

Abstract
Participatory intervention approaches that are embedded in existing organizational structures may improve the efficiency and effectiveness of organizational interventions, but concrete tools are lacking. In the present article, we use a realist evaluation approach to explore the role of kaizen, a lean tool for participatory continuous improvement, in improving employee well-being in two cluster-randomized, controlled participatory intervention studies. Case 1 is from the Danish Postal Service, where kaizen boards were used to implement action plans. The results of multi-group structural equation modeling showed that kaizen served as a mechanism that increased the level of awareness of and capacity to manage psychosocial issues, which, in turn, predicted increased job satisfaction and mental health. Case 2 is from a regional hospital in Sweden that integrated occupational health processes with a pre-existing kaizen system. Multi-group structural equation modeling revealed that, in the intervention group, kaizen work predicted better integration of organizational and employee objectives after 12 months, which, in turn, predicted increased job satisfaction and decreased discomfort at 24 months. The findings suggest that participatory and structured problem-solving approaches that are familiar and visual to employees can facilitate organizational interventions.
Keywords: distributed cognitions, lean, mental health, participatory interventions, psychosocial risk management, work environment
Introduction
The gold standard for intervention evaluation has been the randomized controlled trial. This type of evaluation, however, merely answers the question of whether or not an intervention worked (Nielsen, 2013). Posing only this relatively simple question may partly explain why we still understand little about the processes and tools that may facilitate successful intervention outcomes. Realist evaluation (Pawson, 2013) may offer a valuable way forward. A central aspect of realist evaluation involves answering the complex question of ‘what works for whom in which circumstances?’ Realist evaluation seeks to answer this question by studying how the mechanisms of an intervention work (what makes it work?) in a certain context to bring about certain outcomes in what are also known as Context-Mechanism-Outcome (CMO) configurations (Pawson, 2013; Pawson and Tilley, 1997). Thus, context is not viewed as a confounding influence that should be controlled, but rather as a factor that influences how the intervention brings about its outcome through certain mechanisms. CMO configurations are central to realist evaluation as they allow development and test of coherent theories about context, mechanisms and outcomes. According to realist evaluation, these cannot be tested in separate hypotheses but need to be understood in terms of how they relate to each other (Nielsen and Miraglia, in press; Pawson and Manzano-Santaella, 2012). In the present study, we apply the principles of realist evaluation using two cluster-randomized controlled organization-level interventions to explore how kaizen, a tool for participatory, continuous improvement used in lean management, can be used in psychosocial risk management to improve employee well-being, broadly defined as both job satisfaction and health (Danna and Griffin, 1999).
In the first study, we develop and test a CMO configuration to explore the context (a national postal service with experience using kaizen boards) in which an organizational, participatory intervention using kaizen boards as a tool to implement and evaluate actions (mechanism) is implemented to enhance participants’ ability to manage psychosocial issues and improve employee well-being (outcomes). The second study is set in a hospital that had implemented kaizen two years prior to the intervention. Because the hospital units varied in the degree to which they had implemented kaizen, kaizen work was seen as a contextual factor that varied across units. We therefore followed Dahler-Larsen’s (2001) recommendation to consider context as a local and dynamic phenomenon.
The present article contributes to the literature in three ways. First, the study addresses Nielsen’s (2013) call to explore different participatory processes and the tools that organizations may use to facilitate them. To the best of our knowledge, only one study has done this previously – a qualitative study showing that visualization tools helped keep up momentum by acting as a reminder for the intervention activities (Ipsen et al., 2015). In the present article, we expand this finding by exploring the role of a visualization tool (kaizen) already in use in participating organizations. In this way, we make a second contribution by addressing the call to create alignment between employee and organizational objectives (von Thiele Schwarz and Hasson, 2013) and to integrate participatory organizational interventions with existing structures and procedures (Zoni and Lucchini, 2012).
Third, it has been argued that the effects of lean, as well as the use of lean tools such as kaizen, on employee well-being deserve further attention (Bamber et al., 2014). A review of the effects of lean on employee well-being provides inconclusive evidence as to whether lean has a positive or a negative impact on employee well-being (Hasle et al., 2012). A possible explanation for the inconclusive findings is that lean consists of different practices and tools, each of them with potentially different influences. Thus, rather than investigating the relationship between the broader construct of lean and employee well-being, we explore the role of a specific tool, kaizen, as a means for improving employee well-being. By using two different studies, we are further able to investigate the role of kaizen used in two different ways: as a mechanism for the implementation and evaluation of action plans (Study 1) and as a preexisting, contextual factor (Study 2).
Is lean mean?
Lean is a management or production philosophy (or a theory, method or tool for improvement, as it has also been called) that stems from the Japanese manufacturing industry and has spread across Europe (Womack et al., 2007). Lean is a multifaceted approach focused on creating value for the end costumer, reducing unnecessary activities (i.e. waste), and focusing on continuous improvements, set-up time reduction, just-in-time production, failure prevention and production leveling (Pettersen, 2009). The impact of lean in general (McCann et al., 2015; Niepcel and Molleman, 1998) and on employee well-being in particular has been disputed (Hasle, 2014). Some studies have suggested that there is a negative relationship, in that lean leads to a slimmer organization, increased pace and reduced job variation, thereby threatening employee well-being (see, for example, Hasle et al., 2012; Parker, 2003). Others have indicated that lean is related to increased decision latitude, learning and involvement in changes in the workplace and, consequently, to increased employee well-being (Brännmark and Holden, 2013; Dellve et al., 2015; Ståhl et al., 2015). One reason for the inconsistent findings is that definitions and operationalizations vary between studies (Pettersen, 2009). As a result, the conclusions are based on very different practices, some which may affect job resources and others job demands, with different effects on employee well-being (Cullinane et al., 2014). Answering the question of whether or not lean is mean may therefore be futile. Instead, asking how specific lean tools relate to employee well-being may be one way forward.
Kaizen as a participatory, systematic lean approach to improving employee well-being
In the present study, we focus on one of the most widely used lean approaches: kaizen (Pettersen, 2009; Radnor et al., 2012). Kaizen is a structured, iterative and participatory approach for making continuous improvement (Jacobson et al., 2009). This approach converges with recommendations from the organizational intervention literature (Nielsen et al., 2010a), but to date only a few studies have investigated the relationship between kaizen and employee outcomes directly, indicating that kaizen may be positively associated with employee well-being (Cheser, 1998; García et al., 2014). In kaizen, one of the main reasons for engaging employees in continuous improvement is the assumption that the people closest to the work process are best suited to quickly identify areas in need of improvement and, consequently, implement action plans (Ulhassan et al., 2015).
Both the organizational intervention literature and the kaizen literature recommend systematic, iterative problem-solving over a period of time (i.e. cycles of systematic observation, measurement and change in work procedures and practices that are modified and evaluated). The difference is that in kaizen the cycles are much shorter than in organizational interventions; in kaizen, full cycles – including planning, acting, testing and evaluating – are proposed to be completed in days or weeks rather than months or years (Haun et al., 2015), which often is the case in organizational interventions (Nielsen et al., 2010a). This suggests that kaizen may be a tool for organizational interventions that can speed up the process and build momentum for continuous change.
The realization of a participatory problem-solving approach through visual management
Kaizen also has the advantage of using concrete tools and artifacts to facilitate the participatory, iterative problem-solving process, which is a feature that has been called for but rarely tested in the intervention literature (Nielsen et al., 2010b). Kaizen uses visual management tools to display the process visually, allowing employees to easily view the process (Aherne and Whelton, 2010), thereby facilitating participation (Ulhassan et al., 2015). Based on the theory of distributed cognition, visualization is a physical representation of the participatory problem-solving process that enables shared awareness of the process and issues at hand (Hutchins, 1995). Cognitions are embedded in the environment through social (i.e. collaborative) and technological means (i.e. artifacts). According to the distributed cognition theory, kaizen is more than the sum of its parts (the individuals and the tools). Instead, its potential is realized through its ability to create participation (i.e. interaction between individuals) and interaction between individuals and artifacts (the kaizen boards), allowing knowledge to be spread across time and space (Hollan et al., 2000). Kaizen boards can thus promote communication and interaction for both those meeting face to face around the kaizen board and individuals who are distant in space or time (Hutchins, 2000; Parry and Turner, 2006). Because it is a neutral medium, it may also facilitate the social process by mitigating tensions between employees (Riley et al., 2007). In sum, we suggest that kaizen may be a useful tool for psychosocial risk management interventions based on its participatory and problem-solving approach and because it provides a means for physically representing the intervention process, which increases its visibility and, hence, its presence in daily practice.
