

Abstract
OBJECTIVE:
The aim of this study was to evaluate the histological responses of cementum, root dentin, and pulp following intentional root injuries caused via self-tapping and self-drilling miniscrews.
MATERIALS AND METHODS:
Fourteen patients (with a mean age of 15.7 years and age range of 14–18 years) who were scheduled for the extraction of all four first premolars as part of their orthodontic treatment plan participated in this study. The roots of the right and the left quadrants' first premolars were designedly injured using self-tapping miniscrews and self-drilling miniscrews, respectively. Teeth were extracted eight weeks after the injury. Cementum repair was assessed through histological examinations.
RESULTS:
In this study, 40 teeth (75.4%) showed reparative cementum formation and 13 teeth (24.5%) showed no repair. There was no significant difference between the two groups regarding the formation of reparative cementum (P = 0.3). In all examined teeth, the inflammatory response of the pulp to the cold test was within the normal range.
CONCLUSION:
This study showed that in most cases, the healing of cementum was observed eight weeks after the injury and the two methods of miniscrew insertion showed no significant difference when it comes to the healing process.
Keywords: Cementum, root resorption, temporary anchorage devices
Introduction
Anchorage control is essential in orthodontics and can affect the outcome of the treatment considerably. Temporary Anchorage Devices (TADs) have become popular in clinical orthodontics due to several advantages especially in the treatment of non-compliant patients.[1,2]
TADs have the ability to provide absolute anchorage and this fact eliminates the undesirable side effects associated with the conventional biomechanics in orthodontics, thus making possible the impossible considered biomechanics.[3]
Some of the most widely used TADs are miniscrews,[1] and these miniscrews can be placed readily at various sites such as in the interradicular alveolar bone and the palatal bone.[4,5,6] Considerable risks exist when miniscrews are placed in interdental areas.[7] Root damage can occur from either improper placement of the miniscrews or tooth contact with the miniscrews during orthodontic treatment.[8] Two methods were used for the placement of miniscrews: self-tapping technique, which requires the preparation of a pilot hole before insertion, and the self-drilling technique, which does not require predrilling.[9]
Son et al.[10] compared the effect of root contact on the stability of miniscrews in these two methods and they reported that the self-drilling method showed significantly higher mobility than the self-tapping method. Herman and Cope[11] assessed the extent of root damage after inserting self-tapping manually driven miniscrews. The greatest depth of perforation observed on the roots of the extracted teeth was 0.25 mm with maximum manual force.
In response to traumatic dental injuries, there are two ways in which resorption can happen:(1) external resorption and (2) inflammatory and replacemental resorption or ankyloses.[12]
Andreasen[13] evaluated the healing process after surgical injuries in the roots of rat teeth. He concluded that the repair of cementum and PDL occurred after 14 days and increased over a course of long-term observation.
Asschericlex et al.[14] histologically examined three teeth injured secondarily to miniscrew placement and concluded that the initial repair of the periodontal structures occurs in 12 weeks after the removal of screws, with healing nearly completely achieved after 20 weeks.
The aim of this study was to evaluate the histological response of cementum, root dentin, and pulp following intentional root injuries caused by self-tapping and self-drilling miniscrews.
Material and Methods
Fourteen female orthodontic patients (14–18 years old with a mean age of 15.7 years) were included in this study. The selected patients were in their permanent dentition stage and they were candidates for the extraction of all four first premolars as part of their orthodontic treatment plan.
Patients who had systemic diseases, decayed teeth, and restorations on their first premolars, as well as patients with periodontal breakdown and periapical pathology of first premolars were excluded from the study. All patients and their parents received explanations about the protocol of the study and signed a consent form, which was approved by ethics committee of Mashhad University of Medical Sciences.
Required photographs and radiographs for the orthodontic treatment were taken for each patient. Standard edgewise 0.022-in brackets (Dentarum, Germany) were bonded to the first premolar teeth. The custom-made wire guide was fabricated. The guide was comprised of a stem of 0.017 × 0.025-in stainless steel wire, to which five 0.016 × 0.022-in stainless steel wires were welded horizontally at the intervals of 2 mm from each other [Figure 1]. To determine the exact insertion site of miniscrews, the guide wire was inserted in the vertical slot of brackets along the long axis of the tooth. Then, a periapical radiograph (with paralleling cone technique) was taken. This method helped us to determine the exact placement of miniscrew to ensure root contact.
