

Abstract
Among Ugandan fisherfolk, HIV prevalence (with estimates ranging from 15 to 40 %) is higher than in the general population (about 7 %), potentially due to high-risk behaviors and low access to HIV testing and health-care. We conducted semi-structured interviews on barriers to linkage to care with 10 key stakeholders and 25 fisherfolk within 1–2 months of their testing HIV-positive at clinic outreach events in Ugandan Lake Victoria communities. Interviews were recorded, transcribed, translated, and coded using grounded theory methods. Participants cited low healthcare access and quality of care, mobility, competing needs for work during clinic hours, stigma, and low social support as barriers. Over 10 % of clients screened positive for HIV at outreach events, and only half accessed care. Linkage to care issues may begin with the failure to attract high-risk fisherfolk to testing. New models of HIV testing and treatment delivery are needed to reach fisherfolk.
Keywords: HIV testing, Fisherfolk, Linkage to care, Uganda
Introduction
Worldwide, fisherfolk (which includes fishermen and their families, people who support the fish trade business, and sex workers) are at very high risk for HIV relative to the general population in their regions [1]. Some of the highest-prevalence fisherfolk areas are in sub-Saharan Africa, including in the Eastern African nations of Kenya and Uganda, which border Lake Victoria. For example, in Ugandan Lake Victorian fisherfolk communities, HIV prevalence is estimated to be 15–40 % [2, 3]—much higher than in the Ugandan general population, for whom HIV prevalence is estimated to be 7.3 % (8.3 % among women, 7.1 % among men) among those aged 15–49 [4]. Although exact statistics are not available, it is estimated that about a tenth of the Ugandan labor force is involved in the fisheries sector, and fishing regions (lakes, rivers, etc.) cover about 20 % of the country [5].
Several reasons have been proposed for the high HIV prevalence among fisherfolk. Globally, research has found high levels of substance abuse, multiple sex partners, and transactional sex among fisherfolk [1, 6-14]. Moreover, fisherfolk have underutilized antiretroviral treatment (ART), as compared with other subgroups [15, 16], in part due to their high mobility (they follow fish populations around the lake) and irregular work schedules; they are frequently far from healthcare, not consistently near the same clinic, and not available during clinic hours [1, 8, 10, 17-21]. Such underutilization of ART can lead to a higher likelihood of HIV transmission, if infected [22].
Community-based HIV counseling and testing (CHCT), i.e., non-healthcare-based testing, is increasing in Uganda and other parts of sub-Saharan Africa, and holds promise in efficiently reaching individuals from vulnerable populations, including mobile populations such as fisherfolk, who have limited or no access to healthcare [23, 24]. CHCT, which is typically delivered in temporary or mobile venues, brings services to settings where people work or reside and has increased the number of people who are aware of their serostatus [25]. However, because CHCT is by nature not located within health clinics, it poses challenges for timely linkage to care after diagnosis. For example, because fisherfolk are highly mobile and spend extended periods of time working away from home [1], it may not be feasible for them to initiate care immediately at a clinic location soon after they test positive.
Prior research has not examined barriers to linkage to care among fisherfolk after CHCT, although studies have indicated several barriers to HIV testing among fisherfolk that are also relevant to linkage to care. Clinic-related barriers have included patient perceptions of long wait times, understaffing, and poor referral systems [26]. Psychosocial barriers to HIV testing have included internalized HIV stigma (and fear of being seen accessing services), HIV-related discrimination, and fatalistic attitudes about health due to a high risk of accidents and drowning during deep-water fishing [10, 21, 26-28]. In particular, research indicates the presence of HIV stigma in fisherfolk communities, including loss of financial benefits (from inability to get loans or business), which can discourage testing (because of anticipation of stigma if found to be seropositive), as well as linkage to care (because of anticipation of stigma if seen accessing care or taking medications) [10, 29].
Understanding barriers to linkage to HIV care for fisherfolk, and strategies for how to overcome barriers, is critical in this new era of biomedical HIV prevention in which early treatment not only prolongs the survival of those living with HIV, but also can protect their seronegative partners from infection [21]. In the present study, we used semi-structured interviews to qualitatively explore barriers to and facilitators of linkage to care, and potential novel solutions for linkage to care, in Ugandan fishing communities in and around Lake Victoria. We recruited a range of fisherfolk, from mainland lakeshore landing sites, as well as harder-to-reach island communities that have low access to healthcare. We interviewed fisherfolk who recently screened positive for HIV at CHCT clinic outreach events. We also interviewed key stakeholders who were involved with CHCT in fisherfolk communities (e.g., healthcare providers, fisherfolk involved in community mobilization for testing events, fisherfolk who were tested and found to be HIV-negative), to gain additional perspectives on how CHCT and linkage to care could be improved for this population.
Methods
Community Partnership
We conducted this study in the context of a partnership among three research institutions, Boston Children’s Hospital, Makerere University School of Public Health, and RAND Corporation, and a medical organization that delivers HIV testing, Mildmay Uganda. The mission of Mildmay Uganda is to respond effectively to HIV and related health issues through specialized care, treatment, training, education, and research.
Testing Setting and Protocol
This study took place in four Ugandan fisherfolk communities in and around Lake Victoria: Kiyindi landing site in Buikwe District, on the shores of Lake Victoria, and on Kavenyanja Island (in Kachanga Village), Bussi Island, and Zzinga Island in Wakiso District, Lake Victoria. (See Fig. 1 for a map of the study area.) At the time of data collection, fisherfolk in these areas received HIV testing mainly through CHCT clinic outreach events conducted by Mildmay Uganda. During these events, medical staff mobilized and tested fisherfolk in temporary structures (e.g., tents) or in community venues (e.g., schools, churches). Monthly testing events were held at each community site, typically testing 25–40 people per event on Bussi Island, and 50 people per event on Kavenyanja and Zzinga Islands.
Fig. 1.

Map of Study Area in Lake Victoria, Uganda
In addition to daytime CHCT events, fisherfolk were tested at “moonlight clinics,” held at Kyanjazi landing site on Bussi Island approximately once per month from 7 pm until 12 am. These moonlight clinics provided additional HIV testing opportunities for those who worked during the daytime CHCT events [e.g., fishermen, bar attendants, motorcycle taxi (“boda–boda”) drivers]. Each moonlight clinic typically provided testing for about 50 people.
