathogenesis of delirium. A need to focus our research. Psychosomatics 1994;35:374–91. [DOI] [PubMed] [Google Scholar]
- [23].van der Mast RC. Pathophysiology of delirium. J Geriatr Psychiatry Neurol 1998;11:138–45. [DOI] [PubMed] [Google Scholar]
- [24].Gilchrist WJ, Newman RJ, Hamblen DL, et al. Prospective randomised study of an orthopaedic geriatric inpatient service. BMJ 1988;297:1116–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Thingstad P, Taraldsen K, Saltvedt I, et al. The long-term effect of comprehensive geriatric care on gait after hip fracture: the Trondheim Hip Fracture Trial—a randomised controlled trial. Osteoporos Int 2016;27:933–42. [DOI] [PubMed] [Google Scholar]
- [26].Buecking B, Timmesfeld N, Riem S, et al. Early orthogeriatric treatment of trauma in the elderly. Dtsch Arztebl Int 2013;110:255–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Kammerlander C, Roth T, Friedman SM, et al. Ortho-geriatric service—a literature review comparing different models. Osteoporos Int 2010;21:6379–446. [DOI] [PubMed] [Google Scholar]
- [28].Wang H, Li C, Zhang Y, et al. The influence of inpatient comprehensive geriatric care on elderly patients with hip fractures: a meta-analysis of randomized controlled trials. Int J Clin Exp Med 2015;8:19815–30. [PMC free article] [PubMed] [Google Scholar]
- [29].The Cochrane Collaboration, Lefebvre C, Manheimer E, Glanville J. Higgins JPT, Green S. Chapter 6: searching for studies. Box 6.4.d: Cochrane highly sensitive search strategy for identifying randomized trials in MEDLINE: sensitivity- and precision-maximizing version. Cochrane Handbook for Systemic Reviews of Interventions Version 5.1.0 (updated March 2011) 2008;Available from: http://handbook.cochrane.org/. Accessed May 1, 2017. [Google Scholar]
- [30].The Cochrane Collaboration, Higgins JPT, Altman DG, Sterne JAC. Higgins JPT, Green S. Chapter 8: assessing risk of bias in included studies. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011) 2011;Available from: http://handbook.cochrane.org/. Accessed May 1, 2017. [Google Scholar]
- [31].GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004;328:1490–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Watne LO, Torbergsen AC, Conroy S, et al. The effect of a pre- and postoperative orthogeriatric service on cognitive function in patients with hip fracture: randomized controlled trial (Oslo Orthogeriatric Trial). BMC Med 2014;63:1–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Vidan M, Serra JA, Moreno C, et al. Efficacy of a comprehensive geriatric intervention in older patients hospitalized for hip fracture: a randomized, controlled trial. J Am Geriatr Soc 2005;53:1476–82. [DOI] [PubMed] [Google Scholar]
- [34].Shyu YI, Liang J, Tseng MY, et al. Comprehensive care improves health outcomes among elderly Taiwanese patients with hip fracture. J Gerontol A Biol Sci Med Sci 2013;68:188–97. [DOI] [PubMed] [Google Scholar]
- [35].Prestmo A, Hagen G, Sletvold O, et al. Comprehensive geriatric care for patients with hip fractures: a prospective, randomised, controlled trial. Lancet 2015;385:1623–33. [DOI] [PubMed] [Google Scholar]
- [36].Marcantonio ER, Flacker JM, Wright RJ, et al. Reducing delirium after hip fracture: a randomized trial. J Am Geriatr Soc 2001;49:516–22. [DOI] [PubMed] [Google Scholar]
- [37].Lundstrom M, Olofsson B, Stenvall M, et al. Postoperative delirium in old patients with femoral neck fracture: a randomized intervention study. Aging Clin Exp Res 2007;19:178–86. [DOI] [PubMed] [Google Scholar]
- [38].Deschodt M, Braes T, Flamaing J, et al. Preventing delirium in older adults with recent hip fracture through multidisciplinary geriatric consultation. J Am Geriatr Soc 2012;60:733–9. [DOI] [PubMed] [Google Scholar]
