

Abstract
The display of antisocial behaviors in children and adolescents has been of interest to criminologists and developmental psychologists for years. Exposure to social adversity is a well-documented predictor of antisocial behavior. Additionally, measures of autonomic nervous system (ANS) activity, including heart rate variability (HRV), pre-ejection period (PEP), and heart rate, have been associated with antisocial behaviors including rule-breaking and aggression. Social neuroscience research has begun to investigate how neurobiological underpinnings affect the relationship between social adversity and antisocial/psychopathic behavior in children and adolescents. This study investigated the potential mediating effects of ANS activity on the relationship between social adversity and antisocial behavior in a group of 7- to 10-year-old children from the community (N = 339; 48.2% male). Moderated multiple mediation analyses revealed that low resting heart rate, but not PEP or HRV, mediated the relationship between social adversity and antisocial behavior in males only. Social adversity but not ANS measures were associated with antisocial behavior in females. Findings have implications for understanding the neural influences that underlie antisocial behavior, illustrate the importance of the social environment regarding the expression of these behaviors, and highlight essential gender differences.
Keywords: Heart rate, Gender, Antisocial behavior, Social adversity, Arousal, Aggression
Antisocial behaviors and callous-unemotional/psychopathic traits constitute a predominant risk factor for future criminal behavior (Dyck et al. 2012). Early life displays of antisocial behavior often persist into adolescence and adulthood (Moffitt and Caspi 2001), which makes early intervention critical as well as difficult. Propagation of such behavior is often reinforced in high crime areas, representing a counter-culture attitude that supports aggressive behavior and mistrust of societal rules (Ingoldsby et al. 2006; Simons et al. 2012). Social neuroscience perspectives on antisocial behavior and risk-taking have begun to investigate how neurobiological processes influence the relationship between early-life exposure to social adversity and persistent behavioral deficits that may result in future criminal offending (Choy et al. 2015).
Social Adversity and Antisocial Behavior
Social adversity, an umbrella term that refers to issues such as violent crime, segregation, exposure to delinquent peers, poverty, and poor parenting (Beaver et al. 2008; Moffitt and Caspi 2001; Scarpa and Ollendick 2003), is one of the strongest risk factors for developing antisocial behavior. Early and continued exposure to social adversity has detrimental effects for developing youth, and can exacerbate preexisting behavioral issues (Liu 2004). Research shows that the progression of antisocial behavior and subsequent delinquency is shaped by antisocial attitudes (Mills et al. 2004), poor schooling and a lack of collective efficacy in the community (Ingoldsby et al. 2006), delinquent peer affiliations during adolescence (Monahan et al. 2009), and malnutrition (Raine et al. 2003). Behavioral genetic studies have also demonstrated that shared and non-shared environmental influences play significant roles in predisposing individuals to antisocial behavior (i.e., Eley et al. 2003). In addition, the social environment influences biological risk factors that have been linked to antisocial and criminal behavior.
Low Heart Rate and Antisocial Behavior
Low resting heart rate (HR) is one of the most robust and well-replicated biological markers of antisocial behavior (Ortiz and Raine 2004), and has been linked to proactive and instrumental aggression (Ortiz and Raine 2004; Scarpa et al. 2010), callous-unemotional traits (Frick and White 2008), antisocial behavior (Mezzacappa et al. 1997), and rule-breaking/delinquency (Jennings et al. 2013). Theories of under-arousal and sensation-seeking speculate that individuals with hypoactive autonomic nervous system (ANS) activity (i.e., those with low resting HR) participate in risky or thrill-seeking behaviors and/or proactive displays of aggression in an attempt to elevate their autonomic arousal to more comfortable levels (Scarpa and Raine 2004). Alternatively, fearlessness theory proposes that low levels of arousal reflect a fearless temperament; a lack of internal arousal that would otherwise cue bodily structures involved in feedback and associative learning impairs fear processing (Hawes et al. 2009).
Parasympathetic and Sympathetic Nervous System Activity and Antisocial Behavior
There is a research gap concerning the potentially separable effects of the sympathetic and parasympathetic nervous systems on antisocial behavior. The rhythm of the heart is modulated by both sympathetic and parasympathetic inputs that accelerate and slow the heartbeat, respectively. The balance of these two systems is critical for the development and execution of socially adaptive functions such as approach, avoidance, and arousal (Thayer and Sternberg 2006). The polyvagal theory (Porges 1995, 2007) argues that the parasympathetic vagal activity that is responsible for slowing the heart acts as a brake, regulating appropriate emotional responses to differing external and internal demands. Modulations in vagal activity can be captured by signal power in the high frequency band derived from Fourier transformation of the HR time series (Berntson et al. 1997; Porges 2007). At rest, sympathetic and parasympathetic tone may underlie individual readiness to either respond to threat or restore bodily homeostasis, depending on the situation (Scarpa et al. 2010).
Enhanced vagal activity and high levels of resting heart rate variability (HRV) have been associated with dispositional sympathy and concerned attention (Fabes et al. 1993). Elevated vagal tone can also buffer the development of internalizing and externalizing behaviors in situations of familial adversity (Beauchaine et al. 2007). Low resting HRV has been associated with outcomes in children such as antisocial behavior (Mezzacappa et al. 1997), externalizing (Pine et al. 1998), reactive aggression (Scarpa et al. 2010), and oppositional defiant disorder and conduct disorder (Beauchaine et al. 2007). On the other hand, some studies have shown that high resting HRV is associated with increased proactive aggression (Scarpa et al. 2010) and externalizing behavior (Dietrich et al. 2007).
Pre-ejection period (PEP) is a widely used measure of sympathetic related cardiac activity that measures the time from the depolarization of the left ventricle of the heart to the onset of ejection of blood into the aorta, and represents cardiac output modulated by the beta-adrenal system (Berntson et al. 1994; Musser et al. 2013). Lengthened resting PEPs (reflecting low sympathetic activity) have been correlated with conduct problems and aggression (Beauchaine et al. 2013), externalizing behavior (Brenner and Beauchaine 2011), and oppositional defiant disorder and attention deficit hyperactivity disorder (Crowell et al. 2006), suggesting sympathetic under-activity in child and adolescent populations with externalizing behavioral profiles.
Social Adversity and Autonomic Functioning
Social adversity may play a role in altering or disrupting biological functioning. Early social adversity may act directly on the developing hypothalamic–pituitary–adrenal (HPA) axis to blunt stress responses (e.g., low cortisol and reduced HR reactivity), which in turn can lead to antisocial behavior, risk-taking, impulsivity and poor emotion regulation (Lovallo 2013). For example, exposure to community violence has been associated with low resting HR in urban school-aged children (Krenichyn et al. 2001). In addition, adolescent females exposed to child maltreatment showed lower resting vagal tone than controls (Miskovic et al. 2009), and a recent meta-analysis found that children from clinical or at-risk samples had reduced vagal tone compared to community and non-clinical samples (Graziano and Derefinko 2013). However, no relationship between social adversity and sympathetic cardiac activity has been reported.
Previous research has focused mainly on the moderating effects of cardiovascular measures on behavioral deficits from stress exposure or familial adversity (e.g., Scarpa et al. 2008). In these studies, ANS activity is categorized into high and low groups, i.e., high versus low parasympathetic activity (El-Sheikh and Hinnant 2011). However, few studies have examined how continuous exposure to early childhood adversity affects cardiovascular responding, which in turn leads to subsequent antisocial behavior. Recent evidence suggests that acute and chronic stress can alter brain and bodily functioning over time (Lovallo et al. 2012). The neurosensitivity hypothesis argues that genes and early environmental stress exposure interact with both each other and the central nervous system to influence subsequent physiological activity and behavioral responsivity (Pluess 2015). It is now widely accepted that development does not progress according to a strict gene by environment interactive process; rather, it is a function of cortical reorganization dependent upon the environment, genes, and the history of the organism (Cicchetti and Curtis 2015). Based on this understanding of development, we would expect that neurophysiological abnormalities such as atypical ANS activity mediate the relationship between adversity and behavior problems.
