

Abstract
Because the prevalence of antibiotic resistance markedly increases with time worldwide, anti-H. pylori treatment is continuing to be a great challenge forsphysicians in clinical practice. The Real-world Practice & Expectation of Asia-Pacific Physicians and Patients in Helicobacter Pylori Eradication (REAP-HP) Survey demonstrated that the accepted minimal eradication rate of anti-H. pylori regimen in H. pylori-infected patients was 91%. The Kyoto Consensus Report on Helicobacter Pylori Gastritis also recommended that, within any region, only regimens which reliably produce eradication rates of ≥90% in that population should be used for empirical treatment. This article is aimed to review current first-line eradication regimens with a per-protocol eradication rate exceeding 90% in most geographic areas. In regions with low (≦15%) clarithromycin resistance, 14-day hybrid (or reverse hybrid), 10 ~ 14-day sequential, 7 ~ 14-day concomitant, 10 ~ 14-day bismuth quadruple or 14-day triple therapy can achieve a high eradication rate in the first-line treatment of H. pylori infection. However, in areas with high (>15%) clarithromycin resistance, standard triple therapy should be abandoned because of low eradication efficacy, and 14-day hybrid (or reverse hybrid), 10 ~ 14-day concomitant or 10 ~ 14-day bismuth quadruple therapy are the recommended regimens. If no recent data of local antibiotic resistances of H. pylori strains are available, universal high efficacy regimens such as 14-day hybrid (or reverse hybrid), concomitant or bismuth quadruple therapy can be adopted to meet the recommendation of consensus report and patients’ expectation.
Keywords: Helicobacter pylori, First-line, Therapy, Hybrid therapy, Sequential therapy, Concomitant therapy, Triple therapy
Background
Helicobacter pylori (H. pylori) infect more than 50% of humans globally. It is the major cause of chronic gastritis, peptic ulcer, gastric mucosa-associated lymphoid tissue lymphoma (MALToma), and gastric adenocarcinoma [1, 2]. Eradication of H. pylori can effectively prevent the recurrence of peptic ulcer disease [3, 4]. Anti- H. pylori therapy is currently recommended in the treatment of H pylori-related gastric MALToma [5]. Additionally, eradication of H pylori is advocated as a preventative method in regions with high incidence of gastric adenocarcinoma [6, 7].
A recent survey for H. pylori eradication therapy revealed that 7-day standard triple therapy remained the most popular regimen in the Asia-Pacific region [8]. However, the eradication rate of 7-day standard triple therapy has declined to less than 80% in most countries worldwide owing to increasing resistance rate to antibiotics [9–12]. The Kyoto Consensus Report on Helicobacter Pylori Gastritis recommends that, within any region, only regimens which reliably produce eradication rates of ≥90% in that population should be used for empirical treatment [13]. Current medicine practice emphasizes shared decision making with patients. It is therefore important for physicians to know the expectations of patients and try to meet patients’ expectations on eradication therapy when they prescribe anti-H. pylori regimen. The survey for the Real-world Practice & Expectation of Asia-Pacific Physicians and Patients in Helicobacter Pylori Eradication (REAP-HP) showed that the expected minimal eradication rate in patients was 91.4% [8]. Hence, physicians should prescribe an eradication regimen with cure rate exceeding 90% to treat their H. pylori-infected patients. This article is aimed to review current novel first-line eradication regimens with a per-protocol (PP) eradication rate exceeding 90% in most geographic areas.
Current antibiotic resistance
The main reasons for eradication failure of standard triple therapy include antibiotic resistance, poor compliance and rapid metabolism of proton pump inhibitor (PPI) [10, 14, 15]. Clarithromycin resistance has been identified as the main reason for the failure of standard triple therapy [16, 17]. Pooled data from 20 studies involving 1975 patients treated with standard triple therapy showed an eradication rate of 88% in clarithromycin-sensitive strains versus 18% in clarithromycin-resistant strains [10]. Therefore, the background rate of clarithromycin resistance is critically important for the efficacy of standard triple therapy.
