

Abstract
Economic and societal pressures influence modern medical practice to develop and implement prevention strategies. Anterior cruciate ligament (ACL) injury devastates the knee joint leading to short term disability and long term sequelae. Due to the high risk of long term osteoarthritis in all treatment populations following ACL injury, prevention is the only effective intervention for this life-altering disruption in knee health. The “Sequence of Prevention” Model provides a framework to monitor progress towards the ultimate goal of preventing ACL injuries. Utilizing this model, our multidisciplinary collaborative research team has spent the last decade working to delineate injury mechanisms, identify injury risk factors, predict which athletes are at-risk for injury, and develop ACL injury prevention programs. Within this model of injury prevention, modifiable factors (biomechanical and neuromuscular) related to injury mechanisms likely provide the best opportunity for intervention strategies aimed to decrease the risk of ACL injury, particularly in female athletes. Knowledge advancements have led to the development of potential solutions that allow athletes to compete with lowered risk of ACL injury. Design and integration of personalized clinical assessment tools and targeted prevention strategies for athletes at high risk for ACL injury may transform current prevention practices and ultimately significantly reduce ACL injury incidence. This 2016 OREF Clinical Research Award focuses on the authors' work and contributions to the field. The author's acknowledge the many research groups who have contributed to the current state of knowledge in the fields of ACL injury mechanisms, injury risk screening and injury prevention strategies.
Keywords: tendon and ligament, biomaterials
Establishment of the Extent of the Acl Injury Problem
Anterior cruciate ligament (ACL) injury in a young athlete leads to short term disability, possible loss of scholarship funding and often results in knee articular cartilage destruction and osteoarthritis as early as 10 years after the initial injury insult. 1–8 Since 1980, it is estimated that more than 1.5 million ACL reconstructions were performed in the United States with the expectation that reestablishment of knee joint stability would prevent risk of further joint degeneration. 9,10 With estimated costs for treatment in ACL injured patients in the United States over three billion dollars annually, the physical, emotional and financial consequences for patients, families, and the orthopaedic community are profound.9–11
Adolescent and mature females who participate in pivoting and jumping sports suffer anterior cruciate ligament (ACL) injuries at a 2- to 10-fold greater rate than male athletes participating in the same high-risk cutting and landing sports.12–17 The combination of this greater susceptibility and a 10-fold increase in the female sports population since the inception of Title IX has resulted in a dramatic increase in the number of ACL injuries in females.16 In the United States, 100,000–250,000 ACL injuries occur each year. 11,18 The costs exceed $650 million annually in female varsity athletics alone.19 Neuromuscular control deficits at the hip and trunk may contribute to decreased active neuromuscular control of the lower extremity (LE) that may lead to increased knee abduction loads and strain on the knee ligaments.20–23 The costs associated with ACL injury do not end with the ACL reconstruction and rehabilitation. There is a strong association between ACL injury and development of posttraumatic knee osteoarthritis at a relatively young age, which also occurs with much greater incidence in females than males.7,24 It is estimated that between 50% and 100% of women with an ACL injury will show significant pain, functional limitations, and radiographic signs of knee osteoarthritis within 12–20 years of the index injury.5,7
Although surgical techniques and rehabilitation programs have significantly improved over the past two decades, long-term follow-up studies indicate that restoration of knee joint laxity does not appear to correlate with clinical outcomes. ACL injured patients exhibit osteoarthritis symptoms and radiographic evidence of knee joint degeneration, irrespective of surgical intervention.4,5 Thus, the initial joint trauma suffered during the ACL injury event may serve as a major precursor to joint degeneration that may not be avoided despite ACL reconstruction. 5 In order for many young adults to safely participate and enjoy the health benefits of sports and physical activity, prevention of ACL injury may be the most effective intervention.
Many intrinsic and extrinsic risk factors have been theorized to place certain athletes at risk for ACL injury. Even though an athlete exhibits predisposing factors that may place them at high risk for ACL injury, this does not guarantee they will tear their ACL. An inciting event (mechanism of injury) must occur that leads to the ACL injury. To achieve the ultimate goal of ACL injury reduction in high-risk populations, it is important to both identify the risk factors that predispose an athlete to injury and clearly define what occurs during an inciting ACL injury event in order to develop the best intervention strategies for targeted treatments of risk factors.
Coronal plane knee motion and moments and trunk displacement predict ACL injury risk in female athletes. Knee abduction loads and neuromuscular control of the trunk both predict ACL injury risk with high sensitivity and specificity. Knee abduction load predicted ACL injury risk with 78% sensitivity and 73% specificity.22 Trunk displacement predicted risk of knee, knee ligament and ACL injuries with high sensitivity and specificity in female, but not male, athletes.25 A logistic regression model that incorporated lateral trunk motion predicted ACL injury risk in females with 83% sensitivity and 76% specificity, but did not predict knee or ACL injury risk in males. The mechanism of ACL injury may differ in females and males, especially with respect to the dynamic positioning of the knee, as females demonstrate greater valgus collapse of the LE primarily in the coronal plane.26 Most ACL injuries in females occur by non-contact mechanisms during landing and lateral pivoting.27 The mechanism of non-contact ACL injuries as observed on video has several common components in female athletes: high knee abduction, lateral trunk motion with the body shifted over one leg and the plantar surface of the foot fixed flat on the playing surface, displaced away from the trunk and low knee flexion.26–29 Unanticipated perturbation of the trunk is another common component of the mechanism.26
In 1992, van Mechelen and colleagues provided a framework to monitor progress in musculoskeletal injury prevention via the ‘Sequence of Prevention’ Model (Fig. 1).30 Within this model of injury prevention, our work over the past 15 years has focused on utilizing this model to target the most modifiable risk factors (biomechanical and neuromuscular) related to ACL injuries with the goal to provide the most effective interventions for the orthopaedic community. Specifically, we have focused on defining what are the underlying risk factors for ACL injury, who are the athletes at risk for ACL injury, and determination of when those athletes become most vulnerable to injury. In addition, we have targeted how to prevent ACL injury by identifying which prevention strategies are most effective and when implementation of these strategies offer the greatest benefit to young athletes. The current manuscript summarizes the findings of over 100 reports related to sequence of ACL injury prevention published by our research team from 1996 to 2016 presented in various orthopaedic, sports medicine, and biomechanic related peer-reviewed journals (Fig. 2). Our research was collectively funded by numerous institutions including the National Institutes of Health/NIAMS, The Orthopaedic Research and Education Foundation (OREF), National Football League Charities, American College of Sports Medicine, The Ohio State University Sports Health and Performance Institute, and the Cincinnati Children's Hospital Research Foundation.
Figure 1.
The Sequence of Prevention Model30 as described by van Mechelen et al.
Figure 2.
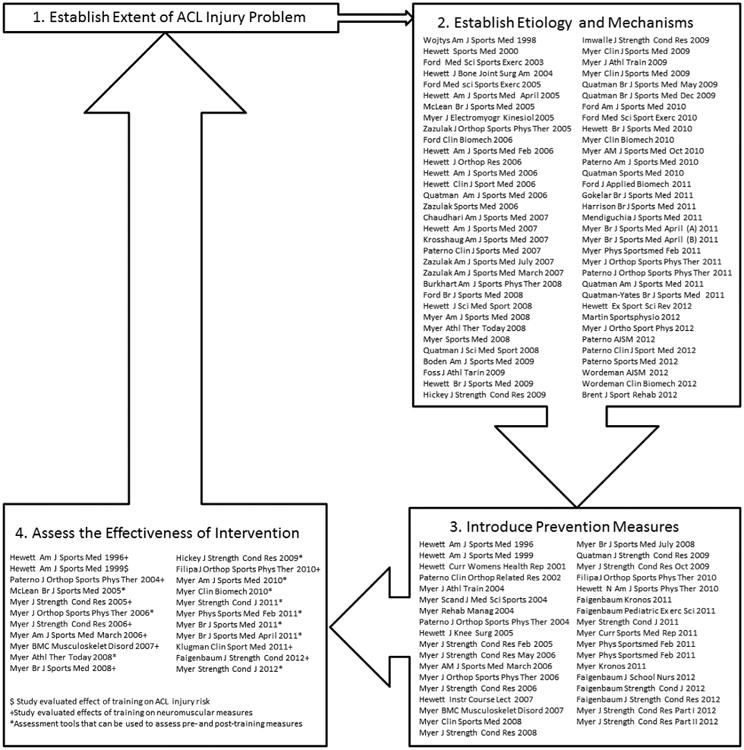
The Sequence of Prevention Model30 applied to ACL injury prevention measures explored in our laboratory. Published manuscripts available from our laboratory are categorized within the model.