Gender Differences
Current endeavors have sought to fill a gap in the investigation and reporting of gender differences in biological research (Clayton and Collins 2014). A meta-analysis suggests that HR predicts antisocial behavior for both boys and girls (Ortiz and Raine 2004). However, of the eight studies cited that included female-only samples, three failed to demonstrate statistically significant results for low resting HR as a predictor of antisocial behavior (Maliphant et al. 2003; Rogeness et al. 1990). Twelve studies in the review used mixed gender samples: four did not show a statistically significant relationship between antisocial behavior and low resting HR (Delamater and Lahey 1983; Garralda et al. 1989, 1991; Van Hulle et al. 2000), three were not published in peer-reviewed journals (Little 1978; Schmeck and Poustka 1995; Van Voorhees and Scarpa 2002), one did not control for gender (Cauffman et al. 2005), and one lacked a true control group, comparing only adolescence-limited antisocial behavior to life-course persistent antisocial behavior, with low numbers of females in the life-course persistent category preventing appropriate gender comparisons (Moffitt and Caspi 2001).
Recent evidence suggests that gender moderates the relationship between autonomic responding and antisocial behavioral displays (Beauchaine 2009), though this line of inquiry is relatively underdeveloped. One study showed that HR at age 11 in girls did not correlate with effortful control, impulsivity, or aggression at age 16, though it did for boys (Sijtsema et al. 2010). Another investigation revealed that resting HR in adolescent girls aged 16–18 years was positively correlated with antisocial behaviors while in males of the same age was negatively correlated with antisocial behaviors (Crozier et al. 2008). Similarly, increased electrodermal responding (a sympathetic measure) was related to increased conduct problems in females aged 8– 12 while lower baseline parasympathetic cardiovascular activity was seen in boys high in aggression (Beauchaine et al. 2008).
The Current Study
The current study has three aims. First, given that both social adversity and antisocial behaviors have been associated with low resting HR, it was predicted that the connection between social adversity and antisocial behaviors could be partially explained by reduced resting HR. To our knowledge, only one study has investigated the mediating effects of HR on social adversity and facets of criminality (Choy et al. 2015). The authors assessed various aspects of antisocial behavior in a community sample of children 11–12 years old who participated in a stress task in which they were asked to give a 4-min speech following a 2-min “preparation phase.” Reduced HR during stress but not resting HR was found to mediate the relationship between social adversity and antisocial behavior (Choy et al. 2015).
We used a factor analytic approach to produce a single common factor for general antisocial behavior. We focused on a common factor measure because antisocial behavior is defined by both cognitive-behavioral elements and criminogenic elements, and is reflective of both characteristic personality traits and conduct violations/overt behaviors (Caspi et al. 2002; Huizinga et al. 2006; Mackey et al. 2016). We additionally examined mediation effects for constituent subscale measures (e.g., externalizing and callous-unemotional behavior) to explore if each had a different etiology with respect to social adversity and ANS responding.
Second, we hoped to clarify if either parasympathetic-(HRV) or sympathetic-related (PEP) cardiac activity contributes more substantially to the relationship between social adversity and antisocial behavior. Given that low resting HRV has been associated with both antisocial behavior and social adversity, and high HRV has been more consistently associated with adaptive behaviors such as emotion regulation, we predicted that low HRV would mediate the relationship between social adversity and antisocial behavior. Since no relationship between social adversity and resting PEP has been reported, we did not formulate any hypothesis on the potential mediating role of PEP. Finally, we aimed to explore if gender moderated the mediating effects of ANS functioning between social adversity and antisocial behavior.
Method
Participants
The sample consisted of 7- to 10-year-old boys and girls (Mean age = 9.06, SD = 0.60; 48.2% male) living in Brooklyn, New York, who were recruited as part of an ongoing longitudinal investigation on the development of behavior problems in childhood. Fliers soliciting enrollment in a study on the “factors that contribute to healthy and happy childhoods” were placed in public areas and targeted mailings were also sent to parents of children living in the geographic catchment area. A phone screening process was conducted to exclude anyone that was taking medications, seeing a therapist, had a diagnosed psychiatric disorder, intellectual disability, or a pervasive developmental disorder. No records were kept for excluded individuals. A total of 445 children were screened and 340 participated, including 52% African-American, 11% Hispanic, 21% Caucasian, 2% Asian, and 14% of mixed/other. Compared to the Kings County (Brooklyn) or New York population, our sample consisted of slightly more African-Americans, and had lower median family income ($43,200 compared to $45,215). Mean years of education of the mother (M = 14.37, SD = 4.11) was slightly higher than that of the father (M = 13.19, SD = 4.15, t = 5.65, p < 0.001). Fifty-nine percent of children lived with both biological parents, and 29% lived alone with their biological mother. Of the families in which biological parents were not living together, 9% had remarried at the time of the study. Two percent of children lived in a single-parent household, and the remaining 1% resided with a single parent and other adults (often grandparents). One child was excluded from the final sample due to missing physiological data.
Procedures
We invited participants and their primary caregivers to the university for a 2-hour laboratory assessment that included caregiver and child behavioral interviews, neurocognitive testing, psychophysiological recording, and social risk factor assessment. Caregivers consisted predominately of biological mothers (86.4%). All interview data were collected by graduate-level research assistants who were trained by the Principle Investigator. During physiological recording, children completed an emotion learning task, a reward paradigm, and an emotion regulation task on the computer. There were rest periods at the onset and conclusion of the physiological recording. For the purpose of the current study, psychophysiological data from the two rest periods were used. Monetary compensation was provided to participating families at the end of the assessment. The university Institutional Review Board approved all procedures, and both parental consent and child assent were obtained.
Measures
Child Behavior Checklist (CBCL; Achenbach and Rescorla 2001)
Caregivers completed the CBCL, a rating scale composed of 112 items concerning the child’s behavior now or within the past 6 months; e.g. “Argues a lot,” or “Impulsive or acts without thinking.” Items are rated on a 3-point scale (0 = not true, 1 = sometimes or somewhat true, 2 = very true or often true). The CBCL has demonstrated both validity and reliability for the assessment of child psychopathology (Dutra et al. 2004). For the present investigation, the aggression and rule-breaking subscales were used (18 items and 17 items, respectively). Subscale scores were derived by summing the raw scores from each item. Cronbach’s α in the current sample was 0.87 and 0.71 for aggression and rule-breaking, respectively. Externalizing Behavior is the sum of the rule-breaking and aggression subscale scores.
The Antisocial Process Screening Device (APSD; Frick and Hare 2001)
Caregivers completed the narcissism (7 items) and impulsivity subscales (5 items) of the APSD, a rating scale composed of 20 items that assesses psychopathic traits in youth. Caregivers are asked how well specific statements describe their child; e.g. “Engages in illegal activities,” and “Becomes angry when corrected or punished.” Items are rated on a 3-point scale (0 = not at all true, 1 = sometimes true, 2 = definitely true). Subscale scores were derived by summing the raw scores from each item. The APSD has demonstrated validity as a representative measure of psychopathic traits in youth in both community and arrested samples (Falkenbach et al. 2003; Frick et al. 2000). The APSD callous-unemotional subscale was supplemented by the Inventory of Callous-Unemotional Traits (see below) as a measure of callous-unemotional traits. Cronbach’s α was 0.70 and 0.60 for narcissism and impulsivity, respectively.
Inventory of Callous-Unemotional Traits (ICU; Frick 2004; Gao and Zhang 2016)
Caregivers completed the ICU to assess the amount of callous-unemotional traits in youth. Factor analyses on the current sample supported a modified ICU form with three subscales (callousness, uncaring, and unemotional) (Gao and Zhang 2016). The modified ICU Scores of individual subscales and total ICU score (sum of the three subscale scores) derived from the modified ICU were used in following analyses. The modified ICU is a 19-item scale derived from the APSD to specifically assess callous-unemotional behaviors associated with antisocial personality and has demonstrated convergent validity with existing self-and parent-report measures of psychopathic behaviors (Gao and Zhang 2016). Caregivers are asked how well certain statements describe their child; e.g. “Seems very cold and uncaring,” and “It is easy to tell how he/she is feeling.” Items are rated on a 4-point scale (0 = not at all true, 1 = somewhat true, 2 = very true, 3 = definitely true). Subscale scores were derived by summing the raw scores from each item. Cronbach’s α was 0.85, 0.71, 0.83, and 0.63 for the total ICU, callousness (7 items), uncaring (8 items), and unemotional subscales (4 items), respectively.
