

Abstract
Patent foramen ovale has been associated with multiple pulmonary diseases, such as pulmonary hypertension, platypnea-orthodeoxia syndrome, and chronic obstructive pulmonary disease. A connection between patent foramen ovale and chronic pulmonary disease was first described more than 2 decades ago in case reports associating patent foramen ovale with more severe hypoxemia than that expected based on the severity of the primary pulmonary disease. It has been suggested that patients with both chronic pulmonary disease and patent foramen ovale are subject to severe hypoxemia because of the right-to-left shunt. Furthermore, investigators have reported improved systemic oxygenation after patent foramen ovale closure in some patients with chronic pulmonary disease. This review focuses on the association between chronic pulmonary disease and patent foramen ovale and on the dynamics of a right-to-left shunt, and it considers the potential benefit of patent foramen ovale closure in patients who have hypoxemia that is excessive in relation to the degree of their pulmonary disease.
Keywords: Diagnostic imaging; exercise tolerance; foramen ovale, patent/complications/diagnosis/diagnostic imaging/physiopathology/surgery/therapy; heart septal defects, atrial/prevention & control; hemodynamics; hypertension, pulmonary/complications/etiology/physiopathology; hypoxia/complications/diagnosis/etiology; pulmonary disease, chronic obstructive/complications/physiopathology/therapy; recovery of function; risk factors
In fetal circulation, the foramen ovale functions as a one-way valve that enables blood to flow from the right atrium (RA) to the left atrium (LA) so that oxygenated blood from the placenta can bypass the unaerated lungs and directly enter the fetus' systemic circulation. This mechanism is maintained throughout evolution; all placental mammals have a foramen ovale.1,2 After birth, an infant's pulmonary vascular resistance decreases, and there is a concomitant increase in LA pressure and decrease in RA pressure. The septum primum is forced against the LA side of the septum secundum, and the 2 septa eventually fuse, leaving behind the fossa ovalis, a depression that marks the site of the foramen ovale. Functional closure of the foramen ovale is incomplete in about 20% of the population.3–8 Most people with a patent foramen ovale (PFO) remain asymptomatic. Nevertheless, interatrial shunting through a PFO can occur with strenuous effort that simulates a Valsalva maneuver, such as yelling, straining during bowel evacuation, coughing, and exercise.
Anatomic variants associated with PFOs also promote shunting. A residual eustachian valve can direct flow preferentially from the inferior vena cava toward the interatrial septum. Even with minimal interatrial communication, the size of a remnant eustachian valve appears to be an independent risk factor for a right-to-left (RL) shunt.9–11 Significant tricuspid valve regurgitation in the presence of a PFO can project blood to the superior aspect of the RA and then through the interatrial communication, causing RL shunting.12 An atrial septal aneurysm—a bulge in the fossa ovalis—can occur with an interatrial communication and appears to be an additional risk factor for cryptogenic stroke and hypoxemia.13–15 On occasion, excessive hypoxemia is due to the opening of a PFO associated with unwinding of the aorta or with hemidiaphragmatic paralysis, the latter of which is exacerbated when a patient moves from a lying to a standing position (orthodeoxia).16,17
Patent foramen ovale has been linked with paradoxical embolic stroke, platypnea-orthodeoxia syndrome, decompression illness, exacerbation of obstructive sleep apnea, obesity hypoventilation syndrome, chronic pulmonary disease, and migraine headache with aura. The proposed mechanisms and clinical characteristics of PFOs associated with these conditions have been described in detail.18–29 In patients with PFO who have one of these conditions, the LA pressure is typically 5 to 8 mmHg higher than the RA pressure; however, in patients with chronic pulmonary disease, such as chronic obstructive pulmonary disease (COPD), elevated intrathoracic pressure and pulmonary artery pressure (PAP) can cause the RA pressure to surpass the LA pressure, resulting in RL shunting.30–34 Hypoxemia occurs if a large amount of deoxygenated venous blood shunts to the left side of the heart; this could explain why a patient with PFO might experience decreased arterial oxygenation to a degree greater than that expected based on the patient's underlying pulmonary disease.35–37 However, based on our own clinical observation of such patients, it is difficult to distinguish the relative contributions of the RL shunt versus the underlying pulmonary disease to the patient's hypoxemia.
In the United States, COPD affects as many as 32 million people, or 10% of the population. Moreover, at least 20% of COPD patients also have PFOs, which means that more than 6 million patients are affected by both COPD and PFO.38 More than one million Medicare patients use supplemental oxygen because of COPD, and the annual cost is over $2 billion.39,40 This review takes into account the potential public health impact of eliminating RL shunts and explores the current understanding of how PFO can progress from an incidental finding to an active contributor to hypoxemia in patients with chronic pulmonary disease.
