

Sir,
Bronchogenic carcinoma is a common malignancy worldwide and accounts for 27% of cancer-related deaths. Metastasis to parotid gland usually occurs from head and neck tumors. Metastasis to the parotid gland from a primary small cell carcinoma in the lung is rare and unusual.
A 52-year-old male presented to the otorhinolaryngology outpatient department with complaints of right-sided facial swelling over the mandible over 1½ months, which had gradually increased in size over 1½ months [Figure 1]. There was a pain in the swelling for 1 day. No facial weakness was noted. He also complained of pain on the right side of the chest for 1 month. He was a chronic smoker with pack-years of 60 and had stopped when the above symptoms started. He was also a chronic alcoholic. On local examination, the swelling was 4 cm × 3 cm in size in the right parotid region, hard in consistency, and the skin over the swelling was fixed in the posteroinferior portion of the swelling. There was no discharge from the swelling. He did not have any comorbidities. Blood investigations revealed hemoglobin of 14.4 g/dl, the total count of 7700 cells/mm3 with a differential of 66% neutrophils, 28% lymphocytes, 5% eosinophils, and a platelet count of 2.5 lakhs. Chest radiograph showed an opacity in the right upper zone [Figure 2]. A fine needle aspiration of the parotid swelling was performed which revealed that the smears were cellular and show hyperchromatic cells arranged singly and in clusters. A differential diagnosis of lymphoproliferative disease and small cell carcinoma was made. A screening contrast enhanced computed tomography of the neck, thorax, and abdomen were performed, the report of which is as follows, scan showed a lobulated mass lesion in the apical and anterior segment of the right upper lobe measuring 6.5 cm × 8.7 cm × 5.2 cm, showing heterogenous enhancement on postcontrast. Few foci of calcification were present in the center of the mass. Posterolaterally, the mass was in contact with the chest wall. Few subcentimetric nodules were in the right middle lobe and in the lingula. Rest of the lung parenchyma was normal. Trachea and main bronchi were normal. There was no significant mediastinal lymphadenopathy. Mediastinal vascular structures were normal. Also observed was a well-defined mass lesion measuring 3.5 cm × 3 cm in size in superficial lobe of the right parotid gland showing mild enhancement on the postcontrast scan. The left parotid, both submandibular and thyroid glands were normal. In the abdomen, a well-defined mass lesion measuring 2.8 cm × 2.7 cm was noted in the subdiaphragmatic region on the left side, which showed homogenous enhancement on postcontrast scan, superiorly was seen to abut the diaphragm and anterolaterally was seen in the left kidney. Mild stranding of fat surrounding the lesion was noted. Opinion was findings suggestive of primary lymphoma of the lung. Mass in superficial lobe of the right parotid gland and subdiaphragmatic lesion on the left side could represent metastasis. After computed tomography, the patient was referred to the Department of Pulmonary Medicine; a computed tomography-guided trucut biopsy of the lung mass was performed. The report showed fibrocollagenous tissue enclosing the groups of hyperchromatic small cells arranged singly and in sheets, cells showed hyperchromasia, dispersed chromatin and were fragile suggestive of small cell carcinoma. A diagnosis of primary small cell carcinoma of lung with metastasis to parotid gland and abdomen was made. The patient was started on platinum-based chemotherapy consisting of cisplatin and etoposide. Due to pain in the chest and parotid gland, he received radiotherapy to both the sites. After radiotherapy and three cycles of chemotherapy, there was marked reduction in parotid gland swelling [Figure 3]. Chest radiograph after radiotherapy and three cycles of platinum based chemotherapy showed persistence of opacity in right upper zone [Figure 4]. A repeat computed tomography done after three cycles of chemotherapy showed a decrease in the size of the primary tumor 5.9 cm × 6.3 cm × 2.7 cm in size. Few foci of dense calcification were noted in the center. Superiorly, the mass was in contact with the chest wall; however, no rib erosion was noted. Bilateral subcentimetric paratracheal and subcarinal lymph nodes were noted. In the neck, an ill-defined hypodense nonenhancing area was noted involving the superficial lobe of the right parotid gland along the inferior aspect. It was measured 1.3 cm × 1.5 cm in size. In the abdomen, inhomogenously enhancing lesion was noted in the subdiaphramatic region on the left side measuring 5.2 cm × 2.5 cm (the previous size 2.8 cm × 2.7 cm) with minimal stranding of adjacent fat. It was seen to involve the crura of left hemidiaphragm, and it showed loss of fat plane with superior aspect of the left kidney which was displaced inferiorly. Inhomogeneously, enhancing soft tissue density lesions were noted in both adrenal glands measuring 4.1 cm × 3.4 cm on the left side and 1.1 cm × 1.8 cm on the right side.
Figure 1.