Figure 1.

Custom-made wire guide
Self-tapping and self-drilling miniscrews (G2A, 8 mm length, 1.4 mm diameter Jeil, Seoul, South Korea) were used in this study. Self-drilling miniscrews were inserted in the mesial side of the first premolars of left quadrants (upper and lower) under local anesthesia. The custom-made guide determined the exact insertion site, so that the miniscrews were inserted 6 mm above the cementoenamel junction (CEJ) and to standardize the degree of damage, nearly half of the diameter of the miniscrew (0.7 mm) was designed to establish root contact. After causing intentional injury to the roots, the miniscrews were removed immediately.
In the mesial side of first premolars of upper and lower right quadrants, a hole of 1 mm in diameter and 6 mm in length was drilled with a number 1 pilot drill (Jeil, Seoul, South Korea) using a slow speed (35 rpm) handpiece under continuous saline-solution irrigation. Then, a self-tapping miniscrew (Jeil, G2A, Seoul, South Korea) was inserted in the prepared hole and after root contact establishment, the miniscrew was removed immediately. Similar to the self-drilling miniscrews half of the diameter of miniscrew (0.7 mm) had established root contact. The exact insertion site was determined similar to the previous group.
In days 0, 1, and 56, the pulp test using a cold spray (Denronic, Germany) was performed to evaluate clinical pulpitis. If the patients reported pain for less than 10 seconds, the pulp condition was considered normal and if the pain perception was more than 10 seconds, the pulp condition was reported as pulpitis. Eight weeks after the insertion of the miniscrews, the first premolar teeth of patients were extracted for orthodontic purposes.
Immediately after extraction, the teeth were fixed in a 10% neutrally buffered formalin solution for 48 hours, and then demineralized in 10% ethylendiaminetetraacetic acid (EDTA, MERK, Germany) for 60 days.
After ensuring complete decalcification, the teeth were embedded inside paraffin blocks and serially sectioned in a mesio-distal direction with the microtome set to 4μm. Hematoxylin and Eosin staining was performed for histological examination.
A pathologist examined all histological sections under a light microscope. Root repair, formation of reparative dentin on the pulpal side, and the inflammatory responses of the pulp were evaluated. Results were reported according to the criteria described below:
For the healing of resorption lacuna with restorative cementum:
Without repair
Partial repair: part of the surface of resorption lacuna was covered with reparative cementum
Functional repair: the total surface of resorption lacuna was covered with reparative cementum without root contour reconstruction
Anatomic repair: the complete surface of resorption lacuna was repaired by reparative cementum with the reconstruction of root contour.[15]
For the inflammatory response:
Grade 1: No inflammatory cells
Grade 2: Less than 10 inflammatory cells
Grade 3: severe inflammatory lesion, which appears as an abscess or too many inflammatory cells in coronal pulp
Grade 4: necrosis of pulp.[16]
Results
Fourteen patients (56 teeth) fulfilling the inclusion criteria and exclusion criteria were enrolled for this study. Three teeth were excluded from the study because of the improper preparation of histological sections. None of the patients complained of pain after the trauma. All teeth were extracted eight weeks after the injury and underwent histopathological examination. Of the 53 teeth evaluated histologically, it was evident that the dentin in all specimens was damaged without reparative dentin formation. No pulpal damage was seen in any histological section. The teeth showed a normal repair process by recruitment of cells especially cementoblasts [Figures 2–4].
Figure 2.
