

Abstract
Supplemental Digital Content is available in the text.
INTRODUCTION
Implant-based breast reconstruction is on the rise and the use of meshes have facilitated adoption of novel techniques.1 The disadvantages related to traditional submuscular reconstruction had led to adoption of muscle sparing or prepectoral technique.2
INDICATIONS AND PATIENT SELECTION
It is primarily used in immediate breast reconstruction and in revision surgery. Appropriate selection of patients, tumour biology, and technique are important.3
TECHNIQUE
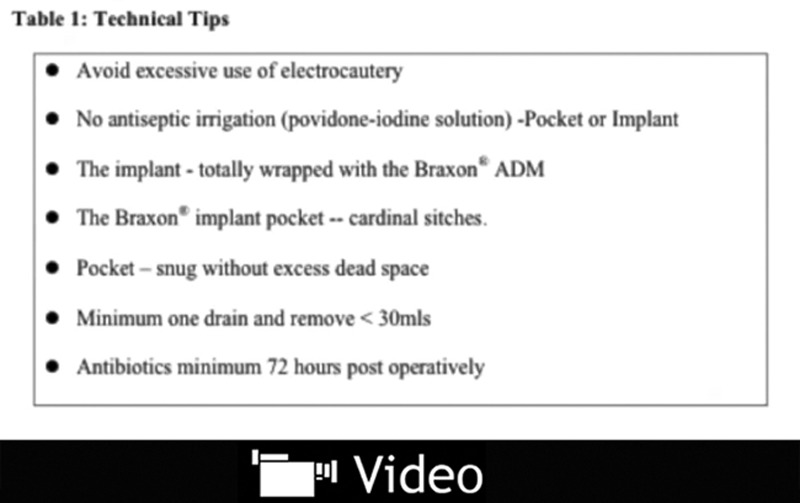
Braxon 30 × 20 cm (Decomed S.r.l., Venezia, Italy) is the only preshaped porcine-derived acelular dermal matrix (ADM) matrix that is available2 (see videos, Supplemental Digital Contents 1–3, which describe the prepectoral technique using braxon preshaped ADM step by step. These videos are available in the Related Videos section of the Full-Text article on PRSGlobalOpen.com or available at http://links.lww.com/PRSGO/A460, http://links.lww.com/PRSGO/A461, and http://links.lww.com/PRSGO/A462). It is 0.6-mm thick, packed dry, and need to be hydrated in saline, so it becomes soft after hydration. It has an anterior flap with a central slit, which when sutured gives the shape. The posterior flap with 2 windows, which is believed, let the seroma fluid out so as to avoid any collection inside the new pocket. The anterior slit and the 2 wings are closed using 2-0 vicryl continuous suture. The desired implant is then placed inside the ADM. A marking pen is used to define the exact size of the matrix that is required to form a wrap around the implant so that the ADM snugs the implant and there is no redundant space inside. It is also useful to leave a 2-mm rim around the edges, which will enable easy anchorage to the chest wall. The anterior and posterior edges of the device are sutured together using 2-0 vicryl to form a pocket for the implant. The inferior aspect of Braxon provides the required ptosis and does not require any anchorage. The lateral space can be closed to improve the shape and reduce any dead space. The new reconstructed ADM implant unit is placed over the prepectoral space and anchored to the muscle using cardinal sutures at 3, 6, 9, and 12-clock positions using 2-0 vicryl sutures. Other sutures can be placed especially laterally and anteriorly between the matrix and subcutaneous layer before the closure of the skin.
All these suture stitches speed up the process of matrix integration and, on the other side, decrease the mechanical stress of the breast implant on the lower pole by suspending the silicone weight. The wound is closed using 3-0 vicryl, and a drain is used.
OUTCOME
The recent prospective, multicenter study using Braxon in 100 cases (median follow-up, 17.9 months) showed 2% implant loss, 1% wound breakdown, 5% seroma, and 2% haematoma.4 Problems such as animation deformity and shoulder dysfunction are avoided, and postoperative pain and physiotherapy are minimal due to preservation of chest wall. It appears to be preferred in young, athletic women and in those who prefer to undisturb the chest wall musculature. Rarely, some very thin patients may develop a visible rim of the implant in the upper pole, which can be corrected by lipomodeling as shown by Becker et al.5 (6.4%) in his series.
CONCLUSIONS
The novel wrap around muscle sparing technique adds a whole new dimension to breast reconstruction.
Video Graphic 1.

See video, Supplemental Digital Content 1, which demonstrates the prepectoral technique using braxon preshaped ADM step by step. This is Part 1. This video is available in the Related Videos section of the Full-Text article on PRSGlobalOpen.com or available at http://links.lww.com/PRSGO/A460.
Video Graphic 2.

See video, Supplemental Digital Content 2, which demonstrates the prepectoral technique using braxon preshaped ADM step by step. This is Part 2. This video is available in the Related Videos section of the Full-Text article on PRSGlobalOpen.com or available at http://links.lww.com/PRSGO/A461.
Video Graphic 3.
See video, Supplemental Digital Content 3, which demonstrates the prepectoral technique using braxon preshaped ADM step by step. This is Part 3. This video is available in the Related Videos section of the Full-Text article on PRSGlobalOpen.com or available at http://links.lww.com/PRSGO/A462.
Supplementary Material
Footnotes
Presented at the Barcelona Breast Meeting (BBM 2015), March 2015, Barcelona, Oncoplastic Reconstructive Breast Surgery (ORBS) meeting, Sept 2015, Nottingham.
Disclosure: The author has no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the author.
Supplemental digital content is available for this article. Clickable URL citations appear in the text.
REFERENCES
- 1.Sbitany H, Serletti JM.Acellular dermis-assisted prosthetic breast reconstruction: a systematic and critical review of efficacy and associated morbidity. Plast Reconstr Surg. 2011;128:1162–1169. [DOI] [PubMed] [Google Scholar]
- 2.Berna G, Cawthorn SJ, Papaccio G, Balestrieri N.Evaluation of a novel breast reconstruction technique using the Braxon® acellular dermal matrix: a new muscle-sparing breast reconstruction. ANZ J Surg. 2014 Sep 29. doi: 10.1111/ans.12849. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 3.Vidya R, Fahad I.A guide to pre-pectoral breast reconstruction: a new dimension to implant based breast reconstruction. Clinical Breast Cancer. 2017 Jan 9. [Epub ahead of print] [Google Scholar]
- 4.Vidya R, Cawthorn S, Masià J, et al. Evaluation of the effectiveness of the prepectoral breast reconstruction with Braxon® dermal matrix: first multicentre European report on 100 cases. Breast J. 2017 May 8. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 5.Becker H, Lind JG, 2nd, Hopkins EG.Immediate implant-based prepectoral breast reconstruction using a vertical incision. Plast Reconstr Surg Glob Open. 2015;3:e412. [DOI] [PMC free article] [PubMed] [Google Scholar]