Parotid gland metastasis from primary small cell carcinoma, presenting as right-sided facial swelling over mandible
Figure 2.
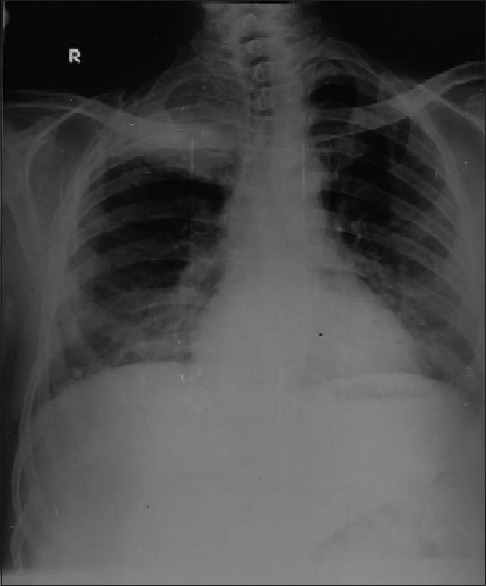
Chest radiograph at diagnosis. Showing opacity in the right upper zone
Figure 3.

Marked decrease in mandibular swelling after receiving three doses of chemotherapy
Figure 4.
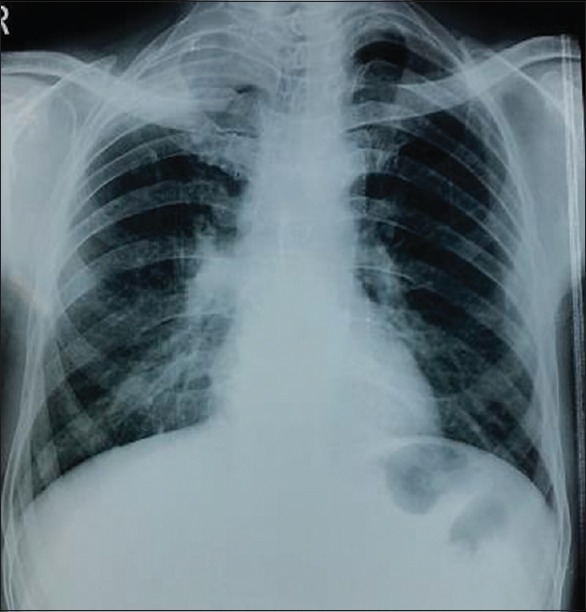
Chest Radiograph after three cycles of platinum based chemotherapy
Small cell lung carcinoma accounts for 15% of all lung cancers. It is associated with paraneoplastic syndromes.[1] It tends to metastasize early. The diagnosis may sometimes be made from a metastatic focus.[2] This case has been reported as it is rare for parotid gland metastasis to be the initial manifestation in bronchogenic carcinoma. Among all parotid gland tumors, small cell carcinoma is seen in 1.7% of cases.[3] In the majority of the cases having secondary spread to the parotid gland, the primary tumor originates from the head or neck region. Distant metastasis to the parotid gland is usually from bronchial carcinoma, renal carcinoma, colon carcinoma, carcinoma of prostate and breast.[4] The mechanism of metastatic disease to the head and neck remains unclear. Regional neoplasms such as cutaneous head and neck cancers are likely secondary to lymphatic spread. It has been postulated that hematologic dissemination is more common than lymphatic spread for infraclavicular primaries, although both are likely to play a role.[5] In our case, the patient was treated with concurrent chemotherapy and radiotherapy because small cell lung cancer is highly responsive to chemotherapy and radiotherapy. After the start of treatment, the facial swelling showed a marked reduction in size, the primary lesion in the lung also showed a reduction in size; however, the subdiaphragmatic metastasis showed an increase in size and he developed metastasis to both the adrenal glands.
Metastasis from small cell carcinoma to the parotid gland is very rare and also metastasis in the subdiaphragmatic area is rare. In patients presenting with malignant swelling in the parotid region, a careful evaluation for distant primary sites should be performed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We wish to thank the Dean, Goa Medical College, Dr PradeepNaik for permitting us to publish this case.
REFERENCES
- 1.Sher T, Dy GK, Adjei AA. Small cell lung cancer. Mayo Clin Proc. 2008;83:355–67. doi: 10.4065/83.3.355. [DOI] [PubMed] [Google Scholar]
- 2.Takatsugi K, Komuta K, Hosen N, Kitada S, Iida S, Nishihara K, et al. Metastasis of small cell lung cancer to the parotid gland as the initial clinical manifestation, followed by metastases to the pituitary gland and lumber spinal cord. Nihon Kokyuki Gakkai Zasshi. 1998;36:246–50. [PubMed] [Google Scholar]
- 3.Ulubas B, Ozcan C, Polat A. Small cell lung cancer diagnosed with metastasis in parotid gland. J Craniofac Surg. 2010;21:781–3. doi: 10.1097/SCS.0b013e3181d7f186. [DOI] [PubMed] [Google Scholar]
- 4.Boeger D, Hocke T, Esser D. The interesting case-no. 68. Metastasis of a small-cell bronchial carcinoma to the parotid gland. Laryngorhinootologie. 2005;84:117–20. doi: 10.1055/s-2004-826220. [DOI] [PubMed] [Google Scholar]
- 5.Meyer I, Shklar G. Malignant tumors metastatic to mouth and jaws. Oral Surg Oral Med Oral Pathol. 1965;20:350–62. doi: 10.1016/0030-4220(65)90167-2. [DOI] [PubMed] [Google Scholar]