Establish The Etiology And Modifiable Mechanisms Of Acl Injuries
Risk Factors
Female athletes have a 2–8 fold greater ACL injury rate compared to male athletes and it is estimated that 5% of female high school varsity athletes per year sustain a primary ACL injury.11,13,15,31 However, prior to puberty, ACL injuries are relatively rare and no sex-related differences in ACL ruptures are observed in pre-pubertal athletes.32,33 Females and males demonstrate important anatomical, hormonal, and neuromuscular factors differences after the onset of puberty which potentially influences the divergence in ACL injury rates between the sexes after puberty.34–36 It is theorized that males and females may even have different mechanisms of ACL injury.37,38
Sex and Hormonal Risk Factors
The sex differences in anatomy, hormones, neuromuscular control and biomechanics likely contribute to ACL injury rate disparity and have been explored extensively in our laboratory.35,39–51 Non-contact ACL injuries during sports likely occur within 30–100 ms from initial contact of the foot onto the ground during sports movements.38,52 Safe attenuation of landing forces and efficient neuromuscular control (recruitment of muscular restraints to resist perturbations and control dangerous external loads to the lower extremity) is essential for the prevention of injury during sports. Post-pubertal females exhibit greater landing forces and force loading rates, lower hamstrings to quadriceps torque ratios at high angular velocities and altered quadriceps and hamstrings activation strategies compared to males. Females may preferentially rely on higher activations of quadriceps muscles relative to hamstrings muscles with incremental increases in landing intensities.53 These neuromuscular differences in females may increase frontal plane knee motions and loads during sports movements.35,40–42,46,48–51,54–56 Post-pubertal females also demonstrate altered hip recruitment strategies for controlling landing with significantly greater hip moments, higher knee to hip moment ratios, decreased gluteus maximus activation, increased rectus femoris activation, and greater hip adduction angles and moments compared to males.39,47,49,57
A large systematic review performed by our group demonstrated that males and females differ in trunk and hip neuromuscular control and biomechanics in all planes of motion (sagittal, coronal, and transverse). Females show greater lateral trunk displacement, altered trunk and hip flexion angles, and greater ranges of trunk motion compared to males.58 The s ex differences in landing strategies combined with decreased torsional stiffness and increased joint laxity in females may increase females risk for ACL injury.41,45,47,59
After the onset of puberty, the sexes differ significantly in hormonal milieu. It has been postulated that the cyclic fluctuations of hormones during the follicular and ovulatory stages of the menstrual cycle may affect the mechanical properties of the ACL.42,60–64 Systematic reviews performed in our laboratory support the theory that the menstrual cycle may be associated with increased knee laxity and ACL injury.42,60,65,66 However, we found no effect of either the menstrual cycle or hormone stabilization (oral contraceptives) on knee or hip joint loading during high risk sport maneuvers.43 Currently, the downstream effects of female hormones associated with the menstrual cycle on ACL injury risk and the ability to modify these effects remain unclear.
Laxity
Evidence indicates that there may be a link between ACL injury and knee joint laxity and generalized joint laxity.59,67 The ovulatory phase of the menstrual cycle has been associated with increased knee joint laxity while the pre-ovulatory phase may be the phase during the cycle when females may be most at risk for ACL injury.65 Studies in our laboratory indicate that after the onset of puberty, females have significantly higher generalized joint laxity compared to males.45 Athletes with increased generalized joint laxity also demonstrate increased midfoot loading that may affect lower extremity biomechanics and potentially increase ACL injury risk.68 The associations between laxity and hormones, coupled with increased generalized joint laxity may contribute to the increased risk of ACL injury in female athletes after puberty.42,59,65 Although laxity may increase the risk for ACL injury, particularly in females, the ability to modify joint laxity presents a challenge. However, it may be possible to indirectly overcome the effects of joint laxity with increased muscular strength and heightened neuromuscular control.
Maturation
The rapid anatomic, hormonal, neuromuscular and biomechanical changes that occur during maturation differ significantly between the sexes and may partially explain the divergence in ACL injury rates between the sexes after puberty.35,50,69 Although often at different rates and chronological ages, both males and females undergo rapid increases in height and body mass that result in a higher center of mass and longer levers (femur and tibia) in the lower extremity. In contrast, our laboratory demonstrated that the sexes have significantly different neuromuscular and biomechanical changes that accompany puberty.39,40,44,70 Neuromuscular function appears to dynamically change throughout the adolescent time period and some individuals experience delays or even regressions in neuromuscular function.36,71 In addition, the importance and function of co-contraction of the hamstrings and quadriceps muscles related to age and skill development varies in the literature due to technical and practical considerations. However, adequate dynamic knee joint stability and efficient movement patterns during adolescence appear to be a necessary component for all functional movements and likely helps resist against excessive knee joint loads.71 Functional deficits in neuromuscular control have been associated with increased ACL injury risk in female athletes.40,47,72
Pre-pubertal children do not appear to demonstrate measurable sex differences in lower extremity bio-mechanical and neuromuscular differences are detectable between the sexes.50,69,73 In contrast, after puberty females exhibit measurable quadriceps dominance, ligament dominance, leg dominance (lower extremity asymmetry) and trunk dominance compared to males.51,74–77 Post-pubertal females also have higher coronal plane knee motions, knee abduction angles and moments and decreased active knee joint stiffness compared to mature males. 40,50,70 Males and females demonstrate increases in active stiffness at the knee after puberty. However, males have greater magnitudes of knee, ankle and hip stiffness throughout the adolescent growth spurt compared to females.39
In contrast to females, males experience increases in power, strength and coordination (neuromuscular spurt) coincident with the anthropomorphic and hormonal changes that accompany puberty.35,50,57 A longitudinal study from our laboratory demonstrated that males exhibit increases in neuromuscular measures such as vertical jump height and ability to attenuate landing forces.35 A longitudinal study of 351 athletes found that males exhibit significant increases in normative hip abduction strength as they mature while females do not.57 For females, the absence of a neuromuscular spurt potentially increases knee injury risk due to possible deficiencies in neuromuscular control and the ability to adapt to perturbations to the longer bony levers and greater mass that accompanies the maturation process.35,44,50,70 Fortunately, evidence from our laboratory demonstrates that a neuromuscular spurt can be induced in females with neuromuscular training programs. Neuromuscular and biomechanical ACL injury risk factors such as poor landing mechanics, inadequate force attenuation abilities and inefficient muscle recruitment can be modified and neuromuscular training programs that target improvements in strength, power and coordination appear to reduce the risk of ACL injury.11,47,75,78,79
Biomechanical and Neuromuscular
Biomechanical and neuromuscular ACL injury risk factors have been extensively explored in our laboratory over the past 15 years. In contrast to anatomic risk factors, neuromuscular and biomechanical deficits can be addressed with intervention strategies.60,74,80 Core body control and lower extremity proprioception are modifiable risk factors and are important for attenuating and adapting to perturbations during sports tasks.81 Decreased ability to control trunk displacement after rapid perturbations, is a highly sensitive for predictor of knee, ligament and ACL injury.81 Deficits in the ability to control the body's core during external perturbations predict knee injury with 90% sensitivity and 56% specificity.81 Single-leg postural control deficits following ACL reconstruction place an athlete at risk for a second ACL injury.72
Muscle strength, activation and synergistic coordination are important to overall neuromuscular function, may enhance proprioception and performance and are likely important factors that could be modifiable for ACL injury prevention tactics. 82 Studies performed in our laboratory demonstrate that males and females exhibit different hip and knee joint muscular activation and recruitment strategies. Females who have decreased relative hamstring strength but high relative quadriceps strength may be at greater risk for ACL injury. 83 Females also adopt different hip muscular recruitment strategies than males, which appears to predispose the females to lower extremity postures (e.g., knee abduction motions, angles, and moments) associated with increased risk for ACL injury. 39,47,49,58,84
Large scale biomechanical evaluations in our laboratory have identified knee abduction, hip external rotation and asymmetries between lower extremities as strong predictors for ACL injury. 22,72 We prospectively measured 3-dimensional kinematics of female athletes (N = 205) during a landing task. Compared to their team controls, the athletes that subsequently sustained an ACL injury after screening exhibited eight degrees greater knee abduction angles and 2.5 times greater knee abduction moments during landing. In addition the athletes that went on to subsequent ACL injury had 20% higher ground reaction forces at landing compared to control teammates.22 Coronal plane motions at the hip significantly contribute to increased knee abduction and likely increase ACL injury risk.85 Reduction of coronal plane hip motion via neuromuscular training that targets the hip and trunk may be necessary to decrease high risk knee abduction postures and ultimately reduce ACL injury risk. 85
Previous Injury
Previous ACL injury significantly increases the odds of sustaining another ACL injury.86–88 Healthy athletes reportedly have a 1 in 60 to 1 in 100 chance of sustaining a primary ACL injury. Return to high activity levels after ACL injury can lead to a 15–25 times greater chance of subsequent re-injury or contralateral ACL injury.89–91 A recent study in our laboratory found that females are four times more likely to suffer a second ACL injury and six times more likely to suffer a contralateral ACL injury than males.91 A systematic review of the literature indicates that female patients who have had ACL reconstruction with a hamstring autograft exhibit greater anterior-posterior knee laxity measures compared to males with hamstring autograft reconstruction.92 Deficits in postural control and knee and hip neuromuscular function strongly predict second ACL injury risk after return to sport from ACL reconstruction.93
ACL reconstructed patients often demonstrate asymmetric loading of the lower extremities during sports tasks.94 Specifically, ACL reconstructed patients cleared to return back to sports frequently exhibit patterns of favoring their uninjured contralateral limb and this deficit may persist even after 2 years post-operatively.72,93,94 This asymmetric loading of the contralateral limb may place athletes at further risk for second ACL injury as limb loading asymmetry has been identified as a potential ACL injury risk factor.51 Identification of asymmetry is an important component for safe reintegration of patients back to sports activities. However, bipedal tasks may not be sensitive enough to identify asymmetries in lower extremity loading. Instead, incorporation of single limb tests such as single leg hopping may be important to identify limb asymmetries in strength, landing and movement patterns.95 In addition, after ACL reconstruction, evaluation of ACL integrity of contralateral limbs and alterations of laxity in reconstructed limbs can be difficult. Our laboratory demonstrated that curve shapes from knee arthrometry can serve as a simple and accurate diagnostic tool for individuals without a healthy contralateral limb.96 Persistent lower extremity asymmetries during functional activities may further increase and ACL reconstructed athlete's chance for sustaining a second ACL injury (contralateral or ipsilateral). Rehabilitation programs that target reduction in functional asymmetries prior to the return to sports after ACL reconstruction may be necessary to more safely reintegrate these patients back to sports.