Diagnostic Imaging Methods for Patent Foramen Ovale
Patent foramen ovale can be identified during autopsy or cardiac catheterization. However, it is most often diagnosed during contrast echocardiography. Use of agitated-saline contrast during transesophageal echocardiography (TEE), with and without the use of straining, is the minimally invasive standard for PFO diagnosis.41,42 The more frequently used screening method, transthoracic echocardiography (TTE) with agitated-saline contrast, is limited because it does not enable direct visualization of a PFO; instead, the images capture agitated-saline bubbles in the LA. More recent data have suggested a role for transcranial Doppler (TCD) in PFO identification, given TCD's greater sensitivity in comparison with echocardiography and its ability to quantify the degree of RL shunting.43–45
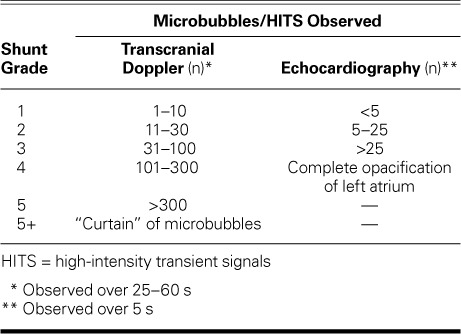
Standardizing PFO sizing is challenging because the degree of shunting differs, depending upon whether the patient is at rest or performing maneuvers that increase intrathoracic pressure. Currently, there is no single accepted grading criterion. Some investigators focus on the anatomic size of the defect, whereas others measure the degree of the shunt based on the number of agitated-saline microbubbles detected in the LA or middle cerebral artery at a specific moment or within a designated time frame. The most accurate technique for measuring PFO size is to position a sizing balloon within the PFO and gently inflate it with diluted contrast medium; however, this method necessitates invasive right-sided heart catheterization.46 Anatomic grading on echocardiography is determined by measuring the separation of the septum primum from the septum secundum; however, this does not always correlate with the degree of shunting. A functional method of shunt-grading involves agitated-saline contrast injections and echocardiography. The degree of shunting depends on the number of microbubbles observed in the LA over 3 s.47 Agitated-saline solution is also used as a contrast agent with TCD, in which the number of saline microbubbles—or high-intensity transient signals (HITS)—reaching the middle cerebral artery are measured during an interval of 25 s to 1 min. The degree of shunting is based on a logarithmic scale of 0 to 5+; in grade 5+, the bubbles form a “curtain” because they are indistinguishable and too numerous to count (Table I).48 Patent foramen ovale corresponds to a TCD shunt of grade 3 or higher and is confirmed by right-sided heart catheterization. Grade 1 and 2 shunts are usually caused by either the transmission of a few bubbles through the pulmonary circulation or by a very small PFO (less than 2 mm, as determined by balloon sizing).49 The sensitivity of power M-mode TCD (98%) has been found to be greater than that of TEE (91%) for PFO detection.48,49 However, although TCD sensitivity surpasses that of echocardiography and intracardiac echocardiography, it is also more likely to produce false-positive results.45 Thus, TCD is not specific. The operator is unable to view the PFO anatomy and cannot distinguish between a PFO, a fenestrated atrial septal aneurysm, a systemic venous-to-pulmonary venous collateral fistula, or a pulmonary arteriovenous fistula. Nevertheless, because it is more comfortable for the patient than is TEE, TCD is useful as the initial screening tool for identifying an RL shunt.43,49,50
TABLE I.
Methods for Grading Shunts
Patent Foramen Ovale Prevalence in Hypoxemic COPD Patients
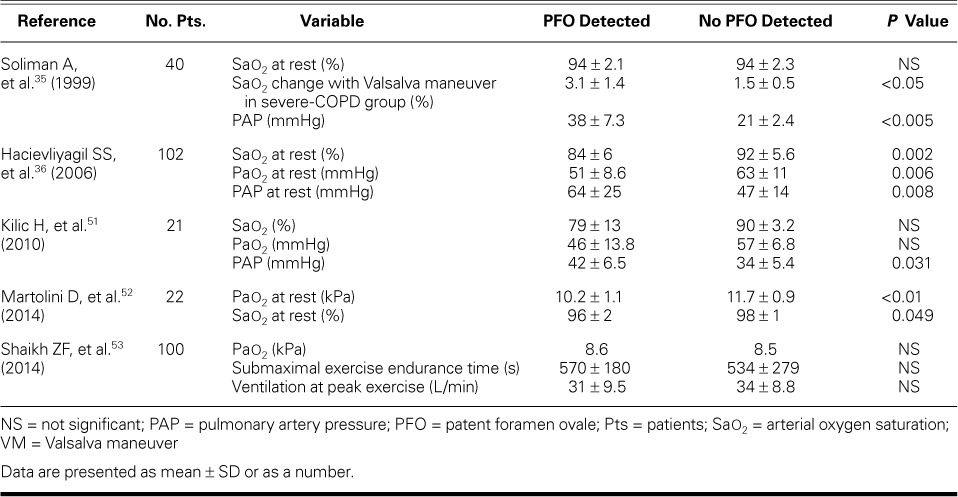
Soliman and colleagues35 were the first to describe a relationship between PFO and COPD in 20 patients with severe COPD (Global Initiative for Chronic Obstructive Lung Disease stages III–IV) (Table II). With the use of contrast TEE and pressure-generating movements (coughs and Valsalva maneuvers), the investigators found that the prevalence of PFO in the COPD group was twice that in control subjects (70% vs 35%; P <0.05). More PFOs were detected in their control group than in the control groups of most other population studies, perhaps because they defined a positive shunt as having a minimum of 5 microbubbles seen in the LA within 3 cardiac cycles; this was a low cutoff compared to those used in other studies.3–8 In a Turkish study similar to that of Soliman and colleagues, Hacievliyagil and associates36 detected a 2-fold increase in PFO prevalence in COPD patients with hypoxemia in comparison with healthy controls. Although Kilic and colleagues51 found no association between PFO and hypoxemia in COPD patients, they did detect higher PAP levels in patients with a PFO. Martolini and colleagues52 found a PFO in 12 of 22 patients with COPD, and more of these patients had hypoxemia in comparison with their non-PFO counterparts. Shaikh and co-authors53 were unable to corroborate these findings in their study of 50 patients with COPD and 50 healthy controls; the 2 groups had a PFO prevalence of 46% and 30%, respectively (P=0.15). They used both contrast TTE and TCD to identify PFO, and, like Soliman and colleagues, they used a relatively low cutoff for a positive RL shunt (scattered individual bubbles seen on TTE or ≥3 bubbles seen on TCD), which might account for the authors' observation that there was a higher prevalence of RL shunting in their study. Most shunts were classified as grade 1 or 2. Notably, Shaikh and coauthors did detect a statistically significant difference in the prevalence of large PFOs (defined as grade >3 with use of TCD or TTE) in 13 of 50 COPD patients compared with 3 of 50 control subjects (P=0.01).
TABLE II.
Comparison of Hypoxemia Markers in Studies of Patients with Chronic Obstructive Pulmonary Disease with and without PFO
Two Cases of Hypoxemia in the Presence of Patent Foramen Ovale
The following 2 cases, which involve patients treated at our clinic, illustrate hypoxemia in the presence of PFO and the impact of PFO closure.