The prevalence of antibiotic resistance varies in different geographic regions and appears to be increasing with time in most countries worldwide [18–24]. For example, an increase in clarithromycin resistance was observed in Korea from 7.0% in 2009 to 16.0% in 2011 [23]. The resistance rate of H. pylori to clarithromycin in Japan had increased gradually from 2% in 1996 to approximately 30% in 2004 [22]. In China, a marked increase of clarithromycin resistance was seen from 8.6% in 2000 to 20.7% in 2009 [21]. The recent clarithromycin resistance rates of H. pylori in China, Taiwan, Japan, Turkey, Italy and the United States are approximately 50, 15, 30, 40, 30 and 13%, respectively [20]. The prevalence of metronidazole resistance quite varies in different countries. The resistance rate of H. pylori to metronidazole remains high in China (41.6 - 67.4% between 2008 and 2015). In contrast, the prevalence of metronidazole resistance is extremely low in Japan [22]. Nishizawa et al. described an overall resistance rate of 2.1% in patients studied from 2012 to 2104 [24]. In Korea, the prevalence of metronidazole resistance had increased from 45.1% in 2009 to 56.3% in 2011 [23]. Besides clarithromycin and metronidazole, amoxicillin is also one of the most commonly used antibiotics in first-line anti-H. pylori therapy. However, resistance to amoxicillin remains extremely low (less than 5%) in most countries [16, 20, 23, 24].
Updated H. pylori therapy
With the rising prevalence of antimicrobial resistance, standard triple therapy is no longer effective in most countries [15–17]. The eradication rate of the 7-day standard triple therapy in 14 hospitals over the Tokyo metropolitan area in 2010 was only 66.5 and 378.7% by intention-to-treat (ITT) and per-protocol (PP) analyses, respectively [25]. The regimen achieved a success rate of 68.5% by PP analysis in Korea [26]. Clinicians should therefore avoid triple therapies unless it has been proven to achieve an adequate success rate locally. Currently, several strategies including bismuth quadruple, non-bismuth quadruple (i.e., sequential, concomitant and hybrid) and high-dose dual therapies have proposed to increase the eradication rate [27–32]. Figure 1 summaries the regimens of these new therapies.
Fig. 1.
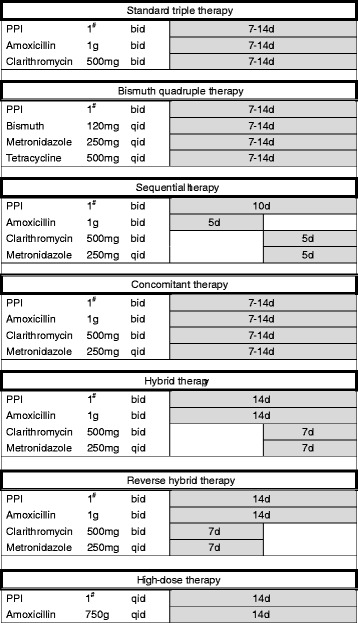
Current anti-H pylori regimens
Sequential therapy
Sequential therapies developed by Zullo et al. consists of a 5-day dual therapy with a PPI (standard dose, b.i.d.) and amoxicillin (1 g, b.i.d.) followed by a 5-day triple therapy with a PPI (standard dose, b.i.d.), clarithromycin (500 mg, b.i.d.) and metronidazole (500 mg, b.i.d.) [27]. Clarithromycin resistance also reduces the efficacy of sequential therapy. However, the impact of clarithromycin resistance on sequential therapy is markedly less than that on standard triple therapy because sequential therapy contains metronidazole as an additional antibiotic [16]. A randomized, double-blind, placebo-controlled trial demonstrated that the PP eradication rates of sequential therapy and standard triple therapy for clarithromycin-resistant strains were 89 and 29%, respectively [33]. The eradication rate of 10-day sequential therapy was superior to that of 7-day standard triple therapy in several randomized controlled trials [16, 33]. However, meta-analysis revealed that 10-day sequential therapy was not superior to 14-day standard triple therapy [34]. Either clarithromycin or metronidazole resistance can undermine the efficacy of sequential therapy [16, 35]. The eradication rates of 10-day sequential therapy for the strains with non-resistance, single clarithromycin resistance, single metronidazole resistance and dual resistances were 95, 70, 78, and 43%, respectively, in a recent prospective randomized controlled trial [35]. In addition, this therapy is more complex and requires changing antibiotics during the treatment course which may reduce the treatment compliance of patients.