Genetics
It is speculated that genetics may play a role in the risk for ACL injury. Genetics influence laxity as demonstrated by inheritable collagen disorders such as Ehlers Danlos and Marfan's Syndrome. Although limited information is currently available in the literature about the genetic factors that may increase ACL injury risk, it is probable that ACL injury risk factors may be partially influenced by genetics.97–99 We tested fraternal twin sisters prior to their sports seasons and both went on to subsequent ACL injuries. Both sisters demonstrated multiple potential ACL injury risk factors including increased knee abduction angles, decreased knee flexion angles, increased generalized joint laxity, decreased hamstrings/quadriceps torque ratios and smaller femoral condylar notch widths.100 The genetic traits that may predispose athletes to ACL injury are not clear at this time. However, a pleiotropic genetic predisposition is likely and identification of such genetic traits may potentially help clinicians identify at risk athletes and target specific risk factors within family members to minimize ACL injury risk.
Mechanisms of ACL Injury
The knee joint potentially translates and rotates within all three planes (sagittal, frontal and transverse). The majority of motion occurs in the sagittal plane (knee flexion/extension) and motion beyond the normal physiologic ranges in any plane may result in ligamentous injury. A systematic review by our laboratory demonstrated that ACL injuries are more likely to occur during multi-planar rather than uni-planar mechanisms. Evaluation of videos of ACL injury events provide evidence that during the injury athletes have increased lateral trunk motion, greater knee abduction motions, flatfoot position at initial ground contact and increased hip flexion compared to non-injury conditions.38,101,102 Males and females also demonstrate differences in mechanisms of injury. 34,37,38,102 Females often demonstrate the same knee valgus collapse ACL injury mechanism as males, but they often had significantly higher knee and hip flexion during injury compared to males.38
Although many techniques exist to study ACL injury mechanisms such as athlete interviews, arthroscopic studies, video analyses, cadaveric studies, in vivo laboratory studies and mathematical modeling, the inherent limitations of each technique makes it challenging to make clearly define ACL injury mechanisms.102 In order to address this problem, our laboratory has developed a new research paradigm (in sim) that integrates in vivo, in vitro (cadaveric), and in silico (computer modeling methods).103 The goal of the in sim approach is to provide a more comprehensive understanding of the complex joint biomechanics that lead to ACL injury. Our laboratories have utilized the in sim approach to evaluate ACL injury mechanisms and tibio-femoral cartilage pressure distributions with comparisons to in vivo bone bruise patterns (occurs in over 80% of patients with acute ACL injury).104,105 Landing data from young female athletes that went on to subsequent ACL injury was used as input into a validated finite element model and normal landing and injury conditions were simulated in silico. In vivo video data of female athletes during an ACL injury event was used to provide input for simulated ACL injury conditions.38,52 The results supported a valgus collapse mechanism with potential multi-planar loads of tibial abduction combined with anterior tibial translation or external or internal tibial rotations.104 Many ACL injury mechanism studies demonstrate lower extremity biomechanical loading patterns that may be avoided with neuromuscular training programs. Modification of landing techniques and education of dangerous knee postures may be important injury prevention strategies in the future.
Prediction of Risk
Over the past two decades we have prescreened biomechanical, anatomical and neuromuscular measures on over 3,000 athletes prior to their athletic seasons and tracked them to determine who sustained subsequent ACL injury.10,46,74,77,78 Our biomechanical epidemiologic studies indicate that high knee abduction moments and knee abduction angles and ground reaction forces during a jump landing task are important predictors for ACL injury risk (78% sensitivity and 73% specificity).22 Athletes that went on to subsequent ACL injury also demonstrated a 16% shorter stance time and high ground reaction forces at landing compared to uninjured teammates.22 Side-to-side differences in anterior-posterior knee displacement (1.3mm or greater) and positive knee hyperextension increased the odds of ACL injury, fourfold and fivefold, respectively.59 Decreased hamstring strength but similar quadriceps strength to males was often exhibited by females that went on to subsequent ACL injury. In contrast, females that did not suffer an ACL injury demonstrated decreased quadriceps strength relative to males.83
Deficits in the ability to control the body's core appears to be important predictor for knee injuries in female athletes.81 Deficits in core stability predicted knee injury with 90% sensitivity and 56% specificity in females, while no similar associations were apparent in male athletes.81 Athletes that exhibited large lateral trunk excursions after sudden perturbation often went on to sustain knee injuries. Trunk displacement, proprioception and history of low back pain was highly predictive of ACL injury risk in females (91% accuracy) and ligamentous injury of the knee (91% sensitivity and 68% specificity).81
Athletes that have sustained a previous ACL injury are at high risk of second ACL injury if they return to sport.72 In a cohort of athletes that returned to sport after ACL reconstruction, net hip torque impulse, frontal knee plane range of motion during landing, asymmetries in sagittal plane knee moments during landing and deficits and postural stability predicted second ACL injury risk with 92% sensitivity and 88% specificity.93 Identification of the specific deficits that can be addressed during the rehabilitation stage may be a critical step in reduction of up to a 25% chance of second ACL injury in young athletes that return to sport.
Clinical Assessment Tools to Identify At-Risk Athletes
Development of clinical assessment tools to identify athletes at risk for ACL injury would aid clinicians to target the populations that will benefit most from intervention. Although we have identified important predictors of ACL injury that are potentially modifiable like measures of high knee abduction moment during landing tasks, these measurements utilized expensive measurement tools (e.g., motion analysis systems, force plates) and labor-intensive data collection and reduction techniques to identify important biomechanical risk factors.22 Our research has helped us develop inexpensive; less labor intensive assessment tools that can be performed relatively quickly and easily in the clinical setting and have been shown to identify high knee abduction moments with 73% sensitivity and 70% specificity.77,106–110 Clinical correlates to laboratory-based measures identify, stratify and can used to target subjects at increased risk for highly effective interventions.109 Identification of athletes with high knee abduction moments is possible with less expensive equipment and time because measures that can be performed without a motion analysis system of knee abduction motion, knee flexion range of motion, body mass, tibial length and quadriceps to hamstring ratio account for nearly 80% of the measured variance in knee abduction moment during landing.107 These clinical prediction tools show moderate to high inter-rater reliability (intra-class correlation co-efficiencies 0.60–0.97) and we have continued to simplify and optimize the screening tools to include a calibrated physician's scale, a standard measuring tape, standard camcorder, ImageJ software, and an isokinetic dynamometer. These optimized measures predict high knee abduction moments status with 84% sensitivity and 67% specificity.108,111 A clinician-friendly nomogram tool demonstrates over 75% prediction accuracy for identification of high knee abduction moments in individual athletes.108,111 Creation of clinician-friendly, inexpensive techniques to identify and subsequently enroll athletes into appropriate injury prevention programs may help reduce ACL injuries in athletes.