Three different brands of rapid HIV tests were used: Alere Determine, (Alere Co. LTD Japan), HIV 1/2 Stat Pak (Chembio Diagnostics, Inc., New York), and Uni-Gold™ HIV (Trinity Biotech, Ireland). Consistent with Uganda national policy algorithms for HIV testing [30], clients were considered to have screened positive at a CHCT event if they received positive screening test results on two different brands of rapid HIV tests done in immediate succession (during the event). If the two tests had disparate results, a third rapid test was used as a tie-breaker. If all three rapid tests were reportedly weakly reactive, specimens were sent for ELISA testing. (Specimens from Kiyindi CHCT events were sent to Kawolo District hospital in Buikwe district, and specimens from island CHCT events were brought to Mildmay Uganda’s main office in Lweza.)
Per Ugandan Ministry of Health policy [31], all clients who tested HIV-positive were given a “referral slip,” which provided test results and the name and district of a referral facility for obtaining ART. In addition, in recognition of the high HIV prevalence among fisherfolk, in 2013, the Ugandan Ministry of Health initiated a “test-and-treat” model [32] of offering regular HIV testing and administering ART to all fisherfolk clients testing positive, regardless of disease stage and without requiring CD4 test results (i.e., treatment as prevention) [31]. As a result, all CHCT event clients testing positive in Kavenyanja, Zzinga, and Bussi Islands were given cotrimoxazole (an antibiotic) at the testing event and referred to future island CHCT events to receive ART.
Eligibility and Recruitment
Client Interviews
Clients were eligible for semi-structured interviews if they were 18 years old or older and had screened positive for HIV at a Mildmay Uganda CHCT event between May 2014 and September 2014. They were interviewed 1–2 months after the CHCT event, between June and November 2014. During post-test counseling, counselors provided information about the study to clients who had tested positive and asked if they were interested in participating. Interested participants were referred to a member of the study team, who was present at the CHCT event to discuss the study in person. Study staff scheduled a 60-min interview session 1–2 months following the test date, to allow time for the participant to seek care.
A total of 47 individuals screened positive at the 6 CHCT outreach events, of whom 36 were approached and asked to participate in the current study (see Table 1). Eleven individuals were not approached about the study because they had previously been diagnosed with HIV, because the interviewer was not available during the event to speak with clients, or because the interviewer had already recruited a sufficient number of people for the study. Of the 36 approached, semi-structured interviews were conducted with 27 fisherfolk clients (11 women, 16 men), and clients were compensated 10,000 Ush (about 3.00 USD) for participating. Nine clients (8 men, 1 woman) were not interviewed, of whom 4 could not be reached to schedule an interview, 3 were not available for an interview, 1 migrated out of the study area, and 1 was hospitalized and died prior to the interview. One interview on Kavenyanja Island (with a female client) was discontinued too early to get usable data (because she needed to return to work), and one interview in Kiyindi (with a female client) was excluded because the participant was visiting the island for work and was not a member of the fisherfolk community. Thus, 25 interviews were analyzed (9 women, 16 men). The final sample included 8 clients from Kiyindi landing site, 4 from Bussi Island, 9 from Kavenyanja Island, and 4 from Zzinga Island.
Table 1.
Characteristics of the study sample (n = 35)
| Characteristics | HIV-Positive Clients (n = 25) | Stakeholders (n = 10) |
|---|---|---|
| Age range (years)a | ||
| 18–30 | 12 | 2 |
| 31–40 | 8 | 5 |
| > 40 | 4 | 3 |
| Gender | ||
| Women | 9 | 5 |
| Men | 16 | 5 |
| Occupation | ||
| Fisherman | 10 | 3 |
| Commercial sex worker | 1 | 0 |
| Businessman/Businesswomanb | 11 | 1 |
| Senior counselor | 0 | 1 |
| Community health worker | 0 | 1 |
| Health officerc | 0 | 3 |
| Beach management unit chairman | 0 | 1 |
| Fisherman’s wife (unemployed) | 3 | 0 |
One client was missing age
Client Businessmen/Businesswomen included: 4 fish sellers, 1 fish cleaner, 1 fish roaster, 1 alcohol seller, 1 bartender, 1 banana seller, 2 businessmen/businesswomen (unspecified type); Stakeholder businessmen/women included 1 brothel manager
Stakeholder Health Officers included: 1 nursing officer, 1 community liaison, 1 district liaison officer
Key Stakeholder Interviews
We conducted 60-min semi-structured interviews with 5 healthcare-related stakeholders who were involved in programmatic, community health, medical, and nursing roles related to CHCT with fisherfolk; and 5 fisherfolk stakeholders who were involved in CHCT with fisherfolk (e.g., in community mobilization or as testing clients). Stakeholders were purposively identified through study team members from the medical organization, who worked closely with formal and informal leaders in fisherfolk communities to mobilize clients for testing events. Oral informed consent was obtained at the beginning of the interview session. Stakeholders were compensated Ush 15,000 (about 6.00 USD) for participation.
Procedures
Client interviews and key stakeholder interviews were conducted in Luganda or in English. Interviews were recorded, transcribed verbatim, and translated into English (if necessary). Sociodemographic data (age, gender, highest level of education completed, employment status, and relationship status) were self-reported by participants at the time of the interview. Written informed consent was obtained at the beginning of the interview session. All study procedures were approved by the Intuitional Review Boards of all of the coauthors’ institutions. Permission to conduct the study was also obtained from the Uganda National Council for Science and Technology.
Qualitative Protocol
The qualitative protocols are summarized in Table 2. Open-ended, general questions about barriers to care (not specific to HIV) were asked before probes about barriers specific to linkage to HIV care to avoid bias [33] and to allow for the emergence and exploration of new topics [34].
Table 2.