Diagnostic Interview Schedule for Children (DISC-IV; Shaffer et al. 2000)
The trained research assistant administered the DISC-IV to caregivers, a structured interview that assesses the lifetime number of conduct disorder (CD) and oppositional defiant disorder (ODD) symptoms in children, e.g., if the child has ever used alcohol or been suspended or expelled from school. The DISC has shown validity for assessing various psychopathologies in youth (Schwab-Stone et al. 1996). Although none of the participants in our sample met the diagnostic criteria for CD or ODD, 44% of the boys had at least one CD symptom, and 22% of boys had at least 2 CD symptoms in their lifetime. In contrast, only 28% of girls had one or more CD symptoms. For ODD, 84% of the boys had at least one symptom, and 75% of boys had at least 2 symptoms in their lifetime. In girls, 81% had one or more ODD symptoms. In the following analyses, ODD and CD symptom counts were combined to create a variable called “ODD/CD Symptoms.”
Social Adversity
A self-report social adversity index was created based on caregivers’ answers to questions defined in previous literature (Gao et al. 2010; Moffitt 1990). A total adversity score was created by adding 1 point for each of the following ten variables: Divorced Parents (single parent family, remarriage, or living with guardians other than parents), Foster Home, Public Housing, Welfare Food Stamps, Parent Ever Arrested (either parent has been arrested at least once), Parents Physically Ill, Parents Mentally Ill, Crowded Home (five or more family members per room within the home), Teenage Mother (aged 19 years or younger when child was born), and Large Family (having five or more siblings by age 3 year). All items were assessed for the participants’ lifetime and were scored either 0 (no) or 1 (yes), with a high total score indicating higher social adversity.
Psychophysiological Data Acquisition and Reduction
Psychophysiological data were collected continually using a BIOPAC MP150 system (Biopac Inc., CA). HR, HRV, and PEP were each averaged from the initial 2-min rest period at the onset of the computerized tasks and the 2-min rest period at the culmination of the computerized tasks. For subjects with unavailable or unsuitable data (due to movement) for either of the two rest periods, we used the available rest period data for that participant (N = 37). Children were instructed to sit quietly and rest during the rest periods.
HR
HR was analyzed offline with Kubios HRV software (Version 2.2; Tarvainen et al. 2014). Electrocardiography (ECG) signal was recorded using ECG100C with two prejelled Ag-AgCl disposable vinyl electrodes placed at a modified Lead II configuration. Research assistants cleaned the contact area using NuPrep™ prior to affixing the electrodes. All intervals were visually inspected and corrected for false or undetected R-waves, movement artifacts, and ectopic beats. Heart rate was measured in beats per minute (bpm), based on the average of inter-beat intervals (IBI; R-R wave intervals).
HRV
ECG channel recording was analyzed offline using Kubios HRV software (Version 2.2; Tarvainen et al. 2014). After visually inspecting the R-waves, the IBI time series was decomposed into separate component HRV frequencies using Fast Fourier transformation algorithms. Power in the high frequency range (0.15–0.40 Hz; ms2), indexing parasympathetic activity (Berntson et al. 1997), was used in statistical analysis.
PEP
PEP, an index of sympathetic-related cardiac activity (Berntson et al. 1994; Brenner and Beauchaine 2011), was measured using the NICO100C and ECG100C amplifiers. Electrodes were configured according to previous research (Sherwood et al. 1990). The QRS and dZ/dt B waveforms were ensemble-averaged using AcqKnowledge 4.2. PEP was measured as the time (ms) elapsed, between the onset of the Q-wave and the impedance dZ/dt B-point.
Statistical Analyses
All analyses were conducted using SPSS 22.0 and 23.0. Pearson correlations were conducted to examine the associations among study variables and independent samples t-tests to investigate gender differences. We performed a factor analysis of the eight behavioral subscale measures (aggression, rule-breaking, CD/ODD symptoms, impulsivity, narcissism, unemotional behavior, callousness, and uncaring behavior) to reduce the measures to a single comprehensive factor score for general antisocial behavior. This factor score was then entered as the dependent variable into a moderated multiple mediation analysis using the PROCESS macro for SPSS (Hayes 2013), with social adversity as the independent variable, the three physiological measures as parallel mediators, and gender as a moderator. Figure 1 shows a schemata of the moderated multiple mediation model (a statistical representation of the model can be found in Hayes 2015, Fig. 2 Panel A).
Fig. 1.
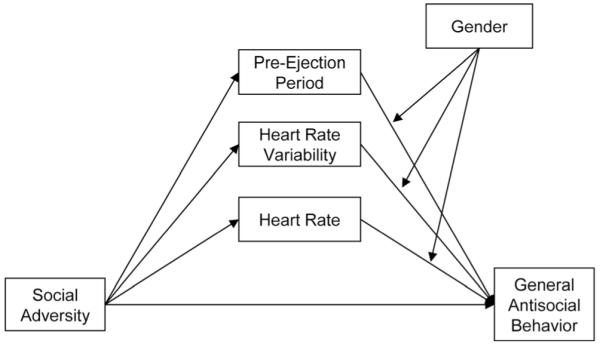
oderated multiple mediation model of the relationship between social adversity and antisocial behavior
Specifically, we tested whether gender moderated the link between ANS mediators and antisocial behavior. A moderated, multiple mediator model allows investigators to evaluate the contribution of each mediator and moderator while controlling for other paths in the model (Duffy et al. 2012; Hayes 2015). The PROCESS macro computes the bootstrapped bias corrected 95% confidence intervals (CI) of the conditional indirect effects by taking 10,000 bootstrapped samples (Hayes 2013). Confidence intervals of the conditional indirect effect that do not contain zero indicate significant mediation effects. Complete mediation occurs when path c’ (the direct effect) is equal to 0, suggesting the association between X and Y is fully accounted for by the mediators, and partial mediation occurs when path c’ is a value other than 0 but significantly less than path c (Baron and Kenny 1986). We ran additional moderated multiple mediation models substituting other behavioral outcomes for general antisocial behavior. In order to rule out reverse causation, additional mediation models were constructed with the independent variable as social adversity, the dependent variable as one of the three ANS measures, and the mediator as general antisocial behavior.
Results
Descriptive Statistics and Correlational Analyses
Outliers beyond 3SDs above or below the means were removed from analyses. Logarithmic transformations were applied to HRV, rule-breaking behavior, aggression, externalizing (total), ODD/CD symptoms, callousness, narcissism, and social adversity prior to further analyses to reduce skewness. The single factor solution of the eight behavioral measures was standardized using the Anderson-Rubin method (M = 0, SD = 1). This general antisocial behavior factor accounted for approximately 52% of the variance (Eigenvalue = 4.134) with factor loadings ranging from 0.455 for unemotional behavior to 0.819 for aggression.
Males and females differed significantly on both behavioral measures and physiological measures. Means, standard deviations, and group comparisons of all variables are listed in Table 1. In males, social adversity was positively associated with general antisocial behavior, ODD/CD symptoms, narcissism, and impulsivity, and HRV. As expected, HR was negatively associated with general antisocial behavior, externalizing, aggression, rule-breaking, ICU total score, and uncaring behavior. In females, social adversity was positively associated with general antisocial behavior, externalizing, aggression, rule-breaking, and narcissism, but neither HR nor HRV were associated with behavioral measures. In both males and females, PEP was not linked to any of the antisocial behavior outcomes nor social adversity. Correlations organized by gender are presented in Table 2, and were substantively unchanged when controlling for ethnicity.
Table 1.