Integration of kaizen and psychosocial risk management
Overall, for the reasons outlined above, we suggest that kaizen may be directly related to better employee well-being but that kaizen may also have an indirect effect on employee well-being if it is used as a means to integrate psychosocial risk management, and interventions aimed at changing the way work is organized, designed and managed (Holden, 2011; Sainfort et al., 2001). Ikuma et al. (2010) found that integrating safety management with kaizen resulted in fewer hazards, improved safety and better productivity. It has also previously been shown that integrating psychosocial risk management (including both health protection and health promotion) with kaizen can have positive effects on employees’ work ability and self-rated productivity (von Thiele Schwarz et al., 2015). Overall, using preexisting tools such as kaizen for psychosocial interventions may have several specific benefits, including capitalizing on employees’ familiarity with the tools and minimizing the burden associated with using parallel systems and processes (Smith, 2002).
The person–job fit theory (Kristof-Brown et al., 2005) provides a theoretical basis for understanding why integrative approaches may have positive effects above and beyond those of kaizen alone. The main objective of kaizen is generally to improve organizational outcomes (Haun et al., 2015). Using kaizen as a means to improve the way work is organized, designed and managed encourages mutual consideration of organizational and employee objectives. This may promote improved person–environment fit regarding both the fit between environment supplies and employee values and between environmental demands and employee abilities (Edwards, 1996). Given that the supplies–values fit has been linked to employee dissatisfaction and the demands–abilities fit to employee strain (Kristof-Brown et al., 2005), it can be argued that the person–environment fit provides a theoretical framework for linking the integration of organizational interventions with kaizen to employee well-being in terms of both attitudes toward the job (e.g. job satisfaction) and cognitive and emotional outcomes related to the experience of strain.
Study 1 Introduction
In the following section, we develop our CMO configuration for Study 1.
Study 1 Context
The context was the Danish Postal Service, which was undergoing changes owing to decreases in the amount of mail being sent and the privatization of parcel services, both of which were affecting employees’ working conditions and well-being. In 2012, a national representative survey found that mail delivery service workers scored low on their influence on how tasks are accomplished and on the extent to which they are involved in decisions concerning the work environment, and reported experiencing mental health problems (http://www.arbejdsmiljoforskning.dk/da/arbejdsmiljoedata). Together, these results suggested that an organizational intervention was needed in this context, in particular a participatory intervention that could help increase employee involvement.
A contextual factor above and beyond the occupational setting that may influence the intervention process is employee pre-intervention well-being (Nielsen and Abildgaard, 2013). Based on Hobfoll’s (1989) conservation of resources theory, we assume that employees with better well-being will have more individual resources, and be more likely to try to gain additional resources through engagement in an intervention (Nielsen and Randall, 2012). More specifically, we propose that employees who experience good mental health possess the necessary resources to engage in the intervention (i.e. to use kaizen boards as a mechanism to further improve their well-being). Similarly, overall levels of job satisfaction may lead employees to exert more effort and increase their involvement (Taris and Schreurs, 2009), possibly resulting in employees engaging more with kaizen boards. In support of these assumptions, Nielsen and Randall (2012) found that employees who were satisfied with their jobs before the intervention participated more in the intervention process, and employees who reported high levels of affective well-being, defined as degree of positive state of mind, prior to the intervention reported that more procedures had changed as a result of the intervention. In realist evaluation terms, we consider employee well-being to be both an outcome and a local, dynamic contextual factor that influences how the intervention plays out (i.e. the mechanism). Based on this line of argument, we hypothesize that:
Hypothesis 1a: Preexisting levels of mental health and job satisfaction will be positively associated with the use of kaizen boards.
Study 1 Mechanism
We propose that kaizen boards are a mechanism for ensuring a successful intervention outcome because they are a systematic, structured approach with which participants are familiar (von Thiele Schwarz et al., 2013). In our scenario, the postal service had used kaizen boards for a number of years. Study 1 employed a cluster-randomized controlled wait-list design. Both the first intervention group and the wait-list control group were supported by an internal consultant in the active phase. We compared the sustainable phase of the first intervention group (no longer supported by the internal consultant) and the active phase of the wait-list control group (supported by the internal consultant). This comparison allows us to explore whether the intervention was sustainable without the support of an internal consultant (Framke and Sørensen, 2015: Nielsen et al., 2010a). Thus, we hypothesize that:
Hypothesis 1b: The use of kaizen boards will bring about positive intervention outcomes through their ability to enhance participants’ awareness of and capability to manage their psychosocial work environment (i.e. improved psychosocial risk management; intermediate outcome), and this will be similar for both participatory approaches.
Study 1 Intermediate and distal outcomes
Pawson (2013) argued that it is necessary to identify both intermediate and distal outcomes. A crucial intermediate outcome of Study 1 may be improved awareness of and capability to manage psychosocial issues because employees and managers act as co-learners in an empowerment process (Mikkelsen, 2005) and engage in a collaborative problem-solving dialogue (Rosskam, 2009). A crucial distal outcome is employee well-being.
We included employees’ mental health and job satisfaction as distal outcomes reflecting employee well-being. Mental health was included because the mail delivery workers scored low on this measure in the national survey and mental health has previously been shown to improve following an organizational intervention (Bond and Bunce, 2001). Job satisfaction has also been found to improve following organizational interventions (Nielsen and Randall, 2012). We suggest that these outcomes may be the result of using particular tools that improve the management of psychosocial work environment issues. In addition to the positive experience related to the participatory process itself, this is likely to be related to actual changes in the psychosocial work environment (e.g. Mikkelsen, 2005; Rosskam, 2009). We do not, however, make predictions on specific improvements in working conditions because the participatory intervention was designed to allow improvement areas to vary by team (Holman and Axtell, 2016). This dispersion makes it difficult to study working conditions as a proximal outcome. Thus, Hypothesis 1c can be specified as follows:
Hypothesis 1c: The use of kaizen boards will bring about improvements in job satisfaction and mental health (employee well-being) through their ability to enhance participants’ awareness of and capability to manage their psychosocial work environment (i.e. improved psychosocial risk management).
Translating these hypotheses into a testable CMO-configuration, we propose the following CMO configuration:
Context-Mechanism-Outcome 1: In the context of the Danish Postal service and in light of pre-intervention well-being, the use of kaizen boards (mechanism) will bring about positive intervention outcomes (distal outcomes) because the boards enhance participants’ awareness of and capability to manage their psychosocial work environment (improved psychosocial risk management) (intermediate outcome).
Study 1 Methods
Study 1 Participants and procedure
The cluster-randomized controlled wait-list design consisted of a baseline with two follow-ups. A 12-month interval was selected to account for seasonal effects among workers who spend a substantial amount of their working time outdoors. After completion of the baseline questionnaire, the two geographical postal areas were randomly assigned to the first or second intervention groups. Randomization took place at the area level to minimize contamination. The areas had separate management and human resource departments, and the research team found no evidence of any contamination between the two groups. During the first year, Group 1 received the intervention supported by the internal consultant (active phase) while Group 2 remained on the wait list. After the first follow-up, Group 1 continued with the intervention but without the support of the internal consultant (the sustainable phase) while Group 2 entered the active phase. In the present study, we study the time between the two follow-ups (T1 to T2) because it was not until then that the use of kaizen boards was made a part of the intervention, in both groups. Kaizen boards were introduced as a result of learning from the active phase of Group 1. The aim was to improve employee ownership of the implementation of action plans by using existing tools.
Only mail delivery service workers were included in the study. They were organized in teams. In the first intervention group, 11 teams were included; in the second group nine teams participated. At the first follow-up (denoted Time 1), 148 employees in Group 1 (response rate 90%) and 215 in Group 2 (91%) completed the questionnaire. At the second follow-up (denoted Time 2), 140 employees in Group 1 (response rate 84%) and 137 in Group 2 (response rate 89%) completed the questionnaire. Downsizing took place during the intervention, which accounts for the reduced sample size. At the first time point, employees ranged from 19 to 78 years (mean Group 1: 42.2 years [SD 11.7]; Group 2: 46.0 years [SD 11.5]). In total, 45.2% were women (43.3% in Group 1 and 46.6% in Group 2). The average tenure in the current position was 16.1 years (13.6 years [SD 11.1] in Group 1 and 17.8 years [SD 10.6] in Group 2). There were no gender differences between the two groups (χ2 1, (N = 188) = .34, p > .05), but employees in Group 2 were significantly older (t(187) = −2.93, p < .05) and had longer tenure (t(183) = −3.78, p < .001). An attrition analysis was performed by running a multiple logistic regression where missingness was predicted by demographic and study variables at T1 (Goodman and Blum, 1996). The missingness was indeed non-random, with intervention group being the only significant predictor. This indicates that beyond the known non-random attrition owing to downsizing in one of the organizations, the other variables were not related to missingness.
Study 1 Intervention
The intervention was a participatory intervention involving the five phases of the problem-solving cycle: preparation, screening, action planning, implementation and evaluation (Nielsen et al., 2010a). Kaizen boards were used to monitor and evaluate changes, identifying whether changes had been successfully implemented, and had the desired outcomes in terms of improving well-being; that is, in the fourth and fifth phases of the intervention. Work teams were responsible for developing and following up on action plans. Thus, the intervention was at the team level. At the area level, steering groups were established to oversee the intervention process. These steering groups consisted of management and two employee representatives from each team. These steering groups agreed upon the strategies for implementing the intervention and monitored the overall progress of it. The internal occupational health consultant functioned as a facilitator at steering group meetings, supporting the development of the process. Kaizen boards were used to monitor implementation and to ensure integration with existing structures, avoid redundancy, and use tools with which the employees were familiar. More information about the project and additional analyses can be found in Abildgaard et al. (2016), Nielsen and Abildgaard (2012), Nielsen and Daniels (2016) and Nielsen et al. (2014).