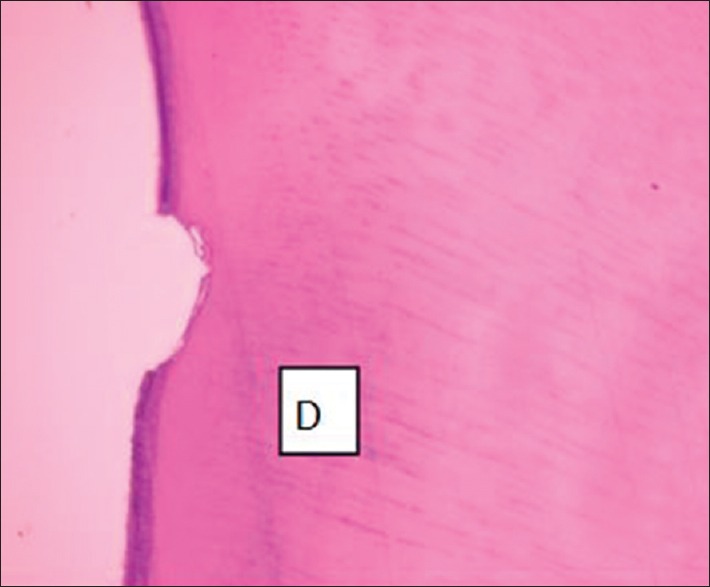
Roor resorption without repair. Dentin (D). (H and E staining, original magnification 100×)
Figure 4.
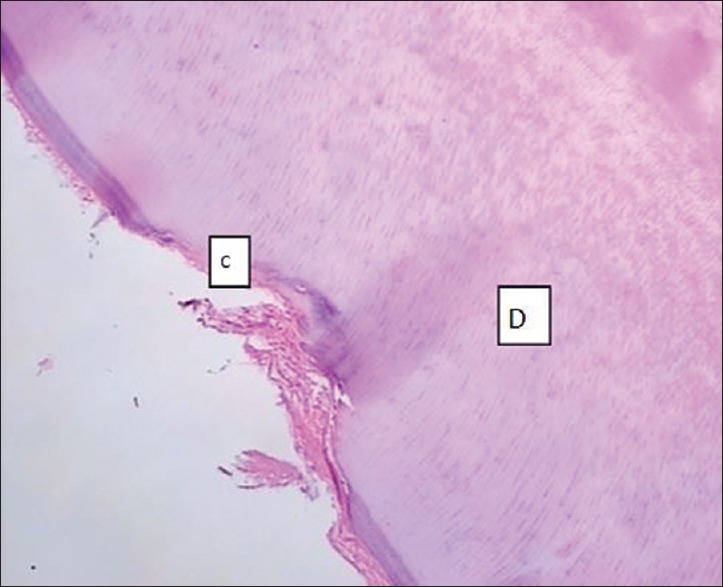
Partial repair with cellular cementum. Cementum (C), Dentin (D). (H and E staining, original magnification 100×)
Figure 3.
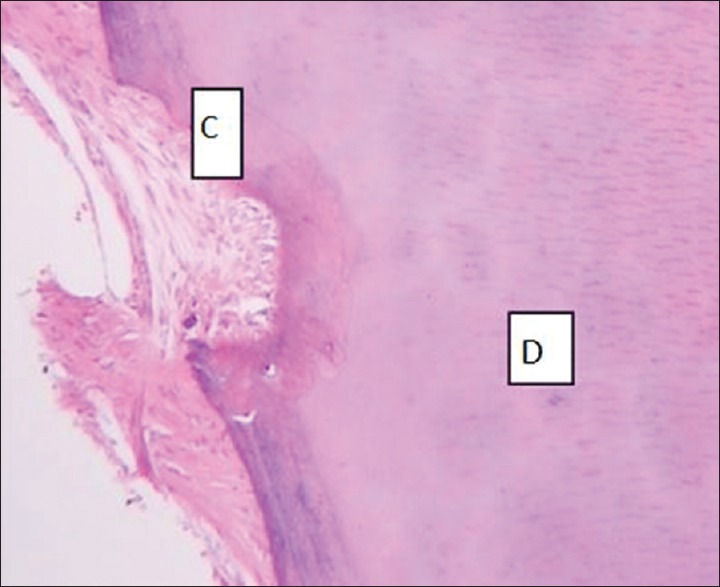
Functional repair with cellular cementum. Cementum (C), Dentin (D). (H and E staining, original magnification 400×)
Nearly 75% of the examined teeth (N = 40) showed repair with cellular cementum (either partial or functional) and the others (N = 13) showed no cementum repair.