Patient 1. A 61-year-old man with a history of COPD (forced expiratory volume 1 [FEV1], 56%) and tobacco dependence was referred by his pulmonologist for worsening hypoxemia thought to be disproportionate to his pulmonary disease. Resting oxygen saturation was 84% without supplemental oxygen; it improved to 97% on 6 L of supplemental oxygen and fell to as low as 70% during exercise. During a 6-minute walk test (6MWT) without supplemental oxygen, the patient's oxygen saturation decreased from 88% to 77%, and his pulse rate increased from 84 to 92 beats/min (total distance, 363 m). The patient underwent TEE with agitated-saline contrast, which showed a moderate-sized, interatrial RL shunt generated during the Valsalva maneuver (Figs. 1A, 1B, and 2A). Left- and right-sided cardiac catheterization results included an RA pressure of 12 mmHg, a systolic PAP of 35 mmHg, a pulmonary vein saturation of 98%, and a pulmonary capillary wedge pressure (PCWP) of 9 mmHg. Coronary angiograms revealed only mild, nonobstructive coronary artery disease. On intracardiac echocardiography, a moderate-sized PFO (tunnel length, 6 mm) was confirmed; there was no septal aneurysm, significant tricuspid regurgitation, or prominent eustachian valve. The RL shunt was determined to be caused by the PFO, with shunting exacerbated by the patient's elevated RA pressure caused by COPD. The PFO was closed with a 25-mm Gore Helex® septal occluder (W.L. Gore & Associates, Inc.; Flagstaff, Ariz) and confirmed by postprocedural color-Doppler TEE (Fig. 1C) and 3-dimensional TEE with agitated-saline contrast medium (Fig. 2B). After closure, oxygen saturation rose to 91% at rest without supplemental oxygen. One month after closure, TTE revealed unchanged pulmonary artery and RA pressures, and there were no obvious leaks around the closure device. In a post-procedural 6MWT without supplemental oxygen, the patient's total walking distance increased to 422 m; his oxygen saturation decreased from 92% to 84%; and his pulse rate increased from 78 beats/min to 91 beats/min. He reported symptomatic improvement of his dyspnea during exertion.
Fig. 1.
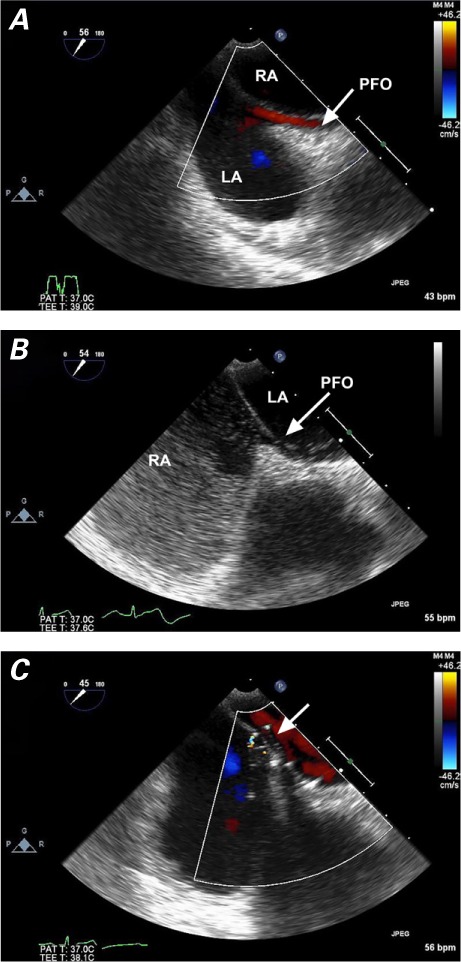
Patient 1. Transesophageal echocardiograms (mid-esophageal, bicaval view) show an interatrial right-to-left shunt in a patient whose hypoxemia was out of proportion to his chronic obstructive pulmonary disease. A) Color-flow Doppler mode shows flow across the patent foramen ovale (PFO) from the right atrium (RA) to the left atrium (LA). B) Agitated-saline contrast injection reveals shunting of bubbles from the RA to the LA through the PFO. C) After patent foramen ovale closure with a Gore Helex septal occluder (arrow), color-flow Doppler mode reveals no residual flow.
Fig. 2.
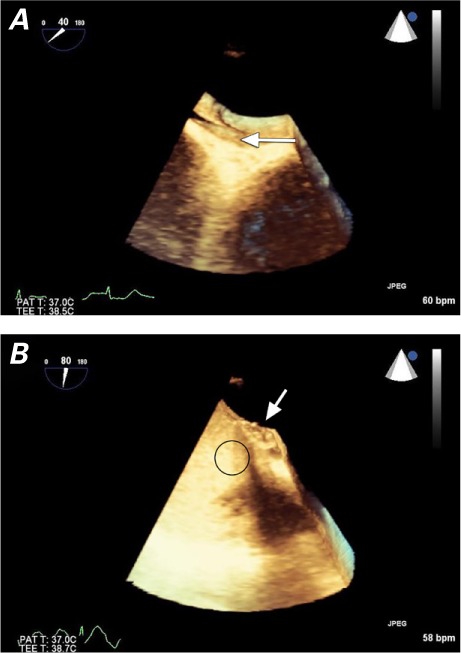
Patient 1. Three-dimensional, volume-rendered, transesophageal echocardiograms show A) the interatrial shunt before closure of the patent foramen ovale (arrow), and B) no residual shunting after closure with a Gore Helex septal occluder (arrow), upon agitated-saline contrast injection (oval).
Patient 2. A 59-year-old man was referred to our clinic by his pulmonologist to be considered for percutaneous PFO closure in the presence of progressive, exercise-induced hypoxemia. The patient's medical history was significant for diabetes mellitus, obstructive sleep apnea (treated with noninvasive positive-pressure ventilation at night), asthma with COPD (FEV1, 55%) and morbid obesity (body mass index, 44 kg/m2). The patient reported no history of tobacco use and had no known coronary artery disease. He had experienced gradually worsening hypoxemia; his resting oxygen saturation was 94%, and it fell to 87% with only mild exertion. In the presence of an unchanged pulmonary function test, the pulmonologist was concerned that the patient's hypoxemia seemed excessive for the extent of his chronic pulmonary dysfunction. A TEE from the referring center, which had been performed with agitated-saline contrast medium, showed an interatrial RL shunt; normal atrial pressures and normal PAP were noted. Results of left- and right-sided cardiac catheterization included a systolic PAP of 40 mmHg, normal PCWP, and no coronary artery disease. The patient's worsening hypoxemia was attributed to the increased RL shunt through the PFO in the presence of obstructive sleep apnea, COPD, and morbid obesity. His pulmonologist and cardiologist decided that PFO closure might improve his oxygenation. During right-sided heart catheterization with intracardiac echocardiographic imaging, an 18-mm PFO (measured through balloon sizing) was revealed (Fig. 3); no septal aneurysm, significant tricuspid regurgitation, or prominent eustachian valve was detected. The PFO was closed with a 19-mm Amplatzer® Atrial Septal Defect Occluder (St. Jude Medical, part of Abbott Laboratories; St. Paul, Minn) (Fig. 4). A postdeployment color-flow Doppler study confirmed successful sealing with no interatrial communication. Within several days of closure, the patient reported subjective improvement in dyspnea and exercise capacity. His oxygen saturation remained at 94% at rest and during exertion.