Concomitant therapy
Concomitant therapy is another novel regimen proven successful in the presence of clarithromycin resistance [16, 30]. It is a 4-drug regimen containing a PPI (standard dose, b.i.d.), clarithromycin (500 mg, b.i.d.), amoxicillin (1 g, b.i.d.) and metronidazole (500 mg, b.i.d.) which are all given for the entire duration of therapy (Fig. 1). Meta-analysis demonstrated that concomitant therapy is more effective than standard triple therapy (90% versus 78% by ITT analysis) [36]. Dual clarithromycin and metronidazole resistance undermines the efficacy of concomitant therapy. A recent randomized controlled trial revealed that the eradication rates of 7-day concomitant therapy for the H pylori strains with nonresistance, single clarithromycin resistance, single metronidazole resistance, and dual clarithromycin and metronidazole resistance were 100.0, 100.0, 100.0, and 66.7%, respectively [16].
The efficacy of concomitant therapy was also related to the duration of treatment [37]. A tendency toward better results with longer treatments (7–10 days versus 3–5 days) has been observed [37]. Concomitant therapy is less complex than sequential therapy as this regimen does not involve changing drugs halfway through.
Hybrid and reverse hybrid therapies
Hybrid therapy was introduced by Hsu et al. in Taiwan in 2011 [29]. This regimen consists of a dual therapy with a proton pump inhibitor (PPI) and amoxicillin for 7 days followed by a quadruple regimen with a PPI, amoxicillin, clarithromcyin and metronidazole for 7 days. It produced an eradication rate of 99.1% by PP analysis and 97.4% by ITT analysis in Taiwan [16]. A systemic review showed that the eradication rates of hybrid therapy for clarithromycin-sensitive and resistant strains were 99.1 and 85.7%, respectively [38]. The impact of metronidazole resistance on the efficacy of the new therapy also appeared minor (susceptible strains: 100% [68/68]; resistant strains: 94.2% [49/52]) [38]. Several randomized controlled trials demonstrated that hybrid regimens were comparable with or more effective than sequential regimens [38–42]. A recent large multicentre randomized controlled trial demonstrated that both 14-day hybrid and 14-day concomitant therapies cured more than 90% of patients with H pylori infections in areas of high clarithromycin and metronidazole resistance [43]. However, significantly more patients were compliant with hybrid therapy (98.8%) than concomitant therapy (95.2%) [43]. Meta-analysis revealed that hybrid therapy and concomitant therapy achieved comparable eradication rate [38]. Recently, the Taiwan H pylori Consensus Report recommends 14-day hybrid, concomitant and bismuth quadruple therapies as choices of anti-H pylori treatment in areas with either high or low clarithromycin resistance [44].
Switching drugs halfway through the course increases the complexity of an anti-H pylori regimen. Reversing the sequence of drug administration (a quadruple regimen followed by a dual regimen) may simplify hybrid therapy (a one-step two-phase therapy; Fig. 1). A pilot multicenter, randomized trial demonstrated that reverse hybrid therapy was highly effective in Taiwan (eradication rate by PP analysis: 96%) and superior to standard triple therapy [43]. A retrospective cohort study demonstrated that reverse hybrid therapy yielded a similar eradication rate as standard hybrid therapy [45]. The new therapy appears to be a simple, highly effective, and well-tolerated treatment for H pylori infection in the era of increasing antibiotic resistance.
High-dose dual therapy
High-dose dual therapy developed by Yang et al. is another emerging treatment for H pylori infection [32]. The new therapy consists of high-dose PPI (one tablet q.i.d) and amoxicillin (750 mg q.i.d), which may keep the intragastric pH at a value higher than 6.5 regardless of CYP2C19 genotype [46] and maintain steady plasma concentration of amoxicillin above the minimal inhibitory concentration for H pylori [47]. The efficacy of the new therapy was significantly higher than that of standard triple therapy in Taiwan [42]. However, it was less effective as the first-line therapy for eradicating H pylori in Korea [48]. Currently, data on high-dose dual therapy are scarce, and further studies to investigate the simple regimens are needed.
