

Abstract
Context:
Uncorrected refractive errors are the leading cause of visual impairment.
Aims:
To assess the prevalence and patterns of spectacles use among those aged ≥40 years in the South Indian state of Telangana.
Settings and Design:
This was a population-based, cross-sectional study, in which 6150 people were enumerated from 123 clusters in the two districts of Telangana state (Adilabad and Mahbubnagar) using a two-stage cluster random sampling methodology.
Materials and Methods:
Participants were visited in their households and presenting visual acuity (VA) was assessed in all cases followed by pinhole VA if presenting VA was worse than 6/12. A questionnaire was used to collect information on the current and previous spectacles use, type of spectacles, and details of the spectacles provider.
Statistical Analysis Used:
Stata statistical software version 12.
Results:
Among 5881 participants examined, 53.7% were women, and 82% had no formal education. The prevalence of current spectacles use was 28.8% (95% confidence interval: 27.6–30.0). On applying multiple logistic regression analysis, spectacles use was significantly associated with older age groups, female gender, higher levels of education, and residing in Adilabad district. Bifocals were the most commonly used type of spectacles (56.3%), and private eye clinics (70.3%) were the leading service providers. The spectacles coverage was 53.6%.
Conclusions:
We reported on prevalence and patterns of spectacles use using a large representative sample and a high response rate. More than half of those who may benefit from spectacles were using them, suggestive of a reasonable primary eye care coverage in the two districts studied.
Keywords: Rapid assessment of visual impairment, refractive errors, spectacles coverage, Telangana
Uncorrected refractive errors (UREs) are a leading cause of visual impairment.[1] Although a major cause, URE had received major attention only in the recent past and included in the VISION 2020 global initiative.[2,3] Population-based studies conducted in the last two decades in India have revealed that UREs are the second largest cause of blindness and the leading cause of moderate visual impairment.[4,5] While URE can be corrected using spectacles, several barriers limit the uptake of services.[6,7] The primary eye care vision centre model is conceived and implemented as part of a larger service delivery model by L V Prasad Eye Institute (LVPEI) in South India to address the burden of uncorrected refractive errors.[8,9]
LVPEI has an integrated system of secondary and primary eye care facilities covering the underserved populations in rural areas in Andhra Pradesh and Telangana. While secondary centres are full-fledged eye facilities with an ophthalmologist and a team of personnel providing comprehensive eye care services, primary eye care vision centres are staffed by a 1-year trained vision technician who provides primary eye care including refraction and dispensing facilities.[10]
Telangana was carved out from the larger state of Andhra Pradesh as a new state. In Telangana, the refraction services including both refraction and spectacles dispensing are provided by private eye clinics (ophthalmology practices) and optical outlets in urban areas.[11] While the larger optical chains are staffed by qualified optometrists or trained paramedical ophthalmic personnel, smaller optical outlets have a visiting ophthalmologist or are part of eye clinics. In rural areas, optical services are limited or nonexistent. In remote areas, outreach eye screening camps are conducted occasionally by nongovernment agencies where both refraction services and spectacles are provided “free of cost” to the participants.[11]
Refractive error correction through the dispensing of spectacles forms the main activity of primary eye care service models such as vision centres. Understanding the prevalence and patterns of spectacles use can provide insight into the primary eye care situation in a given region. A similar study was conducted in one urban and two rural locations and showed a variation in spectacles use with geographical location, suggesting a need for more local studies for planning primary eye care services.[11]
We conducted a large, population-based, cross-sectional study among those aged 40 years and older to understand the prevalence and patterns of spectacles use and spectacles coverage in the districts of Adilabad and Mahbubnagar in the newly formed state of Telangana in India.
Materials and Methods
Ethics approval
The Institutional Review Board of Hyderabad Eye Research Foundation approved the study protocol. The study adhered to the tenets of the Declaration of Helsinki. Verbal informed consent was obtained from each participant after explaining the study procedure and before starting the eye examination. Data collection for the project was carried out from February to April in Adilabad district and October to December 2014 in Mahbubnagar district.[12]
Study area
The combined population of the two districts of Adilabad and Mahbubnagar was 6.8 million (Census 2011). Mahbubnagar is the largest district in the state and is closer to the capital Hyderabad. It has the highest proportion of rural population (85%) as compared to other districts including Adilabad (72%). The overall proportion of rural population in Telangana is 69%. The literacy rate in the rural population in Mahbubnagar district (52%) is lower compared to Adilabad district (55.7%), both of which are lower than the state average. Both the districts are considered among the 250 backward districts in the country.
