

Abstract
Introduction
Removal of pulmonary secretions in mechanically ventilated patients usually requires suction with closed catheter systems or flexible bronchoscopes. Manual ventilation is occasionally performed during such procedures if clinicians suspect inadequate ventilation. Suctioning can also be performed with the ventilator entirely disconnected from the endotracheal tube (ETT). The aim of this study was to investigate if these two procedures generate negative airway pressures, which may contribute to atelectasis.
Methods
The effects of device insertion and suctioning in ETTs were examined in a mechanical lung model with a pressure transducer inserted distal to ETTs of 9 mm, 8 mm and 7 mm internal diameter (ID). A 16 Fr bronchoscope and 12, 14 and 16 Fr suction catheters were used at two different vacuum levels during manual ventilation and with the ETTs disconnected.
Results
During manual ventilation with ETTs of 9 mm, 8 mm and 7 mm ID, and bronchoscopic suctioning at moderate suction level, peak pressure (PPEAK) dropped from 23, 22 and 24.5 cm H2O to 16, 16 and 15 cm H2O, respectively. Maximum suction reduced PPEAK to 20, 17 and 11 cm H2O, respectively, and the end-expiratory pressure fell from 5, 5.5 and 4.5 cm H2O to –2, –6 and –17 cm H2O. Suctioning through disconnected ETTs (open suction procedure) gave negative model airway pressures throughout the duration of the procedures.
Conclusions
Manual ventilation and open suction procedures induce negative end-expiratory pressure during endotracheal suctioning, which may have clinical implications in patients who need high PEEP (positive end-expiratory pressure).
Keywords: endotracheal suctioning, airway pressure, manual ventilation, Open suction procedure, bronchoscopy, closed catheter system, peak pressure, end-expiratory pressure
Key messages.
Manual (bag) ventilation contributes to negative end-expiratory pressures during endotracheal suctioning.
Open suctioning, with the ETT disconnected from the ventilator, provides even more negative pressures during endotracheal suctioning.
Both procedures may contribute to the development of atelectasis and should be avoided, to the extent possible, in patients who need high PEEP.
Introduction
Removal of pulmonary secretions in mechanically ventilated patients usually requires suction with closed catheter systems (closed-circuit suctioning) or flexible bronchoscopes. If the suction device obstructs larger parts of the endotracheal tube (ETT) lumen, ventilation volumes and ventilator circuit pressures may change dramatically. Under such conditions, concerned personnel may switch to ventilation with a self-expanding bag with the intention to maintain adequate ventilation—in spite of current guidelines that recommend the ventilator to be connected during suction procedures.1 An alternative strategy, if copious secretions cannot be adequately eliminated during closed catheter suctioning, is to disconnect the ETT from the ventilator in order to more effectively remove airway secretions through an open suction procedure.2 Manual hyperinflation is also a frequently used manoeuvre that intends to mimic a forceful cough in critically ill intubated and mechanically ventilated patients.3
In previous lung model and animal studies of open and closed endotracheal suctioning, Stenqvist and colleagues have found that closed system suctioning may cause subatmospheric pressures in the lungs,4 and have shown that open and closed system suctioning at atmospheric pressure (continuous positive airway pressure (CPAP), 0 cm H2O) is more effective than closed system suctioning during pressure-controlled ventilation (PCV) and CPAP 10 cm H2O.5 They also found that frequent drug inhalation and endotracheal suctioning predispose to de-recruitment of the lungs,6 and that volume-controlled ventilation (VCV) can be used to rapidly restitute lung aeration and oxygenation after lung collapse induced by open suctioning.7
We have previously reported on the effects of ETT device insertion and suctioning on airway pressures in a lung model during pressure-controlled and volume-controlled mechanical ventilation.8 For comparison, we now investigated how suctioning during manual ventilation and during ETT disconnection affected airway pressures in the same model. Our main hypotheses were that endotracheal suctioning during manual ventilation creates pressure reductions similar to those seen in mechanical ventilation with volume-controlled mode, and that suctioning with the ETT disconnected from the bag/ventilator (open suction procedure) provides even more negative pressures distal to the ETT.