Bismuth quadruple therapy
Bismuth-containing quadruple therapy containing a PPI, bismuth, metronidazole and tetracycline is recommended as the choice treatment for H pylori infection in areas of either low or high clarithromycin resistance in the Maastricht V/Florence Consensus Report [49]. The optimal treatment duration of bismuth-containing quadruple therapy remains unclear. However, the efficacy of bismuth quadruple therapy for 1–3 days, 4 days or 7 days was less effective than when given for 10–14 days [50]. Bismuth quadruple therapy for 10–14 days achieved ≧ 85% eradication rate, even in areas with a high prevalence of metronidazole resistance [50]. However, 14-day bismuth quadruple therapy had a much higher frequency of adverse events than 14-day hybrid therapy (55.5% vs 15.7%, P < 0.001) [51].
Quinolone-containing triple therapy
A quinolone-containing triple therapy is effective as the first-line therapy for H pylori infection. Its cure rates range from 72 to 96% [52]. The regimen might be considered in populations with clarithromycin resistance greater than 15–20% and quinolone resistance less than 10% [53]. Nonetheless, a quinolone-based triple therapy is not generally recommended as a first-line therapy due to concerns of the rising prevalence of quinolone-resistant strains. Additionally, the increased use of quinolone would likely lead to the development of more quinolone-resistant pathogens for respiratory and urogenital tract infection.
Conclusion
Current consensus report on H. pylori eradication therapy recommends that only regimens that reliably produce eradication rates of ≥90% should be used for empirical treatment. The REAP-HP Survey also revealed that the accepted minimal eradication rate of anti-H. pylori therapy in infected patients was 91%. To meet the recommendation of the consensus report and patients’ expectation, 14-day triple, 14-day hybrid (or reverse hybrid), 10 ~ 14-day sequential, 7 ~ 14-day concomitant or 10 ~ 14-day bismuth quadruple therapy can be adopted as the first-line treatment for H. pylori infection in areas with low (≦15%) clarithromycin resistance (Fig. 2). In areas with high (>15%) clarithromycin resistance, standard triple therapy should be abandoned, and 14-day hybrid (or reverse hybrid), 10 ~ 14-day concomitant or 10 ~ 14-day bismuth quadruple therapy can be used to treat H. pylori infection. If no recent data of local antibiotic resistances of H. pylori strains are available, universal high efficacy regimens such as 14-day hybrid (or reverse hybrid), concomitant or bismuth quadruple therapy can be adopted to meet the recommendation of consensus report and patients’ expectation.
Fig. 2.
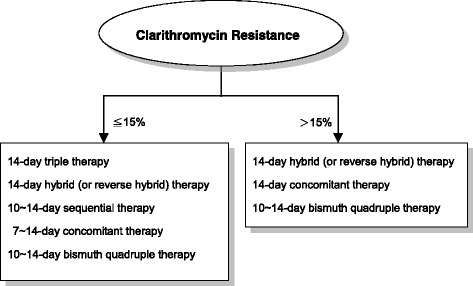
Recommended anti-H pylori regimens in regions with different clarithromycin resistant rates
Acknowledgements
The authors are indebted to Miss Joyce Chen for figure preparation.
Funding
The study was funded by the Kaohsiung Veterans General Hospital (Grant Numbers: VGHKS106–091 and VGHKS105–81) and the Ministry of Science and Technology, Exacutive Yuan, ROC, Taiwan (Grant Number: MOST 104–2314-B-075B-001-MY2). The grant from the Kaohsiung Veterans General Hospital was contributed to English revision, and the grant from the Ministry of Science and Technology, Executive Yuan, ROC, Taiwan was contributed to reference search.
Availability of data and materials
Data sharing not applicable to this article as no datasets were generated or analyzed during the study.