Prevention Techniques
Overview of Prevention Techniques
Identification of risk factors and mechanisms of injury that are modifiable through neuromuscular based injury prevention programs would allow many athletes to continue sports participation and reduce risk for ACL injury.112 Detection and treatment of quantifiable neuromuscular control deficits and functional movements that significantly increase risk for ACL injury has been a high priority in our laboratory because these are likely the most modifiable risk factors.11,21,60,74–76,78,80,84,94,106,110–120
We define deficits in muscle strength, power, coordination or activation patterns that potentially increase injury risk due to increased joint loads as neuromuscular control deficits.115 Females often demonstrate neuromuscular control deficits that likely play a role in ACL injury risk.115 One neuromuscular deficit, which is operationally termed “ligament dominance,” can be defined as an imbalance between the neuromuscular and ligamentous control of dynamic knee joint stability.121 This control imbalance is demonstrated by an inability to control lower extremity frontal plane motion during landing and cutting. A second modifiable neuromuscular control deficit often observed in female athletes, which is termed “quadriceps dominance,” can be defined as an imbalance between knee extensor and flexor strength, recruitment and coordination.121 A third neuromuscular control deficit, often observed in female athletes is “leg dominance,” which can be defined as an imbalance between the two lower extremities in strength, coordination and control.121 The fourth neuromuscular control deficit, often observed in female athletes is “trunk dominance” or “‘core’ dysfunction,” which can be defined as an imbalance between the inertial demands of the trunk and control and coordination to resist it. Deficits in control of the body's core during sports tasks make it difficult to dissipate external perturbations and lead to excessive frontal plane trunk displacements, high ground reaction forces and large knee abduction loads.77,122
The adolescent phase is a critical stage for neuromuscular control development during which children may overcome certain deficits or develop new ones. If not addressed, neuromuscular deficits may continue into adulthood and increase an athlete's risk for ACL injury.22,35,39,40,50 There is clear evidence that neuromuscular training programs can enhance athletic performance through increased strength, power and coordination as well as address neuromuscular deficits.75,78,114 We have demonstrated that it is possible to induce a neuromuscular spurt and improve neuromuscular deficits in females with training. 112,114 Neuromuscular training potentially reduces ACL injury risk by approximately 50% and enhances athletic performance measures in females.11,112,114
Studies of Prevention Techniques
Integrated neuromuscular training programs (biomechanical, neuromuscular control, and strength training techniques) have effectively improved performance and decreased risk for ACL injury. 11,112,114,117 Current neuromuscular training programs necessitate integrated, somewhat comprehensive protocols with a combination of power, strength and coordination training since single neuromuscular component interventions have failed to significantly impact knee injury rates in females.123,124 Compliance to training programs is crucial for prevention techniques to successfully work. Unfortunately, comprehensive ACL injury prevention programs often require extensive commitments in time and involvement for players and coaches, which has impeded widespread acceptance and utilization by athletes and teams to implement the training necessary to reduce ACL injury risk. In order to address this challenge, our laboratory has focused on creating more efficient and effective training protocols to address neuromuscular deficits and high risk landing biomechanics.125,126 We have conducted comparative studies of plyometric training versus dynamic stabilization as well as evaluated the effects of targeted training of the trunk, hip and knee on power, strength, coordination, limb asymmetries, ground reaction forces at landing, and knee abduction measures.78,79,112–114,117,127
Plyometric and balance training both appear to reduce high-risk knee abduction and flexion measures.112,114,117 Targeted core muscular (trunk) training can increase hip abduction strength and potentially improve neuromuscular control of lower limb alignment during sports activities.113 Studies from our lab show that targeted core training and improvements in lower extremity strength can improve single-limb postural stability and neuromuscular control.79,127
The optimal length of training necessary to reduce ACL injury risk and whether it can be incorporated with in season sports training remains unclear. Females that demonstrate high knee abduction measures appear to be more responsive to neuromuscular training than athletes with lower knee abduction measures. However, despite 4–7 weeks of training, their reduced knee abduction measures were not reduced to levels consistent with their control teammates.114 There is some evidence that isolated preseason or in-season training in short doses may not provide the training dosage necessary to reduce ACL injury risk in females.114,128 Collectively, our research indicates that comprehensive protocols that incorporate plyometric, strength and balance exercises may provide the most effective ACL injury prevention strategies.
Timing of Intervention
Preadolescence or early puberty seems to be a critical phase related to the increased ACL injury risk in female athletes. After the onset of puberty, the sexes demonstrate differences in laxity and neuromuscular control in addition to a divergence in ACL injury rates.35,36,39,40,45 With the increased obesity problem in children, there has been a greater promotion of physical activity and interest in strength and conditioning programs. However, there is concern about the optimal age to safely incorporate strength training programs.129–131 In the past, high school female athlete participation in weightlifting activities was significantly less than males with access, desire or available resources likely limiting the incorporation of strength training measures into their sports programs.132
Integrative neuromuscular training can lead to significant improvements in health and motor skill performance fitness components in children and can be successfully integrated into physical education activities.133 Given the evidence that neuromuscular training programs that incorporate strength training may help reduce ACL injury risk, introduction and participation in such programs even at an early age may be important for preventing ACL injuries. Resistance training can be safely effectively implemented provided that the training is supervised by qualified professionals and age appropriate techniques and safety guidelines are followed.107,111,129,134
Preliminary data indicate integrative neuromuscular training protocols implemented in pre-adolescent (Tanner [1] and early adolescent (Tanner [2] stages may artificially induce the “neuromuscular spurt”).78 Induction of a neuromuscular spurt, particularly in females has the potential to reduce the risk of sports-related injury.11,75,135,136 The optimal time to provide injury prevention is not fully delineated. However, introduction of integrative neuromuscular training at any age and maintained throughout childhood into adulthood promotes positive health outcomes, has the potential to enhance sports performance and reduce the risk of sports-related and more specifically, ACL injury in young athletes.78,107,111,137
Assess The Effectiveness Of Intervention
The development of clinical assessment tools that reliably and accurately assess high risk neuromuscular deficits are important to provide clinicians with objective, inexpensive feedback about the effectiveness of neuromuscular training programs.77 Common assessment tools such as the star excursion balance test, functional hop tests, strength measures, balance and stability measures and dynamometry, in addition to development of new techniques to help identify lower extremity asymmetry and high risk landing and cutting techniques are paramount to evaluating our effectiveness of neuromuscular training.79,106,109,110,127,128,134 Development of real-time assessment tools provides clinicians with the ability to offer immediate biofeed-back and targeted directions for neuromuscular training programs.111 These assessment tools as well as standard performance tests (e.g., power cleans, bench press, leg press) have been used to identify biomechanical and neuromuscular risk factors for ACL injury and provide measures of athletic performance.128 Assessments of the reliability of the assessment tools and performance measures have helped evaluate and optimize intervention strategies.138 In order to provide immediate, objective feedback that can be systematically tracked and used to evaluate intervention effectiveness, we have developed a tuck jump assessment tool that measures limb symmetry, foot positioning, knee abduction, technique degradation, coordination and landing forces during a high-level effort movement.106,128 In addition, we have developed techniques to assess frontal and sagittal plane biomechanics using inexpensive tools that can be used for individual assessments as well as large-scale screening techniques similar to what occurs during NFL combine testing.94,109,110,134,139
Clinical assessment tools such as the tuck jump assessment and nomogram that predicts high knee abduction measures may also help rehabilitation specialists working with athletes to monitor functional deficits and determine level of readiness to meet the functional demands of sports with minimal risk of reinjury. History of previous ACL injury is one of the highest predictive risk factors for future ACL injury risk and of the athletes that return to sport after ACL reconstruction nearly 25% may experience a second ACL injury.72 It is paramount that we identify clinical assessment tools that help improve functional deficits during the rehabilitation phases after ACL reconstruction and evaluate functional readiness to return to sport safely. Future work in our laboratory will focus on development of new clinical assessment tools of function and evaluation of the effectiveness and predictive ability of these tools on ACL injury risk.
Summary and Conclusions
There is strong, nearly unequivocal evidence that neuromuscular training reduces biomechanical risk factors for ACL injury and decreases ACL injury incidence in athletes. Assessment of relative injury risk using widespread neuromuscular screening techniques should be further employed. Development of more specific injury prevention protocols that are designed to decrease risk in high risk athletes and more precise determination of the most efficacious timing of intervention is important. Pre- or early adolescent athletes may have the greatest potential for both the development of optimal biomechanical movements and decreased injury risk during sports participation. Neuromuscular training is currently the only effective tool for lowering the incidence rate of ACL injuries which, in turn, has a direct link to reduction in the rate of post traumatic osteoarthritis associated with severe joint trauma associated with participation in sport and activity. This post traumatic osteoarthritis occurs with or without surgical reconstruction. We have made significant strides toward these goals, but we must ontinue until strong epidemiological evidence shows that ACL injury risk is unequivocally decreased in young athletes.
The findings of the authors' studies outlined above were the first to identify the mechanisms that underlie increased risk of ACL injury in high risk athletes, especially in female athletes, to develop validated ACL injury risk screening approaches and to direct athletes into neuromuscular training designed for and targeted to those specific injury mechanisms. Athletes who are in the higher percentiles for specific risk factors can be identified for neuromuscular training prior to participation. Education and public awareness of the high occurrence and mechanisms of ACL injury has been shown to decrease injuries in skiers by greater than 50%.140 Critical analysis and verbal, visual, or bio-feedback regarding technique may decrease reaction forces and lead to a reduction of ACL injuries.141 Questions remain to be answered, including: (i) when interventions should be instituted and (ii) whether a “neuromuscular spurt” to increase lower extremity neuromuscular control can be induced with training at the proper age.
In conclusion, the summarized findings have led to advances in the understanding of the mechanisms and prevention of ACL injuries in female athletes, who are at a 2- to 10-fold increased risk of ACL injury than males. Finally, our objectives were to determine the mechanisms by which athletes become more susceptible to ACL injury, to develop screening tools to quantify risk levels and to optimize the effectiveness of interventions designed to prevent ACL injuries. Prophylactic interventions to reduce the risk of suffering ACL injury could prevent a significant percentage of the 100,000–250,000 injuries that occur each year in the United States and likely greater than 350,000 worldwide.11,18 The President's council on physical fitness recommends that women, both young and old, remain active to maintain optimal health.142 Reduction of female injury rates from five times to equal males' would potentially allow females annually to continue the health benefits of sports participation and avoid the long-term complications of osteoarthritis, which occurs with a 10–100-fold greater incidence in ACL-injured than in uninjured athletes.5,7
Acknowledgments
This comprehensive body of research was the result of a large team of individuals that have helped contribute to the data collection. We would like to thank all co-authors and colleagues at both the mayo Clinic Biomechanics Laboratories and the Ohio State and Cincinnati Children's Sports Medicine Biodynamics Labs for their help with the solutions to this important and devastating ACL injury dilemma. The authors' would also like to reiterate an acknowledgement to the many research groups who have contributed to the current state of knowledge in the fields of ACL injury mechanisms, ACL injury risk screening and ACL injury prevention strategies.