Materials and methods
Bench model set-up
The effects of device insertion and suctioning through ETTs were examined with a standard silicone self-expanding ventilation bag (Laerdal Medical, Stavanger, Norway) connected to a mechanical lung model (Adult/Paediatric Demonstration Lung Model, IngMar Medical, Pittsburgh, Pennsylvania, USA). The lung model was connected to an artificial air chamber (figure 1A) in order to obtain end-expiratory model gas volumes comparable with the functional residual capacity of patients with secondary lung disorder.9 Extra weight (750 g) was put on top of the bellows to simulate the reduction in compliance common in patients with acute respiratory failure (figure 1B). A rapid response pressure transducer embedded in a 5 Fr plastic tube (Reggie, Camtech AS, Høvik, Norway) was inserted through an air-tight entrance port (Teleflex angled connector, Teleflex, Morrisville, North Carolina, USA) (figure 1C) and positioned 5 cm distal to the ETT. Real-time pressure changes were recorded (figure 1D) as depicted in figure 2. These pressures simulate airway pressures and are described as ‘model airway pressures’. ETTs of 9 mm, 8 mm and 7 mm internal diameter (ID) and lengths of 26, 25 and 24 cm, respectively, were used (Mallinckrodt, Hazelwood, Missouri, USA) (figure 1E).
Figure 1.
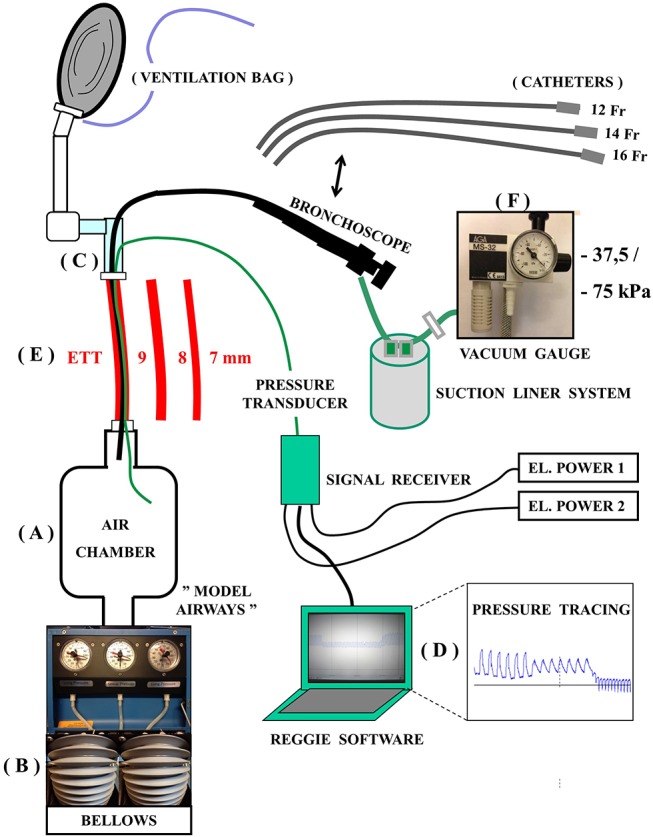
Test design: design and connections of the mechanical lung model test system. ETT, endotracheal tube.
Figure 2.

Manual ventilation versus open suction procedure. Pressures distal to ETT 7 mm during bronchoscopic suctioning: changes in peak, mean and end-expiratory model airway pressures (PPEAK MA, PMEAN MA and PEEP MA) distal to an ETT with 7 mm inner diameter during bronchoscope insertion (16 Fr) and maximum suction (−765 cm H2O (−75 kPa)) are shown. For comparison, unpublished tracings from a previous study of mechanical ventilation are shown below. The total effect of suctioning compared with normal ventilation is shown as Δ PPEAK MA and Δ PEEP MA. Note that during the suction procedure, PMEAN MA is −10 cm H2O in manual ventilation, −18 cm H2O with the ETT disconnected and 7 cm H2O during mechanical volume-controlled ventilation. ETT, endotracheal tube.