Qualitative Interview Protocol on Barriers to and Facilitators of Linkage to Care
| Topic | Protocol question |
|---|---|
| Testing description | What did you think of the testing event? What worked well? What did not work as well?a |
| What strategies do you use to follow up with clients who test positive, after you provide a clinic referral? What works well?b | |
| What does not work as well? How can the linkage protocols be improved?b | |
| General barriers to care | What are the major factors that prevent regular access to healthcare (visiting a doctor; in general, not specific to HIV) in this fishing community? [FOR EACH LISTED] Why do you think that this is a barrier?a |
| General facilitators of care | What are the major factors that facilitate regular access to healthcare (visiting a doctor; in general, not specific to HIV) in this fishing community? [FOR EACH LISTED] Why do you think that this is a facilitator?a |
| Barriers to HIV care | What are the major barriers or challenges that could prevent people in fishing communities from getting timely care for HIV after they test positive? [FOR EACH LISTED] Why do you think that this is a barrier?a |
| How do you think people’s beliefs and attitudes about HIV, health, and healthcare can affect whether they get care after testing positive?a | |
| How do you think people’s beliefs and attitudes about traditional healers can affect whether they get care after testing positive?a | |
| How do you think community norms around HIV, healthcare, and traditional healers can affect whether they get care after testing positive?a | |
| Facilitators of HIV care | What are the major factors that could facilitate people in fishing communities getting timely care for HIV after they test positive? [FOR EACH LISTED] Why do you think that this is a facilitator?a |
| Perceived need | Do you think how healthy or unhealthy a person feels might affect whether he or she gets timely care for HIV after testing positive? Why or why not?a |
| Psychological barriers | In what ways might stigma be a challenge to someone getting timely care after testing positive?a |
| In what ways might lack of social support be a challenge to getting timely care after testing positive?a | |
| Tangible barriers | In what ways is lack of transportation to healthcare a barrier to getting timely care after testing positive?a |
| What about not being able to get an appointment at the clinic, because the clinic is too busy or not open at convenient times?a | |
| How is the cost of medical care a challenge or not a challenge to receiving timely HIV care?a | |
| How can quality of healthcare services in fishing communities affect getting timely care after testing positive?a | |
| Personal healthcare | Did you visit a healthcare provider after you tested positive? [IF YES] How long after you tested positive did you visit a healthcare provider for the first time?c |
| Do you think it is necessary for you to get HIV care? Why or why not?c |
HIV-positive clients and stakeholders
Stakeholders only
HIV-positive clients only
Client Protocol
Similar to other qualitative research on HIV care use [35, 36], we adapted the Behavioral Model of Health Services Use [27] as a framework for the interview protocol, which allowed us to explore predisposing characteristics and enabling factors related to timely linkage to HIV care. Predisposing characteristics affect the general tendency to use or not use care (e.g., socio-demographic characteristics) [37], and enabling factors facilitate or impede use of care (e.g., stigma, discrimination, distance to clinic) [38]. Based on prior literature, we asked about both structural factors [1, 8, 10, 17-21], such as those related to clinic systems and fisherfolk mobility, and psychosocial factors [3, 10, 26], such as stigma, disclosure, and lack of social support. The qualitative protocol contained probes about specific factors and examined the acceptability of several different potential programmatic solutions for facilitating linkage to HIV care.
Stakeholder Protocol
The stakeholder protocol contained similar questions as the client protocol. Healthcare providers were additionally asked to describe the testing scenario for each setting, the role of stakeholders’ organizations in facilitating linkage to care, and their ideas for feasible and acceptable ways to improve linkage to care.
Qualitative Analysis
Data were organized and managed in Dedoose (version 6.1.18), and analyzed using grounded theory [39] to identify themes indicative of barriers to and facilitators of healthcare utilization and linkage to HIV care, and potential interventions to improve linkage. Four members of the research team (three Americans and one Ugandan) read all transcripts to identify themes (overarching categories describing the phenomenon under study), and independently developed an initial listing of types of barriers to and facilitators of linkage to HIV care. From these listings, the team developed a codebook listing each theme accompanied by a detailed description, inclusion/exclusion criteria, and typical examples. Two coders then marked segments of text corresponding to each theme on a random sample of 20 % of transcripts, and Cohen’s Kappa was calculated to determine inter-rater reliability. Final Kappa values ranged from 0.7 to 1.0 (mean 0.84). After attainment of inter-rater reliability, one coder systematically applied the codebook to all interviews. American and Ugandan members of the team then jointly examined the distribution of themes within and between participant groups (i.e., linked versus not linked to care within clients; clients versus key stakeholders). By including multiple (i.e., American and Ugandan) perspectives on the analysis team, we were able to discuss the cultural context of the narratives as we jointly interpreted the data.
Because the protocol dictated that we conduct multiple interviews within the same timeframe (with multiple clients who attended the same testing events), interviews could not be transcribed and translated in time for investigators to determine whether saturation was reached (i.e., that all main variations of each theme emerged) prior to the next testing event and set of interviews. Thus, we designed the study to include a sufficient number of participants to ensure that saturation would be reached, as suggested by prior research [40, 41].
Results
Descriptive Characteristics of the Sample
Table 1 shows the characteristics of the sample. Of the 25 HIV-positive clients interviewed, about half (n = 12) were young (aged 18–30 years), and the majority (n = 16) were men. The largest subgroup was of fisherman (n = 10), and 6 were involved in the fish business (4 fish sellers, 1 fish cleaner, and 1 fish roaster); one was a commercial sex worker, 1 sold alcohol, 1 worked as a bartender, 1 sold bananas, 2 did not clarify the specifics of their business (describing themselves simply as a businessman/businesswoman), and 3 were unemployed wives of fishermen. Of the 10 stakeholders, most (n = 7) were under age 40, and half were men and half were women. The healthcare provider stakeholders included a clinic counselor/expert client, a nursing officer, and a community health worker from the local community, and a community liaison and a district liaison officer (i.e., coordinators of community mobilization and CHCT events at the community and district levels) from the testing organization. The community stakeholders included 3 fishermen, the chairman of a beach management unit (BMU, a public community fisheries management institution), and a brothel manager.
Percentage of Seropositive HIV Tests and Percentage of Clients Linked to Care
Across 6 testing events, 450 clients were tested and of those, 47 clients (10.4 %) were identified to be seropositive. Of those 47 clients, 36 were approached and asked to participate in the current study. As shown in Fig. 2, among the 36 clients who screened positive for HIV, 20 (55.6 %) reported that they linked to care within 1–2 months post-testing. Of the 36 clients, 27 were interviewed, of whom 25 were eligible and had usable data (16 who linked to care and 9 who did not). Of the 9 clients who were not interviewed, 5 were reached by phone, and 3 reported that they were linked to care and 2 reported that they were not linked to care.
Fig. 2.