This article is a 2016 OREF Clinical Research Award recipient. Grant sponsor: National Institutes of Health/NIAMS; Grant numbers: R01-AR049735, R01-AR056259, R01-AR055563, R03-AR057551, R21-AR065068-01A1, U01-AR067997; Grant sponsor: Orthopaedic Research and Education Foundation (OREF); Grant sponsor: Orthopaedic Research Society (the 2016 OREF Clinical Research Award); Grant sponsor: National Football League Charities; Grant sponsor: American College of Sports Medicine Foundation Plus One Active Research Grant; Grant sponsor: Ohio State University Sports Health and Performance Institute; Grant sponsor: Cincinnati Children's Hospital Research Foundation.
Footnotes
Authors' Contributions: All authors contributed to the study design, data collection, data analysis, and reporting for this manuscript. All authors have read and approved the final submitted manuscript.
References
- 1.Freedman KB, Glasgow MT, Glasgow SG, et al. Anterior cruciate ligament injury and reconstruction among university students. Clin Orthop Related Res. 1998;356:208–212. doi: 10.1097/00003086-199811000-00028. [DOI] [PubMed] [Google Scholar]
- 2.Hewett TE, Ford KR, Xu YY, et al. Utilization of ACL injury biomechanical and neuromuscular risk profile analysis to determine the effectiveness of neuromuscular training. Am J Sports Med. 2016 doi: 10.1177/0363546516656373. doi:10.1177. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ruiz AL, Kelly M, Nutton RW. Arthroscopic ACL reconstruction: a 5–9 year follow-up. Knee. 2002;9:197–200. doi: 10.1016/s0968-0160(02)00019-4. [DOI] [PubMed] [Google Scholar]
- 4.Lohmander LS, Englund PM, Dahl LL, et al. The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. Am J Sports Med. 2007;35:1756–1769. doi: 10.1177/0363546507307396. [DOI] [PubMed] [Google Scholar]
- 5.Myklebust G, Bahr R. Return to play guidelines after anterior cruciate ligament surgery. Br J Sports Med. 2005;39:127–131. doi: 10.1136/bjsm.2004.010900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gillquist J, Messner K. Anterior cruciate ligament reconstruction and the long-term incidence of gonarthrosis. Sports Med. 1999;27:143–156. doi: 10.2165/00007256-199927030-00001. [DOI] [PubMed] [Google Scholar]
- 7.Lohmander LS, Ostenberg A, Englund M, et al. High prevalence of knee osteoarthritis, pain, and functional limitations in female soccer players twelve years after anterior cruciate ligament injury. Arthritis Rheum. 2004;50:3145–3152. doi: 10.1002/art.20589. [DOI] [PubMed] [Google Scholar]
- 8.Gray J, Taunton JE, McKenzie DC, et al. A survey of injuries to the anterior cruciate ligament of the knee in female basketball players. Int J Sports Med. 1985;6:314–316. doi: 10.1055/s-2008-1025861. [DOI] [PubMed] [Google Scholar]
- 9.Miyasaka KC, Daniel DM, Stone ML. The incidence of knee ligament injuries in the general popluation. Am J Knee Surg. 1991;43:43–48. [Google Scholar]
- 10.Kim S, Bosque J, Meehan JP, et al. Increase in outpatient knee arthroscopy in the united states: a comparison of national surveys of ambulatory surgery, 1996 and 2006. J Bone Joint Surg Am. 2011;93:994–1000. doi: 10.2106/JBJS.I.01618. [DOI] [PubMed] [Google Scholar]
- 11.Hewett TE, Lindenfeld TN, Riccobene JV, et al. The effect of neuromuscular training on the incidence of knee injury in female athletes. A prospective study. Am J Sports Med. 1999;27:699–706. doi: 10.1177/03635465990270060301. [DOI] [PubMed] [Google Scholar]
- 12.Zelisko JA, Noble HB, Porter M. A comparison of men's and women's professional basketball injuries. Am J Sport Med. 1982;10:297–299. doi: 10.1177/036354658201000507. [DOI] [PubMed] [Google Scholar]
- 13.Chandy TA, Grana WA. Secondary school athletic injury in boys and girls: a three-year comparison. Phys Sports Med. 1985;13:106–111. [Google Scholar]
- 14.Malone TR, Hardaker WT, Garrett WE, et al. Relationship of gender to anterior cruciate ligament injuries in intercollegiate basketball players. J Southern Orthop Assoc. 1993;2:36–39. [Google Scholar]
- 15.Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer. NCAA data and review of literature. Am J Sports Med. 1995;23:694–701. doi: 10.1177/036354659502300611. [DOI] [PubMed] [Google Scholar]
- 16.NCAA. NCAA injury surveillance system summary. Indianapolis: National Collegiate Athletic Association; 2002. [Google Scholar]
- 17.Deitch JR, Starkey C, Walters SL, et al. Injury risk in professional basketball players: a comparison of Women's National Basketball Association and National Basketball Association Athletes. Am J Sports Med. 2006;34:1077–1083. doi: 10.1177/0363546505285383. [DOI] [PubMed] [Google Scholar]
- 18.Toth AP, Cordasco FA. Anterior cruciate ligament injuries in the female athlete. J Gend Specif Med. 2001;4:25–34. [PubMed] [Google Scholar]
- 19.Myer GD, Ford KR, Hewett TE. Rationale and clinical techniques for anterior cruciate ligament injury prevention among female athletes. J Athl Train. 2004;39:352–364. [PMC free article] [PubMed] [Google Scholar]
- 20.Bendjaballah MZ, Shirazi-Adl A, Zukor DJ. Finite element analysis of human knee joint in varus-valgus. Clin Biomech (Bristol, Avon) 1997;12:139–148. doi: 10.1016/s0268-0033(97)00072-7. [DOI] [PubMed] [Google Scholar]
- 21.Hewett TE, Myer GD, Ford KR. Reducing knee and anterior cruciate ligament injuries among female athletes: a systematic review of neuromuscular training interventions. J Knee Surg. 2005;18:82–88. doi: 10.1055/s-0030-1248163. [DOI] [PubMed] [Google Scholar]
- 22.Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33:492–501. doi: 10.1177/0363546504269591. [DOI] [PubMed] [Google Scholar]
- 23.Markolf KL, Burchfield DM, Shapiro MM, et al. Combined knee loading states that generate high anterior cruciate ligament forces. J Orthop Res. 1995;13:930–935. doi: 10.1002/jor.1100130618. [DOI] [PubMed] [Google Scholar]
- 24.von Porat A, Roos EM, Roos H. High prevalence of osteoarthritis 14 years after an anterior cruciate ligament tear in male soccer players: a study of radiographic and patient relevant outcomes. Ann Rheum Dis. 2004;63:269–273. doi: 10.1136/ard.2003.008136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Zazulak BT, Hewett TE, Reeves NP, et al. Factors related to core stability predict knee ligament injury risk. Am J Sport Med. 2007;35:1123–1130. doi: 10.1177/0363546507301585. [DOI] [PubMed] [Google Scholar]
- 26.Krosshaug T, Nakamae A, Boden BP, et al. Mechanisms of anterior cruciate ligament injury in basketball: video analysis of 39 cases. Am J Sports Med. 2006;35:359–367. doi: 10.1177/0363546506293899. [DOI] [PubMed] [Google Scholar]
- 27.Olsen OE, Myklebust G, Engebretsen L, et al. Injury mechanisms for anterior cruciate ligament injuries in team handball: a systematic video analysis. Am J Sports Med. 2004;32:1002–1012. doi: 10.1177/0363546503261724. [DOI] [PubMed] [Google Scholar]
- 28.Griffin LY. The henning program. In: Griffin LY, editor. Prevention of noncontact ACL injuries. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2001. pp. 93–96. [Google Scholar]
- 29.Ireland ML. The female ACL: why is it more prone to injury? Orthop Clin North Am. 2002;33:637–651. doi: 10.1016/s0030-5898(02)00028-7. [DOI] [PubMed] [Google Scholar]
- 30.van Mechelen W, Hlobil H, Kemper HC. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med. 1992;14:82–99. doi: 10.2165/00007256-199214020-00002. [DOI] [PubMed] [Google Scholar]
- 31.Malone TR, Hardaker WT, Garrett WE, et al. Relationship of gender to anterior cruciate ligament injuries in intercollegiate basketball players. J South Orthop Assoc. 1993;2:36–39. [Google Scholar]
- 32.Andrish JT. Anterior cruciate ligament injuries in the skeletally immature patient. Am J Orthop. 2001;30:103–110. [PubMed] [Google Scholar]
- 33.Gallagher SS, Finison K, Guyer B, et al. The incidence of injuries among 87,000 massachusetts children and adolescents: results of the 1980–81 statewide childhood injury prevention program surveillance system. Am J Public Health. 1984;74:1340–1347. doi: 10.2105/ajph.74.12.1340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hewett TE, Myer GD, Ford KR. Anterior cruciate ligament injuries in female athletes: part 1, mechanisms and risk factors. Am J Sports Med. 2006;34:299–311. doi: 10.1177/0363546505284183. [DOI] [PubMed] [Google Scholar]
- 35.Quatman CE, Ford KR, Myer GD, et al. Maturation leads to gender differences in landing force and vertical jump performance: a longitudinal study. Am J Sports Med. 2006;34:806–813. doi: 10.1177/0363546505281916. [DOI] [PubMed] [Google Scholar]