Suction devices and flow rates
Endotracheal suctioning was performed as in clinical practice, using closed catheter systems with outer diameter 12 Fr in ETT 7 mm and 14 Fr in ETT 8 and 9 mm. Bronchoscopic suctioning was performed with a 16 Fr bronchoscope (Olympus LF-TP, Tokyo, Japan; suction channel diameter 2.6 mm, working length 600 mm). Open suctioning was performed with either 12, 14 or 16 Fr catheters or a bronchoscope inserted through disconnected ETTs.
Catheters and bronchoscopes were connected to an AGA MS-32 ejector suction device (AGA, Espoo, Finland) (figure 1F) with a vacuum gauge (WIKA Instrument, Lawrenceville, Georgia, USA) that was further connected to a suction liner system (Serres hospital products, Kauhajoki, Finland) with standard tubes from the ejector to the suction bag via a VAC-GARD filter (Hospira, Lake Forest, Illinois, USA). The accuracy of the vacuum gauge scale was checked against a water column.
The suction levels used were a moderate vacuum pressure level of −382 cm H2O (−37.5 kPa) and a maximum level of −765 cm H2O (−75 kPa). Flow rates through suction devices were measured by a spirometer (Vmax 22, Viasys, Yorba Linda, California, USA) to 8.8 L/min and 14.1 L/min through the bronchoscope suction channel (moderate and maximum suction pressure). In 12 Fr catheters, the flow rate was 9.6 L/min and 15 L/min, respectively, and in 14 Fr catheters 9.6 L/min and 17 L/min.
Experimental procedures
Suctioning during manual ventilation
The effects of device insertion and suctioning through ETTs during manual ventilation were examined using a ventilation bag equipped with a positive end-expiratory pressure (PEEP) valve set to 5 cm H2O. Ventilation was performed by an experienced anaesthesiologist visually blinded from test equipment and unaware of the test design. Ventilation at a steady pace, analogous to a real patient situation (I:E ratio, 1:2 and 15 inflations/min), was achieved using a metronome set at 45 bpm.
Peak and end-expiratory model airway pressures (PPEAK MA and PEEP MA) were measured distal to the ETT for 30 s: (1) before insertion of suction catheter/bronchoscope, (2) after insertion but before suctioning, (3) during suctioning with the tip of the catheter/bronchoscope positioned 5 cm distal to the ETT and (4) after removal of the suctioning device, as depicted in figure 2. It was verified that the pressure returned to 0 cm H2O (pretest calibration level) after each recording. The sequence was carried out with closed catheter systems in ETT 9 mm, 8 mm and 7 mm ID, using both moderate and maximum suction pressure. After a 15 min break, the entire procedure was repeated with a 16 Fr bronchoscope in reversed order to avoid possible influence by the order of which the test equipment was used.
Open suctioning
Open suctioning was performed in repeated interventional sequences with ETTs disconnected, using both 12, 14 and 16 Fr catheters and a 16 Fr bronchoscope in all three tube sizes with moderate and maximum suction pressure.
Suctioning during mechanical ventilation
In order to graphically compare test results with mechanical ventilation under standardised conditions, the lung model was connected to a ventilator (SERVO-i, Maquet, Solna, Sweden) as in the previous study8 for a 2×2 min recording sequence with ETT 7 mm inner diameter and conventional ventilator setting (I:E ratio, 1:3; flow trigger F/5) in VCV and PCV mode.
Data management
Manual ventilation before and during scope insertion was performed twice to assess user differences (presented as median values and ranges in figure 3). The median difference between first-round and second-round manual ventilation was 1 cm H2O (0–4).
Figure 3.

Suction pressure variation in different ETT sizes: model airway pressures are recorded as described in figure 3 using both bronchoscopic and closed catheter suction systems during manual ventilation (left panel) and with the ETT disconnected (right panel). Each manual ventilation procedure was performed with both moderate and maximum suction levels. ETT, endotracheal tube.