Fig. 3.
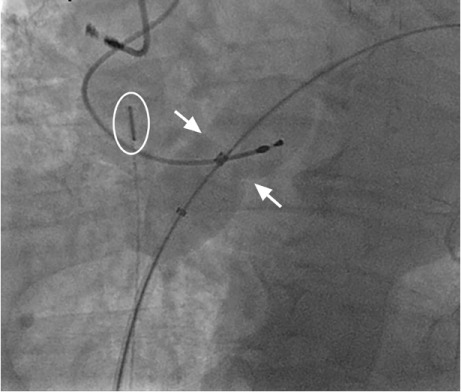
Patient 2. Fluoroscopic image shows balloon sizing for patent foramen ovale (PFO) closure. The balloon catheter was placed over a guidewire and passed across the PFO and into the left atrium. The balloon was inflated gently until an indentation was seen at the level of the PFO (arrows) and there was no flow around the balloon, as determined by Doppler-flow imaging through an intracardiac echocardiographic catheter (oval).
Fig. 4.
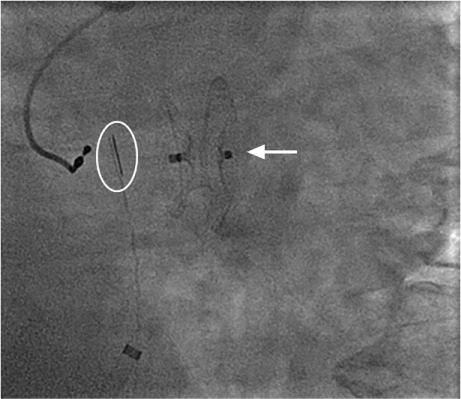
Patient 2. Fluoroscopic image shows a 19-mm Amplatzer Atrial Septal Defect Occluder (arrow) in place across the interatrial septum, after release from the delivery cable. An intracardiac echocardiographic catheter (oval) is also seen.
Pulmonary Hypertension and COPD with Patent Foramen Ovale
Patients classified by the World Health Organization as having group 3 pulmonary hypertension (PH), which includes PH associated with lung diseases and sleep-related breathing disorders, are more likely to have severe COPD, and up to 30% of patients with moderate-to-severe COPD have elevated pulmonary pressures that correlate with lower 5-year survival rates when the mean PAP exceeds 25 mmHg.54–57 Hypoxemia in COPD is thought to be caused by a ventilation-perfusion mismatch, in which unoxygenated blood is directed through capillaries that feed nonfunctional alveoli. As COPD progresses, PAP rises because of hypoxia-induced pulmonary vasoconstriction, and RA pressure subsequently increases.58,59 If PFO is present, elevated RA pressure can increase the degree of RL shunting, worsening hypoxemia beyond the level expected based on the patient's degree of pulmonary disease.11,60–62 Conversely, RL shunting in a patient with PFO can be minimized with the use of supplemental oxygen, inhaled nitrous oxide, or a phosphodiesterase (PDE)-5 inhibitor, which reduce the hypoxia-driven rise in PAP. Boerrigter and colleagues62 reported this phenomenon in 2 hypoxemic patients with PFO and PH secondary to COPD. When these patients were given supplemental oxygen, their PAP and arterial oxygenation improved substantially. In the first patient, the PFO was initially undetected on echocardiography, when the patient was not receiving supplemental oxygen. After percutaneous PFO closure, oxygen saturation improved from 71% with exertion to above 90%. The second patient did not undergo PFO closure.
Boerrigter and colleagues' report is consistent with those of earlier investigators who have identified an association between elevated PAP in COPD and RL shunting through a PFO.35,36,51,53,62 These findings indicate the need for further investigation of PFO closure in the presence of PH. In patients who are unsuitable for PFO closure, PDE-5 inhibitor therapy and inhaled nitrous oxide are promising; several case reports have described improved arterial oxygenation after initiation of these therapies.62–65 Larger studies are warranted to elucidate their potential benefit.
Hypoxemia with Patent Foramen Ovale
There appears to be an association between PFO and hypoxemia in certain chronic pulmonary diseases; however, the challenge is separating the degree of hypoxemia caused by an intracardiac shunt from that caused by a pulmonary shunt. Theoretically, these 2 causes can be distinguished from one another by calculating the shunt fraction while a patient is on 100% supplemental oxygen. In reality, though, the dynamic nature of an RL shunt—which might be present only during the Valsalva maneuver or throughout the respiratory cycle—makes it challenging to quantify what degree of shunting causes clinically noticeable hypoxemia. With the increased use of cardiac magnetic resonance imaging, the shunt fraction can be estimated by measuring the ratio of pulmonary blood flow to systemic blood flow (often measured in the pulmonary artery and aorta, respectively).66 Hypoxemia produced by an intracardiac RL shunt can be confirmed using right-sided heart catheterization. The oxygen saturation in the pulmonary veins, measured by crossing the PFO, can be compared to the systemic arterial oxygen saturation. In the presence of systemic hypoxemia, low pulmonary venous oxygen saturation levels would indicate pulmonary disease as the main culprit, whereas normal pulmonary venous oxygen saturation would indicate that the intracardiac RL shunt is the cause of hypoxemia.51 Alternatively, the partial pressure of oxygen in arterial blood can be compared at rest and after balloon occlusion of the PFO. If the cardiac RL shunt is the main contributor to hypoxemia, balloon occlusion of the PFO should raise systemic oxygen levels.