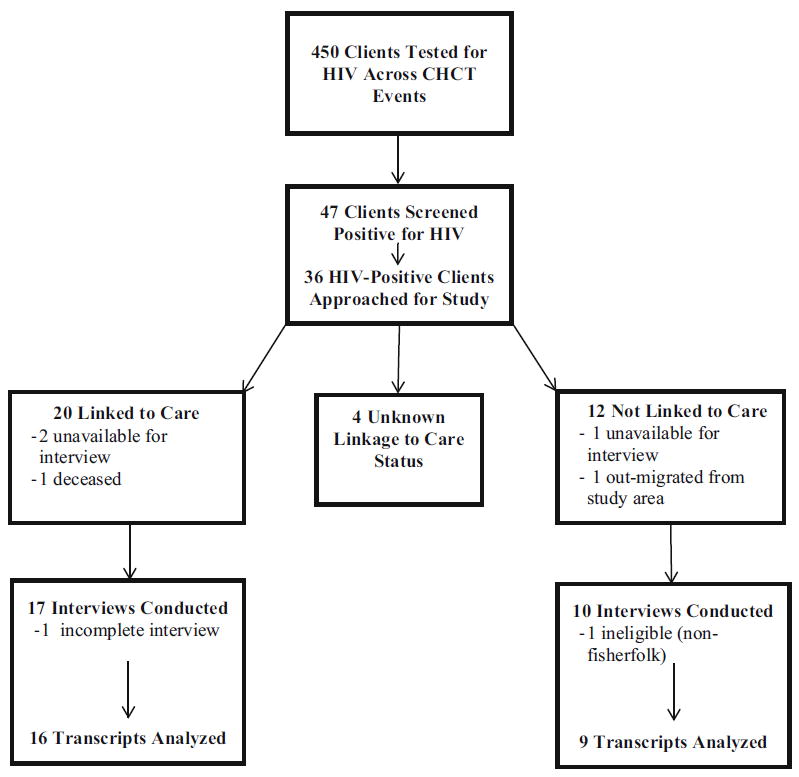
Flow chart of HIV-positive clients interviewed after community HIV counseling and testing (CHCT) events
Overview of Qualitative Results
Overall, structural barriers related to access to healthcare were paramount across narratives, and psychosocial barriers were less emphasized. Primarily, the narratives indicated that fisherfolk had difficulty linking to HIV care because they were highly mobile and not consistently close to clinics, and that the cost of transportation could be prohibitive. The quality of healthcare was a key factor; fisherfolk and stakeholders noted that existing service delivery (including clinic hours and long queues) was not conducive to fisherfolks’ hectic work and irregular travel schedules. Fisherfolks’ competing need to work during clinic hours led to particular difficulties in getting care. In terms of psychosocial barriers, stigma was commonly discussed, although key stakeholders seemed to minimize stigma’s effects. Those who were not linked to care told vivid stories of discrimination experienced by themselves as well as others who were living with HIV. Social support and disclosure to close, non-stigmatizing others was seen as a facilitator of linkage to care that could help to counteract the effects of stigma. Overall, clients and stakeholders suggested tailoring healthcare delivery to fisherfolk lifestyles, through expanding clinic hours, building clinics in fisherfolk communities, and increasing healthcare outreach hours and locations in fisherfolk communities.
Structural Barriers
Transportation and Mobility
Key stakeholders and fisherfolk clients were in agreement that transportation issues were primary in terms of getting to care and staying on treatment. Due to their considerable knowledge of the population, stakeholders were able to draw from experiences with multiple kinds of fisherfolk and provide a broad perspective. Stakeholders described the mobility of the population, and the need for fishermen to migrate seasonally to find the best source of fish, impeding timely linkage to HIV care.
You test them here and there is more fish there; they will not wait, they have to go for the fish—they follow their fish…If it [the fish] migrates very far for so many months then they will take those so many months—Female Community Liaison (stakeholder).
Healthcare provider stakeholders in particular described the challenges of fisherfolk not being able to access care in the same place each time, and not being able to get enough treatment to last them months at a time while they were traveling on the lake.
There are some who say “I will come back” but again when they go, of course there are people who are moving from place to place, and somebody might not even happen to come back—Female Nursing Officer (stakeholder).
Clients cited similar barriers to linking to care and to getting refills for medications, including the cost of transport, the inconvenient schedules of ferries from islands to clinics on the mainland, and the need to travel long distances to get to a clinic.
The problem is with the health centers; they are very far. Some people get problems with transport in cases [when the] drugs are finished and [he/she] doesn’t have money to spend on transport—Fisherman (client, linked to care).
Those who had linked to care tended to discuss more facilitators to linkage to care related to transportation than did those who had not linked. They reported that the CHCT events in fisherfolk communities were helpful in overcoming transportation barriers; they also described the value of having social support, in terms of someone who could pick up medications on their behalf if needed.
At times it may be a very long distance [to the clinic] yet the sickness would have made you so weak that you may not have the energy to reach your destination! My friend, I assure you that there is no way you can access care, unless when you have someone you trust enough to give them your treatment card and send them to the hospital to help you pick the drugs—Wife of a Fisherman (client, linked to care).
Those who had not linked to care tended to cite the cost of transport as the highest barrier to accessing care, alongside the scarcity of facilities in convenient locations, such as landing sites.
For instance, if you send someone to Kiyindi, one imagines spending 16,000 Ush [about 4.00 USD] going there, she or he may wonder, “Why is my money getting wasted like that? Let me give up.” When the dose is over, she or he says, “After all, I have healed.” And some don’t know that even after the dose is over, she or he has to go back—Businesswoman (client, not linked to care).
Competing Needs
The theme of competing needs was intertwined with issues of transportation and mobility. Several participants mentioned competing work needs in particular as a reason for not accessing care, due to inconvenient clinics hours and location, as well as long clinic queues. For example, fisherfolk said that they would lose wages if they waited in clinic queues and took the time to travel to the clinic. Women and men discussed similar competing needs related to work, but women additionally spoke of the competing needs of childcare and food preparation. Fishermen especially seemed to balance the benefit of getting treatment against the need to earn money and keep their jobs, and oftentimes the value of having to work and getting paid outweighed the need to get treatment. In addition to fishing itself, specific tasks related to fishing (e.g., boat off-loading, drying fish, selling fish, cleaning up) left little time to visit the clinic before taking to the waters again.
The economic status, too—it may be that the time when he [fisherman] is able to make 10,000 Ush [about 3.00 USD] but yet it is the same time when you [healthcare workers] have come to the school [to hold a CHCT event]. So, he imagines the time he is going to spend going to the school [to be tested], yet he left his family starving, he may decide that he first makes that 10,000 Ush before going to the school, and by the time he is done making that money, you health [workers] would have left—Male Fish Trader (client, not linked to care).
Perceptions of competing needs seemed to be more common among fisherfolk who were not linked to care, who felt that clinic hours were not conducive to their work schedules. Those clients explained that, while they made attempts to visit the clinic, they often left after seeing a long line ahead of them, and felt too discouraged to return later in the day.
Now imagine you have told me to go to Lugazi hospital, what time will I leave work to get to Lugazi? Remember you have to sit and wait in the taxi park; when you board the taxi at 6:00, what time will you come back? Remember there are queues at the health center and you have to join those queues. Remember at home the kids need to eat. So it would be hard for one to get drugs—Businesswoman (client, not linked to care).
Those linked to care, however, were more persistent, despite the hindrance of long lines at the clinic. For example, they explained that, if the clinic were closed by the time they arrived, they would continue to make attempts when they could, and wait in line if necessary in order to access drugs. Many described a sense of responsibility to get care and treatment, irrespective of the logistical and work related challenges faced while trying.