Pressures measured during open suction procedure were unchanged when repeatedly recorded with the same ETT diameter and suction vacuum settings. For bronchoscopic and catheter-based suctioning, a total of 2–4 complete recordings were performed for each permutation. As no differences were registered, the registrations were not repeated to perform statistical analysis.
The study was exempt from a requirement for ethical approval in line with the Integrated Research Application System decision tool.
Results
During manual ventilation with a self-expanding bag connected to ETTs of 9 mm, 8 mm and 7 mm ID, PPEAK MA was reduced from 23, 22 and 24.5 cm H2O to 16, 16 and 15 cm H2O, respectively, during bronchoscopic suctioning with moderate suction level (figure 3, upper left). The reduction was more modest during closed catheter suctioning (figure 3, lower left). When maximum suction pressure was applied during bronchoscopic suctioning, PPEAK MA was reduced to 20, 17 and 11 cm H2O, respectively (figure 3, upper left).
The effects on end-expiratory pressures were more dramatic. When maximum suction pressure was used during bronchoscopic suctioning, PEEP MA fell from 5, 5.5 and 4.5 cm H2O to –2, –6 and –17 cm H2O, respectively. During closed catheter suctioning, PEEP MA fell from 5.5 cm H2O to – 4, –5 and –7 cm H2O, respectively (figure 3, left panels).
Suctioning through a disconnected ETT (open suction procedure) created negative model airway pressures throughout the duration of the procedure in all tube sizes (figure 3 and table 1). When bronchoscopic suctioning was performed, the P MA was reduced to −2, −5 and −18 cm H2O for ETT 9 mm, 8 mm and 7 mm ID, respectively, which in principle was similar to that of manual ventilation (figure 3, upper panels). For catheter suctioning, pressures were less negative with the ETT disconnected than during manual ventilation (figure 3, lower panels). For each permutation, pressure changes induced by moderate and maximum suction were significant (table 1).
Table 1.
Effects of ETT obstruction and suction pressure
| Open suction procedure (ETT disconnected) |
Before suction | Moderate suction | Maximum suction | |
| PMEAN MA
(cm H2O) |
PMEAN MA
(cm H2O) |
PMEAN MA
(cm H2O) |
||
| ETT 9 | Catheter 12 Fr | 0 | −0.5 | −1.5 |
| Catheter 14 Fr | 0 | −1 | −2 | |
| Catheter 16 Fr | 0 | −2 | −3 | |
| Br.scope 16 Fr | 0 | −1.5 | −2 | |
| ETT 8 | Catheter 12 Fr | 0 | −1 | −2 |
| Catheter 14 Fr | 0 | −2 | −4 | |
| Catheter 16 Fr | 0 | −3 | −7 | |
| Br.scope 16 Fr | 0 | −2 | −5 | |
| ETT 7 | Catheter 12 Fr | 0 | −2 | −5 |
| Catheter 14 Fr | 0 | −4 | −10 | |
| Catheter 16 Fr | 0 | −9 | −23 | |
| Br.scope 16 Fr | 0 | −8 | −18 | |
The effects of altered ETT diameter relative to suction devices and vacuum pressures during open suction procedure are shown. Pressures are measured distal to ETTs, with the ETT disconnected from the test model. Pressures did not change during 30 s of suctioning or when recording was repeated; pressure changes induced by moderate and maximum suction were significant for each permutation. 16 Fr catheters are normally not used clinically in ETT 7 mm ID, but the measurement is included for comparative reasons.
ETT, endotracheal tube.
Discussion
Performing endotracheal suctioning without disconnecting the patient from the ventilator is suggested in the American Association for Respiratory Care clinical practice guidelines.1 One reason given for this is that manual ventilation has been reported to be ineffective for providing an FiO2 of 1.0.10 In real-life situations, when suctioning or diagnostic procedures are performed through a narrow ETT lumen, physicians may respond to low Vt ventilator alarms by switching the ventilator from PCV to VCV, after which the peak pressure alarm may be activated. In our experience, this may lead physicians to change to manual bag ventilation, in an attempt to secure patient ventilation during the suction procedure.