Although an RL shunt through a PFO can alter systemic oxygen levels, its effect on exercise tolerance is unclear. Hacievliyagil and colleagues36 reported lower systemic and pulmonary oxygen saturation levels, higher dyspnea scores, shorter distances walked during a 6MWT, and higher desaturation rates in COPD patients with a PFO compared to those without a PFO. Martolini and colleagues52 also found an association between PFO and reduced systemic and pulmonary oxygen levels, although they observed preserved exercise tolerance in patients with PFO, noting that RL shunting, recorded as the number of HITS observed, was greater in PFO patients during a 6MWT. Similarly, Shaikh and colleagues53 reported increased shunting in PFO patients during exercise, but the patients' functional capacities were preserved. Future studies should not only measure shunting and oxygen saturations in PFO patients, but also evaluate functional testing as a primary metric, because the severity of RL shunting might not necessarily correlate with clinical symptoms.
There remains a paucity of prospective data for oxygen-saturation status before and after PFO closure in patients with chronic pulmonary disease. Ilkhanoff and colleagues67 found that, in their study of patients with interatrial septal defects (including PFO), mean arterial oxygen saturation improved from 86.7% to 95.9% (P=0.002) after closure. Although the immediate post-procedural improvement of hypoxemia in these patients is encouraging, the short follow-up period and lack of pre- versus postprocedural clinical metrics makes extrapolating the outcome to other patients challenging. In their retrospective study of 9 patients with chronic pulmonary disease, El Tahlawi and co-authors68 found no significant improvement in New York Heart Association (NYHA) functional class after PFO closure and concluded that hypoxemia in this patient group was more likely related to pulmonary shunting than to intracardiac shunting. Conversely, Devendra and associates37 reported improved oxygen saturation (10.1% average improvement; P <0.001) and NYHA functional class (1.5 median improvement in class; P=0.008) in 10 patients with PFO and exercise-induced hypoxemia after PFO closure. More recently, a larger study of 97 patients with underlying chronic pulmonary disease showed that patients had an improvement ≥I in NYHA functional class (51% of patients; P <0.001) and reduced supplemental oxygen requirements (34% of patients; P <0.001) after PFO closure. Using contrast TTE, the authors of the study determined that having a larger RL shunt was associated with a greater likelihood of clinical improvement after closure (P <0.0087).61 Although limitations exist in this single-arm study, its finding that there is the potential for improved functional status after PFO closure suggests that a prospective, randomized study using similar metrics would be instructive.
Evaluating the Role of Patent Foramen Ovale Closure
Which chronic pulmonary disease patients would benefit from PFO closure remains unclear. Fenster and Carroll60 outlined the discrepancies of hypoxemia in RL shunting and called for a multidisciplinary study to adequately address the management of patients with chronic pulmonary disease and PFO. A study of this magnitude would need to take several key factors into consideration: for example, determining whether PFO closure is suitable only in patients with larger grades of RL shunting (≥ grade 4 as established by TCD).53,61 Restricting PFO closure to this group would prevent unnecessary procedures in patients whose PFOs are unlikely to produce hypoxemia. Patients with anatomic variants—including shunts of various sizes, atrial septal aneurysms, tricuspid regurgitation, and residual eustachian valves—might also benefit from screening and RL shunt correction.
In future clinical trials, the preferred imaging method for initial PFO screening should also be established. Because the quality of TTE images is often poor in COPD patients who have hyperinflated lungs, TCD, which is more sensitive, might prove more useful for initial screening.48 Patients suspected of having a large RL shunt could then undergo TEE to confirm the presence of a PFO, which could finally be verified by right-sided heart catheterization. Care must be taken to differentiate between patients with hypoxemia due to intracardiac shunting as opposed to other pulmonary diseases. Echocardiography in tandem with cardiac magnetic resonance could be another option to screen for PFO, enabling shunt fractions to be calculated and a diagnosis of PFO to be ruled out in patients with intrapulmonary shunts. Cardiac magnetic resonance would also be helpful in conducting further research to quantify the relationship between the degree of shunting and onset of clinically significant hypoxemia.
Closure of PFOs in patients with PH is controversial. Although elevated PAP in the presence of PFO can exacerbate hypoxemia, closing a PFO in patients with PH might be detrimental, because the RL shunt might act as a “pop-off ” valve, diminishing the effect of high PAP on the right side of the heart. Prior reports of PFO closure in PH have not described any incidents of right ventricular failure.27,62 In general, however, PFO closure in a patient with PH is considered unsafe and is not advised until more outcome data are available. In the meantime, pharmacologic intervention with inhaled PDE-5 inhibitors or nitrous oxide has shown promising results in these patients.
Clinical metrics to analyze, before and after PFO closure, include submaximal exercise capacity (6MWT) and maximal exercise capacity with use of cardiopulmonary exercise variables (oxygen consumption and anaerobic thresholds). The long-term consequences of PFO closure on a patient's functional capacity, quality of life, supplemental oxygen use, likelihood of hospitalization, and need for lung transplantation should also be considered. Given the potential impact of interventional PFO closure on public health, the cost-to-benefit ratio of this treatment deserves focused attention. Although it is still challenging to identify the appropriate cohort for intervention, we hypothesize that, in certain chronic pulmonary disease patients with hypoxemia, PFO closure might result in substantial improvements in quality of life.