Study 1 Measures
To measure use of kaizen boards as a mechanism, an index with two items was used: ‘My team leader has used the kaizen board to manage the action plans developed in project XX’ and ‘We have, as a team, used the kaizen board to manage the action plans developed in project XX.’ We included a tailored, seven-item scale measuring improved psychosocial risk management to assess awareness of and capability to manage the psychosocial work environment and to tap into the extent to which participants perceived they had experienced an increased focus on issues related to this area and their well-being, as well as the extent to which they felt there had been any changes in their ability to successfully manage such issues. An example of an item is the following: ‘In the past year, the dialogue concerning well-being and psychosocial risk management has improved.’ For both scales, a five-point Likert scale ranging from 1 = strongly disagree to 5 = strongly agree was used. Employee well-being is measured with two indicators. Mental health was measured using a five-item scale from Ware and Gandek (1998); an example item is the following: ‘Have you felt so down in the dumps that nothing could cheer you up?’ A six-point Likert scale ranging from 1 = not at all to 7 = all the time was used. To facilitate the interpretation of these scales, scale scores were converted to a 100-point scale where a high value indicated a positive outcome. Job satisfaction was measured using one item – ‘How satisfied are you with your job, all in all?’ – and was rated on a five-point Likert scale from 1 = very dissatisfied to 5 = very satisfied. Single-item job satisfaction measures have been found to be valid and reliable (Wanous et al., 1997).
Study 1 Analysis
Multigroup structural equation modeling (SEM) using a maximum likelihood estimation method was performed. The first question was whether a model was the same or different between groups (i.e. whether a proposed pattern of relationships was invariant across the two intervention groups). First, we tested whether the multilevel structure of the data (at the team level) influenced the relationship between the predictors and the outcomes using linear mixed models with the group variable (intervention/control) as a predictor and with random intercepts for teams to adjust for within-team dependence. Neither the variance in the random intercepts nor the effect of the intervention was significant, showing that the team level did not influence the results and, thus, that a multilevel approach was not needed. Next, we investigated whether the proposed causal structure, outlined in Figure 1, held up for both intervention groups (i.e. whether the proposed structural relationship was group-invariant). The fit of the models was evaluated using a chi-square root mean square error of approximation (RMSEA) and comparative fit index (CFI). RMSEAs lower than .05 were considered a close fit, and between .05 and .08 an acceptable fit. CFI values above .90 were considered an acceptable fit (Anderson and Gerbing, 1988). For all tests, the level of significance was set at .05. The analyses were conducted using SPSS 22.0 and Amos 22.0.
Figure 1.
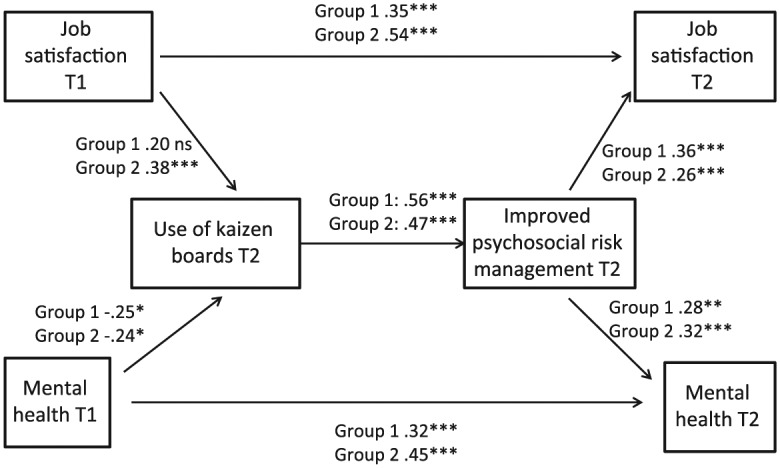
Standardized path coefficients for the two intervention groups for the no equality constraint multi-group model (Study 1).
T = time; * p < .05; ** p < .01; *** p < .001.
To test the validity of the hypothesized model, we first tested a general model with all parameters restricted to be equal across groups (pattern-same, invariant model for both intervention groups), thus including all individuals. Then the goodness of fit of the models for each of the two groups was investigated by relaxing the constraints on the parameters so that the models for the two groups were allowed to differ. Equality constraints were then separately imposed on single paths, one at a time. Each time the difference in the chi-square test statistic was calculated and the change in chi-square tested. A path that resulted in a significant change in the chi-square was considered a group-variant path (i.e. to differ between groups), and a path with a nonsignificant difference a group-invariant path (i.e. similar in the two groups).
Study 1 Results
Prior to multigroup SEM, the means, standard deviations and correlation matrix of the variables were calculated (Table 1), revealing significant correlations between the main variables in the expected direction.
Table 1.
Means, standard deviations and correlations with Cronbach’s alpha in the marginal for Study 1.
| Study variable | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1. Use of kaizen boards T2 | .44a* | |||||
| 2. Improved psychosocial risk management T2 | .52* | .89 | ||||
| 3. Mental health T1 | −.10 | −.01 | .75 | |||
| 4. Job satisfaction T1 | .16* | .24* | .41* | NA | ||
| 5. Mental health T2 | .17* | .30* | .38* | .22* | .82 | |
| 6. Job satisfaction T2 | .34* | .41* | .27* | .52* | .57* | NA |
| Total mean (SD) | 57.83 (19.7) | 60.36 (13.82) | 80.91 (15.4) | 4.04 (.78) | 76.37 (18.68) | 3.94 (.84) |
| Group 1 mean (SD) | 52.82 (17.94) | 56.53 (14.3) | 79.86 (15.5) | 4.07 (.81) | 73.48 (20.0) | 3.9 (.85) |
| Group 2 mean (SD) | 60.85 (20.16) | 62.72 (13.02) | 81.57 (15.3) | 4.03 (.76) | 78.23 (17.64) | 4.0 (.83) |
T = time; SD = standard deviation * p < .05; a Inter-item correlation. N T1 = 363, T2 = 277.
To test the overall CMO configuration (CMO1), the hypothesized path model (outlined in Figure 1) was tested using pooled data. The goodness-of-fit test showed a good fit with the data across all fit indexes (χ2 = 16.75 (6), p = .01; RMSEA = .06; CFI = .97). In a sequence of equality constraints separately imposed on each single path of the model, one at a time, the change in chi-square test statistic was compared with the model without imposing equality constraints. The results showed that the paths were group-invariant, and there was no overall difference between the models for the two groups. The only difference that emerged was between job satisfaction at the first follow-up and job satisfaction at the second follow-up. This path was significant in both groups, but the coefficient was significantly larger for Group 2. Thus, Hypothesis 1b was supported, indicating that the relationship between mechanisms and outcomes was similar regardless of whether the intervention was supported by an occupational health consultant or not.
Figure 1 also shows the standardized path coefficients for the no-equality-constraint multigroup model (χ2 = 18.65 (12), p = .097; RMSEA = 0.034; CFI = .981). As shown, all hypothesized paths, with one exception (the path from job satisfaction to the use of kaizen boards in Group 1), were significant in both groups. This provides partial support for our Hypothesis 1a (that baseline levels of mental health and job satisfaction would be positively associated with the use of kaizen boards), as better mental health was associated with more use of kaizen boards in both groups, and higher job satisfaction significantly related to increased use of kaizen boards, but only in Group 2. Hypothesis 1c was also confirmed: the use of kaizen boards predicted improved psychosocial risk management, and this, in turn, was related to higher job satisfaction and better mental health (after controlling for baseline levels).
Study 1 Discussion
Extending existing research on participatory organizational interventions (Nielsen and Randall, 2012), we explored whether the mechanism of using a specific tool to facilitate the fourth and fifth phases of a structured, participatory process (i.e. kaizen boards) brought about improved psychosocial risk management and whether this, in turn, improved employee well-being (outcome). We found support for our CMO configuration: a path model in which the use of kaizen boards predicted awareness of and ability to deal with psychosocial issues, which, in turn, predicted employee job satisfaction and mental health after controlling for baseline levels, was confirmed. Given that the mental health and job satisfaction overall seemed to decrease over time (albeit only significantly for mental health and only in one of the groups), the results further support the importance of using appropriate tools for implementing organizational-level interventions. Without the use of kaizen and the subsequent improved psychosocial risk management, outcomes may even worsen, in particular in a context of downsizing (de Jong et al., 2016). This may be related to disappointment with a lack of implementation (Nielsen et al., 2007). We also found support for the first subhypothesis (Hypothesis 1a) for three out of four relationships: good mental health was associated with increased use of kaizen boards in both groups, whereas job satisfaction was only positively associated with the use of kaizen in Group 2. We found a consistent structural pattern for both groups, linking the use of kaizen boards to improved psychosocial risk management (Hypothesis 1b), suggesting that the use of kaizen boards may be a successful mechanism regardless of whether an intervention is supported by an occupational health consultant. The results of Study 1 will be further discussed together with the results of Study 2 in the general discussion.