On suction device insertion, initial peak and end-expiratory airway pressures during manual ventilation may be similar to those seen during VCV.8 Depending on the force used to squeeze the ventilation bag, pressures may also be considerably higher. As soon as suctioning is performed, however, end-expiratory pressures fall below 0 during the expiratory phase of manual ventilation, which in a clinical setting would be associated with risk of atelectasis11 and lung collapse, as described by Stenqvist and colleagues in a clinical evaluation.12 As there is no trigging of premature inspirations during manual ventilation, contrary to mechanical ventilation with high trigger sensitivity,8 these negative effects may be accentuated during manual ventilation.
The human factor also plays an important role in manual ventilation. The more rapid loss of bag volume when suction changes from moderate to maximum, for instance, may lead physicians to squeeze the ventilation bag harder, which may explain the increase in peak pressures seen in ETT 9 and 8 mm ID (figure 3, upper left panel).
One could also argue that if multiple anaesthesiologists had performed blinded manual bag ventilation, more diversity would have been added to peak and end-expiratory pressure recordings. As stabile peak-expiratory and end-expiratory pressures were obtained using only one anaesthesiologist, however, with only 1 cm H2O median difference between first-round and second-round manual ventilation at a completely steady pace; the recordings seem sufficient to test our hypothesis.
The most negative pressures in this bench study were observed during open suctioning. This procedure always contributes to negative airway pressures, regardless of suction device and ETT size, and is most profound when a 16 Fr bronchoscope is used in a 7 mm ID ETT. The main benefit from open suctioning, however, is reported to be more effective removal of secretions.13 To our knowledge, open suction is also more frequently used than manual ventilation in most intensive care units. The downside of both procedures is that the resulting negative endobronchial pressure might contribute to atelectasis and warrant recruitment.
According to these results, patients whose oxygenation level or Vt depend on high ventilator PEEP should not be subject to manual bag ventilation during suctioning. Ventilator alarms indicating a fall in Vt for a limited period of time can, in most situations, be ignored in patients without critically high intracranial pressures. The increase in CO2 in normothermic and sedated persons, when ventilation is reduced by bronchoscope insertion, is less than 1 kPa/min,14 which probably pose a lesser risk to patients than further development of atelectases. For the same reason, open suction procedures should be avoided, if possible.
The usefulness of open suctioning relative to closed catheter systems is debated. When comparing open suctioning and traditional closed catheter suctioning in patients with respiratory failure, Lasocki and colleagues13 found that closed suctioning prevented hypoxaemia more effectively than open suctioning, but reduced secretions less effectively.
Lindgren and colleagues found open and closed system suctioning performed at atmospheric pressure (CPAP 0 cm H2O) to be much more effective than closed system suctioning during PCV and CPAP 10 cm H2O.5 The loss off PEEP during suctioning at atmospheric pressure may also contribute to other unwanted effects, such as increased fluid leakage (microaspiration) past endotracheal cuffs.15
Conclusions
This bench study shows that manual (bag) ventilation contributes to negative end-expiratory pressures during endotracheal suctioning—contrary to what is usually seen in mechanical ventilation when closed suction systems and conventional ventilator settings are used. Open suctioning, with the ETT disconnected from the ventilator, provides negative pressures for the duration of the suction procedure. Both procedures may therefore contribute to the development of atelectasis and should be avoided, to the extent possible, in patients who need high PEEP.
Footnotes
Contributors: HO helped design the study, participated in pretest measurements and worked extensively on manuscript and figure texts.
FH participated in measurements and experimental procedures and did revision of the manuscript.
FB helped design the study, was involved in the interpretation of pretest measurements and participated in the revision of the manuscript.
OHS helped design the study, worked on the manuscript and did thorough revision of all text and figure legends.
ERN (corresponding author) designed the study, made modifications to the lung model, did pretest measurements, carried out experimental procedures, drafted the manuscript and produced figures and legends.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: Supplementary data files have been shared in a previous publication (reference 8).