In case he or she finds the health center closed, he or she is inconvenienced. Personally, I would go back the next day and wait until they open. When I find them busy, I can be patient for them to finish what they are doing—Female Commercial Sex Worker (client, linked to care).
Key stakeholders echoed the frustrations of fisherfolk with regard to clinic hours, but explained that clinics are generally understaffed and unable to operate on a more flexible schedule, because staff live on the mainland and must travel to and fro in order to provide services. Moreover, government facilities only offer ART on specific days, and close early; because fisherfolk are highly mobile, they are likely to miss announcements for clinic days, and may be unaware of clinic schedules in different sites or unable to get to the clinic before it closes. For example, Kiyindi landing site was located less than a mile from a health clinic, but ART was only dispensed one day a week, with restricted daytime hours.
Proposed Solutions to Structural Barriers
Key stakeholders proposed novel solutions to structural issues that involved tailoring clinic structures and ART delivery systems to fisherfolk communities, which they viewed as distinct from other Ugandan healthcare delivery areas. One such solution was to deliver ART to fisherfolk communities in similar outreach clinic events as the CHCT events. (This practice of providing ART was since initiated by the testing organization, but it was not conducted by governmental clinics or on a wide scale in the country.)
What can be made differently is actually that HCT event can also be made double as HCT and outreach event…As you are doing HCT, another fisherman will come [saying], “Me I have come for septrine.” You give them, they go and ride their boats. “I have come for my [ART].” You give them, they go and offload their fish.–Female District Liaison Officer (stakeholder).
Enabling fisherfolk to access care from anywhere on the lake was also proposed, as well as expanding clinic hours to be more conducive to fishermen’s schedules.
First of all the clinics operate on specific clinic days. For example, you may find that this facility’s clinic days are Mondays so if fishermen can’t get on the landing site where the clinic is on Mondays, they have issues of accessing care. That is why I was talking about outreaches are best for them—Female Community Liaison (stakeholder).
Key stakeholders also suggested educating healthcare workers about the fisherfolk lifestyle, to encourage more flexible practices.
Changing the attitude of the health workers to knowing that the fisherfolk is a special group…if they know fishermen can seek care like after 3 o’clock, then they can get to work…Even the health workers in those facilities need to be trained—Female District Liaison Officer, (stakeholder).
Fisherfolk clients echoed the need to bring medications to the places where they lived and worked, due to the general low access to healthcare on the islands and around the lake. A prevailing suggestion was to build more government health centers on the islands.
If we had a nearby health center here, it means that we patients would get the service on time…Here at our landing site, we should get where we can put a clinic where we patients can meet healthcare providers. Here, the health center is very far from us and we spend too much money going there to get drugs—Fisherman (client, linked to care).
In addition, fisherfolk suggested expanding the number of days and locations of clinic outreach events. This would allow clients to consistently get medications and refills without disruption in treatment.
The recommendation I would give is that you put more efforts in sending in more drugs and to visit us all the time—Male Fish Trader (client, not linked to care).
There also seemed to be a widespread perception among fisherfolk of a need for more education around HIV and medications, so that they understood the purpose of taking the medications and getting to care, and also of methods used for preventing HIV.
The only thing that is desired by everyone at the landing site is to be educated further… Whoever is given the responsibility of a counselor should be competent enough to come to the villages and teach the people on how to prevent infection such that those that are not yet infected can protected themselves. Almost it is on the landing sites where there should be hospital because almost everyone here is infected; those living without HIV are very few—Businessman (client, linked to care).
It is through that health education that one develops interest (for treatment)—Female Fish Seller (client, not linked to care).
Psychosocial Barriers
Stigma
All clients felt that stigma was a persistent challenge. Some clients and stakeholders noted that fear of stigma drives some to travel far away to get care, to decrease the chance of seeing someone they know at the clinic.
It is hard for most of the people to go and get drugs because there are people that know them yet they wouldn’t want to be known. Sometimes, most of them fear their husbands, i.e., when one finds out that she is infected but doesn’t want her husband to know about it and that is the problem. It is the setback and a challenge to us as people here at the landing site since we are so afraid of being talked about—Businesswoman (client, linked to care).
Stigma was generally expressed differently by those who were and were not linked to care. Those who were not linked to HIV care acknowledged the presence of stigma, and for example, feared gossip and social isolation as well as potential loss of social standing, and felt shame about their diagnosis. However, those linked to care, especially fisherman, further maintained the attitude that stigma, although present, could not prevent them from starting treatment, citing social support and personal strength.
Let me tell you about that thing [stigma]; if you are not strong-hearted it really affects you. Imagine you would be in the middle of a conversation with colleagues and they back-bite someone, “That one is already sick!” you would feel so down already and feel that they may be referring to you.…it is what causes fear in most of the people not to come for treatment simply because of our colleagues on the village [that stigmatize others]… I however gave in with all my heart to search for a longer life [started on ART]—Wife of a Fisherman (client, linked to care).
Fear of stigma seemed to be more prohibitive to those who had not linked to care; they did not want to be seen waiting at the clinic for ART, and described the potential for violence or disputes to erupt following disclosure to spouses and family members. In addition, clients who had not linked to care relayed concrete discrimination experiences, sharing stories of being isolated by family members who knew or heard rumors of their serostatus. Such in-depth stories did not emerge among clients who were linked to care.
Personally, I told my mother that I am sick [HIV-positive] but as I was urinating at night, she told me, “Don’t piss in the same container with us, you will transmit the illness to us!”… She started isolating me and she would say that I should avoid recklessly touching things at home because that illness [HIV] is spread that way—Businesswoman (client, not linked to care).
While key stakeholders acknowledged that clients did not want to be seen getting ART at the clinic, many seemed unaware of the extent to which stigma affected the community. Several mentioned that stigma seemed to be decreasing, having been more of a challenge earlier in the epidemic. Others described fear of stigma as a motivator to get to care, rather than a barrier.
Because many of them are also sick, it’s also better there [stigma is less]…I see like for us here fear of AIDS is vanishing, people now test—Male BMU Chairman (stakeholder).
Disclosure and Social Support
Lack of disclosure was closely tied to stigma. Clients and stakeholders noted that many fear being stigmatized as a result of disclosure, which ultimately led to low social support and difficulty accessing care.
Yes some of them go for testing secretly and when they find out they are positive they don’t disclose to their families… So there he can’t get the help because there is no one he has told—Fisherman (stakeholder).
All clients stressed the importance of having support from friends and family in order to access care, especially in terms of providing transport to the clinic, medication reminders, and picking up medication on their behalf.