Like other districts in the state, the health-care facilities in general and eye care facilities in particular are confined to large towns. A few nongovernmental organizations provide eye care services through “outreach” screening camps in Mahbubnagar district, and the government-run hospital at Adilabad also provides eye care including cataract surgeries. LVPEI has established a rural network of eye care centres in both these districts. In Adilabad, two secondary eye care centres (the first in 1996 and the second in 2005) followed by 19 primary eye care centres (vision centres) were established. In Mahbubnagar, a secondary centre was established in 1998 followed by the establishment of 10 primary eye care centres. In both the districts, the LVPEI rural eye care network is one of the largest eye care service providers, offering cataract surgeries.
Sampling procedure
The sampling procedure used in this study is described elsewhere.[11,12,13] In brief, a cluster random sampling methodology was used to select 123 study clusters in two districts. As this study was nested within another large study that was aimed to assess the prevalence of visual impairment, the sample size exceeded the calculated minimum required to study spectacles use. All the villages in the geographical area were listed and a population proportionate to size method was adopted to randomly select the study clusters. The compact segment sampling method was used to select the individual households within the study clusters.[14] Repeated attempts were made to ensure high response rate.
Data collection
The data collection protocol is described in our previous publications.[11,12,13] In brief, a study team that comprised an experienced vision technician and a community eye health worker visited households selected in the clusters and carried out the data collection. After collecting personal and demographic information and information on the present and past spectacles use, a clinical eye examination was conducted. Visual acuity (VA) was assessed using a standard Snellen chart at a distance of 6 m. Both unaided and pinhole VA was recorded. Aided VA was also recorded if a participant reported using spectacles. VA assessment was recorded with pinhole if it was worse than 6/12.
All teams used the same protocols for data collection, and the quality of data collection was closely monitored. A questionnaire was used to collect information on the current and previous use of spectacles. Among those who reported using spectacles at the time of the eye examination, the type of spectacles, spectacles provider, and amount paid to procure spectacles were asked. The spectacles providers were classified as “private eye clinics” where services are provided either by an ophthalmologist or other trained eye care providers such as ophthalmic assistants either on daily or on weekly visits and also included eye examinations.[11] It is typical of clinics where eye examinations are conducted. The “optical shops” were places where no formally trained eye care personnel are usually available. The “eye camps” are makeshift screening camps where spectacles are given at “no cost” to the participants. LVPEI eye care centres included the primary (vision centres) and secondary care facilities of LVPEI.
Among the participants who reported the previous use of spectacles, the reason for discontinuation of spectacles was elicited. All the questions were asked in the local language and responses were recorded on a precoded data collection form that had a list of possible responses. If the participant gave a reason that was not in the list, then the response was specified and marked as other reason. This procedure was similar to that used in our previous studies to allow comparison between the different districts and regions.[11] The data collection workflow is shown in Fig. 1.
Figure 1.
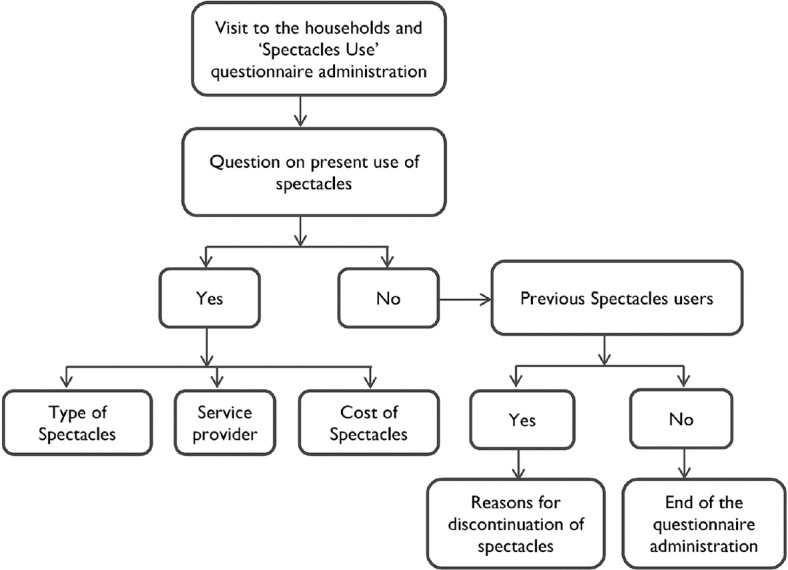
Flowchart showing the different stages of data collection
Definitions
We used the spectacles coverage definitions as reported elsewhere.[11] “Unmet need” was defined as unaided VA < 6/18 and improving to 6/18 or better with a pinhole in the better eye and not using spectacles for distance vision. “Met need” was defined as unaided VA < 6/18 and improving to 6/18 or better with their spectacles in the better eye. In other words, unmet need means uncorrected/undercorrected refractive error and met needs means “corrected” refractive error. The total of “unmet need” and “met need” was considered as the “total need” or prevalence of refractive errors. Based on this, SC is calculated: SC (%) = Met need/total need × 100.[11]
Data management
Data analysis was conducted using Stata statistical software version 12 (College Station, TX: StataCorp LP).[15] Point prevalence estimates are calculated and presented with 95% confidence intervals (CIs). Multivariable analysis was done using multiple logistic regression analysis to assess the association between the current spectacles use and demographic variables such as age, gender, education, and area of residence. Adjusted odds ratio (OR) with 95% CI is presented. A P < 0.05 was considered statistically significant for all estimates.