Descriptive statistics
| Measure | Males |
Females |
Gender differences |
|||||
|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Min | Max | Mean (SD) | Min | Max | t | df | |
| HR | 85.13 (10.06) | 61.15 | 113.75 | 88.24 (10.22) | 65.41 | 117.96 | −2.78 ** | 328 |
| HRVa | 3.22 (0.50) | 1.79 | 4.28 | 3.23 (0.44) | 1.99 | 4.23 | −0.21 | 329 |
| PEP | 84.38 (16.94) | 39.00 | 132.50 | 82.28 (14.21) | 40.00 | 120.00 | 1.22 | 327 |
| General Antisocial Behavior | 0.14 (1.03) | −1.73 | 3.03 | −0.13 (0.96) | −1.65 | 2.54 | 2.46 * | 312 |
| Externalizing Behaviora | 7.29 (6.75) | 0 | 30 | 5.81 (5.89) | 0 | 27 | 2.25 * | 334 |
| Aggressiona | 5.17 (5.24) | 0 | 25 | 4.11 (4.33) | 0 | 21 | 1.96 * | 335 |
| Rule-Breaking Behaviora | 2.23 (2.15) | 0 | 14 | 1.71 (1.96) | 0 | 9 | 2.65 ** | 334 |
| ODD/CDa | 5.24 (4.11) | 0 | 19 | 3.98 (3.61) | 0 | 15 | 2.77 ** | 328 |
| Narcissisma | 2.00 (2.12) | 0 | 12 | 1.75 (1.90) | 0 | 9 | 1.20 | 328 |
| Impulsivity | 2.77 (1.80) | 0 | 8 | 2.45 (1.71) | 0 | 8 | 1.66 | 328 |
| ICU | 15.75 (7.65) | 0 | 38 | 14.61 (7.95) | 0 | 36 | 1.33 | 332 |
| Callousnessa | 2.04 (2.36) | 0 | 13 | 1.84 (2.56) | 0 | 15 | 1.48 | 332 |
| Uncaring | 9.69 (4.90) | 0 | 24 | 9.09 (5.05) | 0 | 21 | 1.10 | 332 |
| Unemotional | 4.02 (2.25) | 0 | 10 | 3.68 (2.41) | 0 | 10 | 1.31 | 332 |
| Social Adversitya | 3.05 (2.07) | 0 | 10 | 2.91 (2.01) | 0 | 8 | 0.58 | 332 |
Descriptive statistics show untransformed values; standard deviations appear in parentheses next to means; independent samples t-tests conducted on transformed values (a ) for males and females; boldface type denotes significant difference between males and females
HR heart rate, HRV heart rate variability, PEP pre-ejection period, ODD/CD Oppositional Defiant Disorder/Conduct Disorder, ICU Inventory of Callous-Unemotional Traits
p ≤ 0.01,
p ≤ 0.05, two-tailed
Table 2.
Correlations by gender
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | HR | 1 | −0.59** | −0.15 | −0.05 | −0.08 | −0.05 | −0.11 | −0.02 | 0.08 | −0.02 | 0.02 | .00 | 0.02 | −0.04 | −0.09 |
| 2 | HRVa | −0.71** | 1 | 0.05 | 0.01 | 0.09 | 0.04 | 0.12 | −0.01 | −0.08 | −0.03 | 0.02 | −0.01 | 0.05 | −0.03 | 0.11 |
| 3 | PEP | −0.13 | 0.08 | 1 | 0.04 | −0.03 | −0.03 | −0.03 | −0.10 | 0.09 | 0.08 | 0.05 | 0.02 | 0.06 | 0.05 | −0.04 |
| 4 | General Antisocial Behavior | −0.25** | 0.04 | 0.06 | 1 | 0.84** | 0.81** | 0.78** | 0.60** | 0.77** | 0.75** | 0.78** | 0.69** | 0.70** | 0.44** | 0.18* |
| 5 | Externalizinga | −0.23** | 0.09 | 0.04 | 0.86** | 1 | 0.96** | 0.83** | 0.55** | 0.62** | 0.62** | 0.48** | 0.46** | 0.45** | 0.22** | 0.22** |
| 6 | Aggressiona | −0.27** | 0.11 | 0.06 | 0.83** | 0.96** | 1 | 0.68** | 0.57** | 0.60** | 0.59** | 0.46** | 0.44** | 0.42** | 0.23** | 0.21** |
| 7 | Rule-Breaking Behaviora | −0.19* | 0.11 | 0.05 | 0.80** | 0.85** | 0.71** | 1 | 0.44** | 0.54** | 0.52** | 0.48** | 0.48** | 0.45** | 0.18* | 0.24** |
| 8 | ODD/CDa | −0.13 | 0.01 | −0.04 | 0.58** | 0.45** | 0.48** | 0.31** | 1 | 0.39** | 0.38** | 0.35** | 0.38** | 0.31** | 0.17* | 0.13 |
| 9 | Narcissisma | −0.14 | −0.02 | 0.07 | 0.80** | 0.66** | 0.63** | 0.65** | 0.37** | 1 | 0.54** | 0.48** | 0.40** | 0.46** | 0.24** | 0.20* |
| 10 | Impulsivity | −0.05 | −0.08 | 0.07 | 0.80** | 0.61** | 0.59** | 0.57** | 0.39** | 0.67** | 1 | 0.47** | 0.47** | 0.45** | 0.19* | 0.13 |
| 11 | ICU total | −0.18* | 0.11 | 0.04 | 0.79** | 0.52** | 0.51** | 0.52** | 0.35** | 0.46** | 0.49** | 1 | 0.71** | 0.92** | 0.65** | 0.07 |
| 12 | Callousnessa | −0.14 | 0.12 | −0.02 | 0.70** | 0.53** | 0.53** | 0.49** | 0.32** | 0.52** | 0.55** | 0.62** | 1 | 0.54** | 0.22** | 0.11 |
| 13 | Uncaring | −0.17* | 0.05 | 0.06 | 0.68** | 0.45** | 0.45** | 0.44** | 0.38** | 0.39** | 0.40** | 0.91** | 0.38** | 1 | 0.45** | 0.07 |
| 14 | Unemotional | −0.09 | 0.12 | 0.05 | 0.46** | 0.24** | 0.21** | 0.30** | 0.06 | 0.15 | 0.24** | 0.74** | 0.31** | 0.53** | 1 | 0.02 |
| 15 | Social Adversitya | −0.15 | 0.16* | 0.11 | 0.20* | 0.09 | 0.09 | 0.12 | 0.19* | 0.18* | 0.20* | 0.06 | 0.02 | 0.08 | 0.00 | 1 |
Area above diagonal shows Pearson’s correlations for females, area below the diagonal shows Pearson’s correlations for males
HR heart rate, HRV heart rate variability, PEP pre-ejection period, ODD/CD Oppositional Defiant Disorder/Conduct Disorder, ICU Inventory of Callous-Unemotional Traits
Log-transformed variables
p ≤ 0.01,
p ≤ 0.05, two-tailed
Moderated Multiple Mediation Analyses
Bootstrapping analyses revealed a direct association between social adversity and HR, b = −4.61, p < 0.05, and social adversity and HRV, b = 0.25, p < 0.05, but no association between social adversity and PEP, b = 2.93, p = 0.41. Gender moderated the relationship between HR and antisocial behavior, b = 0.04, p < 0.01, but not the relationship between HRV and antisocial behavior, b = 0.48, p = 0.12, or PEP and antisocial behavior, b = 0.00, p = 0.57. HR, b = −0.08, p < 0.01, and HRV, b = −0.98, p = 0.05, significantly predicted antisocial behavior after controlling for the other variables in the model, though PEP did not, b = −0.00, p = 0.67. The direct effect of social adversity on antisocial behavior remained significant, b = 0.75, p < 0.01, 95% CI = [0.32, 1.19], suggesting partial mediation.
Conditional indirect effects showed that the indirect effect of HR on the relationship between social adversity and antisocial behavior was significant for males, b = 0.19, 95% CI = [0.02, 0.47], but not for females, b = 0.01, 95% CI = [−0.09, 0.14]. Similarly, the conditional indirect effect of HRVon the relationship between social adversity and antisocial behavior was significant for males, b = −0.12, 95%CI = [−0.35, −0.01], but not for females, b = −0.01, 95% CI = [−0.13, 0.11]. However, there was no significant interaction effect between HRV and gender in the model, and the index of moderated mediation was also not significant, 95% CI = [−0.02, 0.41], suggesting gender did not actually moderate the indirect effect of HRV on the relationship between social adversity and antisocial behavior. PEP did not mediate the relationship between social adversity and antisocial behavior, nor was there a moderating effect of gender (all conditional indirect effects ns). See Table 3 for models results.1,2
Table 3.