References
- 1. Smith B, . editor Large animal internal medicine. St. Louis: Mosby; 2002. p 452. [Google Scholar]
- 2. Beard RW. Fetal physiology and medicine: the basis of perinatology (reproductive medicine). New York: Marcel Dekker Inc.; 1984. p 300. [Google Scholar]
- 3. Nootens MT, Berarducci LA, Kaufmann E, Devries S, Rich S.. The prevalence and significance of a patent foramen ovale in pulmonary hypertension. Chest 1993; 104 6: 1673– 5. [DOI] [PubMed] [Google Scholar]
- 4. Sardesai SH, Marshall RJ, Mourant AJ.. Paradoxical systemic embolisation through a patent foramen ovale. Lancet 1989; 1 8640: 732– 3. [DOI] [PubMed] [Google Scholar]
- 5. Movsowitz C, Podolsky LA, Meyerowitz CB, Jacobs LE, Kotler MN.. Patent foramen ovale: a nonfunctional embryological remnant or a potential cause of significant pathology? J Am Soc Echocardiogr 1992; 5 3: 259– 70. [DOI] [PubMed] [Google Scholar]
- 6. Lynch JJ, Schuchard GH, Gross CM, Wann LS.. Prevalence of right-to-left atrial shunting in a healthy population: detection by Valsalva maneuver contrast echocardiography. Am J Cardiol 1984; 53 10: 1478– 80. [DOI] [PubMed] [Google Scholar]
- 7. Di Tullio MR, Sacco RL, Sciacca RR, Jin Z, Homma S.. Patent foramen ovale and the risk of ischemic stroke in a multi-ethnic population. J Am Coll Cardiol 2007; 49 7: 797– 802. [DOI] [PubMed] [Google Scholar]
- 8. Meissner I, Khandheria BK, Heit JA, Petty GW, Sheps SG, Schwartz GL, . et al. Patent foramen ovale: innocent or guilty? Evidence from a prospective population-based study. J Am Coll Cardiol 2006; 47 2: 440– 5. [DOI] [PubMed] [Google Scholar]
- 9. Vale TA, Newton JD, Orchard E, Bhindi R, Wilson N, Ormerod OJ.. Prominence of the eustachian valve in paradoxical embolism. Eur J Echocardiogr 2011; 12 1: 33– 6. [DOI] [PubMed] [Google Scholar]
- 10. Cheng TO. Reversible orthodeoxia. Ann Intern Med 1992; 116 10: 875. [DOI] [PubMed] [Google Scholar]
- 11. Cheng TO. Mechanisms of platypnea-orthodeoxia: what causes water to flow uphill? Circulation 2002; 105 6: e47. [PubMed] [Google Scholar]
- 12. Hsu PF, Leu HB, Lu TM, Yu WC, Hsu TL.. Platypnea-orthodeoxia syndrome occurring after a blunt chest trauma with acute tricuspid regurgitation. Am J Med 2004; 117 11: 890– 1. [DOI] [PubMed] [Google Scholar]
- 13. Alsheikh-Ali AA, Thaler DE, Kent DM.. Patent foramen ovale in cryptogenic stroke: incidental or pathogenic? Stroke 2009; 40 7: 2349– 55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Overell JR, Bone I, Lees KR.. Interatrial septal abnormalities and stroke: a meta-analysis of case-control studies. Neurology 2000; 55 8: 1172– 9. [DOI] [PubMed] [Google Scholar]
- 15. Estagnasie P, Djedaini K, Le Bourdelles G, Coste F, Dreyfuss D.. Atrial septal aneurysm plus a patent foramen ovale. A predisposing factor for paradoxical embolism and refractory hypoxemia during pulmonary embolism. Chest 1996; 110 3: 846– 8. [DOI] [PubMed] [Google Scholar]
- 16. Knapper JT, Schultz J, Das G, Sperling LS.. Cardiac platypnea-orthodeoxia syndrome: an often unrecognized malady. Clin Cardiol 2014; 37 10: 645– 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Semet F, Hascoet S, Dauphin C, Berry M, Bouisset F, Gautier M, . et al. Platypnea orthodeoxia syndrome: focus on predisposing anatomical factors [abstract]. Arch Cardiovasc Dis Suppls 2015; 7 1: 49 Available from: http://www.sciencedirect.com/science/article/pii/S1878648015716290. [Google Scholar]
- 18. Carroll JD, Saver JL, Thaler DE, Smalling RW, Berry S, MacDonald LA, . et al. Closure of patent foramen ovale versus medical therapy after cryptogenic stroke. N Engl J Med 2013; 368 12: 1092– 100. [DOI] [PubMed] [Google Scholar]
- 19. Kasper W, Geibel A, Tiede N, Just H.. Patent foramen ovale in patients with haemodynamically significant pulmonary embolism. Lancet 1992; 340 8819: 561– 4. [DOI] [PubMed] [Google Scholar]
- 20. Morthy SS, Losasso AM, Gibbs PS.. Acquired right-to-left intracardiac shunts and severe hypoxemia. Crit Care Med 1978; 6 1: 28– 31. [DOI] [PubMed] [Google Scholar]
- 21. Wendel CH, Dianzumba S, Joyner CR.. Right-to-left inter-atrial shunt secondary to an extensive right ventricular myocardial infarction. Clin Cardiol 1985; 8 4: 230– 2. [DOI] [PubMed] [Google Scholar]
- 22. Lemaire F, Richalet JP, Carlet J, Brun-Buisson C, MacLean C.. Postoperative hypoxemia due to opening of a patent foramen ovale confirmed by a right atrium-left atrium pressure gradient during mechanical ventilation. Anesthesiology 1982; 57 3: 233– 6. [DOI] [PubMed] [Google Scholar]
- 23. Wilmshurst PT, Byrne JC, Webb-Peploe MM.. Relation between interatrial shunts and decompression sickness in divers. Lancet 1989; 2 8675: 1302– 6. [DOI] [PubMed] [Google Scholar]
- 24. Moon RE, Camporesi EM, Kisslo JA.. Patent foramen ovale and decompression sickness in divers. Lancet 1989; 1 8637: 513– 4. [DOI] [PubMed] [Google Scholar]
- 25. Schwerzmann M, Wiher S, Nedeltchev K, Mattle HP, Wahl A, Seiler C, . et al. Percutaneous closure of patent foramen ovale reduces the frequency of migraine attacks. Neurology 2004; 62 8: 1399– 401. [DOI] [PubMed] [Google Scholar]
- 26. Seward JB, Hayes DL, Smith HC, Williams DE, Rosenow EC 3rd, Reeder GS, . et al. Platypnea-orthodeoxia: clinical profile, diagnostic workup, management, and report of seven cases. Mayo Clin Proc 1984; 59 4: 221– 31. [DOI] [PubMed] [Google Scholar]