Results
In total, 5881/6150 (95.6%) participants were examined from 123 clusters in the two districts. Among those examined, 53.7% (n = 3158) were women and 82% (n = 4824) had no education. Nearly half of the sample (49.4%; n = 2974) lived in Adilabad district.
Current spectacles use and spectacles providers
Table 1 shows the demographic and spectacles use profile of the current spectacles users stratified by area. The proportion of people using spectacles did not vary across the age groups and gender in Adilabad and Mahbubnagar. In Adilabad, 81.7% (n = 740) of those who were using spectacles had no education as compared to 59.9% (n = 472) in Mahbubnagar. Similar differences were also found with school education and higher education (P < 0.01).
Table 1.
Spectacles use and demographic variables stratified by district
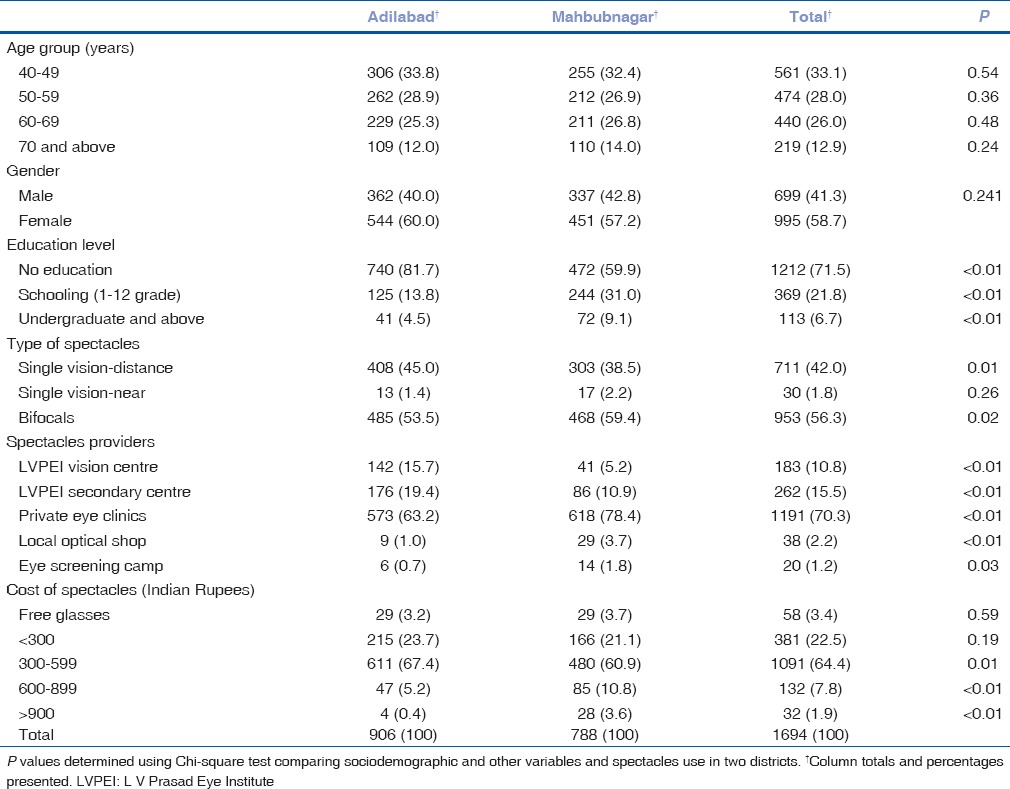
Bifocals were the most commonly used type of spectacles in both districts; however, this proportion was higher in Mahbubnagar (59.4%) as compared to Adilabad (53.5%) (P = 0.02). Overall, private eye clinics were the leading service providers of spectacles; this proportion was higher in Mahbubnagar (78.4%) as compared to Adilabad (63.2%) (P < 0.01). A higher proportion of people took their spectacles from LVPEI secondary centres (P < 0.01) and vision centres (P < 0.01) in Adilabad compared to Mahbubnagar. About two-thirds (64.4%) of the current spectacles users paid Rs. 300 to Rs. 599 for their spectacles in both regions. While the proportion of people who got spectacles for free and paid < Rs. 300 did not vary between the two regions, a higher proportion of people paid Rs. 300–500 in Adilabad compared to Mahbubnagar (67.4% vs. 60.9%; P < 0.01) [Table 1].