Moderated multiple mediation: Indirect effect of Social Adversity (X) on General Antisocial Behavior (Y) through Autonomic Nervous System measures (M) as moderated by Gender (V)
| Variable Model (n = 298) | ||||||
| Outcome | Predictor | B | SE | t-Value | p-Value | |
| Independent variable to mediator | ||||||
| ANS | ||||||
| HR (M1) | SA | −4.606 | 2.185 | −2.108 | 0.036* | |
| HRV (M2) | SA | 0.246 | 0.104 | 2.370 | 0.018* | |
| PEP (M3) | SA | 2.932 | 3.665 | 0.800 | 0.424 | |
| Mediator to dependent variable | ||||||
| General Antisocial Behavior | ||||||
| HR | −0.079 | 0.024 | −3.268 | 0.001** | ||
| HRV | −0.975 | 0.497 | −1.960 | 0.051 | ||
| PEP | −0.005 | 0.011 | −0.427 | 0.670 | ||
| Gender | −5.460 | 2.199 | −2.483 | 0.014* | ||
| HR × Gender | 0.039 | 0.015 | 2.657 | 0.008* | ||
| HRV × Gender | 0.478 | 0.309 | 1.545 | 0.123 | ||
| PEP × Gender | 0.004 | 0.007 | 0.567 | 0.571 | ||
| SA | 0.754 | 0.220 | 3.432 | 0.001** | ||
| Direct Effect of X on Y | ||||||
| B | SE | t-Value | p-Value | 95% CI | ||
| 0.754 | 0.220 | 3.432 | 0.001* | [0.322, 1.187] | ||
| Conditional Indirect Effects at Each Level of the Moderator | ||||||
| Males | Females | |||||
| Mediator | B | SE | 95% CI | B | SE | 95% CI |
| HR | 0.185 | 0.112 | [0.023, 0.474] | 0.006 | 0.052 | [−0.087, 0.135] |
| HRV | −0.122 | 0.084 | [−0.351, −0.009] | −0.005 | 0.060 | [−0.131, 0.114] |
| PEP | −0.002 | 0.020 | [−0.059, 0.028] | 0.011 | 0.029 | [−0.019, 0.122] |
| Index of Moderated Mediation | ||||||
| Mediator | Index | SE | 95% CI | |||
| HR | −0.179 | 0.121 | [−0.515, −0.017] | |||
| HRV | 0.117 | 0.104 | [−0.016, 0.408] | |||
| PEP | 0.012 | 0.035 | [−0.026, 0.142] | |||
Bootstrap samples =10,000. Boldface type denotes significant mediation effect
B unstandardized regression coefficients, SE standard error, SA social adversity, ANS autonomic nervous system, HR heart rate, HRV heart rate variability, PEP pre-ejection period
p ≤ 0.01
p ≤ 0.05, two-tailed
Exploratory analyses were conducted to predict each antisocial measure. The conditional indirect effect of HR on the relationship between social adversity was significant for males for externalizing, b = 0.07, 95% CI = [0.01, 0.16], aggression, b = 0.08, 95% CI = [0.01, 0.18], narcissism, b = 0.05, CI = [0.01, 0.12], uncaring behavior, b = 0.62, 95% CI = [0.05, 1.72], and callous-unemotional traits (ICU total score), b = 0.85, 95% CI = [0.02, 2.54], but not for females (all conditional indirect effects ns).3
Finally, reverse-causality analyses showed that general antisocial behavior marginally mediated the relationship between social adversity and HR (indirect effect: b = −1.14, SE = 0.61, 95% CI = [−2.77, −0.25]). Normal theory tests revealed the indirect effect to be marginally significant, p = 0.05, with a small effect size, κ2 = 0.031. We then tested this model with gender moderating the link between general antisocial behavior and HR, but found no evidence of moderated mediation. Lastly, general antisocial behavior did not mediate the relationship between social adversity and HRV, nor between social adversity and PEP (all indirect effects ns).
Discussion
This study examined the mediating effects of ANS activity on the relationship between social adversity and antisocial behavior in children. We found that in males, low resting HR mediated the relationship between social adversity and antisocial behaviors. Although HRV, an indicator of parasympathetic activity, was related to social adversity in males, it was not related to any of the antisocial measures, nor did it mediate the relationship between social adversity and antisocial behavior. While social adversity was strongly related to female antisocial behavior, resting HR or HRV was not. Finally, PEP, an indicator of sympathetic activity, was not related to any of the antisocial measures and did not mediate the relationship between social adversity and antisocial behavior in either gender group.
To our knowledge, this was the first investigation aiming to tease apart parasympathetic from sympathetic influences on resting HR in the context of ANS mediation between social adversity and antisocial behavior. We found that neither PEP nor HRV were mediators, suggesting that neither sympathetic nor parasympathetic activity alone is responsible for the unique way in which HR influences antisocial behavior. While both the sympathetic and parasympathetic systems affect HR, their relationship to one another is not necessarily related, and as such coinhibition, coactivation, and independently-mediated activity is possible. The investigation into the separable influences of the sympathetic and parasympathetic nervous systems provides a scientifically valuable and novel contribution to developmental research on antisocial behavior. Specifically, the null mediating effects of the sympathetic and parasympathetic measures suggest that contrary to common theoretical assumption, the mechanism underlying low resting heart rate cannot be reduced to sympathetic underarousal.
Our hypotheses were partially supported. The moderated multiple mediation model showed that resting HR mediated the relationship between social adversity and general antisocial behavior (as well as externalizing, aggression, narcissism, uncaring behavior and callous-unemotional traits) in males only. As evidenced by a non-zero indirect effect, low resting HR was a mechanism through which social adversity exerted its influence on antisocial behavior (Table 3) (Hayes 2009). These results parallel Choy et al. (2015)‘s finding that HR during a stressor task mediates the relationship between antisocial behavior and social adversity in 11 to 12 year olds. Together, this supports the theoretical accounts that social adversity leads to a state of blunted arousal (Lovallo et al. 2012), which may then promote antisocial behavior, per the fearlessness and sensation seeking theories. This information is clinically relevant and has implications for shaping public policy and community-related programming. While we do not directly address the extent to which HR-mediated antisocial behavior in males is due to sensation seeking or fearlessness, activities that have the potential to mirror the physiological arousal gained from antisocial behavioral demonstrations, such as organized sports and other “thrill-seeking” recreational activities, could be used to supplement arousal levels in males.
Our sample was younger than that of Choy et al. (2015)‘s. Theoretical accounts of antisocial behavior suggest two alternate pathways: life-course persistent and adolescence-limited. Because our sample is notably pre-adolescent (7–10 years old), our results offer insight into components that may be more relevant to life-course persistent rather than adolescence-limited antisocial behavior. If the ANS is sensitive to environmental changes, the effects of persistent adversity should be cumulative, making early intervention critical, given that life-course persistent antisocial behavior is stable across development (Moffitt and Caspi 2001).
Social adversity remained a robust correlate of general antisocial behavior for girls, specifically externalizing behaviors and psychopathic-like narcissism, though HR did not. Although Choy et al. (2015) found unchanged mediation effects controlling for gender, they did not examine these effects for males and females separately. Our results are consistent with recent research that suggests that in normative populations, the blunted ANS responding characteristic of antisocial behavior and psychopathy is more prevalent in boys rather than in girls (Beauchaine et al. 2008), and that the development and display of antisocial behavior in girls compared to boys is a result of increased susceptibility to social and environmental influences (Beauchaine et al. 2008). Alternatively, if social stressors and environmental adversity do alter physiology in females, these physiological changes may be distinct from those of males and manifest in alternate behavioral outcomes. The Adaptive Calibration Model hypothesizes that extreme stress desensitizes the autonomic response in males, promoting antisocial behavior and elevated risk-taking that is evolutionarily adaptive; in females, however, increased stress can result in increased responsivity, an adaptive mechanism that ultimately promotes rapid adaptation to the changing environment such that fertility is maximized (Del Giudice et al. 2011). These sex differences become more pronounced at the transition from middle childhood to adolescence (Del Giudice et al. 2011), which encapsulates our population sample.
We cannot rule out the possibility that the relationship between social adversity and antisocial behavior in females does not operate mechanistically through cardiovascular changes, though it may be reflected in other measures of ANS activity such as skin conductance (Beauchaine et al. 2008). In addition, current measures of antisocial behavior tend to ignore relational aggression, which is commonly displayed in girls with antisocial behavior (Crick and Grotpeter 1995). Had relational aggression been included we may have seen a relationship between ANS measures and antisocial behavior in girls. Relational aggression was related to blunted physiological responding in maltreated and nonmaltreated children (Murray-Close et al. 2008) as well as in females with a history of sexual abuse (Murray-Close and Rellini 2012). Future studies should incorporate relational aggression into a composite measure of antisocial behavior to address this issue.