- 36.Quatman-Yates CC, Quatman CE, Meszaros AJ, et al. A systematic review of sensorimotor function during adolescence: a developmental stage of increased motor awkwardness? Br J Sports Med. 2011;46:649–655. doi: 10.1136/bjsm.2010.079616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Quatman CE, Hewett TE. The anterior cruciate ligament injury controversy: is “valgus collapse” a sex-specific mechanism? Br J Sports Med. 2009;43:328–335. doi: 10.1136/bjsm.2009.059139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Krosshaug T, Nakamae A, Boden BP, et al. Mechanisms of anterior cruciate ligament injury in basketball: video analysis of 39 cases. Am J Sports Med. 2007;35:359–367. doi: 10.1177/0363546506293899. [DOI] [PubMed] [Google Scholar]
- 39.Ford KR, Myer GD, Hewett TE. Longitudinal effects of maturation on lower extremity joint stiffness in adolescent athletes. Am J Sports Med. 2010;38:1829–1837. doi: 10.1177/0363546510367425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ford KR, Shapiro R, Myer GD, et al. Longitudinal sex differences during landing in knee abduction in young athletes. Med Sci Sports Exerc. 2010;42:1923–1931. doi: 10.1249/MSS.0b013e3181dc99b1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Harrison AD, Ford KR, Myer GD, et al. Sex differences in force attenuation: a clinical assessment of single-leg hop performance on a portable force plate. Br J Sports Med. 2011;45:198–202. doi: 10.1136/bjsm.2009.061788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Hewett TE, Myer GD, Zazulak BT. Hamstring to quadriceps peak torque ratios diverge with increasing isokinetic angular velocity in females and males. J Sci Med Sport. 2006;11:452–459. doi: 10.1016/j.jsams.2007.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Chaudhari AM, Lindenfeld TN, Andriacchi TP, et al. Knee and hip loading patterns At different periods In the menstrual cycle and their implications for the ACL injury disparity between women & men. Am J Sports Med. 2007;35:793–800. doi: 10.1177/0363546506297537. [DOI] [PubMed] [Google Scholar]
- 44.Hewett TE, Myer GD, Ford KR, et al. Preparticipation physical exam using a box drop vertical jump test in young athletes: the effects of puberty and sex. Clin J Sport Med. 2006;16:298–304. doi: 10.1097/00042752-200607000-00003. [DOI] [PubMed] [Google Scholar]
- 45.Quatman CE, Ford KR, Myer GD, et al. The effects of gender and pubertal status on generalized joint laxity in young athletes. J Sci Med Sport. 2008;11:257–263. doi: 10.1016/j.jsams.2007.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Ford KR, Myer GD, Smith RL, et al. A comparison of dynamic coronal plane excursion between matched male and female athletes when performing single leg landings. Clin Biomech. 2006;21:33–40. doi: 10.1016/j.clinbiomech.2005.08.010. [DOI] [PubMed] [Google Scholar]
- 47.Zazulak BT, Ponce PL, Straub SJ, et al. Gender comparison of hip muscle activity during single-leg landing. J Orthop Sports Phys Ther. 2005;35:292–299. doi: 10.2519/jospt.2005.35.5.292. [DOI] [PubMed] [Google Scholar]
- 48.Myer GD, Ford KR, Hewett TE. The effects of gender on quadriceps muscle activation strategies during a maneuver that mimics a high ACL injury risk position. J Electromyogr Kinesiol. 2005;15:181–189. doi: 10.1016/j.jelekin.2004.08.006. [DOI] [PubMed] [Google Scholar]
- 49.Ford KR, Myer GD, Toms HE, et al. Gender differences in the kinematics of unanticipated cutting in young athletes. Med Sci Sports Exerc. 2005;37:124–129. [PubMed] [Google Scholar]
- 50.Hewett TE, Myer GD, Ford KR. Decrease in neuromuscular control about the knee with maturation in female athletes. J Bone Joint Surg Am. 2004;86-A:1601–1608. doi: 10.2106/00004623-200408000-00001. [DOI] [PubMed] [Google Scholar]
- 51.Ford KR, Myer GD, Hewett TE. Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exerc. 2003;35:1745–1750. doi: 10.1249/01.MSS.0000089346.85744.D9. [DOI] [PubMed] [Google Scholar]
- 52.Koga H, Nakamae A, Shima Y, et al. Mechanisms for noncontact anterior cruciate ligament injuries: knee joint kinematics in 10 injury situations from female team handball and basketball. Am J Sports Med. 2010;38:2218–2225. doi: 10.1177/0363546510373570. [DOI] [PubMed] [Google Scholar]
- 53.Ford KR, Myer GD, Schmitt LC, et al. Preferential quadriceps activation in female athletes with incremental increases in landing intensity. J Appl Biomech. 2011;27:215–222. doi: 10.1123/jab.27.3.215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Shultz SJ, Shimokochi Y, Nguyen AD, et al. Measurement of varus-valgus and internal-external rotational knee laxities in vivo? Part II: relationship with anterior-posterior and general joint laxity in males and females. J Orthopaedic Res. 2007;25:989–996. doi: 10.1002/jor.20398. [DOI] [PubMed] [Google Scholar]
- 55.Hsu WH, Fisk JA, Yamamoto Y, et al. Differences in torsional joint stiffness of the knee between genders: a human cadaveric study. Am J Sports Med. 2006;34:765–770. doi: 10.1177/0363546505282623. [DOI] [PubMed] [Google Scholar]
- 56.Ahmad CS, Clark AM, Heilmann N, et al. Effect of gender and maturity on quadriceps-to-hamstring strength ratio and anterior cruciate ligament laxity. Am J Sports Med. 2006;34:370–374. doi: 10.1177/0363546505280426. [DOI] [PubMed] [Google Scholar]
- 57.Brent J, Myer GD, Ford KR, et al. The effect of sex and age on isokinetic hip abduction torques. J Sport Rehabil. 2012;22:41–46. doi: 10.1123/jsr.22.1.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Mendiguchia J, Ford KR, Quatman CE, et al. Sex differences in proximal control of the knee joint. Sports Med. 2011;41:541–557. doi: 10.2165/11589140-000000000-00000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Myer GD, Ford KR, Paterno MV, et al. The effects of generalized joint laxity on risk of anterior cruciate ligament injury in young female athletes. Am J Sports Med. 2008;36:1073–1080. doi: 10.1177/0363546507313572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Hewett TE. Neuromuscular and hormonal factors associated with knee injuries in female athletes: strategies for intervention. Sports Med. 2000;29:313–327. doi: 10.2165/00007256-200029050-00003. [DOI] [PubMed] [Google Scholar]
- 61.Slauterbeck JR, Hardy DM. Sex hormones and knee ligament injuries in female athletes. Am J Med Sci. 2001;322:196–199. doi: 10.1097/00000441-200110000-00008. [DOI] [PubMed] [Google Scholar]
- 62.Wojtys EM, Ashton-Miller JA, Huston LJ. A gender-related difference in the contribution of the knee musculature to sagittal-plane shear stiffness in subjects with similar knee laxity. J Bone Joint Surg Am. 2002;84-A:10–16. doi: 10.2106/00004623-200201000-00002. [DOI] [PubMed] [Google Scholar]
- 63.Arendt EA, Bershadsky B, Agel J. Periodicity of noncontact anterior cruciate ligament injuries during the menstrual cycle. J Gend Specif Med. 2002;5:19–26. [PubMed] [Google Scholar]
- 64.Wojtys EM, Huston LJ, Lindenfeld TN, et al. Association between the menstrual cycle and anterior cruciate ligament injuries in female athletes. Am J Sport Med. 1998;26:614–619. doi: 10.1177/03635465980260050301. [DOI] [PubMed] [Google Scholar]
- 65.Hewett TE, Zazulak BT, Myer GD. The effects of the menstrual cycle on ACL injury risk: a systematic review. Am J Sports Med. 2006;35:659–668. doi: 10.1177/0363546506295699. [DOI] [PubMed] [Google Scholar]
- 66.Hewett TE, Zazulak BT, Myer GD. Effects of the menstrual cycle on anterior cruciate ligament injury risk: a systematic review. Am J Sports Med. 2007;35:659–668. doi: 10.1177/0363546506295699. [DOI] [PubMed] [Google Scholar]
- 67.Rozzi S, Lephardt S, Gear W, et al. Knee joint laxity characteristics of male and female soccer and basketball players. Am J Sports Med. 1999;27:312–319. doi: 10.1177/03635465990270030801. [DOI] [PubMed] [Google Scholar]
- 68.Foss KD, Ford KR, Myer GD, et al. Generalized joint laxity associated with increased medial foot loading in female athletes. J Athl Train. 2009;44:356–362. doi: 10.4085/1062-6050-44.4.356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Beunen G, Malina RM. Growth and physical performance relative to the timing of the adolescent spurt. Exerc Sport Sci Rev. 1988;16:503–540. [PubMed] [Google Scholar]
- 70.Myer GD, Ford KR, Divine JG, et al. Longitudinal assessment of noncontact anterior cruciate ligament injury risk factors during maturation in a female athlete: a case report. J Athl Train. 2009;44:101–109. doi: 10.4085/1062-6050-44.1.101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Ford KR, van den Bogert J, Myer GD, et al. The effects of age and skill level on knee musculature co-contraction during functional activities: a systematic review. Br J Sports Med. 2008;42:561–566. doi: 10.1136/bjsm.2007.044883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Paterno MV, Schmitt LC, Ford KR, et al. Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med. 2010;38:1968–1978. doi: 10.1177/0363546510376053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Malina RM, Bouchard C. Timing and sequence of changes in growth, maturation, and performance during adolescence. In: Bouchard MA, editor. Growth, maturation, and physical activity. Champaign, Il: Human Kinetics; 1991. pp. 267–272. [Google Scholar]