Abbreviations
- H. pylori
Helicobacter pylori
- ITT
Intention to treat
- MALToma
Mucosa-associated lymphoid tissue lymphoma
- PP
Per protocol
- PPI
Proton pump inhibitor
- REAP-HP
Real-world practice & expectation of Asia-Pacific physicians and patients in Helicobacter pylori eradication
Authors’ contributions
CCH and PIH worked equally in study design, data analysis, and drafting of manuscript. KWT and TJT performed reference search and revised the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Vakil N, Megraud F. Eradication therapy for helicobacter pylori. Gastroenterology. 2007;133:985–1001. doi: 10.1053/j.gastro.2007.07.008. [DOI] [PubMed] [Google Scholar]
- 2.Malfertheiner P, Chan FK, McColl KE. Peptic ulcer disease. Lancet. 2009;374:1449–1461. doi: 10.1016/S0140-6736(09)60938-7. [DOI] [PubMed] [Google Scholar]
- 3.Graham DY, Lew GM, Klein PD, Evans DG, Evans DJ, Jr, Saeed ZA, et al. Effect of treatment of helicobacter pylori infection on the long-term recurrence of gastric or duodenal ulcer. A randomized controlled study. Ann Intern Med. 1992;116:705–708. doi: 10.7326/0003-4819-116-9-705. [DOI] [PubMed] [Google Scholar]
- 4.Sung JJ, Chung SC, Ling TK, Yung MY, Leung VK, Ng EK, et al. Antibacterial treatment of gastric ulcer associated with helicobacter pylori. N Engl J Med. 1995;332:139–142. doi: 10.1056/NEJM199501193320302. [DOI] [PubMed] [Google Scholar]
- 5.Zucca E, Dreyling M. Gastric marginal zone lymphoma of MALT type: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann Oncol. 2009;200(Suppl 4):113–114. doi: 10.1093/annonc/mdp146. [DOI] [PubMed] [Google Scholar]
- 6.Asaka M. A new approach for elimination of gastric cancer deaths in Japan. Int J Cancer. 2013;132:1272–1276. doi: 10.1002/ijc.27965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Fock KM, Katelaris P, Sugano K, Ang TL, Hunt R, Talley NJ, et al. Second Asia-Pacific consensus guidelines for helicobacter pylori infection. J Gastroenterol Hepatol. 2009;24:1587–1600. doi: 10.1111/j.1440-1746.2009.05982.x. [DOI] [PubMed] [Google Scholar]
- 8.Chuah Y-Y, Wu D-C, Chuah S-K, Yang J-C, Lee T-H, Yeh H-Z, et al. The survey for Real-World-Practice & Expectation of Asia-Pacific physicians and patients in Helicobacter Pylori eradication (REAP-HP survey). Helicobacter. 2017; in press [DOI] [PubMed]
- 9.Gumurdulu Y, Serin E, Ozer B, Kayaselcuk F, Ozsahin K, Cosar AM, et al. Low eradication rate of helicobacter pylori with triple 7–14 days and quadruple therapy in Turkey. World J Gastroenterol. 2004;10:668–671. doi: 10.3748/wjg.v10.i5.668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Megraud F. H pylori antibiotic resistance: prevalence, importance, and advances in testing. Gut. 2004;53:1374–1384. doi: 10.1136/gut.2003.022111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kim JS, Kim BW, Hong SJ, Kim JI, Shim KN, Kim JH, et al. Sequential therapy versus triple therapy for the first line treatment of helicobacter pylori in Korea: a Nationwide randomized trial. Gut Liver. 2016;10:556–561. doi: 10.5009/gnl15470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.De Francesco V, Margiotta M, Zullo A, Hassan C, Troiani L, Burattini O, et al. Clarithromycin-resistant genotypes and eradication of helicobacter pylori. Ann Intern Med. 2006;144:94–100. doi: 10.7326/0003-4819-144-2-200601170-00006. [DOI] [PubMed] [Google Scholar]