If that person is living alone, s/he may be demotivated to go and take his/her drugs but if s/he is living with people, one may tell him/her to take drugs in case s/he hasn’t—Male Fish Trader (client, not linked to care).
However, as with stigma, more clients who had linked to care said that not disclosing their status to friends and family would not prevent them from seeking care.
If I haven’t disclosed to others, it doesn’t stop me from accessing treatment—Fisherman (client, linked to care).
Proposed Solutions to Psychosocial Barriers
Some stakeholders suggested working with BMUs or community organizations (e.g., the Red Cross) to dispense medications, to help overcome the stigma of being seen visiting a clinic. This would also allow for greater accessibility of ART outside of clinic hours.
One solution could be going to them like we have today, and sit at a certain corner. Then we go and whisper to the BMU Chairman that [among] those who we tested here, there are those who are positive. We are sitting at a certain corner so that they come stealthily, they wouldn’t like to be seen…Use the Red Cross Office which is near there. After all it is near the public toilets. So one can [act] as if he is going to the public toilet—Male Community Health Worker (stakeholder).
Clients also felt that formal social support should be offered by health workers. They explained that a follow up phone call from a counselor or a trained peer could motivate them to get care and take their medication, even if they had not yet disclosed to family or friends.
Having someone that can encourage you or motivate you and remind you [of] the time for getting drugs, or to visit you sometime to ask you about the challenges you have found or the condition you are living in at that time. That arrangement would be very good—Male Fish Trader (client, not linked to care).
Several clients suggested training local community members to provide reminders about clinic outreach events and medication refills, and to offer general referrals and basic first aid care so that clients do not have to rely upon health workers who are only in fisherfolk communities for short periods of time.
In my opinion about what can enable people, before the date for getting drugs reaches, it requires that we get people to come and remind us…I would wish the healthcare providers could train about five people in our communities about what to do if they found patients in such and such condition, to offer first aid—Fisherman (client, not linked to care).
Discussion
In this study of barriers to linkage to care among fisherfolk, we found that the confluence of structural barriers related to clinic systems with fisherfolk mobility and work schedules led to great challenges in accessing care. Clinic systems are typically not set up to accommodate fisherfolk lifestyles, which involve busy workdays away from the mainland, with competing needs and little time for personal breaks to access healthcare. Although fisherfolk acknowledged the effects of stigma, psychosocial barriers were weighed less heavily than these structural barriers in impeding care access. Our findings are consistent with prior research indicating that fisherfolks’ mobility has considerable influence on their relatively low healthcare-seeking behaviors, [1, 8, 10, 17-21] and our study adds to prior literature in its focus on linkage to HIV care.
Over half of fisherfolk did access HIV care within 1–2 months of testing positive, despite these barriers. We found that their perseverance was facilitated by social support (e.g., someone to pick up medications) and clinic accommodations (e.g., holding midnight clinics), as well as a strong belief in the importance of accessing care to stay healthy. Some fisherfolk were determined to get care, despite logistical barriers. On the other hand, fisherfolk who did not link to care were more likely to be deterred by structural barriers, including long clinic lines or inconvenient clinic hours (that overlapped with work hours). In contrast to our research, which largely suggests similar structural barriers among those linked and not linked to care, but qualitative differences in attitudes about overcoming the barriers, U.S. studies have found greater perceived structural barriers among those not retained in care [35]. Further, those who did not link to care more often described experiencing discrimination and losing social support from friends and family than did those who accessed care—a powerful deterrent that was underestimated by key stakeholders. These reports of HIV stigma among fisherfolk are consistent with those of other studies [10, 29]. We did not, however, find evidence for fatalism as a barrier to care-seeking, in contrast to prior fisherfolk research [10], potentially because participants in the present study tended to emphasize structural factors as a primary barrier, more than psychosocial factors.
We found that only 10 % of fisherfolk tested were found to be HIV positive. This percentage is lower than that found in prior research, which has suggested that the prevalence of HIV among fisherfolk may be as high as 15–40 % [2, 3]. One of the reasons for our lower estimate may be because the events mainly identified those who were newly testing positive, and one would expect higher numbers if all individuals in the community were tested, including those who already were aware of their positive serostatus. Moreover, testing conducted through clinic outreach events may not attract those who do not wish to be tested in a public setting and who feel HIV stigma (possibly because they are at high HIV risk and suspect that they are seropositive). In addition, the competing needs for HIV care identified here are also likely to impact the extent to which fisherfolk can take the time out of their busy workday to get tested. Thus, linkage to care issues may begin with the failure to attract large numbers of high-risk fisherfolk to clinic outreach testing events, and different models of testing as well as healthcare may be needed for this population.
The results of the present study, combined with key stakeholder and client suggestions, suggest several ways in which linkage to care could be improved among fisherfolk. Clearly, systems-level changes in healthcare delivery to fisherfolk are needed. In the present study, we collaborated with a private non-profit organization that was able to flexibly deliver healthcare to fisherfolk by bringing testing and ART directly to isolated island communities; as suggested by participants in the present study (and since this study was conducted), this organization started to conduct outreach testing events in which they also provide ART. Such models need to be supported by and expanded to the public sector as well. Further, other types of testing models may be more conducive to testing larger numbers of fisherfolk and increasing serostatus awareness in fisherfolk communities, a first step to increasing the number of fisherfolk on ART. For example, home-based HIV counseling and testing, as well as home-based ART provision, have been shown to be cost-effective and acceptable to clients in rural Ugandan communities [32, 42-46], as well as in other sub-Saharan countries [47-49], and thus may be worthy of further exploration for fisherfolk.
Limitations to generalizability should be considered. Participants were recruited through convenience sampling, and the sample is not meant to be representative of fisherfolk. The narratives and behaviors of the Ugandan fisherfolk in the present study may not reflect those of fisherfolk in other regions of the world, with different healthcare infrastructures and HIV epidemiologies. Further, we interviewed only nine participants who did not link to care, and it is possible that, with more participants, additional differences would have emerged between clients who linked to care versus who did not link to care. In addition, our study focused on linkage to care after testing among people newly diagnosed with HIV. However, people cycle in and out of care, and the engagement process is multi-faceted and non-linear [50]. Thus, similar research is needed to explore factors that not only affect initial engagement in care, but also re-engagement and retention over time, in order to develop tailored interventions to overcome specific barriers at each stage of the care continuum.
Conclusion
In sum, high population mobility, competing needs, low or inconvenient access to healthcare, and HIV stigma all play a role in impeding linkage to HIV care among fisherfolk. New, flexible models of outreach for HIV testing and treatment delivery are needed to reach fisherfolk at highest risk, to accommodate their mobile lifestyles and competing needs.