Study 2 Introduction
To extend the scope of Study 1, Study 2 set out to test the paths between kaizen work, integrating organizational and employee objectives and employee well-being (outcome) in a three-wave multigroup model. In the following, we develop our CMO configuration for Study 2.
Study 2 Context
In realist evaluations context is often understood as a setting. This approach has been criticized for focusing too much on context as something preexisting, stable, and already distributed, as indicated by the fact that the arrows in CMO configurations are unidirectional, only pointing away from the context, not back to it. Instead, it has been argued that context should be approached as local, dynamic phenomena (Blamey and Mackenzie, 2007). Defined in this way, context is something that varies, for example, between units of an organization, as well as, potentially, over time (Dahler-Larsen, 2001). In the present study, we consider the kaizen work as such a local, dynamic contextual factor within the broader context of a hospital that, two years prior to the intervention, had introduced kaizen as a process for continual improvements. Although the directives to use kaizen were the same for all units, in practice their use varied across units. Given that the intervention relied on the kaizen system as a tool for integration of psychosocial risk management, kaizen provided a potentially powerful contextual constraint. In Study 2, kaizen is therefore considered a context variable that may differ between groups as well as changing over time. Thus, we investigate the reciprocal relationships between context, mechanism and outcomes across all three time points.
Although the main objective of the present study is to elucidate the role of kaizen for employee well-being and the mechanisms involved, in line with the line of reasoning outlined in Study 1, we also consider the possibility of a reversed relationship between these factors. Based on this argument, we hypothesize the following:
Hypothesis 2a: Baseline levels of job satisfaction and discomfort will be positively associated with kaizen work and integration of organizational and employee objectives.
Study 2 Mechanism
We propose that the way kaizen is used (kaizen work) will lead to improvements in employee well-being (outcome) through the integration of organizational and employee objectives (mechanism). The rationale for the mechanism is based on the person–environment fit model: greater integration of organizational and employee objectives implies that employees will have better opportunities to develop continuous improvements that ensure their well-being. We investigate whether and how kaizen work differs between a control group and an intervention group, where both groups have the same context in terms of the objective to use kaizen for continuous improvement but only the intervention group used kaizen as a tool to integrate organizational and employee objectives in its improvement work. We therefore hypothesize the following:
Hypothesis 2b: The relationship between kaizen work and employee well-being will differ between the intervention and control group in that kaizen work will bring about positive intervention outcomes through greater integration of organizational and employee objectives in the intervention group.
Study 2 Outcomes
As in Study 1, we use job satisfaction as an employee well-being outcome. Our other well-being outcome is, similar to Study 1, an indicator of emotional load, though here measured as the experience of discomfort with work. Statistics Sweden uses this item as an emotional, negative response to work and as an early indicator of stress-related ill health, such as burnout (Gustafsson et al., 2008; Swedish Work Environment Authority & Statistics Sweden, 2013). We first address whether kaizen work is related to employee well-being even when it is not used explicitly for that purpose, as kaizen’s overall objective of reducing waste has the potential to both increase job satisfaction and decrease discomfort with work, not only because it may reduce unnecessary procedures and, thus, decrease workload but also because it may enable employees to experience that they create value and, thus, increase meaningfulness. We hypothesize the following:
Hypothesis 2c: Kaizen work at baseline will be directly related to subsequent improvement in employee well-being (i.e. improvements in job satisfaction and discomfort with work) in both the control and the intervention group.
The justification for job satisfaction being an outcome when an organizational intervention is set within a kaizen context follows the logic outlined in the introduction of Study 1. Job satisfaction is likely to increase as employees (in the intervention group) use kaizen for dual purposes – both organizational and employee objectives – through the mechanism of integrating these dual perspectives. Similarly, discomfort with work is likely to decrease when employees, in the local context of kaizen work and through the mechanism outlined above, are enabled to make changes in the way work is organized, designed and managed so that it better fits their personal needs, abilities and resources. Based on this, we hypothesize the following:
Hypothesis 2d: The relationship between kaizen work and employee well-being will differ between the intervention and control group in that the kaizen work will bring about improvements in job satisfaction and discomfort with work through greater integration of organizational and employee objectives in the intervention group.
Translating these hypotheses into a testable CMO-configuration, we propose the following CMO configuration:
Context-Mechanism-Outcome 2: Kaizen work and pre-intervention employee well-being (context) will be positively associated with employee well-being (outcome), and the effect will be greater when kaizen involves greater integration of organizational and employee objectives (mechanism).
Study 2 Methods
Study 2 Participants and procedure
Study 2 employed a cluster-randomized controlled design and was conducted in a county district hospital in Sweden employing about 500 individuals. All units working directly with patients were included (n = 12). Before the intervention, all units were matched based on size, type of care and preexisting kaizen work (the kaizen context). One unit in each pair was randomly assigned to the intervention group and the other to the control group. The data analyzed were collected at baseline (Time 0) and 12 (Time 1) and 24 (Time 2) months later. The intervention ran from month 3 onward, gradually becoming normal practice in the intervention units. The study was approved by the regional ethical committee. At each time point, all employees at the hospital, excluding hourly employees and those on long-term sick leave, received a Web-based questionnaire. At baseline (T0), 172 employees in the intervention group (90%) and 209 (91%) in the control group completed the questionnaire. At the first follow-up, one year later (T1), 175 employees in the intervention group (85%) and 192 in the control group (79%) completed the questionnaire, and at the second follow-up (T2), two years after T0, 171 in the intervention group (80%) and 204 in the control group (78%). The mean age was 45.8 years (SD 10.9) in the intervention group and 44.1 years (SD 12.2) in the control group. Regarding the gender distribution, 93.6% in the intervention group and 88.0% in the control group were women. Mean tenure at the current workplace was 19.5 years (SD 12.1) in the intervention group and 16.8 years (SD 12.1) in the control group. As in Study 1, we performed an attrition analysis to determine whether subject attrition led to non-random sampling over time, testing if demographic variables and the main study variables (kaizen, integrate, job satisfaction, discomfort with work and intervention group) could predict the probability of remaining in the sample over time (Goodman and Blum, 1996). Two multiple logistic regressions with a dummy-coded variable for stayers versus leavers as an outcome were performed, one including job satisfaction at T1 and the other including discomfort with work at T1 with the other variables being the same. The logistic regression including job satisfaction was significant (χ2 [6] = 41.3, p < .001, Nagelkerke R2 = .168). Integrate (B = –.028; p = .02) and age (B = −0.05, p < .001) were significant predictors of the probability of remaining in the sample. The logistic regression including discomfort with work was also significant (χ2 [6] = 45.4, p < .001, Nagelkerke R2 = .185). Integrate (B = –.031; p < .001), age (B = −0.049, p < .001) and discomfort with work (B = .011; p < .037) were significant predictors of the probability of remaining in the sample. This suggests a non-random attrition of study subjects over time, albeit not between conditions.
Study 2 Intervention
The intervention was organized so that integration would build on the kaizen work and contain a high level of employee participation. The intervention involved two main components. Similar to Study 1, the first component was to use the kaizen problem-solving approach to identify, plan, conduct and evaluate issues related to psychosocial risk management. The second component involved analyzing the possible consequences of all improvement suggestions for employee well-being, regardless of which area the problem/suggestion concerned. In each unit one or two employee representatives were responsible for supporting their colleagues in accomplishing this. The representatives were supported by human resources staff, who, in turn, received support from an external consultant. The control units kept working with kaizen for continuous improvements. As part of an organizational decision, this also involved using kaizen for the annual safety inspection, but beside that, they did not use kaizen to continuously identify and manage psychosocial risk management or analyze consequences for employee well-being. The overall effects of the intervention and an evaluation of intervention fidelity have been presented elsewhere (Augustsson et al., 2013; von Thiele Schwarz et al., 2015).
Study 2 Measures
All items were measured on a visual analogue scale with 0 (disagree completely) and 10 (agree completely) as endpoints. To assess preexisting kaizen work, a three-item, tailored scale was used. An example of an item is the following: ‘I work actively with the kaizen system.’ Cronbach’s alpha was .70 at T0. To assess integration of organizational and employee objectives, a tailored scale with four items was used. An example of an item is the following: ‘In my unit we integrate health promotion with kaizen.’ Cronbach’s alpha was .85 at T0. Employee well-being was measured with two indicators. Global job satisfaction was measured using a three-item scale from Hellgren et al. (1997). A sample item is the following: ‘I feel satisfied with my work.’ Cronbach’s alpha was 94.4. Discomfort with work was measured using a single item: ‘Do you sometimes feel uneasy on your way to work?’ High levels of discomfort have been shown to predict higher cortisol levels, and the item has been suggested to indicate lack of recovery from work-stress-related health problems in healthy adults (Gustafsson et al., 2008). As such, it is used by Statistics Sweden in its biannual work environment survey (Swedish Work Environment Authority & Statistics Sweden, 2013).