Table 1 shows the status of cementum repair in the injured teeth. There was no significant difference in cementum repair status between the upper right (self-tapping) and the upper left (self-drilling) quadrants. In addition, there was no statistically significant difference in cementum repair status between the lower right (self-tapping) and the lower left (self-drilling) quadrants [Table 1]. Comparison between the right side (self-tapping) and the left side (self-drilling) showed that there was no significant difference regarding cementum repair between these two groups [Table 2]. In all examined teeth, the histopathological evaluation of pulp showed few or no inflammatory cells (grade1) and the clinical evaluation of pulp (the cold test result) was reported within the normal range [Figure 5].
Table 1.
Status of cementum repair in injured teeth

Table 2.
Comparison between the right side (self-tapping) and left side (self-drilling) regarding cementum repair

Figure 5.
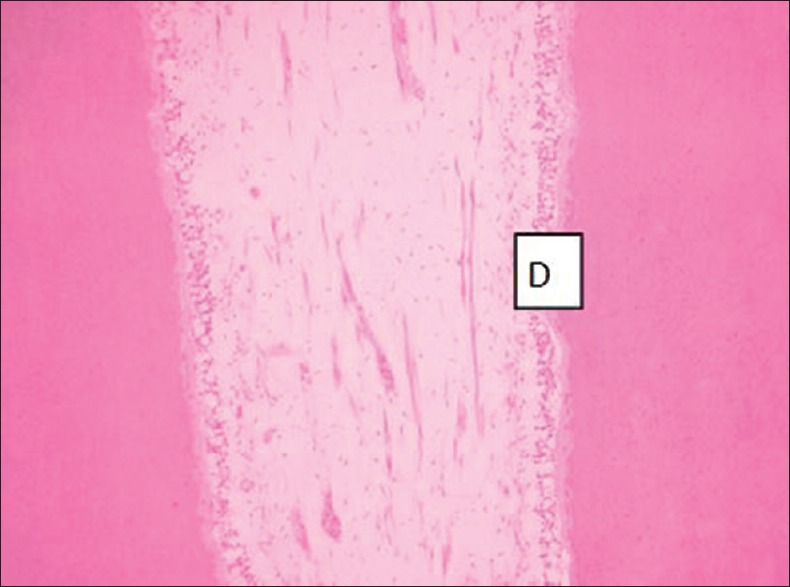
Photomicrograph showing grade 1 inflammatory response of pulp. Dentin (D) (H and E staining, original magnification 400×)
Discussion
Cementum repair after intentional root injuries caused by TADs has been evaluated qualitatively[3,17,18] and quantitatively.[19] In our study, we compared the healing status of the cementum after intentional root injury using two methods of miniscrew insertion; self-drilling vs. self-tapping techniques.
The histological examination was used to evaluate cementum repair, which has been well documented in the literature.[20] In our study, 40 teeth (75.4%) showed repair with cellular cementum (22 teeth, partial and 18 teeth, functional). No anatomical repair was observed in the repaired teeth. Owmann et al.[15] reported that anatomical repair occurred only in the apical third of the root. However, in our study, the middle third of the root was injured using the miniscrew. Healing cementum was almost exclusively of the cellular type. In our study, histological examination was performed eight weeks after the removal of TADs.
Kadiaglou et al. showed that after the elimination of the stimulus, cementum repair may be observed after 3 or 4 weeks by scanning electron microscopy (SEM).[8] Nevertheless, in the study of Chen et al. cementum repair was not observed even after 24 weeks.[21] It should be noted that these two studies were performed on animals. Ahmed et al.[19] evaluated the reparative potential of cementum histologically after initial root contact with self-drilling miniscrews in human subjects and concluded that the cementum repair was nearly completed in 8 weeks. Brisceno et al.[3] used self-tapping miniscrews for this purpose. In our study, we used split mouth design to compare self-drilling miniscrews and self-tapping miniscrews with regard to the amount of root injury.
At the self-tapping side, 69.2% of the injured teeth showed repair and at the self-drilling side, 81.5% showed cementum repair. Hole preparation in the self-tapping technique may compromise the healing process,[22] although there was no statistically significant difference between these two different techniques (P = 0.3). Renjen et al.[18] also reported that there was no significant difference in the healing status of roots between self-tapping and self-drilling miniscrews.