One of the limitations is that we offer only a cross-sectional view of antisocial behavior. Future directions should include a longitudinal perspective that looks at the stability of the mediator effect over time (Selig and Preacher 2009). Though we could not conclusively rule out reverse-causation (we found that antisocial behavior marginally mediated the relationship between social adversity and heart rate), this model was statistically weak and is theoretically unlikely, given the cross-sectional nature of the data. Second, our social adversity measure does not account for other psychosocial influences such as peer influence or neighborhood crime statistics. Third, several behavioral measures have relatively low levels of reliability and combining them may lead to lower reliability, therefore we suggest cautious interpretation of the results. However, previous studies have shown comparable alpha levels for both the unemotional subscale of the ICU (Essau et al. 2006) and the impulsivity subscale of the APSD (Lynam 2006; Ross et al. 2007). Lastly, our sample is predominantly low-income, therefore these results may not be as readily generalizable to the broader population. Regardless, our results contribute to the growing body of knowledge concerning the mediating effects of biological processes on the link between social adversity and antisocial behavior. It is important to follow up on the discrepancies that we saw between males and females as concerns physiological arousal and antisocial behavior. Accumulating evidence suggests that there are meaningful differences between males and females regarding the etiology and developmental courses of antisocial behavior.
Acknowledgements
This study was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health to Yu Gao under Award Number SC2HD076044. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. We would like to thank the Psychophysiology Lab research staff for their assistance in collecting data and the families for their participation.
Footnotes
Moderated multiple mediation analyses were also conducted using a composite score of antisocial behavior, derived from summing the subscale scores (externalizing behavior, ODD/CD symptoms, narcissism, impulsivity, and callous-unemotional behavior) in order to maintain consistency and comparability with Choy et al. (2015). Results were the same using the composite score.
The SPSS PROCESS macro which uses bootstrapped confidence intervals to index moderated mediation is also robust to highly skewed raw data (Hayes 2015).
Exploratory analyses were also conducted with a standardized antisocial behavior factor score. A factor score for antisocial behavior was constructed from standardized values of each subscale measure and entered as a dependent variable in the moderated multiple mediation model. All results were substantively the same.
Conflicts of Interest The authors declare that they have no conflicts of interest to report.
Compliance with Ethical Standards
Ethical Approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent Informed consent was obtained from all individual participants included in the study.
References
- Achenbach TM, Rescorla LA. Manual for the ASEBA School-Age Forms & Profiles. University of Vermont, Research Center for Children, Youth, & Families; Burlington: 2001. [Google Scholar]
- Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Beauchaine TP. Some difficulties in interpreting psychophysiological research with children. Monographs of the Society for Research in Child Development. 2009;74:80–88. doi: 10.1111/j.1540-5834.2009.00509.x. [DOI] [PubMed] [Google Scholar]
- Beauchaine TP, Gatzke-Kopp L, Mead HK. Polyvagal theory and developmental psychopathology: emotion dysregulation and conduct problems from preschool to adolescence. Biological Psychology. 2007;74:174–184. doi: 10.1016/j.biopsycho.2005.08.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beauchaine TP, Hong J, Marsh P. Sex differences in autonomic correlates of conduct problems and aggression. Journal of the American Academy of Child & Adolescent Psychiatry. 2008;47:788–796. doi: 10.1097/CHI.0b013e318172ef4b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beauchaine TP, Gatzke-Kopp L, Neuhaus E, Chipman J, Reid MJ, Webster-Stratton C. Sympathetic- and parasympathetic-linked cardiac function and prediction of externalizing behavior, emotion regulation, and prosocial behavior among preschoolers treated for ADHD. Journal of Consulting and Clinical Psychology. 2013;81:481–493. doi: 10.1037/a0032302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beaver KM, Eagle Schutt J, Boutwell BB, Ratchford M, Roberts K, Barnes JC. Genetic and environmental influences on levels of self-control and delinquent peer affiliation: results from a longitudinal sample of adolescent twins. Criminal Justice and Behavior. 2008;36:41–60. [Google Scholar]
- Berntson GG, Cacioppo JT, Binkley PF, Uchino BN, Quigley KS, Fieldstone A. Autonomic cardiac control. III. Psychological stress and cardiac response in autonomic space as revealed by pharmacological blockades. Psychophysiology. 1994;31:599–608. doi: 10.1111/j.1469-8986.1994.tb02352.x. [DOI] [PubMed] [Google Scholar]
- Berntson GG, Bigger JT, Eckberg DL, Grossman P, Kaufmann PG, Malik M, et al. Heart rate variability: origins, methods, and interpretive caveats. Psychophysiology. 1997;34:623–648. doi: 10.1111/j.1469-8986.1997.tb02140.x. [DOI] [PubMed] [Google Scholar]
- Brenner SL, Beauchaine TP. Pre-ejection period reactivity and psychiatric comorbidity prospectively predict substance use initiation among middle-schoolers: a pilot study: predictors of adolescent substance use. Psychophysiology. 2011;48:1588–1596. doi: 10.1111/j.1469-8986.2011.01230.x. [DOI] [PubMed] [Google Scholar]
- Caspi A, McClay J, Moffitt TE, Mill J, Martin J, Craig IW, et al. Role of genotype in the cycle of violence in maltreated children. Science. 2002;297:851–854. doi: 10.1126/science.1072290. [DOI] [PubMed] [Google Scholar]
- Cauffman E, Steinberg L, Piquero AR. Psychological, neuropsychological and physiological correlates of serious antisocial behavior in adolescence: the role of self-control. Criminology. 2005;43:133–176. [Google Scholar]
- Choy O, Raine A, Portnoy J, Rudo-Hutt A, Gao Y, Soyfer L. The mediating role of heart rate on the social adversity-antisocial behavior relationship: a social neurocriminology perspective. Journal of Research in Crime and Delinquency. 2015;52:303–341. [Google Scholar]
- Cicchetti D, Curtis WJ. The developing brain and neural plasticity: implications for normality, psychopathology, and resilience. In: Cicchetti D, Cohen DJ, editors. Developmental psychopathology. John Wiley & Sons, Inc.; Hoboken: 2015. pp. 1–64. [Google Scholar]
- Clayton JA, Collins FS. NIH to balance sex in cell and animal studies. Nature. 2014;509:282–283. doi: 10.1038/509282a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crick NR, Grotpeter JK. Relational aggression, gender, and social-psychological adjustment. Child Development. 1995;66:710. doi: 10.1111/j.1467-8624.1995.tb00900.x. [DOI] [PubMed] [Google Scholar]
- Crowell SE, Beauchaine TP, Gatzke-Kopp L, Sylvers P, Mead H, Chipman-Chacon J. Autonomic correlates of attention-deficit/hyperactivity disorder and oppositional defiant disorder in preschool children. Journal of Abnormal Psychology. 2006;115:174–178. doi: 10.1037/0021-843X.115.1.174. [DOI] [PubMed] [Google Scholar]
- Crozier JC, Dodge KA, Fontaine RG, Lansford JE, Bates JE, Pettit GS, Levenson RW. Social information processing and cardiac predictors of adolescent antisocial behavior. Journal of Abnormal Psychology. 2008;117:253–267. doi: 10.1037/0021-843X.117.2.253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Del Giudice M, Ellis BJ, Shirtcliff EA. The adaptive calibration model of stress responsivity. Neuroscience & Biobehavioral Reviews. 2011;35:1562–1592. doi: 10.1016/j.neubiorev.2010.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Delamater AM, Lahey BB. Physiological correlates of conduct problems and anxiety in hyperactive and learning-disabled children. Journal of Abnormal Child Psychology. 1983;11:85–100. doi: 10.1007/BF00912180. [DOI] [PubMed] [Google Scholar]
- Dietrich A, Riese H, Sondeijker FEPL, Greaves-Lord K, van Roon AM, Ormel J, et al. Externalizing and internalizing problems in relation to autonomic function. Journal of the American Academy of Child & Adolescent Psychiatry. 2007;46:378–386. doi: 10.1097/CHI.0b013e31802b91ea. [DOI] [PubMed] [Google Scholar]
- Duffy RD, Bott EM, Allan BA, Torrey CL, Dik BJ. Perceiving a calling, living a calling, and job satisfaction: testing a moderated, multiple mediator model. Journal of Counseling Psychology. 2012;59:50–59. doi: 10.1037/a0026129. [DOI] [PubMed] [Google Scholar]
- Dutra L, Campbell L, Westen D. Quantifying clinical judgment in the assessment of adolescent psychopathology: reliability, validity, and factor structure of the child behavior checklist for clinician report. Journal of Clinical Psychology. 2004;60:65–85. doi: 10.1002/jclp.10234. [DOI] [PubMed] [Google Scholar]
- Dyck HL, Campbell MA, Schmidt F, Wershler JL. Youth psychopathic traits and their impact on long-term criminal offending trajectories. Youth Violence and Juvenile Justice. 2012;11:230–248. [Google Scholar]
- Eley TC, Lichtenstein P, Moffitt TE. A longitudinal behavioral genetic analysis of the etiology of aggressive and nonaggressive antisocial behavior. Development and Psychopathology. 2003;15:383–402. doi: 10.1017/s095457940300021x. [DOI] [PubMed] [Google Scholar]
- El-Sheikh M, Hinnant JB. Marital conflict, respiratory sinus arrhythmia, and allostatic load: interrelations and associations with the development of children’s externalizing behavior. Development and Psychopathology. 2011;23:815–829. doi: 10.1017/S0954579411000320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Essau CA, Sasagawa S, Frick PJ. Callous-unemotional traits in a community sample of adolescents. Assessment. 2006;13:454–469. doi: 10.1177/1073191106287354. [DOI] [PubMed] [Google Scholar]
- Fabes RA, Eisenberg N, Eisenbud L. Behavioral and physiological correlates of children’s reactions to others in distress. Developmental Psychology. 1993;29:655. [Google Scholar]
- Falkenbach DM, Poythress NG, Heide KM. Psychopathic features in a juvenile diversion population: reliability and predictive validity of two self-report measures. Behavioral Sciences & the Law. 2003;21:787–805. doi: 10.1002/bsl.562. [DOI] [PubMed] [Google Scholar]
- Frick PJ. The inventory of callous-unemotional traits. 2004. Unpublished Rating Scale.