Acknowledgments
This research was funded by R21MH098657 from the National Institute of Mental Health (LM Bogart, Principal Investigator). We gratefully acknowledge Betty Nakibuka, Muhumya Esau, Jak Ategeka and the Mildmay field team, and the Village Health Teams at Kavenyanja, Kiyindi, and Zzinga for their essential contributions to community mobilization and data collection activities.
References
- 1.Kissling E, Allison EH, Seeley JA, et al. Fisherfolk are among groups most at risk of HIV: cross-country analysis of prevalence and numbers infected. AIDS. 2005;19(17):1939–46. doi: 10.1097/01.aids.0000191925.54679.94. [DOI] [PubMed] [Google Scholar]
- 2.Smolak A. A meta-analysis and systematic review of HIV risk behavior among fishermen. AIDS Care. 2014;26(3):282–91. doi: 10.1080/09540121.2013.824541. [DOI] [PubMed] [Google Scholar]
- 3.Opio A, Muyonga M, Mulumba N. HIV infection in fishing communities of Lake Victoria Basin of Uganda–a cross-sectional sero-behavioral survey. PLoS ONE. 2013;8(8):e70770. doi: 10.1371/journal.pone.0070770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Uganda Ministry of Health, ICF International, Uganda Centers for Disease Control and Prevention Uganda AIDS Indicator Survey 2011: Preliminary Report. Kampala, Uganda: Uganda Ministry of Health; 2012. [Google Scholar]
- 5.Tanzarn N, Bishop-Sambrook C. The dynamics of HIV/AIDS in small-scale fishing communities in Uganda. Rome, Italy: HIV/ AIDS Programme, Food and Agriculture Organization (FAO) of the United Nations; 2003. [Google Scholar]
- 6.Sileo KM, Kintu M, Chanes-Mora P, Kiene SM. “Such behaviors are not in my home village, I got them here”: A qualitative study of the influence of contextual factors on alcohol and HIV risk behaviors in a fishing community on Lake Victoria, Uganda. AIDS Behav. 2016;20(3):537–47. doi: 10.1007/s10461-015-1077-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Tumwesigye NM, Atuyambe L, Wanyenze RK, et al. Alcohol consumption and risky sexual behaviour in the fishing communities: evidence from two fish landing sites on Lake Victoria in Uganda. BMC Public Health. 2012;12:1069. doi: 10.1186/1471-2458-12-1069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kiwanuka N, Ssetaala A, Nalutaaya A, et al. High incidence of HIV-1 infection in a general population of fishing communities around Lake Victoria, Uganda. PLoS ONE. 2014;9(5):e94932. doi: 10.1371/journal.pone.0094932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Seeley J, Nakiyingi-Miiro J, Kamali A, et al. High HIV incidence and socio-behavioral risk patterns in fishing communities on the shores of Lake Victoria,Uganda. Sex Transm Dis. 2012;39(6):433–9. doi: 10.1097/OLQ.0b013e318251555d. [DOI] [PubMed] [Google Scholar]
- 10.Allison EH, Seeley JA. HIV and AIDS among fisherfolk: A threat to ‘responsible fisheries’? Fish Fish. 2004;5(3):215–34. [Google Scholar]
- 11.Pickering H, Okongo M, Bwanika K, Nnalusiba B, Whitworth J. Sexual behaviour in a fishing community on Lake Victoria, Uganda. Health Transit Rev. 1997;7(1):13–20. [PubMed] [Google Scholar]
- 12.Zafar M, Nisar N, Kadir M, Fatmi Z, Ahmed Z, Shafique K. Knowledge, attitude and practices regarding HIV/AIDS among adult fishermen in coastal areas of Karachi. BMC Public Health. 2014;10(14):437. doi: 10.1186/1471-2458-14-437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Duwal SD, Garba MA, Yusuf AA, et al. Vulnerability of fishing communities to HIV/AIDS and impact on fish productivity in Nigeria. IOSR-JAVS. 2015;8(2):52–9. [Google Scholar]
- 14.Nagoli J, Holvoet K, Remme M. HIV and AIDS vulnerability in fishing communities in Mangochi district, Malawi. Afr J AIDS Res. 2010;9(1):71–80. doi: 10.2989/16085906.2010.484575. [DOI] [PubMed] [Google Scholar]
- 15.Ostermann J, Reddy EA, Shorter MM, et al. Who tests, who doesn’t, and why? Uptake of mobile HIV counseling and testing in the Kilimanjaro Region of Tanzania. PLoS ONE. 2011;6(1):e16488. doi: 10.1371/journal.pone.0016488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mugisha E, van Rensburg GH, Potgieter E. Factors influencing utilization of voluntary counseling and testing service in Kasenyi fishing community in Uganda. J Assoc Nurses AIDS Care. 2010;21(6):503–11. doi: 10.1016/j.jana.2010.02.005. [DOI] [PubMed] [Google Scholar]
- 17.Uganda Ministry of Agriculture Animal Industry and Fisheries. Uganda Strategy for Reducing the Impact of HIV and AIDS on Fishing Communities. Kampala, Uganda: Ministry of Agriculture, Animal Industry and Fisheries; 2005. [Google Scholar]
- 18.Nunan F. Mobility and fisherfolk livelihoods on Lake Victoria: implications for vulnerability and risk. Geoforum. 2010;41(5):776–85. [Google Scholar]
- 19.Nunan F, Luomba J, Lwenya C, Yongo E, Odongkara K, Ntambi B. Finding space for participation: fisherfolk mobility and co-management of Lake Victoria fisheries. Environ Manag. 2012;50(2):204–16. doi: 10.1007/s00267-012-9881-y. [DOI] [PubMed] [Google Scholar]
- 20.Kwena ZA, Camlin CS, Shisanya CA, Mwanzo I, Bukusi EA. Short-term mobility and the risk of HIV infection among married couples in the fishing communities along Lake Victoria, Kenya. PLoS ONE. 2013;8(1):e54523. doi: 10.1371/journal.pone.0054523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kher A. Review of the Social Science Literature on Risk and Vulnerability to HIV/AIDS Among Fishing Communities in Sub-Saharan Africa. Norwich, UK: The School of Development Studies, University of East Anglia; 2008. [Google Scholar]
- 22.Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493–505. doi: 10.1056/NEJMoa1105243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Matovu JK, Makumbi FE. Expanding access to voluntary HIV counselling and testing in sub-Saharan Africa: alternative approaches for improving uptake, 2001–2007. Trop Med Int Health. 2007;12(11):1315–22. doi: 10.1111/j.1365-3156.2007.01923.x. [DOI] [PubMed] [Google Scholar]