- 74.Hewett TE, Paterno MV, Myer GD. Strategies for enhancing proprioception and neuromuscular control of the knee. Clin Orthop. 2002;402:76–94. doi: 10.1097/00003086-200209000-00008. [DOI] [PubMed] [Google Scholar]
- 75.Hewett TE, Stroupe AL, Nance TA, et al. Plyometric training in female athletes. Decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24:765–773. doi: 10.1177/036354659602400611. [DOI] [PubMed] [Google Scholar]
- 76.Hewett TE, Ford KR, Hoogenboom BJ, et al. Understanding and preventing ACL injuries: current biomechanical and epidemiologic considerations—update 2010. N Am J Sports Phys Ther. 2010;5:234–251. [PMC free article] [PubMed] [Google Scholar]
- 77.Myer GD, Brent JL, Ford KR, et al. Real-time assessment and neuromuscular training feedback techniques to prevent ACL injury in female athletes. Strength Cond J. 2011;33:21–35. doi: 10.1519/SSC.0b013e318213afa8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Myer GD, Brunner HI, Melson PG, et al. Specialized neuromuscular training to improve neuromuscular function and biomechanics in a patient with quiescent juvenile rheumatoid arthritis. Phys Ther. 2005;85:791–802. [PubMed] [Google Scholar]
- 79.Paterno MV, Myer GD, Ford KR, et al. Neuromuscular training improves single-limb stability in young female athletes. J Orthopaedic Sports Phys Ther. 2004;34:305–316. doi: 10.2519/jospt.2004.34.6.305. [DOI] [PubMed] [Google Scholar]
- 80.Hewett TE, Myer GD, Ford KR. Prevention of anterior cruciate ligament injuries. Curr Women Health Rep. 2001;1:218–224. [PubMed] [Google Scholar]
- 81.Zazulak BT, Hewett TE, Reeves NP, et al. The effects of core proprioception on knee ligament injury: a prospective biomechanical-epidemiological study. San Diego, California: Accepted AOSSM Specialty Day; 2007. [DOI] [PubMed] [Google Scholar]
- 82.Hewett TE, Zazulak BT, Myer GD, et al. A review of electromyographic activation levels, timing differences, and increased anterior cruciate ligament injury incidence in female athletes. Br J Sports Med. 2005;39:347–350. doi: 10.1136/bjsm.2005.018572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Myer GD, Ford KR, Barber Foss KD, et al. The relationship of hamstrings and quadriceps strength to anterior cruciate ligament injury in female athletes. Clin J Sport Med. 2009;19:3–8. doi: 10.1097/JSM.0b013e318190bddb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Myer GD, Chu DA, Brent JL, et al. Trunk and hip control neuromuscular training for the prevention of knee joint injury. Clin Sports Med. 2008;27:425–448. doi: 10.1016/j.csm.2008.02.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Imwalle LE, Myer GD, Ford KR, et al. Relationship between hip and knee kinematics in athletic women during cutting maneuvers: a possible link to noncontact anterior cruciate ligament injury and prevention. J Strength Cond Res. 2009;23:2223–2230. doi: 10.1519/JSC.0b013e3181bc1a02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Pinczewski LA, Lyman J, Salmon LJ, et al. A 10-year comparison of anterior cruciate ligament reconstructions with hamstring tendon and patellar tendon autograft: a controlled, prospective trial. Am J Sports Med. 2007;35:564–574. doi: 10.1177/0363546506296042. [DOI] [PubMed] [Google Scholar]
- 87.Salmon L, Russell V, Musgrove T, et al. Incidence and risk factors for graft rupture and contralateral rupture after anterior cruciate ligament reconstruction. Arthroscopy. 2005;21:948–957. doi: 10.1016/j.arthro.2005.04.110. [DOI] [PubMed] [Google Scholar]
- 88.Wright RW, Dunn WR, Amendola A, et al. Risk of tearing the intact anterior cruciate ligament in the contra-lateral knee and rupturing the anterior cruciate ligament graft during the first 2 years after anterior cruciate ligament reconstruction: a prospective MOON cohort study. Am J Sports Med. 2007;35:1131–1134. doi: 10.1177/0363546507301318. [DOI] [PubMed] [Google Scholar]
- 89.Messina DF, Farney WC, DeLee JC. The incidence of injury in Texas high school basketball. A prospective study among male and female athletes. Am J Sports Med. 1999;27:294–299. doi: 10.1177/03635465990270030401. [DOI] [PubMed] [Google Scholar]
- 90.Gomez E, DeLee JC, Farney WC. Incidence of injury in Texas girls' high school basketball. Am J Sports Med. 1996;24:684–687. doi: 10.1177/036354659602400521. [DOI] [PubMed] [Google Scholar]
- 91.Paterno MV, Rauh MJ, Schmitt LC, et al. Incidence of contralateral and ipsilateral anterior cruciate ligament (ACL) injury after primary ACL reconstruction and return to sport. Clin J Sport Med. 2012;22:116–121. doi: 10.1097/JSM.0b013e318246ef9e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Paterno MV, Weed AM, Hewett TE. A between sex comparison of anterior-posterior knee laxity after anterior cruciate ligament reconstruction with patellar tendon or hamstrings autograft: a systematic review. Sports Med. 2012;42:135–152. doi: 10.2165/11596940-000000000-00000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Paterno MV, Ford KR, Myer GD, et al. Limb asymmetries in landing and jumping 2 years following anterior cruciate ligament reconstruction. Clin J Sport Med. 2007;17:258–262. doi: 10.1097/JSM.0b013e31804c77ea. [DOI] [PubMed] [Google Scholar]
- 94.Paterno MV, Schmitt LC, Ford KR, et al. 2011. effects of sex on compensatory landing strategies upon return to sport after anterior cruciate ligament reconstruction. J Orthop Sports Phys The. 2011;41:553–559. doi: 10.2519/jospt.2011.3591. [DOI] [PubMed] [Google Scholar]
- 95.Myer GD, Schmitt LC, Brent JL, et al. Utilization of modified NFL combine testing to identify functional deficits in athletes following ACL reconstruction. J Orthop Sports Phys Ther. 2011;41:377–387. doi: 10.2519/jospt.2011.3547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Wordeman SC, Paterno MV, Quatman CE, et al. Arthrometric curve-shape variables to assess anterior cruciate ligament deficiency. Clin Biomech. 2012;27:830–836. doi: 10.1016/j.clinbiomech.2012.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Posthumus M, September AV, O'Cuinneagain D, et al. The COL5A1 gene is associated with increased risk of anterior cruciate ligament ruptures in female participants. Am J Sports Med. 2009;37:2234–2240. doi: 10.1177/0363546509338266. [DOI] [PubMed] [Google Scholar]
- 98.Posthumus M, September AV, O'Cuinneagain D, et al. The association between the COL12A1 gene and anterior cruciate ligament ruptures. Br J Sports Med. 2010;44:1160–1165. doi: 10.1136/bjsm.2009.060756. [DOI] [PubMed] [Google Scholar]
- 99.Flynn RK, Pedersen CL, Birmingham TB, et al. The familial predisposition toward tearing the anterior cruciate ligament: a case control study. Am J Sports Med. 2005;33:23–28. doi: 10.1177/0363546504265678. [DOI] [PubMed] [Google Scholar]
- 100.Hewett TE, Lynch TR, Myer GD, et al. Multiple risk factors related to familial predisposition to anterior cruciate ligament injury: fraternal twin sisters with anterior cruciate ligament ruptures. Br J Sports Med. 2010;44:848–855. doi: 10.1136/bjsm.2008.055798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Boden BP, Torg JS, Knowles SB, et al. Video analysis of anterior cruciate ligament injury: abnormalities in hip and ankle kinematics. Am J Sports Med. 2009;37:252–259. doi: 10.1177/0363546508328107. [DOI] [PubMed] [Google Scholar]
- 102.Quatman CE, Quatman-Yates CC, Hewett TE. A ‘plane’ explanation of anterior cruciate ligament injury mechanisms: a systematic review. Sports Med. 2010;40:729–746. doi: 10.2165/11534950-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 103.Quatman CE, Quatman CC, Hewett TE. Prediction and prevention of musculoskeletal injury: a paradigm shift in methodology. Br J Sports Med. 2009;43:1100–1107. doi: 10.1136/bjsm.2009.065482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Quatman CE, Kiapour A, Myer GD, et al. Cartilage pressure distributions provide a footprint to define female anterior cruciate ligament injury mechanisms. Am J Sports Med. 2011;39:1706–1713. doi: 10.1177/0363546511400980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Speer KP, Spritzer CE, Bassett FH, 3rd, et al. Osseous injury associated with acute tears of the anterior cruciate ligament. Am J Sports Med. 1992;20:382–389. doi: 10.1177/036354659202000403. [DOI] [PubMed] [Google Scholar]