In our study, none of the injured teeth showed formation of reparative dentine on the pulpal side. Also, in Brisceno et al.[3] and Renjen et al.[18] studies, the formation of reparative dentine was not reported. It has been shown that the formation of the reparative dentine occurs following chronic traumatic injuries and it is stimulated when the remaining dentin is reduced more than 1.5 mm.[3]
It has been reported that deep injuries to the root following the insertion of miniscrews could devitalize the injured tooth.[23] In our study, the inflammatory status of pulp was reported as grade 1 for all teeth and the cold test was within the normal range. In the previous studies, similarly, clinical pulpitis was not observed.[8,18] Despite the absence of clinically significant damages, clinicians should be conscious when placing miniscrews and precise clinical and radiographic evaluation of the insertion site should be taken into consideration.
Conclusion
In this study, in most cases, the cementum repair — either partial or functional — was observed eight weeks after the injury, which represented the beginning of repair in this period. Teeth injured by self-tapping miniscrews showed less cementum repair compared to the teeth injured by self-drilling miniscrews. However, this difference was not statistically significant. Thus, as suggested in previous studies, all preventive procedures before inserting the miniscrews should be considered to avoid damage to the adjacent teeth.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to extend their appreciation to the vice chancellor for research of Mashhad University of Medical Sciences for the financial support.
References
- 1.Bae SM, Park HS, Kyung HM, Kwon OW, Sung JH. Clinical application of micro-implant anchorage. J Clin Orthod. 2002;36:298–302. [PubMed] [Google Scholar]
- 2.Deguchi T, Takano-Yamamoto T, Kanomi R, Hartsfield JK, Jr, Roberts WE, Garetto LP. The use of small titanium screws for orthodontic anchorage. J Dent Res. 2003;82:377–81. doi: 10.1177/154405910308200510. [DOI] [PubMed] [Google Scholar]
- 3.Brisceno CE, Rossouw PE, Carrillo R, Spears R, Buschang PH. Healing of the roots and surrounding structures after intentional damage with miniscrew implants. Am J Orthod Dentofac Orthop. 2009;135:292–301. doi: 10.1016/j.ajodo.2008.06.023. [DOI] [PubMed] [Google Scholar]
- 4.Herman RJ, Currier GF, Miyake A. Mini-implant anchorage for maxillary canine retraction: A pilot study. Am J Orthod Dentofac Orthop. 2006;130:228–35. doi: 10.1016/j.ajodo.2006.02.029. [DOI] [PubMed] [Google Scholar]
- 5.Park HS, Lee SK, Kwon OW. Group distal movement of teeth using microscrew implant anchorage. Angle Orthod. 2005;75:602–9. doi: 10.1043/0003-3219(2005)75[602:GDMOTU]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Sugawara J, Daimaruya T, Umemori M, Nagasaka H, Takahashi I, Kawamura H, et al. Distal movement of mandibular molars in adult patients with the skeletal anchorage system. Am J Orthod Dentofac Orthop. 2004;125:130–8. doi: 10.1016/j.ajodo.2003.02.003. [DOI] [PubMed] [Google Scholar]
- 7.Kuroda S, Sugawara Y, Deguchi T, Kyung HM, Takano-Yamamoto T. Clinical use of miniscrew implants as orthodontic anchorage: Success rates and postoperative discomfort. Am J Orthod Dentofac Orthop. 2007;131:9–15. doi: 10.1016/j.ajodo.2005.02.032. [DOI] [PubMed] [Google Scholar]
- 8.Kadioglu O, Buyukyilmaz T, Zachrisson BU, Maino BG. Contact damage to root surfaces of premolars touching miniscrews during orthodontic treatment. Am J Orthod Dentofac Orthop. 2008;134:353–60. doi: 10.1016/j.ajodo.2006.09.069. [DOI] [PubMed] [Google Scholar]