- 27. Mehrotra AK, Cork DP, Weiss SA, Shah AP.. Dramatic improvement in hypoxemic respiratory failure after patent foramen ovale closure in a patient with obesity hypoventilation syndrome. Cardiovasc Revasc Med 2012; 13 5: 295– 7. [DOI] [PubMed] [Google Scholar]
- 28. Post MC, Thijs V, Herroelen L, Budts WI.. Closure of a patent foramen ovale is associated with a decrease in prevalence of migraine. Neurology 2004; 62 8: 1439– 40. [DOI] [PubMed] [Google Scholar]
- 29. Wilmshurst PT, Nightingale S, Walsh KP, Morrison WL.. Effect on migraine of closure of cardiac right-to-left shunts to prevent recurrence of decompression illness or stroke or for haemodynamic reasons. Lancet 2000; 356 9242: 1648– 51. [DOI] [PubMed] [Google Scholar]
- 30. Ptaszek LM, Saldana F, Palacios IF, M Wu S.. Platypnea-orthodeoxia syndrome in two previously healthy adults: a case-based review. Clin Med Cardiol 2009; 3: 37– 43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Kyroussis D, Polkey MI, Hamnegard CH, Mills GH, Green M, Moxham J.. Respiratory muscle activity in patients with COPD walking to exhaustion with and without pressure support. Eur Respir J 2000; 15 4: 649– 55. [DOI] [PubMed] [Google Scholar]
- 32. Maltais F, Reissmann H, Gottfried SB.. Pressure support reduces inspiratory effort and dyspnea during exercise in chronic airflow obstruction. Am J Respir Crit Care Med 1995; 151 4: 1027– 33. [DOI] [PubMed] [Google Scholar]
- 33. Raeside DA, Brown A, Patel KR, Welsh D, Peacock AJ.. Ambulatory pulmonary artery pressure monitoring during sleep and exercise in normal individuals and patients with COPD. Thorax 2002; 57 12: 1050– 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Hopkinson NS, Dayer MJ, Moxham J, Polkey MI.. Abdominal muscle fatigue following exercise in chronic obstructive pulmonary disease. Respir Res 2010; 11: 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Soliman A, Shanoudy H, Liu J, Russell DC, Jarmukli NF.. Increased prevalence of patent foramen ovale in patients with severe chronic obstructive pulmonary disease. J Am Soc Echocardiogr 1999; 12 2: 99– 105. [DOI] [PubMed] [Google Scholar]
- 36. Hacievliyagil SS, Gunen H, Kosar FM, Sahin I, Kilic T.. Prevalence and clinical significance of a patent foramen ovale in patients with chronic obstructive pulmonary disease. Respir Med 2006; 100 5: 903– 10. [DOI] [PubMed] [Google Scholar]
- 37. Devendra GP, Rane AA, Krasuski RA.. Provoked exercise de-saturation in patent foramen ovale and impact of percutaneous closure. JACC Cardiovasc Interv 2012; 5 4: 416– 9. [DOI] [PubMed] [Google Scholar]
- 38. Siddiqi A, Sethi S.. Optimizing antibiotic selection in treating COPD exacerbations. Int J Chron Obstruct Pulmon Dis 2008; 3 1: 31– 44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Croxton TL, Bailey WC.. Long-term oxygen treatment in chronic obstructive pulmonary disease: recommendations for future research: an NHLBI workshop report. Am J Respir Crit Care Med 2006; 174 4: 373– 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Doherty DE, Petty TL, Bailey W, Carlin B, Cassaburi R, Christopher K, . et al. Recommendations of the 6th long-term oxygen therapy consensus conference. Respir Care 2006; 51 5: 519– 25. [PubMed] [Google Scholar]
- 41. Fisher DC, Fisher EA, Budd JH, Rosen SE, Goldman ME.. The incidence of patent foramen ovale in 1,000 consecutive patients. A contrast transesophageal echocardiography study. Chest 1995; 107 6: 1504– 9. [DOI] [PubMed] [Google Scholar]
- 42. Luotolahti M, Saraste M, Hartiala J.. Saline contrast and colour Doppler transoesophageal echocardiography in detecting a patent foramen ovale and right-to-left shunts in stroke patients. Clin Physiol 1995; 15 3: 265– 73. [DOI] [PubMed] [Google Scholar]
- 43. Zito C, Dattilo G, Oreto G, Di Bella G, Lamari A, Iudicello R, . et al. Patent foramen ovale: comparison among diagnostic strategies in cryptogenic stroke and migraine. Echocardiography 2009; 26 5: 495– 503. [DOI] [PubMed] [Google Scholar]
- 44. Gonzalez-Alujas T, Evangelista A, Santamarina E, Rubiera M, Gomez-Bosch Z, Rodriguez-Palomares JF, . et al. Diagnosis and quantification of patent foramen ovale. Which is the reference technique? Simultaneous study with transcranial Doppler, transthoracic and transesophageal echocardiography [in English, Spanish]. Rev Esp Cardiol 2011; 64 2: 133– 9. [DOI] [PubMed] [Google Scholar]
- 45. Van H, Poommipanit P, Shalaby M, Gevorgyan R, Tseng CH, Tobis J.. Sensitivity of transcranial Doppler versus intracardiac echocardiography in the detection of right-to-left shunt [published erratum appears in JACC Cardiovasc Imaging 2014;7(1):117]. JACC Cardiovasc Imaging 2010; 3 4: 343– 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Alibegovic J, Bonvini R, Sigwart U, Dorsaz P, Camenzind E, Verin V.. The role of the sizing balloon in selection of the patent foramen ovale closure device size. Exp Clin Cardiol 2008; 13 1: 42– 6. [PMC free article] [PubMed] [Google Scholar]
- 47. Rana BS, Thomas MR, Calvert PA, Monaghan MJ, Hildick-Smith D.. Echocardiographic evaluation of patent foramen ovale prior to device closure. JACC Cardiovasc Imaging 2010; 3 7: 749– 60. [DOI] [PubMed] [Google Scholar]
- 48. Spencer MP, Moehring MA, Jesurum J, Gray WA, Olsen JV, Reisman M.. Power m-mode transcranial Doppler for diagnosis of patent foramen ovale and assessing transcatheter closure. J Neuroimaging 2004; 14 4: 342– 9. [DOI] [PubMed] [Google Scholar]