- 106.Myer GD, Ford KR, Hewett TE. Tuck jump assessment for reducing anterior cruciate ligament injury risk. Athl Ther Today. 2008;13:39–44. doi: 10.1123/att.13.5.39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Myer GD, Ford KR, Khoury J, et al. Three-dimensional motion analysis validation of a clinic-based nomogram designed to identify high ACL injury risk in female athletes. Phys Sports Med. 2011;39:19–28. doi: 10.3810/psm.2011.02.1858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Myer GD, Ford KR, Khoury J, et al. Development and validation of a clinic-based prediction tool to identify female athletes at high risk for anterior cruciate ligament injury. Am J Sports Med. 2010;38:2025–2033. doi: 10.1177/0363546510370933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Myer GD, Ford KR, Khoury J, et al. Clinical correlates to laboratory measures for use in non-contact anterior cruciate ligament injury risk prediction algorithm. Clin Biomech. 2010;25:693–699. doi: 10.1016/j.clinbiomech.2010.04.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Myer GD, Paterno MV, Ford KR, et al. Rehabilitation after anterior cruciate ligament reconstruction: criteria-based progression through the return-to-sport phase. J Orthop Sports Phys Ther. 2006;36:385–402. doi: 10.2519/jospt.2006.2222. [DOI] [PubMed] [Google Scholar]
- 111.Myer GD, Ford KR, Hewett TE. New method to identify athletes at high risk of ACL injury using clinic-based measurements and freeware computer analysis. Br J Sports Med. 2011;45:238–244. doi: 10.1136/bjsm.2010.072843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Hewett TE, Ford KR, Myer GD. Anterior cruciate ligament injuries in female athletes: part 2, a meta-analysis of neuromuscular interventions aimed at injury prevention. Am J Sports Med. 2006;34:490–498. doi: 10.1177/0363546505282619. [DOI] [PubMed] [Google Scholar]
- 113.Myer GD, Brent JL, Ford KR, et al. A pilot study to determine the effect of trunk and hip focused neuromuscular training on hip and knee isokinetic strength. Br J Sports Med. 2008;42:614–619. doi: 10.1136/bjsm.2007.046086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Myer GD, Ford KR, Brent JL, et al. Differential neuromuscular training effects on ACL injury risk factors in“high-risk” versus “low-risk” athletes. BMC Musculoskel-etal Disord. 2007;8:39. doi: 10.1186/1471-2474-8-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Myer GD, Ford KR, Hewett TE. Rationale and clinical techniques for anterior cruciate ligament injury prevention in female athletes. J Athl Train. 2004;39:352–364. [PMC free article] [PubMed] [Google Scholar]
- 116.Myer GD, Ford KR, Hewett TE. Methodological approaches and rationale for training to prevent anterior cruciate ligament injuries in female athletes. Scand J Med Sci Sports. 2004;14:275–285. doi: 10.1111/j.1600-0838.2004.00410.x. [DOI] [PubMed] [Google Scholar]
- 117.Myer GD, Ford KR, McLean SG, et al. The effects of plyometric versus dynamic stabilization and balance training on lower extremity biomechanics. Am J Sport Med. 2006;34:445–455. doi: 10.1177/0363546505281241. [DOI] [PubMed] [Google Scholar]
- 118.Myer GD, Paterno MV, Ford KR, et al. Neuromuscular training techniques to target deficits before return to sport after anterior cruciate ligament reconstruction. J Strength Cond Res. 2008;22:987–1014. doi: 10.1519/JSC.0b013e31816a86cd. [DOI] [PubMed] [Google Scholar]
- 119.Myer GD, Paterno MV, Hewett TE. Back in the game: a four-phase return-to-sport program for athletes with problem ACLS. Rehab Manag. 2004;17:30–33. [PubMed] [Google Scholar]
- 120.Hewett TE, Myer GD, Ford KR, et al. Dynamic neuromuscular analysis training for preventing anterior cruciate ligament injury in female athletes. Instr Course Lect. 2007;56:397–406. [PubMed] [Google Scholar]
- 121.Myer GD, Ford KR, Hewett TE. Rationale and clinical techniques for anterior cruciate ligament injury prevention among female athletes. J Athl Train. 2004;39:352–364. [PMC free article] [PubMed] [Google Scholar]
- 122.Hewett TE, Myer GD. The mechanistic connection between the trunk, hip, knee, and anterior cruciate ligament injury. Exerc Sport Sci Rev. 2011;39:161–166. doi: 10.1097/JES.0b013e3182297439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Pfeiffer RP, Shea KG, Roberts D, et al. Lack of effect of a knee ligament injury prevention program on the incidence of noncontact anterior cruciate ligament injury. J Bone Joint Surg Am. 2006;88:1769–1774. doi: 10.2106/JBJS.E.00616. [DOI] [PubMed] [Google Scholar]
- 124.Soderman K, Werner S, Pietila T, et al. Balance board training: prevention of traumatic injuries of the lower extremities in female soccer players? A prospective randomized intervention study. Knee Surg Sports Trauma-tol Arthrosc. 2000;8:356–363. doi: 10.1007/s001670000147. [DOI] [PubMed] [Google Scholar]
- 125.Myer GD, Ford KR, Brent JL, et al. 2012. An integrated approach to change the outcome part i: neuromuscular screening methods to identify high ACL injury risk athletes. J Strength Cond Res. 2012;26:2265–2271. doi: 10.1519/JSC.0b013e31825c2b8f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Myer GD, Ford KR, Brent JL, et al. 2012. An integrated approach to change the outcome part ii: targeted neuromuscular training techniques to reduce identified ACL injury risk factors. J Strength Cond Res. 2012;26:2272–2292. doi: 10.1519/JSC.0b013e31825c2c7d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Filipa A, Byrnes R, Paterno MV, et al. Neuromuscular training improves performance on the star excursion balance test in young female athletes. J Orthop Sports Phys Ther. 2010;40:551–558. doi: 10.2519/jospt.2010.3325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Klugman MF, Brent JL, Myer GD, et al. Does an in-season only neuromuscular training protocol reduce deficits quantified by the tuck jump assessment? Clin Sports Med. 2011;30:825–840. doi: 10.1016/j.csm.2011.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Myer GD, Quatman CE, Khoury J, et al. Youth versus adult “weightlifting” injuries presenting to United States emergency rooms: accidental versus nonaccidental injury mechanisms. J Strength Cond Res. 2009;23:2054–2060. doi: 10.1519/JSC.0b013e3181b86712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Faigenbaum AD, Kraemer WJ, Blimkie CJ, et al. Youth resistance training: updated position statement paper from the national strength and conditioning association. J Strength Cond Res. 2009;23:S60–S79. doi: 10.1519/JSC.0b013e31819df407. [DOI] [PubMed] [Google Scholar]
- 131.McCambridge TM, Stricker PR. Strength training by children and adolescents. Pediatrics. 2008;121:835–840. doi: 10.1542/peds.2007-3790. [DOI] [PubMed] [Google Scholar]
- 132.Quatman CE, Myer GD, Khoury J, et al. Sex differences in “weightlifting” injuries presenting to United States emergency rooms. J Strength Cond Res. 2009;23:2061–2067. doi: 10.1519/JSC.0b013e3181b86cb9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Faigenbaum AD, Farrell A, Fabiano M, et al. Effects of integrative neuromuscular training on fitness performance in children. Pediatr Exerc Sci. 2011;23:573–584. doi: 10.1123/pes.23.4.573. [DOI] [PubMed] [Google Scholar]
- 134.Hickey KC, Quatman CE, Myer GD, et al. Methodological report: dynamic field tests used in an NFL combine setting to identify lower-extremity functional asymmetries. J Strength Cond Res. 2009;23:2500–2506. doi: 10.1519/JSC.0b013e3181b1f77b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Hewett TE, Myer GD, Ford KR. Reducing knee and anterior cruciate ligament injuries among female athletes: a systematic review of neuromuscular training interventions. J Knee Surg. 2005;18:82–88. doi: 10.1055/s-0030-1248163. [DOI] [PubMed] [Google Scholar]
- 136.Myer GD, Ford KR, Barber Foss KD, et al. The relationship of hamstrings and quadriceps strength to anterior cruciate ligament injury in female athletes. Clin J Sport Med. 2009;19:3–8. doi: 10.1097/JSM.0b013e318190bddb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Faigenbaum AD, Gipson-Jones TL, Myer GD. Exercise deficit disorder in youth: an emergent health concern for school nurses. J Sch Nurs. 2012;28:252–255. doi: 10.1177/1059840512438227. [DOI] [PubMed] [Google Scholar]
- 138.Faigenbaum AD, McFarland JE, Herman RE, et al. Reliability of the one-repetition-maximum power clean test in adolescent athletes. J Strength Cond Res. 2012;26:432–437. doi: 10.1519/JSC.0b013e318220db2c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.McLean SG, Walker K, Ford KR, et al. Evaluation of a two dimensional analysis method as a screening and evaluation tool for anterior cruciate ligament injury. Br J Sports Med. 2005;39:355–362. doi: 10.1136/bjsm.2005.018598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Johnson RJ. The ACL injury in female skiers. In: Griffin LY, editor. Prevention of noncontact ACL injuries. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2001. pp. 107–111. [Google Scholar]
- 141.Prapavessis H, McNair PJ. Effects of instruction in jumping technique and experience jumping on ground reaction forces. J Orthop Sports Phys Ther. 1999;29:352–356. doi: 10.2519/jospt.1999.29.6.352. [DOI] [PubMed] [Google Scholar]
- 142.President's Council on Physical Fitness. Preventing cardiovascular disease in women: how much physical activity is “good enough”? Res Digest. 2004;5:176–181. [Google Scholar]