Study 2 Statistical analysis
Study 2 set out to test the hypothesized relationship between the kaizen work, degree of integration and well-being outcomes (see Figures 2a and 2b). Using the approach outlined in Study 1, multigroup structural equation modeling was performed, testing whether the same structural model held equally for the intervention and the control groups.
Figure 2a and 2b.
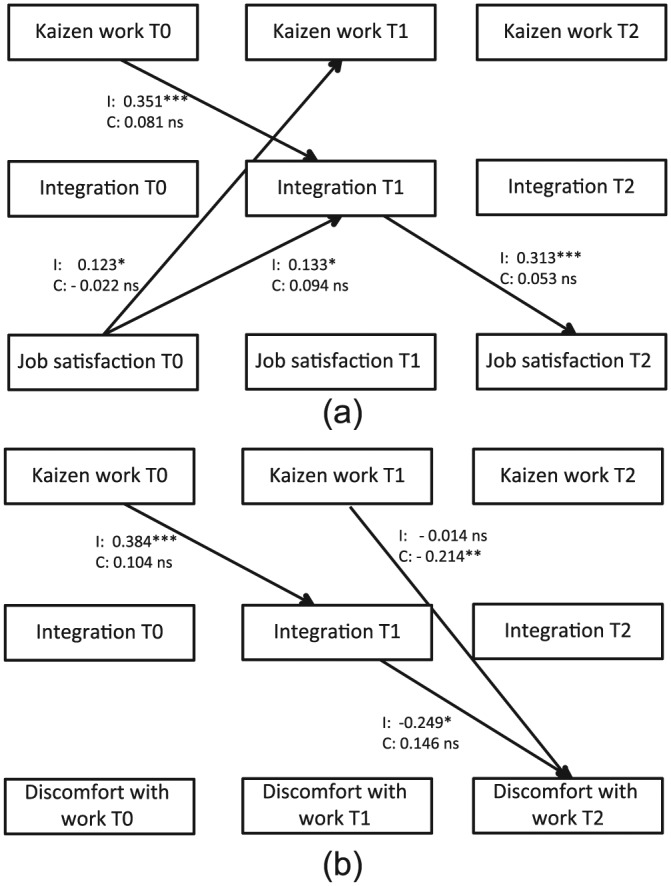
Standardized path coefficients for the significant hypothesized path for intervention (I) and control (C) groups for the no equality constraint multi-group model (Study 2).
T = time; * p < .05; ** p < .01; *** p < .001.
Study 2 Results
Prior to multigroup SEM, the means, standard deviations and correlation matrix of the variables were calculated (Table 2), revealing significant correlations between the main variables in the expected direction.
Table 2.
Study variables, means, standard deviations and inter-correlations for Study 2.
| Scale | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Kaizen work T0 | ||||||||||||
| 2. Integration T0 | .54* | |||||||||||
| 3. Job satisfaction T0 | .35* | .39* | ||||||||||
| 4. Discomfort T0 | −.18* | −.22* | −.54* | |||||||||
| 5. Kaizen work T1 | .71* | .44* | .31* | −.15* | ||||||||
| 6. Integration T1 | .46* | .58* | .34* | −.10 | .63* | |||||||
| 7. Job satisfaction T1 | .21* | .23* | .60* | −.38* | .36* | .43* | ||||||
| 8. Discomfort T1 | −.05 | −.06 | −.30* | .36* | −.18* | −.22* | −.59* | |||||
| 9. Kaizen work T2 | .62* | .41* | .33* | −.10 | .77* | .54* | .34* | −.16* | ||||
| 10. Integration T2 | .40* | .57* | .32* | −.06 | .54* | .77* | .34* | −.17* | .66* | |||
| 11. Job satisfaction T2 | .27* | .30* | .51* | −.31* | .41* | .45* | .61* | −.42* | .41* | .47* | ||
| 12. Discomfort T2 | −.14* | −.11 | −.29* | .38* | −.29* | −.23* | −.46* | .52* | −.27* | −.28* | −.61 | |
| Total mean (SD) | 59.07 (20.8) | 52.46 (18.7) | 76.18 (19.1) | 26.69 (25.4) | 60.07 (21.0) | 58.64 (19.6) | 77.27 (17.0) | 25.54 (24.4) | 58.0 (21.5) | 53.99 (22.7) | 74.47 (20.3) | 31.64 (27.9) |
| Intervention mean (SD) | 57.77 (19.6) | 52.08 (17.0) | 78.52 (17.5) | 23.91 (22.0) | 58.39 (20.9) | 60.56 (18.2) | 78.02 (16.34) | 25.42 (23.7) | 59.0 (19.6) | 57.15 (22.3) | 76.09 (20.4) | 30.68 (26.9) |
| Control mean (SD) | 60.15 (21.7) | 52.77 (20.0) | 74.24 (20.2) | 29.01 (27.8) | 61.61 (21.1) | 56.89 (20.7) | 76.59 (17.658) | 25.64 (25.1) | 57.14 (23.0) | 51.3 (22.9) | 73.14 (20.2) | 32.44 (28.7) |
T = time; SD = standard deviation; * p < .05. N T1 = 381, T2 = 367, T3 = 375.
To test the CMO configuration (CMO2), a path model for the relationship – from kaizen at all time points to integration and outcomes at all (future) time points, from integration to kaizen and outcomes at all future time points, and from outcomes to kaizen and integration at all future time points – was investigated using pooled data for each outcome separately (job satisfaction and discomfort with work). The models provided an excellent fit with the data (job satisfaction χ2 = 2.79 (6), P = .84; RMSEA < .001; CFI > .999; discomfort with work χ2 = 5.39 (6), p = .50; RMSEA < .001; CFI > .999). This provided overall support for the CMO configuration. Next, in a sequence of equality constraints imposed on each single path of the model, the change in the chi-square test statistic was compared with the model with no equality constraints imposed. This comparison showed that there were paths that were not group-invariant. For both job satisfaction and discomfort with work, the path from kaizen work at T0 to integration at T1 and the path from integration at T1 to the outcomes at T2 differed between the intervention and the control groups. For discomfort with work there was also a significant between-group difference in the relationship between discomfort with work at T1 and discomfort at T2. In sum, there was a difference between the intervention and the control groups in how kaizen work related to integration and the outcomes job satisfaction and discomfort with work, thus supporting Hypothesis 2b.
Figure 2a shows the standardized path coefficients for the hypothesized paths for a no-equality-constraint multigroup model for job satisfaction (χ2 = 8.79 (12), p < .720; RMSEA < .001; CFI = .999), while Figure 2b displays the results for discomfort with work (χ2 = 8.48 (12), p < .001; RMSEA < .001; CFI = .999). For job satisfaction, the only paths that were significant in the control group were the autocorrelations. For discomfort with work, in addition to the autocorrelations, there was a significant path from kaizen at T1 to discomfort with work at T2, showing that more kaizen work was related to lower levels of discomfort with work. For the intervention group, in addition to the autocorrelations, the hypothesized paths from kaizen work at T0 to integration at T1 and from integration at T1 to both outcomes at T2, respectively, were all significant. First, this shows that Hypothesis 2c, which proposed that kaizen work at baseline (context) would be directly related to subsequent improvement in employee well-being (outcome) in both the control and the intervention groups, was not supported. Second, it provides support for Hypothesis 2d, showing that more kaizen work was related to improved employee well-being, mediated by a higher degree of integration, in the intervention group. In addition, the results show that higher job satisfaction at T0, but not discomfort with work, was related to more kaizen work and a higher degree of integration at T1 in the intervention group only. This suggests a lack of support for Hypothesis 2a for discomfort with work but partial support for Hypothesis 2a for job satisfaction, whereas the finding that the level of job satisfaction at T1 predicted kaizen work and integration a year later (at T2) indicates reversed causation between job satisfaction and kaizen work and integration, respectively, under the intervention condition.
General discussion
Using a realist evaluation approach, the purpose of the present study was to expand previous research on participatory, organizational interventions by investigating how kaizen, a visual management tool, may have influenced the outcomes of two interventions where kaizen played different roles: as a specific mechanism for the implementation and evaluation of action plans (in Study 1) and as a preexisting, contextual factor influencing the level of integration (in Study 2). We first examined one CMO configuration, which showed that the use of kaizen boards (mechanism) had a positive influence on improvements in psychosocial risk management and, in turn, on employee well-being in terms of job satisfaction and mental health (outcomes) in the context of a national postal service that used kaizen boards to implement action plans. We then expanded this by examining another CMO configuration, outlining the relationships between kaizen work (context), the integration of organizational and employee objectives (mechanism), and employee outcomes in terms of job satisfaction and discomfort with work (outcomes) across three time points and with comparisons between an intervention group, which was explicitly asked to use a kaizen board for considering both organizational and employee objectives, and a control group. Study 2 showed that (i) kaizen work had a limited, positive, direct impact on employee well-being only for one outcome (discomfort with work), only at one time point (between the first and second follow-ups), and only in one group (the control group), and (ii) that the effect of kaizen work on employee well-being was unleashed when kaizen was explicitly used to integrate organizational and employee objectives. In sum, this improves our understanding of the relationship between kaizen and employee well-being by suggesting that in order to maximize the positive relationship between kaizen and employee well-being, organizational and employee objectives should be explicitly targeted within the kaizen system.