- 13.Sugano K, Tack J, Kuipers EJ, Graham DY, El-Omar EM, Miura S, et al. Kyoto global consensus report on helicobacter pylori gastritis. Gut. 2015;64:1353–1367. doi: 10.1136/gutjnl-2015-309252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Graham DY, Akiko S. New concepts of resistance in the treatment of helicobacter pylori infections. Nat Clin Pract Gastroenterol Hepatol. 2008;5:321–331. doi: 10.1038/ncpgasthep1138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Graham DY, Lee YC, Wu MS. Rational helicobacter pylori therapy: evidence-based medicine rather than medicine-based evidence. Clin Gastroenterol Hepatol. 2014;12:177–186. doi: 10.1016/j.cgh.2013.05.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hsu PI, Wu DC, Chen WC, Tseng HH, Yu HC, Wang HM, et al. Randomized controlled trial comparing 7-day triple, 10-day sequential, and 7-day concomitant therapies for helicobacter pylori infection. Antimicrob Agents Chemother. 2014;58:5936–5942. doi: 10.1128/AAC.02922-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Houben MH, van de Beek D, Hensen EF, de Craen AJ, Rauws EA, Tytgat GN. A systemic review of helicobacter pylori therapy – the impact of antimicrobial resistance on eradication rates. Aliment Pharmacol Ther. 1999;13:1047–1055. doi: 10.1046/j.1365-2036.1999.00555.x. [DOI] [PubMed] [Google Scholar]
- 18.Gatta L, Vakil N, Vaira D, Scarpignato C. Global eradication rates for helicobacter pylori infection: systematic review and meta-analysis of sequential therapy. BMJ. 2013;347:f4587. doi: 10.1136/bmj.f4587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Meyer JM, Silliman NP, Wang W, Siepman NY, Sugg JE, Morris D, et al. Risk factors for helicobacter pylori resistance in the UnitedStates: the surveillance of H. Pylori antimicrobial resistance partnership (SHARP) study, 1993–1999. Ann Intern Med. 2002;136:13–24. doi: 10.7326/0003-4819-136-1-200201010-00008. [DOI] [PubMed] [Google Scholar]
- 20.Thung I, Aramin H, Vavinskaya V, Gupta S, Park JY, Crowe SE, et al. Review article:the global emergence of helicobacter pylori antibiotic resistance. Aliment Pharmacol Ther. 2016;43:514–533. doi: 10.1111/apt.13497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sun QJ, Liang X, Zheng Q, Gu WQ, Liu WZ, Xiao SD, et al. Resistance of helicobacter pylori to antibiotics from 2000 to 2009 in shanghai. World J Gastroenterol. 2010;16:5118–5121. doi: 10.3748/wjg.v16.i40.5118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Horiki N, Omata F, Uemura M, Suzuki S, Ishii N, Iizuka Y, et al. Annual change of primary resistance to clarithromycin among helicobacter pylori isolates from 1996 through 2008 in Japan. Helicobacter. 2009;14:86–90. doi: 10.1111/j.1523-5378.2009.00714.x. [DOI] [PubMed] [Google Scholar]
- 23.An B, Moon BS, Kim H, Lim HC, Lee YC, Lee G, et al. Antibiotic resistance in helicobacter pylori strains and its effect on H. Pylori eradication rates in a single center in Korea. Ann Lab Med. 2013;33:415–419. doi: 10.3343/alm.2013.33.6.415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Nishizawa T, Maekawa T, Watanabe N, Harada N, Hosoda Y, Yoshinaga M, et al. Clarithromycin versus Metronidazole as first-line helicobacter pylori eradication: a multicenter, prospective, randomized controlled study in Japan. J Clin Gastroenterol. 2015;49:468–471. doi: 10.1097/MCG.0000000000000165. [DOI] [PubMed] [Google Scholar]
- 25.Kawai T, Takahashi S, Suzuki H, Sasaki H, Nagahara A, Asaoka D, et al. Changes in the first line helicobacter pylori eradication rates using the triple therapy-a multicenter study in the Tokyo metropolitan area (Tokyo helicobacter pylori study group) J Gastroenterol Hepatol. 2014;29(Suppl 4):29–32. doi: 10.1111/jgh.12796. [DOI] [PubMed] [Google Scholar]
- 26.Chung JW, Jung YK, Kim YJ, Kwon KA, Kim JH, Lee JJ, et al. Ten-day sequential versus triple therapy for helicobacter pylori eradication: a prospective, open-label, randomized trial. J Gastroenterol Hepatol. 2012;27:1675–1680. doi: 10.1111/j.1440-1746.2012.07249.x. [DOI] [PubMed] [Google Scholar]