- [39].Deschodt M, Braes T, Broos P, et al. Effect of an inpatient geriatric consultation team on functional outcome, mortality, institutionalization, and readmission rate in older adults with hip fracture: a controlled trial. J Am Geriatr Soc 2011;59:1299–308. [DOI] [PubMed] [Google Scholar]
- [40].Kennie DC, Reid J, Richardson IR, et al. Effectiveness of geriatric rehabilitative care after fractures of the proximal femur in elderly women: a randomised clinical trial. BMJ 1988;297:1083–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Singh NA, Quine S, Clemson LM, et al. Effects of high-intensity progressive resistance training and targeted multidisciplinary treatment of frailty on mortality and nursing home admissions after hip fracture: a randomized controlled trial. J Am Med Dir Assoc 2012;13:24–30. [DOI] [PubMed] [Google Scholar]
- [42].Dai YT, Huang GS, Yang RS, et al. Effectiveness of a multidisciplinary rehabilitation program in elderly patients with hip fractures. J Formos Med Assoc 2001;100:120–6. [PubMed] [Google Scholar]
- [43].Tseng MY, Shyu YI, Liang J. Functional recovery of older hip-fracture patients after interdisciplinary intervention follows three distinct trajectories. Gerontologist 2012;52:833–42. [DOI] [PubMed] [Google Scholar]
- [44].Krichbaum K. GAPN postacute care coordination improves hip fracture outcomes. West J Nurs Res 2007;29:523–44. [DOI] [PubMed] [Google Scholar]
- [45].Reid J, Kennie DC. Geriatric rehabilitative care after fractures of the proximal femur: one year follow up of a randomised clinical trial. BMJ 1989;299:25–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Huusko TM, Karppi P, Avikainen V, et al. Randomised, clinically controlled trial of intensive geriatric rehabilitation in patients with hip fracture: subgroup analysis of patients with dementia. BMJ 2000;321:1107–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].González-Montalvo JI, Alarcón T, Mauleón JL, et al. The orthogeriatric unit for acute patients: a new model of care that improves efficiency in the management of patients with hip fracture. Hip Int 2010;20:229–35. [DOI] [PubMed] [Google Scholar]
- [48].Karlsson Å, Berggren M, Gustafson Y, et al. Effects of geriatric interdisciplinary home rehabilitation on walking ability and length of hospital stay after hip fracture: a randomized controlled trial. J Am Med Dir Assoc 2016;17:464.e9–15. [DOI] [PubMed] [Google Scholar]
- [49].Shyu YI, Liang J, Wu CC, et al. A pilot investigation of the short-term effects of an interdisciplinary intervention program on elderly patients with hip fracture in Taiwan. J Am Geriatr Soc 2005;53:811–8. [DOI] [PubMed] [Google Scholar]
- [50].Shyu YI, Liang J, Wu CC, et al. An interdisciplinary intervention for older Taiwanese patients after surgery for hip fracture improves health-related quality of life. BMC Musculoskelet Disord 2010;11:225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [51].Shyu YI, Liang J, Wu CC, et al. Interdisciplinary intervention for hip fracture in older Taiwanese: benefits last for 1 year. J Gerontol A Biol Sci Med Sci 2008;63:92–7. [DOI] [PubMed] [Google Scholar]
- [52].Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med 1990;113:941–8. [DOI] [PubMed] [Google Scholar]
- [53].Eriksson M1, Samuelsson E, Gustafson Y, et al. Delirium after coronary bypass surgery evaluated by the organic brain syndrome protocol. Scand Cardiovasc J 2002;36:250–5. [DOI] [PubMed] [Google Scholar]
- [54].O’Keeffe ST, Mulkerrin EC, Nayeem K, et al. Use of serial Mini–Mental State Examinations to diagnose and monitor delirium in elderly hospital patients. J Am Geriatr Soc 2005;53:867–70. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.