Kaizen as a mechanism and as a contextual precondition
In line with the theory of distributed cognition, kaizen, being a visual management tool, may increase visibility and, thus, awareness of psychosocial risk management, as well as expand the participatory process beyond those physically present at a certain time. Nevertheless, the results of Studies 1 and 2 indicate different pathways for kaizen. In Study 1, kaizen boards had been introduced prior to the intervention, and rather than introducing a new system for implementing and evaluating action plans produced as part of an organizational intervention, the kaizen boards were utilized. In this way, the use of kaizen boards became a mechanism whereby psychosocial issues could be managed. This mechanism led to improvements in employee well-being through improvements in psychosocial risk management, including increased influence and improved dialogue and opportunities for dealing with psychosocial issues. In Study 2, the intervention directly involved modifying how kaizen was used, from the preexisting kaizen used exclusively for the continuous improvement of organizational objectives to kaizen used for both organizational and employee needs. In this way, kaizen was approached as a local, dynamic contextual factor helping to explain the specific conditions under which an intervention has an effect. Thus, the two studies combined indicate that kaizen can (i) improve psychosocial risk management when used to implement and evaluate actions plans, and (ii) be modified to address employee objectives (including risk management and health promotion).
Contextual preconditions
In the present studies, we approached context in two different ways: in Study 1, we took the traditional realist approach and considered context as a preexisting, stable contextual factor; and in Study 2, we included the use of kaizen as a contextual factor that varied, thus approaching context as a dynamic, local (in this case even individual) phenomenon. In both studies we included preexisting levels of well-being; that is, we approached well-being as a contextual factor that could influence the outcomes. The results demonstrate that some preintervention levels of well-being seem to affect outcomes. In both studies high job satisfaction had a positive influence on the other variables (though in Study 2, only in the intervention group). In Study 1, mental health was related to more use of kaizen, whereas in Study 2, discomfort with work had no influence. Overall, the results show that our understanding of what works for whom under what circumstances can increase if we (i) consider preexisting levels of well-being as a contextual factor and (ii) expand the view of context to encompass dynamic and local factors that vary across individuals and over time.
Implications for research and practice
Together, our two studies emphasize the importance of using specific tools, in this case kaizen, a lean management tool, to trigger improvements in psychosocial risk management and, subsequently, better well-being. Our results suggest that occupational health consultants and organizations should explore which tools in their existing performance management systems may be expanded or adapted to also encompass psychosocial risk management. Previous studies have highlighted the importance of using occupational health consultants to ensure a smooth intervention process (Sørensen and Holman, 2014). Our results, however, indicate that when using an existing management tool (i.e. kaizen), positive intervention outcomes may be achieved regardless of whether the process is facilitated by an occupational health consultant or not. One interpretation is that the kaizen boards may also have some of the functions that occupational health consultants have; for example, as an antecedent for completing action plans, maintaining a structured process, and so forth. This finding also indicates that the use of existing organization-specific tools may be a way to facilitate internal capacity-building.
This study also offers some insight into the relationship between lean and employee well-being – an area that has been understudied (Bamber et al., 2014). First, the findings show that studying a specific lean tool, in this case kaizen, may be a way forward for understanding the implications of lean for employee well-being. Second, we went beyond investigating the relationship between a specific lean tool and employee well-being by also looking at the way the tool was used. Specifically, we investigated how well-being was affected if used explicitly as a means to work with psychosocial work environment issues. Our findings imply that, even though looking at how specific lean tools relate to employee well-being may help untangle the relationship between lean and employee well-being, looking at how and for what purposes the tools are used may be even more helpful.
Our studies also suggest the circumstances in which participatory organizational interventions may have their effects. In addition to using familiar visual tools that increase the visibility of psychosocial issues and opportunities to participate in managing them, Study 2 indicated that one important mechanism is an increased understanding of how employee and organizational objectives are interrelated. Such an understanding is important at all hierarchical levels of an organization because it provides a basis for more sensible decision-making that considers dual outcomes simultaneously.
Strengths and limitations
The study has several strengths. First, the realist evaluation approach, combined with multigroup structural equation modeling, is an innovative approach that enabled the complex question, ‘What works for whom in which circumstances?’ to be investigated in a systematic and structured way. Second, we included two studies with different intervention strategies in different countries with relatively large sample sizes. In addition to testing two different samples, we further tested two different groups within each sample: facilitated versus nonfacilitated intervention groups in Study 1; and intervention and control groups in Study 2. In this way, we found these relationships not only once but twice, under somewhat different circumstances, thus providing both novel evidence and replication of findings – something greatly needed in psychology (Open Science Collaboration, 2015). The use of different and shared outcomes in the two different interventions further increased the generalizability. Third, we utilized an analytical approach that allowed the integration of process evaluation (i.e. kaizen) in the outcome evaluation (Semmer, 2006). Fourth, we controlled for pretest levels on study variables, thereby ruling out threats to internal validity (Cook and Campbell, 1979).
Some limitations need to be considered. This includes only using self-report measures to capture outcomes. It could be argued that objective measures, for example, observations or behavioral indicators of well-being, should have been used, but this was not possible because of practical and ethical constraints. Moreover, although objective data in the form of actual kaizen documentation would have provided additional information, this was not feasible because kaizen documentation is done at the unit level, not the individual level, which was the unit of analysis in these studies. Furthermore, the objective of the interventions was to improve employees’ perceptions of their well-being, and therefore, self-reports were appropriate outcomes (Kompier and Kristensen, 2001). Using self-reports introduced the risk of common method bias. In general, this risk is greater for data from the same time point, for similar constructs and ratings, and for simple models (Chang et al., 2010). Thus, the use of longitudinal data in the present study decreased the possible influence of common method bias in it. The fact that the outcomes reflected respondents’ individual experiences (whereas the predictor reflected the workgroup level), and the use of a complex model that made it less likely that the individuals cognitively constructed the relationship between the variables, decreased the risk further.
Concurrently, the use of longitudinal data introduces the risk of attrition bias. This risk is likely to be inflated in organizational studies, as individuals’ participation is dependent on whether they remain in the organization or not. The larger the attrition between study points, the greater the risk for non-random attrition that has a meaningful influence on the results. The attrition analysis showed that in Study 1, where attrition was large, the only non-random factor influencing attrition was the already known group-difference owing to down-sizing in one of the organizations. On the other hand, there were indications of non-random attrition in Study 2, where attrition was low. Individuals who rated integration higher and were older were more likely to remain in the sample, introducing the risk of the results being more representative for this group. Nevertheless, the risk that the non-random attrition over time affects the main conclusions is mitigated by the fact that there was no difference in attrition between the intervention and the control group.
Moreover, in Study 1, the use of kaizen at T1 was not included in the study and, thus, could not be controlled for. This was because at this time point the decision to use kaizen boards as an implementation and evaluation strategy had not yet been made. In addition, job satisfaction in Study 1 and discomfort with work in Study 2 were single items, meaning that the reliability of these measures could not be investigated. Nevertheless, both these items have been previously validated (Gustafsson et al., 2008; Wanous et al., 1997), and including these measures made it possible to mirror two types of employee well-being outcomes – one related to job attitudes and one to mental health – across the two studies.
Conclusions
The present study establishes the importance of considering the use of specific tools, in this case kaizen, for implementing organizational interventions. We combined a realist evaluation with multigroup structural equation modeling and were thereby able to answer the question of what works for whom in which circumstances. We can conclude that when interventions occur in a context where employees use kaizen, and when kaizen boards are explicitly used to manage psychosocial work environment issues, there are positive intervention outcomes in the form of employee well-being. Thus, kaizen can either be a precondition for improvement in the integration of organizational and employee objectives or a mechanism that allows the implementation of action plans. In either case, kaizen has the potential to be a participatory tool that enables employees to interact and engage in psychosocial risk management and/or integration of organizational and employee objectives in a way that improves their well-being.
Acknowledgments
We would like to thank Maria Stage (Study 1) and Hanna Augustsson (Study 2) for their invaluable support in data collection and Zangin Zeebari for support in the statistical analysis.