- 49. Mojadidi MK, Gevorgyan R, Tobis JM.. A comparison of methods to detect and quantitate PFO: TCD, TTE, ICE and TEE. : Amin Z, Tobis JM, Sievert H, Carroll JD, . Patent foramen ovale. Springer-Verlag; London; 2015. p 55– 65. [Google Scholar]
- 50. Caputi L, Carriero MR, Falcone C, Parati E, Piotti P, Materazzo C, Anzola GP.. Transcranial Doppler and transesophageal echocardiography: comparison of both techniques and prospective clinical relevance of transcranial Doppler in patent foramen ovale detection. J Stroke Cerebrovasc Dis 2009; 18 5: 343– 8. [DOI] [PubMed] [Google Scholar]
- 51. Kilic H, Balci MM, Aksoy MN, Bilgin E, Gulsoy KG, Yeter E, . et al. Patent foramen ovale among patients with mild chronic obstructive pulmonary disease and unexplained hypoxia. Echocardiography 2010; 27 6: 687– 90. [DOI] [PubMed] [Google Scholar]
- 52. Martolini D, Tanner R, Davey C, Patel MS, Elia D, Purcell H, . et al. Significance of patent foramen ovale in patients with GOLD Stage II chronic obstructive pulmonary disease. J COPD F 2014; 1 2: 185– 92. Available from: https://journal.copdfoundation.org/Portals/0/JCOPDF/Files/Volume1-Issue2/JCOPDF-2013-0003-Polkey.pdf. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Shaikh ZF, Kelly JL, Shrikrishna D, de Villa M, Mullen MJ, Hopkinson NS, . et al. Patent foramen ovale is not associated with hypoxemia in severe chronic obstructive pulmonary disease and does not impair exercise performance. Am J Respir Crit Care Med 2014; 189 5: 540– 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Renzetti AD Jr, McClement JH, Litt BD.. The Veterans Administration cooperative study of pulmonary function. 3. Mortality in relation to respiratory function in chronic obstructive pulmonary disease. Am J Med 1966; 41 1: 115– 29. [DOI] [PubMed] [Google Scholar]
- 55. Jones NL, Burrows B, Fletcher CM.. Serial studies of 100 patients with chronic airway obstruction in London and Chicago. Thorax 1967; 22 4: 327– 35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Elwing J, Panos RJ.. Pulmonary hypertension associated with COPD. Int J Chron Obstruct Pulmon Dis 2008; 3 1: 55– 70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Oswald-Mammosser M, Weitzenblum E, Quoix E, Moser G, Chaouat A, Charpentier C, Kessler R.. Prognostic factors in COPD patients receiving long-term oxygen therapy. Importance of pulmonary artery pressure. Chest 1995; 107 5: 1193– 8. [DOI] [PubMed] [Google Scholar]
- 58. Marshall C, Marshall B.. Site and sensitivity for stimulation of hypoxic pulmonary vasoconstriction. J Appl Physiol Respir Environ Exerc Physiol 1983; 55 3: 711– 6. [DOI] [PubMed] [Google Scholar]
- 59. Moudgil R, Michelakis ED, Archer SL.. Hypoxic pulmonary vasoconstriction. J Appl Physiol (1985) 2005; 98 1: 390– 403. [DOI] [PubMed] [Google Scholar]
- 60. Fenster BE, Carroll JD.. Patent foramen ovale in COPD and hypoxia: innocent bystander or novel therapeutic target? Chronic Obstr Pulm Dis (Miami) 2014; 1 2: 151– 4. Available from: https://journal.copdfoundation.org/jcopdf/id/1038/Patent-Foramen-Ovale-in-COPD-and-Hypoxia-Innocent-Bystander-or-Novel-Therapeutic-Target. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Fenster BE, Nguyen BH, Buckner JK, Freeman AM, Carroll JD.. Effectiveness of percutaneous closure of patent foramen ovale for hypoxemia. Am J Cardiol 2013; 112 8: 1258– 62. [DOI] [PubMed] [Google Scholar]
- 62. Boerrigter BG, Boonstra A, Westerhof N, Postmus PE, Vonk-Noordegraaf A.. Cardiac shunt in COPD as a cause of severe hypoxaemia: probably not so uncommon after all. Eur Respir J 2011; 37 4: 960– 2. [DOI] [PubMed] [Google Scholar]
- 63. Elias S, Sviri S, Orenbuch-Harroch E, Fellig Y, Ben-Yehuda A, Fridlender ZG, . et al. Sildenafil to facilitate weaning from inhaled nitric oxide and mechanical ventilation in a patient with severe secondary pulmonary hypertension and a patent foramen ovale. Respir Care 2011; 56 10: 1611– 3. [DOI] [PubMed] [Google Scholar]
- 64. Pitsiou GG, Chavouzis N, Nakou C, Boutou AK, Argyropoulou P, Stanopoulos I.. Successful up-front combination therapy in a patient with idiopathic pulmonary hypertension and patent foramen ovale: an alternative to epoprostenol therapy? J Heart Lung Transplant 2009; 28 6: 651– 3. [DOI] [PubMed] [Google Scholar]
- 65. Karakaya O, Ozdemir N, Kaymaz C, Barutcu I.. Dramatic decrease in the pulmonary artery systolic pressure and disappearance of the interatrial shunt with sildenafil treatment in a patient with primary pulmonary hypertension with atrial septal aneurysm and a severe right to left shunt through the patent foramen ovale. Int J Cardiol 2006; 110 1: 97– 9. [DOI] [PubMed] [Google Scholar]
- 66. Rajiah P, Kanne JP.. Cardiac MRI: Part 1, cardiovascular shunts. AJR Am J Roentgenol 2011; 197 4: W603– 20. [DOI] [PubMed] [Google Scholar]
- 67. Ilkhanoff L, Naidu SS, Rohatgi S, Ross MJ, Silvestry FE, Herrmann HC.. Transcatheter device closure of interatrial septal defects in patients with hypoxia. J Interv Cardiol 2005; 18 4: 227– 32. [DOI] [PubMed] [Google Scholar]
- 68. El Tahlawi M, Jop B, Bonello B, Dragulescu A, Rouault F, Habib G, Fraisse A.. Should we close hypoxaemic patent foramen ovale and interatrial shunts on a systematic basis? Arch Cardiovasc Dis 2009; 102 11: 755– 9. [DOI] [PubMed] [Google Scholar]