- 9.Holmgren EP, Seckinger RJ, Kilgren LM, Mante F. Evaluating parameters of osseointegrated dental implants using finite element analysis-a two-dimensional comparative study examining the effects of implant diameter, implant shape, and load direction. J Oral Implantol. 1998;24:80–8. doi: 10.1563/1548-1336(1998)024<0080:EPOODI>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 10.Son S, Motoyoshi M, Uchida Y, Shimizu N. Comparative study of the primary stability of self-drilling and self-tapping orthodontic miniscrews. Am J Orthod Dentofac Orthop. 2014;145:480–5. doi: 10.1016/j.ajodo.2013.12.020. [DOI] [PubMed] [Google Scholar]
- 11.Herman R, Cope JB. Miniscrew implants: IMTEC mini ortho implants. Semin Orthodont. 2005;11:32–9. [Google Scholar]
- 12.Andreasen JO, Andreasen FM. Root resorption following traumatic dental injuries. Proc Finn Dent Soc. 1992;88(Suppl 1):95–114. [PubMed] [Google Scholar]
- 13.Andreasen JO. Histometric study of healing of periodontal tissues in rats after surgical injury. II. Healing events of alveolar bone, periodontal ligaments and cementum. Odontologisk Revy. 1976;27:131–44. [PubMed] [Google Scholar]
- 14.Asscherickx K, Vannet BV, Wehrbein H, Sabzevar MM. Root repair after injury from mini-screw. Clin Oral Implants Res. 2005;16:575–8. doi: 10.1111/j.1600-0501.2005.01146.x. [DOI] [PubMed] [Google Scholar]
- 15.Owman-Moll P, Kurol J, Lundgren D. Repair of orthodontically induced root resorption in adolescents. Angle Orthod. 1995;65:403–8. doi: 10.1043/0003-3219(1995)065<0403:ROOIRR>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 16.Parolia A, Kundabala M, Rao NN, Acharya SR, Agrawal P, Mohan M, et al. A comparative histological analysis of human pulp following direct pulp capping with Propolis, mineral trioxide aggregate and Dycal. Aust Dent J. 2010;55:59–64. doi: 10.1111/j.1834-7819.2009.01179.x. [DOI] [PubMed] [Google Scholar]
- 17.Hembree M, Buschang PH, Carrillo R, Spears R, Rossouw PE. Effects of intentional damage of the roots and surrounding structures with miniscrew implants. Am J Orthod Dentofac Orthop. 2009;135:280 e1–9. doi: 10.1016/j.ajodo.2008.06.022. [DOI] [PubMed] [Google Scholar]
- 18.Renjen R, Maganzini AL, Rohrer MD, Prasad HS, Kraut RA. Root and pulp response after intentional injury from miniscrew placement. Am J Orthod Dentofac Orthop. 2009;136:708–14. doi: 10.1016/j.ajodo.2007.12.031. [DOI] [PubMed] [Google Scholar]
- 19.Ahmed VK, Rooban T, Krishnaswamy NR, Mani K, Kalladka G. Root damage and repair in patients with temporary skeletal anchorage devices. Am J Orthod Dentofac Orthop. 2012;141:547–55. doi: 10.1016/j.ajodo.2011.11.014. [DOI] [PubMed] [Google Scholar]
- 20.de Vasconcellos LM, Ricardo LH, Balducci I, de Vasconcellos LG, Carvalho YR. Histological analysis of effects of 24% EDTA gel for nonsurgical treatment of periodontal tissues. J Oral Sci. 2006;48:207–14. doi: 10.2334/josnusd.48.207. [DOI] [PubMed] [Google Scholar]
- 21.Chen YH, Chang HH, Chen YJ, Lee D, Chiang HH, Yao CC. Root contact during insertion of miniscrews for orthodontic anchorage increases the failure rate: An animal study. Clin Oral Implants Res. 2008;19:99–106. doi: 10.1111/j.1600-0501.2007.01418.x. [DOI] [PubMed] [Google Scholar]
- 22.Gupta N, Kotrashetti SM, Naik V. A comparitive clinical study between self tapping and drill free screws as a source of rigid orthodontic anchorage. J Maxillofac Oral Surg. 2012;11:29–33. doi: 10.1007/s12663-011-0240-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.McCabe P, Kavanagh C. Root perforation associated with the use of a miniscrew implant used for orthodontic anchorage: A case report. Int Endod J. 2012;45:678–88. doi: 10.1111/j.1365-2591.2012.02022.x. [DOI] [PubMed] [Google Scholar]