References
- 1. AARC Clinical Practice guidelines. Endotracheal suctioning of mechanically ventilated patients with artificial airways 2010. Respir Care 2010;55:758–64. [PubMed] [Google Scholar]
- 2. Vanner R, Bick E. Tracheal pressures during open suctioning. Anaesthesia 2008;63:313–5.doi:10.1111/j.1365-2044.2007.05348.x [DOI] [PubMed] [Google Scholar]
- 3. Paulus F, Binnekade JM, Vroom MB, et al. Benefits and risks of manual hyperinflation in intubated and mechanically ventilated intensive care unit patients: a systematic review. Crit Care 2012;16:R145.doi:10.1186/cc11457 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Stenqvist O, Lindgren S, Kárason S, et al. Warning! suctioning. A lung model evaluation of closed suctioning systems. Acta Anaesthesiol Scand 2001;45:167–72.doi:10.1034/j.1399-6576.2001.450206.x [DOI] [PubMed] [Google Scholar]
- 5. Lindgren S, Almgren B, Högman M, et al. Effectiveness and side effects of closed and open suctioning: an experimental evaluation. Intensive Care Med 2004;30:1630–7.doi:10.1007/s00134-003-2153-9 [DOI] [PubMed] [Google Scholar]
- 6. Grivans C, Lindgren S, Aneman A, et al. A Scandinavian survey of drug administration through inhalation, suctioning and recruitment maneuvers in mechanically ventilated patients. Acta Anaesthesiol Scand 2009;53:710–6.doi:10.1111/j.1399-6576.2009.01957.x [DOI] [PubMed] [Google Scholar]
- 7. Lindgren S, Odenstedt H, Olegård C, et al. Regional lung derecruitment after endotracheal suction during volume- or pressure-controlled ventilation: a study using electric impedance tomography. Intensive Care Med 2007;33:172–80.doi:10.1007/s00134-006-0425-x [DOI] [PubMed] [Google Scholar]
- 8. Nakstad ER, Opdahl H, Heyerdahl F, et al. Can ventilator settings reduce the negative effects of endotracheal suctioning? Investigations in a mechanical lung model. BMC Anesthesiol 2016;16:30.doi:10.1186/s12871-016-0196-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Bikker IG, van Bommel J, Reis Miranda D, et al. End-expiratory lung volume during mechanical ventilation: a comparison with reference values and the effect of positive end-expiratory pressure in intensive care unit patients with different lung conditions. Crit Care 2008;12:R145.doi:10.1186/cc7125 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Barnes TA, McGarry WP. Evaluation of ten disposable manual resuscitators. Respir Care 1990;35:960–8. [PubMed] [Google Scholar]
- 11. Liu XW, Liu Z. The effects of endotracheal suction on gas exchange and respiratory mechanics in mechanically ventilated patients under pressure-controlled or volume-controlled ventilation. Zhonghua Jie He He Hu Xi Za Zhi 2007;30:751–5. [PubMed] [Google Scholar]
- 12. Lindgren S, Odenstedt H, Erlandsson K, et al. Bronchoscopic suctioning may cause lung collapse: a lung model and clinical evaluation. Acta Anaesthesiol Scand 2008;52:209–18.doi:10.1111/j.1399-6576.2007.01499.x [DOI] [PubMed] [Google Scholar]
- 13. Lasocki S, Lu Q, Sartorius A, et al. Open and closed-circuit endotracheal suctioning in acute lung injury: efficiency and effects on gas exchange. Anesthesiology 2006;104:39–47. [DOI] [PubMed] [Google Scholar]
- 14. Nakstad ER, Opdahl H, Skjønsberg OH, et al. Intrabronchial airway pressures in intubated patients during bronchoscopy under volume controlled and pressure controlled ventilation. Anaesth Intensive Care 2011;39:431–9. [DOI] [PubMed] [Google Scholar]
- 15. Chenelle CT, Itagaki T, Fisher DF, et al. Performance of the PneuX system: a bench study comparison with 4 other endotracheal tube cuffs. Respir Care 2017;62:102–12.doi:10.4187/respcare.04996 [DOI] [PubMed] [Google Scholar]