- Frick PJ, Hare RD. Antisocial process screening device (APSD) Multi-health systems; Toronto: 2001. [Google Scholar]
- Frick PJ, White SF. Research review: the importance of callous-unemotional traits for developmental models of aggressive and antisocial behavior. Journal of Child Psychology and Psychiatry. 2008;49:359–375. doi: 10.1111/j.1469-7610.2007.01862.x. [DOI] [PubMed] [Google Scholar]
- Frick PJ, Barry CT, Bodin SD. Applying the concept of psychopathy to children: implications for the assessment of antisocial youth. In: Gacono CB, editor. The clinical and forensic assessment of psychopathy: a practitioner’s guide. Routledge; Abingdon: 2000. pp. 3–24. [Google Scholar]
- Gao Y, Zhang W. Confirmatory factor analyses of self- and parent- report inventory of callous-unemotional traits in 8- to 10-year-olds. Journal of Psychopathology and Behavioral Assessment. 2016;38:331–340. doi: 10.1007/s10862-015-9527-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gao Y, Raine A, Chan F, Venables P, Mednick S. Early maternal and paternal bonding, childhood physical abuse and adult psychopathic personality. Psychological Medicine. 2010;40:1007–1016. doi: 10.1017/S0033291709991279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garralda ME, Connell J, Taylor DC. Peripheral psycho-physiological changes in children with conduct and emotional disorders: a study of resting levels and reactivity to sounds. Behavioural Neurology. 1989;2:125–133. [Google Scholar]
- Garralda ME, Connell J, Taylor DC. Psychophysiological anomalies in children with emotional and conduct disorders. Psychological Medicine. 1991;21:947–957. doi: 10.1017/s0033291700029937. [DOI] [PubMed] [Google Scholar]
- Graziano P, Derefinko K. Cardiac vagal control and children’s adaptive functioning: a meta-analysis. Biological Psychology. 2013;94:22–37. doi: 10.1016/j.biopsycho.2013.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawes DJ, Brennan J, Dadds MR. Cortisol, callous-unemotional traits, and pathways to antisocial behavior. Current Opinion in Psychiatry. 2009;22:357–362. doi: 10.1097/YCO.0b013e32832bfa6d. [DOI] [PubMed] [Google Scholar]
- Hayes AF. Beyond baron and Kenny: statistical mediation analysis in the new millennium. Communication Monographs. 2009;76:408–420. [Google Scholar]
- Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. Guilford Press; New York: 2013. [Google Scholar]
- Hayes AF. An index and test of linear moderated mediation. Multivariate Behavioral Research. 2015;50:1–22. doi: 10.1080/00273171.2014.962683. [DOI] [PubMed] [Google Scholar]
- Huizinga D, Haberstick BC, Smolen A, Menard S, Young SE, Corley RP, et al. Childhood maltreatment, subsequent antisocial behavior, and the role of monoamine oxidase a genotype. Biological Psychiatry. 2006;60:677–683. doi: 10.1016/j.biopsych.2005.12.022. [DOI] [PubMed] [Google Scholar]
- Ingoldsby EM, Shaw DS, Winslow E, Schonberg M, Gilliom M, Criss MM. Neighborhood disadvantage, parent–child conflict, neighborhood peer relationships, and early antisocial behavior problem trajectories. Journal of Abnormal Child Psychology. 2006;34:293–309. doi: 10.1007/s10802-006-9026-y. [DOI] [PubMed] [Google Scholar]
- Jennings WG, Piquero AR, Farrington DP. Does resting heart rate at age 18 distinguish general and violent offending up to age 50? Findings from the Cambridge study in delinquent development. Journal of Criminal Justice. 2013;41:213–219. [Google Scholar]
- Krenichyn K, Saegert S, Evans GW. Parents as moderators of psychological and physiological correlates of inner-city children’s exposure to violence. Journal of Applied Developmental Psychology. 2001;22:581–602. [Google Scholar]
- Little B. Physiological correlates of antisocial behavior in children and young adults. Presented at the Psychophysiology Society Annual Meeting; London: Institute of Psychiatry; 1978. [Google Scholar]
- Liu J. Childhood externalizing behavior: theory and implications. Journal of Child and Adolescent Psychiatric Nursing. 2004;17:93–103. doi: 10.1111/j.1744-6171.2004.tb00003.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lovallo WR. Early life adversity reduces stress reactivity and enhances impulsive behavior: implications for health behaviors. International Journal of Psychophysiology. 2013;90:8–16. doi: 10.1016/j.ijpsycho.2012.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lovallo WR, Farag NH, Sorocco KH, Cohoon AJ, Vincent AS. Lifetime adversity leads to blunted stress axis reactivity: studies from the Oklahoma family health patterns project. Biological Psychiatry. 2012;71:344–349. doi: 10.1016/j.biopsych.2011.10.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lynam DR. The perils of partialling: cautionary tales from aggression and psychopathy. Assessment. 2006;13:328–341. doi: 10.1177/1073191106290562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mackey S, Chaarani B, Kan K-J, Spechler PA, Orr C, Banaschewski T, et al. Brain regions related to impulsivity mediate the effects of early adversity on antisocial behavior. Biological Psychiatry. 2016 doi: 10.1016/j.biopsych.2015.12.027. [DOI] [PubMed] [Google Scholar]
- Maliphant R, Watkins C, Davies J. Disruptive behaviour in non-referred mainstream school children, aged seven to nine: a psychophysiological contribution. Educational Psychology. 2003;23:437–455. [Google Scholar]
- Mezzacappa E, Tremblay RE, Kindlon D, Saul JP, Arseneault L, Seguin J, et al. Anxiety, antisocial behavior, and heart rate regulation in adolescent males. Journal of Child Psychology and Psychiatry. 1997;38:457–469. doi: 10.1111/j.1469-7610.1997.tb01531.x. [DOI] [PubMed] [Google Scholar]
- Mills JF, Kroner DG, Hemmati T. The measures of criminal attitudes and associates (MCAA) the prediction of general and violent recidivism. Criminal Justice and Behavior. 2004;31:717–733. [Google Scholar]
- Miskovic V, Schmidt LA, Georgiades K, Boyle M, MacMillan HL. Stability of resting frontal electroencephalogram (EEG) asymmetry and cardiac vagal tone in adolescent females exposed to child maltreatment. Developmental Psychobiology. 2009;51:474–487. doi: 10.1002/dev.20387. [DOI] [PubMed] [Google Scholar]
- Moffitt TE. Juvenile delinquency and attention deficit disorder: boys’ developmental trajectories from age 3 to age 15. Child Development. 1990;61:893. doi: 10.1111/j.1467-8624.1990.tb02830.x. [DOI] [PubMed] [Google Scholar]
- Moffitt TE, Caspi A. Childhood predictors differentiate life-course persistent and adolescence-limited antisocial pathways among males and females. Development and Psychopathology. 2001;13:355–375. doi: 10.1017/s0954579401002097. [DOI] [PubMed] [Google Scholar]