- 24.Grabbe KL, Menzies N, Taegtmeyer M, et al. Increasing access to HIV counseling and testing through mobile services in Kenya: strategies, utilization, and cost-effectiveness. J Acquir Immune Defic Syndr. 2010;54(3):317–23. doi: 10.1097/QAI.0b013e3181ced126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.World Health Organization. Global HIV/AIDS Response: Epidemic Update and Health Sector Progress Towards Universal Access. Geneva, Switzerland: World Health Organization; 2011. [Google Scholar]
- 26.Mugisha E, van Rensburg GH, Potgieter E. Strategic framework for increasing accessibility and utilization of voluntary counseling and testing services in Uganda. AIDS Res Treat. 2011;2011:912650. doi: 10.1155/2011/912650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995;36(1):1–10. [PubMed] [Google Scholar]
- 28.FHI 360. Contextual barriers, motivations, and coping strategies in the uptake of HCT and condoms among fisherfolk in a fish landing site in Busia District: findings of a rapid qualitative assessment: Communication for Healthy Communities. FHI 360; 2014. [Google Scholar]
- 29.Gordon A. HIV/AIDS in the fisheries sector in Africa. Penang, Malaysia: World Fish Center; 2005. [Google Scholar]
- 30.Uganda Ministry of Health. Uganda National Policy Guidelines for HIV Voluntary Counselling and Testing. Kampala, Uganda: Ministry of Health; 2005. [Google Scholar]
- 31.Uganda Ministry of Health. Addendum to the National Antiretroviral Treatment Guidelines. Kampala, Uganda: Ministry of Health; 2013. [Google Scholar]
- 32.Kyaddondo D, Wanyenze RK, Kinsman J, Hardon A. Home-based HIV counseling and testing: client experiences and perceptions in Eastern Uganda. BMC Public Health. 2012;12:966. doi: 10.1186/1471-2458-12-966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Becker HS. Problems of inference and proof in participant observation. Am Sociol Rev. 1958;23(6):652–60. [Google Scholar]
- 34.Bernard HR. Research Methods in Anthropology: Qualitative and Quantitative Approaches. 2. Thousand Oaks, CA: Sage Publications; 1994. [Google Scholar]
- 35.Yehia BR, Stewart L, Momplaisir F, et al. Barriers and facilitators to patient retention in HIV care. BMC Infect Dis. 2015;15:246. doi: 10.1186/s12879-015-0990-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Holtzman CW, Shea JA, Glanz K, et al. Mapping patient-identified barriers and facilitators to retention in HIV care and antiretroviral therapy adherence to Andersen’s Behavioral Model. AIDS Care. 2015;27(7):817–28. doi: 10.1080/09540121.2015.1009362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Nakigozi G, Makumbi F, Reynolds S, et al. Non-enrollment for free community HIV care: findings from a population-based study in Rakai, Uganda. AIDS Care. 2011;23(6):764–70. doi: 10.1080/09540121.2010.525614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Duff P, Kipp W, Wild TC, Rubaale T, Okech-Ojony J. Barriers to accessing highly active antiretroviral therapy by HIV-positive women attending an antenatal clinic in a regional hospital in western Uganda. J Int AIDS Soc. 2010;13:37. doi: 10.1186/1758-2652-13-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Glaser BG, Strauss AL. The Discovery of Grounded Theory: Strategies for Qualitative Research. Transaction Publishers. 2009 [Google Scholar]
- 40.Guest G, Bunce A, Johnson L. How many interviews are enough?: an experiment with data saturation and variability. Field Methods. 2006;18(1):59–82. [Google Scholar]
- 41.Francis JJ, Johnston M, Robertson C, et al. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychology & Health. 2010;25(10):1229–45. doi: 10.1080/08870440903194015. [DOI] [PubMed] [Google Scholar]
- 42.Mulogo EM, Batwala V, Nuwaha F, Aden AS, Baine OS. Cost effectiveness of facility and home based HIV voluntary counseling and testing strategies in rural Uganda. Afr Health Sci. 2013;13(2):423–9. doi: 10.4314/ahs.v13i2.32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Marseille E, Kahn JG, Pitter C, et al. The cost effectiveness of home-based provision of antiretroviral therapy in rural Uganda. Appl Health Econ Health Policy. 2009;7(4):229–43. doi: 10.2165/11318740-000000000-00000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Apondi R, Bunnell R, Awor A, et al. Home-based antiretroviral care is associated with positive social outcomes in a prospective cohort in Uganda. J Acquir Immune Defic Syndr. 2007;44(1):71–6. doi: 10.1097/01.qai.0000243113.29412.dd. [DOI] [PubMed] [Google Scholar]
- 45.Menzies N, Abang B, Wanyenze R, et al. The costs and effectiveness of four HIV counseling and testing strategies in Uganda. AIDS. 2009;23(3):395–401. doi: 10.1097/QAD.0b013e328321e40b. [DOI] [PubMed] [Google Scholar]
- 46.Tumwesigye E, Wana G, Kasasa S, Muganzi E, Nuwaha F. High uptake of home-based, district-wide, HIV counseling and testing in Uganda. AIDS Patient Care STDS. 2010;24(11):735–41. doi: 10.1089/apc.2010.0096. [DOI] [PubMed] [Google Scholar]
- 47.Helleringer S, Mkandawire J, Reniers G, Kalilani-Phiri L, Kohler HP. Should home-based HIV testing and counseling services be offered periodically in programs of ARV treatment as prevention? A case study in Likoma (Malawi) AIDS Behav. 2013;17(6):2100–8. doi: 10.1007/s10461-012-0365-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Knight LC, Van Rooyen H, Humphries H, Barnabas RV, Celum C. Empowering patients to link to care and treatment: qualitative findings about the role of a home-based HIV counselling, testing and linkage intervention in South Africa. AIDS Care. 2015;27:1–6. doi: 10.1080/09540121.2015.1035633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Tabana H, Nkonki L, Hongoro C, et al. A cost-effectiveness analysis of a home-based HIV counselling and testing intervention versus the standard (facility based) HIV testing strategy in rural South Africa. PLoS ONE. 2015;10(8):e0135048. doi: 10.1371/journal.pone.0135048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Maulsby C, Kinsky S, Jain KM, Charles V, Riordan M, Holtgrave DR. Unpacking linkage and reengagement in HIV care: a day in the life of a positive charge care coordinator. AIDS Educ Prev. 2015;27(5):405–17. doi: 10.1521/aeap.2015.27.5.405. [DOI] [PubMed] [Google Scholar]