Biography
Ulrica von Thiele Schwarz is a psychologist and associate professor in psychology. She co-leads the multi-disciplinary Procome research group at Medical Management Centre, Karolinska Institutet (KI), Stockholm, Sweden, and is the co-director for the Strategic Research Area in Care Sciences (SFO-V) at KI. Her research is focused on uncovering how to design, conduct and evaluate innovative improvement initiatives in organizations, and its effects on organizational and employee outcomes. Her current projects also include an exploration of the adaptation and adherence dilemma in the evidence-to-practice pathway. She is an associate editor of Health Service Management Research and has published her work in journals such as Journal of Occupational Health Psychology, Journal of Occupational and Environmental Medicine, Implementation Science and Safety Science. [Email: ulrica.schwarz@ki.se]
Karina M Nielsen is the Chair of Work and Organisational Psychology at the Institute of Work Psychology, Sheffield University Management School at the University of Sheffield, UK. She is a research affiliate at the CPH-NEW, USA and KI, Sweden. Her research interests lie within the changing organizations. She is particularly interested in the design, implementation and evaluation of organizational interventions and ways to develop methods to understand how and why such interventions succeed or fail. She is currently on the editorial boards of Human Relations, The Leadership Quarterly and Journal of Business and Psychology, and is an associate editor of Work & Stress. She has published her work in journals such as Human Relations, Work & Stress, The Leadership Quarterly and Journal of Occupational Health Psychology. [Email: k.m.nielsen@sheffield.ac.uk]
Terese Stenfors-Hayes, PhD, is assistant professor at Department of Learning, Informatics, Management and Ethics at Karolinska Institutet, Stockholm, Sweden. She is also Director of the Evaluation Unit at Karolinska Institutet. Her research focuses on research methods development and professional development for healthcare professionals. She is the section editor of BMC Medical Education and Associate Editor of The Clinical Teacher. [Email: terese.stenfors-hayes@ki.se]
Henna Hasson, PhD, is associate professor and a co-leader for the Procome research group at Medical Management Centre, Karolinska Institutet, Stockholm, Sweden. She is also Director of the Implementation Unit, at Center for Epidemiology and Community Medicine, Stockholm County Council. Her research focuses on intervention implementation and outcomes. Henna is currently running several international projects aiming to compare the impact of process and context factors across interventions and countries. She has published her work in journals such as Implementation Science, Work & Stress and Journal of Occupational and Environmental Medicine. [Email: Henna.Hasson@ki.se]
Footnotes
Funding: This research was supported by NOS-HS, the Joint Committee for the Nordic Research Councils for the Humanities and Social Sciences (grant number 219610/F10), Vinnvård (grant number VF13-008), Danish National Work Environment Research Fund (grant number 14-2009-09), and AFA Insurance (grant number 110094).
Contributor Information
Ulrica von Thiele Schwarz, Karolinska Institutet, Sweden, ulrica.schwarz@ki.se.
Karina M Nielsen, University of Sheffield, UK, k.m.nielsen@sheffield.ac.uk.
Terese Stenfors-Hayes, Karolinska Institutet, Sweden, terese.stenfors-hayes@ki.se.
Henna Hasson, Karolinska Institutet, Sweden, Henna.Hasson@ki.se.
References
- Abildgaard JS, Nielsen K, Saksvik PO. (2016) How to measure the intervention process? An assessment of qualitative and quantitative approaches to data collection in the process evaluation of organizational interventions. Frontiers in Psychology: Organizational Psychology 22(7): 1380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aherne J, Whelton J. (2010) Applying Lean in Healthcare: A Collection of International Case Studies. New York NY: Productivity Press. [Google Scholar]
- Anderson JC, Gerbing DW. (1988) Structural equation modelling in practice: A review and recommended two-step approach. Psychological Bulletin 103: 411–423. [Google Scholar]
- Augustsson H, von Thiele Schwarz U, Stenfors-Hayes T, Hasson H. (2013) Investigating variations in implementation fidelity of an organizational-level occupational health intervention. International Journal of Behavioural Medicine 22(3): 345–355. [DOI] [PubMed] [Google Scholar]
- Bamber G, Stanton P, Bartram T, Ballardie R. (2014) Human resource management, Lean processes and outcomes for employees: Towards a research agenda. The International Journal of Human Resource Management 25(21): 2881–2891. [Google Scholar]
- Blamey A, Mackenzie M. (2007) Theories of change and realistic evaluation peas in a pod or apples and oranges? Evaluation 13(4): 439–455. [Google Scholar]
- Bond F W, Bunce D. (2001) Job control mediates change in a work reorganization intervention for stress reduction. Journal of Occupational Health Psychology 6(4): 290–302. [PubMed] [Google Scholar]
- Brännmark M, Holden R. (2013) Packages of participation: Swedish employees’ experience of lean depends on how they are involved. IIE Transactions on Occupational Ergonomics and Human Factors 1(2): 93–108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chang SJ, Van Witteloostuijn A, Eden L. (2010) From the editors: Common method variance in international business research. Journal of International Business Studies 41(2): 178–184. [Google Scholar]
- Cheser R. (1998) The effect of Japanese Kaizen on employee motivation in US manufacturing. The International Journal of Organizational Analysis 6(3): 197–217. [Google Scholar]
- Cook T, Campbell D. (1979) Quasi-experimentation: Design & Analysis Issues for Field Settings. Boston MA: Houghton Mifflin. [Google Scholar]
- Cullinane S-J, Bosak J, Flood P, Demerouti E. (2014) Job design under lean manufacturing and the quality of working life: A job demands and resources perspective. The International Journal of Human Resource Management 25(21): 2996–3015. [Google Scholar]
- Dahler-Larsen P. (2001) From programme theory to constructivism on tragic, magic and competing programmes. Evaluation 7(3): 331–349. [Google Scholar]
- Danna K, Griffin R. (1999) Health and well-being in the workplace: A review and synthesis of the literature. Journal of Management 25(3): 357–384. [Google Scholar]
- de Jong T, Wiezer N, de Weerd M, et al. (2016) The impact of restructuring on employee well-being: A systematic review of longitudinal studies. Work & Stress 30(1): 91–114. [Google Scholar]
- Dellve L, Williamsson A, Strömgren M, et al. (2015) Lean implementation at different levels in Swedish hospitals: The importance for working conditions and stress. International Journal of Human Factors and Ergonomics 3(3–4): 235–253. [Google Scholar]
- Edwards J. (1996) An examination of competing versions of the person-environment fit approach to stress. Academy of Management Journal 39(2): 292–339. [Google Scholar]
- Framke E, Sørensen OH. (2015) Implementation of a participatory organisational-level occupational health intervention – focusing on the primary task. International Journal of Human Factors and Ergonomics 3: 254–270. [Google Scholar]
- García J, Maldonado A, Alvarado A, Rivera D. (2014) Human critical success factors for kaizen and its impacts in industrial performance. The International Journal of Advanced Manufacturing Technology 70(9–12): 2187–2198. [Google Scholar]
- Goodman JS, Blum TC. (1996) Assessing the non-random sampling effects of subject attrition in longitudinal research. Journal of Management 22: 627–652. [Google Scholar]
- Gustafsson K, Lindfors P, Aronsson G, Lundberg U. (2008) Relationships between self-rating of recovery from work and morning salivary cortisol. Journal of Occupational Health 50(1): 24–30. [DOI] [PubMed] [Google Scholar]
- Hasle P. (2014) Lean production – an evaluation of the possibilities for an employee supportive lean practice. Human Factors and Ergonomics in Manufacturing & Service Industries 24(1): 40–53. [Google Scholar]
- Hasle P, Bojesen A, Langaa Jensen P, Bramming P. (2012) Lean and the working environment: A review of the literature. International Journal of Operations & Production Management 32(7): 829–849. [Google Scholar]
- Haun J, Mothersell W, Motwani J. (2015) Implementing kaizen in the workplace: A case study. International Journal of Management & Behavioural Sciences (IJMBS) 6: 321–325. [Google Scholar]
- Hellgren J, Sjöberg A, Sverke M. (1997) Intention to quit: Effects of job satisfaction and job perceptions. In: Avallone F, Arnold J, De Witte K. (eds) Feelings Work in Europe. Milano: Guerini, 415–423. [Google Scholar]
- Hobfoll S. (1989) Conservation of resources: A new attempt at conceptualizing stress. American Psychologist 44(3): 513–525. [DOI] [PubMed] [Google Scholar]
- Holden R. (2011) Lean thinking in emergency departments: A critical review. Annals of Emergency Medicine 57(3): 265–278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hollan J, Hutchins E, Kirsh D. (2000) Distributed cognition: Toward a new foundation for human-computer interaction research. ACM Transactions on Computer-Human Interaction (TOCHI) 7(2): 174–196. [Google Scholar]