- 27.Zullo A, De Francesco V, Hassan C, Morini S, Vaira D. The sequential therapy regimen for helicobacter pylori eradication: a pooled-data analysis. Gut. 2007;56:1353–1357. doi: 10.1136/gut.2007.125658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Song ZQ, Zhou LY. Hybrid, sequential and concomitant therapies for Helciobacter pylori eradication: A systemic review and meta-analysis. World J Gastroenterol 2016;22:4766–75. [DOI] [PMC free article] [PubMed]
- 29.Hsu PI, Wu DC, Wu JY, Graham DY. Modified sequential helicobacter pylori therapy: proton pump inhibitor and amoxicillin for 14 days with clarithromycin and metronidazole added as a quadruple (hybrid) therapy for the final 7 days. Helicobacter. 2011;16:139–145. doi: 10.1111/j.1523-5378.2011.00828.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wu DC, Hsu PI, Wu JY, Opekun AR, Kuo CH, Wu IC, et al. Sequential and concomitant therapies with 4 drugs are equally effective for eradication of H pylori infection. Clin Gastroenterol Hepatol. 2010;8:36–41. doi: 10.1016/j.cgh.2009.09.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Malfertheiner P, Bazzoli F, Delchier JC, Celiñski K, Giguère M, Rivière M, et al. Helicobacter pylori eradication with a capsule containing bismuth subcitrate potassium, metronidazole, and tetracycline given with omeprazole versus clarithromycin-based triple therapy: a randomised, open-label, non-inferiority, phase 3 trial. Lancet. 2011;377:905–913. doi: 10.1016/S0140-6736(11)60020-2. [DOI] [PubMed] [Google Scholar]
- 32.Yang JC, Lin CJ, Wang HL, Chen JD, Kao JY, Shun CT, et al. High-dose dual therapy is superior to standard first-line or rescue therapy for helicobacter pylori infection. Clin Gastroenterol Hepatol. 2015;13:895–905. doi: 10.1016/j.cgh.2014.10.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Vaira D, Zullo A, Vakil N, Gatta L, Ricci C, Perna F, et al. Sequential therapy versus standard triple-drug therapy for helicobacter pylori eradication: a randomized trial. Ann Intern Med. 2007;146:556–563. doi: 10.7326/0003-4819-146-8-200704170-00006. [DOI] [PubMed] [Google Scholar]
- 34.Gatta L, Vakil N, Leandro G, Di Mario F, Vaira D. Sequential therapy or triple therapy for helicobacter pylori infection: systematic review and meta-analysis of randomized controlled trials in adults and children. Am J Gastroenterol. 2009;104:3069–3079. doi: 10.1038/ajg.2009.555. [DOI] [PubMed] [Google Scholar]
- 35.Liou JM, Chen CC, Chen MJ, Chen CC, Chang CY, Fang YJ, et al. Sequential versus triple therapy for the first-line treatment of helicobacter pylori: a multicentre, open-label, randomised trial. Lancet. 2013;381:205–213. doi: 10.1016/S0140-6736(12)61579-7. [DOI] [PubMed] [Google Scholar]
- 36.Essa AS, Kramer JR, Graham DY, Treiber G. Meta-analysis: four-drug, three-antibiotic, non-bismuth-containing “concomitant therapy” versus triple therapy for helicobacter pylori eradication. Helicobacter. 2009;14:109–118. doi: 10.1111/j.1523-5378.2009.00671.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kongchayanun C, Vilaichone RK, Pornthisarn B, Amornsawadwattana S, Mahachai V. Pilot study to identify the optimum duration of concomitant helicobacter pylori eradication therapy in Thailand. Helicobacter. 2012;17:282–285. doi: 10.1111/j.1523-5378.2012.00953.x. [DOI] [PubMed] [Google Scholar]
- 38.Hsu PI, Lin PC, Graham DY. Hybrid therapy for helicobacter pylori infection: a systemic review and meta-analysis. World J Gastroenterol. 2015;21:12954–12962. doi: 10.3748/wjg.v21.i45.12954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Sardarian H, Fakheri H, Hosseini V, Taghvaei T, Maleki I, Mokhtare M. Comparison of hybrid and sequential therapies for helicobacter pylori eradication in Iran: a prospective randomized trial. Helicobacter. 2013;18:129–134. doi: 10.1111/hel.12017. [DOI] [PubMed] [Google Scholar]