- Monahan KC, Steinberg L, Cauffman E. Affiliation with antisocial peers, susceptibility to peer influence, and antisocial behavior during the transition to adulthood. Developmental Psychology. 2009;45:1520–1530. doi: 10.1037/a0017417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murray-Close D, Rellini AH. Cardiovascular reactivity and proactive and reactive relational aggression among women with and without a history of sexual abuse. Biological Psychology. 2012;89:54–62. doi: 10.1016/j.biopsycho.2011.09.008. [DOI] [PubMed] [Google Scholar]
- Murray-Close D, Han G, Cicchetti D, Crick NR, Rogosch FA. Neuroendocrine regulation and physical and relational aggression: the moderating roles of child maltreatment and gender. Developmental Psychology. 2008;44:1160. doi: 10.1037/a0012564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Musser ED, Galloway-Long HS, Frick PJ, Nigg JT. Emotion regulation and heterogeneity in attention-deficit/hyperactivity disorder. Journal of the American Academy of Child & Adolescent Psychiatry. 2013;52:163–171.e2. doi: 10.1016/j.jaac.2012.11.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ortiz J, Raine A. Heart rate level and antisocial behavior in children and adolescents: a meta-analysis. Journal of the American Academy of Child & Adolescent Psychiatry. 2004;43:154–162. doi: 10.1097/00004583-200402000-00010. [DOI] [PubMed] [Google Scholar]
- Pine DS, Wasserman GA, Miller L, Coplan JD, Bagiella E, Kovelenku P, et al. Heart period variability and psychopathology in urban boys at risk for delinquency. Psychophysiology. 1998;35:521–529. doi: 10.1017/s0048577298970846. [DOI] [PubMed] [Google Scholar]
- Pluess M. Individual differences in environmental sensitivity. Child Development Perspectives. 2015;9:138–143. [Google Scholar]
- Porges SW. Orienting in a defensive world: mammalian modifications of our evolutionary heritage. A polyvagal theory Psychophysiology. 1995;32:301–318. doi: 10.1111/j.1469-8986.1995.tb01213.x. [DOI] [PubMed] [Google Scholar]
- Porges SW. The polyvagal perspective. Biological Psychology. 2007;74:116–143. doi: 10.1016/j.biopsycho.2006.06.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raine A, Mellingen K, Liu JH, Venables P, Mednick SA. Effects of environmental enrichment at ages 3-5 years on schizotypal personality and antisocial behavior at ages 17 and 23 years. American Journal of Psychiatry. 2003;160:1627–1635. doi: 10.1176/appi.ajp.160.9.1627. [DOI] [PubMed] [Google Scholar]
- Rogeness GA, Cepeda C, Macedo CA, Fisher C, Harris WR. Differences in heart rate and blood pressure in children with conduct disorder, major depression, and separation anxiety. Psychiatry Research. 1990;33:199–206. doi: 10.1016/0165-1781(90)90074-f. [DOI] [PubMed] [Google Scholar]
- Ross SR, Moltó J, Poy R, Segarra P, Pastor MC, Montañés S. Gray’s model and psychopathy: BIS but not BAS differentiates primary from secondary psychopathy in noninstitutionalized young adults. Personality and Individual Differences. 2007;43:1644–1655. [Google Scholar]
- Scarpa A, Ollendick TH. Community violence exposure in a young adult sample: III. Psychophysiology and victimization interact to affect risk for aggression. Journal of Community Psychology. 2003;31:321–338. [Google Scholar]
- Scarpa A, Raine A. The psychophysiology of child misconduct. Pediatric Annals. 2004;33:296–304. doi: 10.3928/0090-4481-20040501-08. [DOI] [PubMed] [Google Scholar]
- Scarpa A, Tanaka A, Haden S. Biosocial bases of reactive and proactive aggression: the roles of community violence exposure and heart rate. Journal of Community Psychology. 2008;36:969–988. [Google Scholar]
- Scarpa A, Haden SC, Tanaka A. Being hot-tempered: autonomic, emotional, and behavioral distinctions between childhood reactive and proactive aggression. Biological Psychology. 2010;84:488–496. doi: 10.1016/j.biopsycho.2009.11.006. [DOI] [PubMed] [Google Scholar]
- Schmeck K, Poustka F. Psychophysiological vulnerability of children with externalizing symptoms. Poster session presented at the annual meeting of the American Academy of Child and Adolescent Psychiatry; New Orleans. 1995. [Google Scholar]
- Schwab-Stone ME, Shaffer D, Dulcan MK, Jensen PS, Fisher P, Bird HR, et al. Criterion validity of the NIMH diagnostic interview schedule for children version 2.3 (DISC-2.3) Journal of the American Academy of Child and Adolescent Psychiatry. 1996;35:878–888. doi: 10.1097/00004583-199607000-00013. [DOI] [PubMed] [Google Scholar]
- Selig JP, Preacher KJ. Mediation models for longitudinal data in developmental research. Research in Human Development. 2009;6:144–164. [Google Scholar]
- Shaffer D, Fisher P, Lucas CP, Dulcan MK, Schwab-Stone ME. NIMH diagnostic interview schedule for children version IV (NIMH DISC-IV): description, differences from previous versions, and reliability of some common diagnoses. Journal of the American Academy of Child & Adolescent Psychiatry. 2000;39:28–38. doi: 10.1097/00004583-200001000-00014. [DOI] [PubMed] [Google Scholar]
- Sherwood A, Allen MT, Fahrenberg J, Kelsey RM, Lovallo WR, Doornen LJ. Methodological guidelines for impedance cardiography. Psychophysiology. 1990;27:1–23. doi: 10.1111/j.1469-8986.1990.tb02171.x. [DOI] [PubMed] [Google Scholar]
- Sijtsema JJ, Veenstra R, Lindenberg S, van Roon AM, Verhulst FC, Ormel J, Riese H. Mediation of sensation seeking and behavioral inhibition on the relationship between heart rate and antisocial behavior: the TRAILS study. Journal of the American Academy of Child & Adolescent Psychiatry. 2010;49:493–502. doi: 10.1097/00004583-201005000-00010. [DOI] [PubMed] [Google Scholar]
- Simons RL, Lei MK, Stewart EA, Beach SRH, Brody GH, Philibert RA, Gibbons FX. Social adversity, genetic variation, street code, and aggression: a genetically informed model of violent behavior. Youth Violence and Juvenile Justice. 2012;10:3–24. doi: 10.1177/1541204011422087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tarvainen MP, Niskanen J-P, Lipponen JA, Ranta-aho PO, Karjalainen PA. Kubios HRV–heart rate variability analysis software. Computer Methods and Programs in Biomedicine. 2014;113:210–220. doi: 10.1016/j.cmpb.2013.07.024. [DOI] [PubMed] [Google Scholar]
- Thayer JF, Sternberg E. Beyond heart rate variability. Annals of the New York Academy of Sciences. 2006;1088:361–372. doi: 10.1196/annals.1366.014. [DOI] [PubMed] [Google Scholar]
- Van Hulle CA, Corley R, Zahn-Waxler C, Kagan J, Hewitt JK. Early childhood heart rate does not predict externalizing behavior problems at age 7 years. Journal of the American Academy of Child & Adolescent Psychiatry. 2000;39:1238–1244. doi: 10.1097/00004583-200010000-00010. [DOI] [PubMed] [Google Scholar]
- Van Voorhees E, Scarpa A. Psychophysiological variables in childhood proactive and reactive aggression. Psychophysiology. 2002;39:S82. [Google Scholar]