- Holman D, Axtell C. (2016) Can job redesign interventions influence a broad range of employee outcomes by changing multiple job characteristics? A quasi-experimental study. Journal of Occupational Health Psychology 21(3): 284–295. [DOI] [PubMed] [Google Scholar]
- Hutchins E. (1995) Cognition in the Wild. Cambridge MA: MIT Press. [Google Scholar]
- Hutchins E. (2000) Distributed cognition. In: Smeltzer NJ, Editor PB. (eds) International Encyclopedia of the Social and Behavioral Sciences. Amsterdam: Elsevier Science, 2068–2072. [Google Scholar]
- Ikuma L, Nahmens I, James J. (2010) Use of safety and lean integrated kaizen to improve performance in modular homebuilding. Journal of Construction Engineering and Management 137(7): 551–160. [Google Scholar]
- Ipsen C, Gish L, Poulsen S. (2015) Organizational-level interventions in small and medium-sized enterprises: Enabling and inhibiting factors in the PoWRS program. Safety Science 71: 264–274. [Google Scholar]
- Jacobson G, McCoin N, Lescallette R, Russ S, Slovis C. (2009) Kaizen: A method of process improvement in the emergency department. Academy Emergency Medicine 16(12): 1341–1349. [DOI] [PubMed] [Google Scholar]
- Kompier MA, Kristensen TS. (2001) Organizational work stress interventions in a theoretical, methodological and practical context. In: Dunham J. (ed.) Stress in the Workplace: Past, Present and Future. London and Philadelphia: Whurr Publishers. [Google Scholar]
- Kristof-Brown AL, Zimmerman RD, Johnson E. (2005) Consequences of individual’s fit at work: A meta-analysis of person-job, person-organization, person-group, and person-supervisor fit. Personnel Psychology 58: 281–342. [Google Scholar]
- McCann L, Hassard J, Granter E, Hyde P. (2015) Casting the lean spell: The promotion, dilution and erosion of lean management in the NHS. Human Relations 68(10): 1557–1578. [Google Scholar]
- Mikkelsen A. (2005) Methodological Challenges in the Study of Organizational Interventions in Flexible Organizations: Anthology for Kjell Grønhaug in Celebration of his 70th birthday. Bergen: Fagbokforlaget, 152–178. [Google Scholar]
- Nielsen K. (2013) Review article: How can we make organizational interventions work? Employees and line managers as actively crafting interventions. Human Relations 66(8): 1029–1050. [Google Scholar]
- Nielsen K, Abildgaard JS. (2012) The validation of a job crafting measure for blue collar workers. Work & Stress 26: 365–384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nielsen K, Abildgaard JS. (2013) Organizational interventions: A research-based framework for the evaluation of both process and effects. Work & Stress 27(3): 278–297. [Google Scholar]
- Nielsen K, Daniels K. (2016) The relationship between transformational leadership and sickness absenteeism: The role of presenteeism. Work & Stress 30: 193–208. [Google Scholar]
- Nielsen K, Miraglia M. (in press) Critical essay: What works for whom in which circumstances? On the need to move beyond the ‘what works?’ question in organizational intervention research. Human Relations. [Google Scholar]
- Nielsen K, Randall (2012) The importance of employee participation and perceptions of changes in procedures in a teamworking intervention. Work & Stress 26(2): 91–111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nielsen K, Randall R, Albertsen K. (2007) Participants’ appraisals of process issues and the effects of stress management interventions. Journal of Organizational Behavior 28(6): 793–810. [Google Scholar]
- Nielsen K, Randall R, Holten A-L, Gonzalez E R. (2010. a) Conducting organizational-level occupational health interventions: What works? Work & Stress 24(3): 234–259. [Google Scholar]
- Nielsen K, Taris T, Cox T. (2010. b) The future of organizational interventions: Addressing the challenges of today’s organizations. Work & Stress 24(3): 219–233. [Google Scholar]
- Nielsen K, Abildgaard JS, Daniels K. (2014) Putting context into organizational intervention design: Using tailored questionnaires to measure initiatives for worker well-being. Human Relations 67(2): 1537–1560. [Google Scholar]
- Niepcel W, Molleman E. (1998) Work design issues in lean production from a sociotechnical systems perspective: Neo-Taylorism or the next step in sociotechnical design? Human Relations 51(3): 259–287. [Google Scholar]
- Open Science Collaboration (2015) Estimating the reproducibility of psychological science. Science 349(6251): aac4716. [DOI] [PubMed] [Google Scholar]
- Parker SK. (2003) Longitudinal effects of lean production on employee outcomes and the mediating role of work characteristics. Journal of Applied Psychology 88(4): 620–634. [DOI] [PubMed] [Google Scholar]
- Parry GC, Turner CE. (2006) Application of lean visual process management tools. Production Planning & Control 17(1): 77–86. [Google Scholar]
- Pawson R. (2013) The Science of Evaluation: A Realist Manifesto. London: SAGE. [Google Scholar]
- Pawson RD, Manzano-Santaella A. (2012) A realist diagnostic workshop. Evaluation: International Journal of Theory, Research and Practice 18(2): 176–191. [Google Scholar]
- Pawson R, Tilley N. (1997) Realistic Evaluation. London: SAGE. [Google Scholar]
- Pettersen J. (2009) Defining lean production: Some conceptual and practical issues. The TQM Journal 21(2): 127–142. [Google Scholar]
- Radnor Z, Holweg M, Waring J. (2012) Lean in healthcare: The unfilled promise? Social Science & Medicine 74(3): 364–371. [DOI] [PubMed] [Google Scholar]
- Riley R, Forsyth R, Manias E, Iedema R. (2007) Whiteboards: Mediating professional tensions in clinical practice. Communication & Medicine 4(2): 165–175. [DOI] [PubMed] [Google Scholar]
- Rosskam E. (2009) Using participatory action research methodology to improve worker health. In: Schnall P, Dobson M, Rosskam E. (eds) Unhealthy Work: Causes, Consequences, Cures. New York, NY: Baywood Publishing Company, 211–229. [Google Scholar]
- Sainfort F, Karsh B-T, Booske B, Smith M. (2001) Applying quality improvement principles to achieve healthy work organizations. Joint Commission Journal on Quality and Patient Safety 27(9): 469–483. [DOI] [PubMed] [Google Scholar]
- Semmer N. (2006) Job stress interventions and the organization of work. Scandinavian Journal of Work, Environment and Health 32(6): 515–527. [DOI] [PubMed] [Google Scholar]
- Smith D. (2002) IMS: Implementing and Operating. London: BSI British Standards Institution. [Google Scholar]
- Sørensen OH, Holman D. (2014) A participative intervention to improve employee well-being in knowledge work jobs: A mixed-methods evaluation study. Work & Stress 28(1): 67–86. [Google Scholar]
- Ståhl A-CF, Gustavsson M, Karlsson N, Johansson G, Ekberg K. (2015) Lean production tools and decision latitude enable conditions for innovative learning in organizations: A multilevel analysis. Applied Ergonomics 47: 285–291. [DOI] [PubMed] [Google Scholar]
- Swedish Work Environment Authority & Statistics Sweden (2013) The work environment 2013. Arbetsmiljöstatistik [Work environment statistics] (2014: 3). Stockholm: Arbetsmiljöverket; Statistiska Centralbyrån [Swedish Work Environment Authority; Statistics Sweden]. [Google Scholar]
- Taris T, Schreurs P. (2009) Well-being and organizational performance: An organizational-level test of the happy-productive worker hypothesis. Work & Stress 23(2): 120–136. [Google Scholar]
- Ulhassan W, Von Thiele Schwarz U, Westerlund H, et al. (2015) How visual management for continuous improvement might guide and affect hospital staff: A case study. Quality Management in Healthcare 24(4): 222–228. [DOI] [PubMed] [Google Scholar]
- von Thiele Schwarz U, Hasson H. (2013) Alignment for achieving a healthy organization. In: Bauer GF, Jenny GJ. (eds) Salutogenic Organizations and Change. The Netherlands: Springer, 107–125. [Google Scholar]
- von Thiele Schwarz U, Stenfors-Hayes T, Augustsson H, Hasson H. (2013) Lean som utgångspunkt för hälsofrämjande arbete [Lean as a starting point for health promotion]. In: Pehr Sederblad (ed.) Lean i Arbetslivet [Lean in the working life]. Solna: Liber Förlag. [Google Scholar]
- von Thiele Schwarz U, Augustsson H, Hasson H, Stenfors-Hayes T. (2015) Promoting employee health by integrating health protection, health promotion, and continuous improvement: A longitudinal quasi-experimental intervention study. Journal of Occupational and Environmental Medicine 57(2): 217–225. [DOI] [PubMed] [Google Scholar]
- Wanous J, Reichers A, Hudy M. (1997) Overall job satisfaction: How good are single-item measures? Journal of Applied Psychology 82(2): 247–252. [DOI] [PubMed] [Google Scholar]
- Ware JE, Gandek B. (1998) Overview of the SF-36 Health Survey and the International Quality of Life Assessment (IQOLA) Project. Journal of Clinical Epidemiology 51: 903–912. [DOI] [PubMed] [Google Scholar]
- Womack J, Jones D, Roos D. (2007) The Machine that Changed the World: The Story of Lean Production. London: Simon & Schuster. [Google Scholar]
- Zoni S, Lucchini R G. (2012) European approaches to work-related stress: A critical review on risk evaluation. Safety and Health at Work 3(1): 43–49. [DOI] [PMC free article] [PubMed] [Google Scholar]