- 40.Chen KY, Lin TJ, Lee HC, Wang CK, Wu DC. Hybrid vs sequential therapy for eradication of helicobacter pylori in Taiwan: a prospective randomized trial. World J Gastroenterol. 2015;21:10435–10442. doi: 10.3748/wjg.v21.i36.10435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.De Francesco V, Hassan C, Ridola L, Giorgio F, Ierardi E, Zullo A. Sequential, concomitant and hybrid first-line therapies for helicobacter pylori eradication: a prospective randomized study. J Med Microbiol. 2014;63:748–752. doi: 10.1099/jmm.0.072322-0. [DOI] [PubMed] [Google Scholar]
- 42.Oh DH, Lee DH, Kang KK, Park YS, Shin CM, Kim N, et al. Efficacy of hybrid therapy as first-line regimen for helicobacter pylori infection compared with sequential therapy. J Gastroenterol Hepatol. 2014;29:1171–1176. doi: 10.1111/jgh.12518. [DOI] [PubMed] [Google Scholar]
- 43.Molina-Infante J, Romano M, Fernandez-Bermejo M, Federico A, Gravina AG, Pozzati L, et al. Optimized nonbismuth quadruple therapies cure most patients with helicobacter pylori infection in populations with high rates of antibiotic resistance. Gastroenterology. 2013;145:121–128.e1. doi: 10.1053/j.gastro.2013.03.050. [DOI] [PubMed] [Google Scholar]
- 44.Sheu BS, Wu MS, Chiu CT, Lo JC, Wu DC, Liou JM, et al. Consensus on the clinical management, screening-to-treat, and surveillance of helicobacter pylori infection to improve gastric cancer control on a nationwide scale. Helicobacter. 2017; doi:10.1111/hel.12368. [DOI] [PMC free article] [PubMed]
- 45.Hsu PI, Wu DC. Reverse hybrid therapy achieves a similar eradication rate as hybrid therapy in the treatment of Helicobacter pylori infection. Gastroenterology. 2016;150(Suppl 1):S73. doi: 10.1016/S0016-5085(16)30361-4. [DOI] [Google Scholar]
- 46.Sugimoto M, Furuta T, Shirai N, Kajimura M, Hishida A, Sakurai M, et al. Different dosage regimens of rabeprazole for nocturnal gastric acid inhibition in relation to cytochrome P450 2C19 genotype status. Clin Pharmacol Ther. 2004;76:290–301. doi: 10.1016/j.clpt.2004.06.008. [DOI] [PubMed] [Google Scholar]
- 47.Craig WA. Pharmacokinetic/pharmacodynamic parameters: rationale for antibacterial dosing of mice and men. Clin Infect Dis. 1998;26:1–10. doi: 10.1086/516284. [DOI] [PubMed] [Google Scholar]
- 48.Kwack W, Lim Y, Lim C, Graham DY. High dose Ilaprazole/amoxicillin as first-line regimen for helicobacter pylori infection in Korea. Gastroenterol Res Pract. 2016;2016:1648047. doi: 10.1155/2016/1648047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Malfertheiner P, Megraud F, O’Morain CA, Gisbert JP, Kuipers EJ, Axon AT, et al. Management of Helicobacter pylori infection — the Maastricht V/Florence consensus report. Gut. 2017;66:6–30. doi: 10.1136/gutjnl-2016-312288. [DOI] [PubMed] [Google Scholar]
- 50.Fischbach L, Evans EL. Meta-analysis: the effect of antibiotic resistance status on the efficacy of triple and quadruple first-line therapies for helicobacter pylori. Aliment Pharmacol Ther. 2007;26:343–357. doi: 10.1111/j.1365-2036.2007.03386.x. [DOI] [PubMed] [Google Scholar]
- 51.Hsu PI, Wu DC, Tsay FW. Both 14-day hybrid and bismuth containing quadruple therapies cure most patients with Helicobacter pylori infection in populations with moderate antibiotic resistance: a randomized controlled trial. Gastroenterology. 2016;150(Suppl 1):S72–S73. doi: 10.1016/S0016-5085(16)30360-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Berning M, Krasz S, Miehlke S. Should quinolones come first in helicobacter pylori therapy? Therap Adv Gastroenterol. 2011;4:103–114. doi: 10.1177/1756283X10384171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Hsu PI, Kao SS. Therapy of helicobacter pylori infection: many drugs for which association? In: Manfredi M, Luigi De'Angelis G, editors. Helicobacter pylori. New York: Nova Science Publishers, Inc; 2013. pp. 347–362. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the study.