Current spectacles use and associations
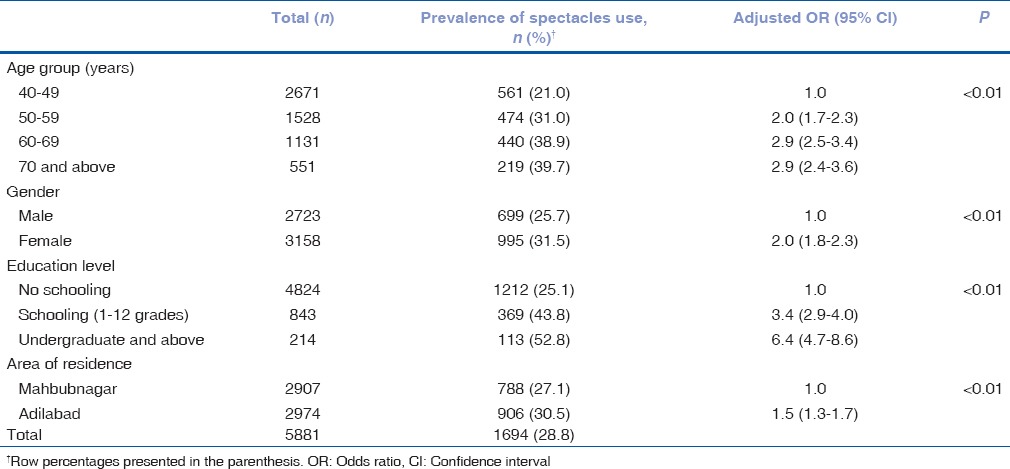
The prevalence of current spectacles use was 28.8% (95% CI: 27.6–30.0; n = 1694). The prevalence varied across the age groups (P < 0.01) and was higher among women (P < 0.01) and among those with higher levels of education (P < 0.01). The prevalence of current spectacles use was also significantly higher in Adilabad district (30.5%; 95% CI: 28.8–32.1) compared to Mahbubnagar (27.1%; 95% CI: 25.5–28.8) (P = 0.004).
The effect of demographic variables on spectacles use was assessed using multiple logistic analysis [Table 2]. The odds of using spectacles were higher in the older age groups. When compared to those aged 40–49 years, those aged 50–59 years had double the odds (OR: 2.0; 95% CI: 1.7–2.3) and those aged 60 years and older had three times higher odds for the use of spectacles (OR: 2.9; 95% CI: 2.5–3.4 in 60–69 years age group and OR: 2.9; 95% CI: 2.4–3.6 among 70 years and older age group). Women were twice as likely to use spectacles compared to men (OR: 2.0; 95% CI: 1.8–2.3). When compared to participants who had no education, those who had school education (OR: 3.4; 95% CI: 2.9–4.0) and those who studied undergraduate or above had higher odds (OR: 6.4: 95% CI: 4.7–8.6) for the current use of spectacles. The present spectacles use was significantly associated with area of residence. Compared to participants from Mahbubnagar, those living in Adilabad had higher odds for spectacles use (OR: 1.5; 95% CI: 1.3–1.7) [Table 2].
Table 2.
Effect of demographic variables on the prevalence of current spectacles use (multiple logistic regression analysis)
Spectacles coverage
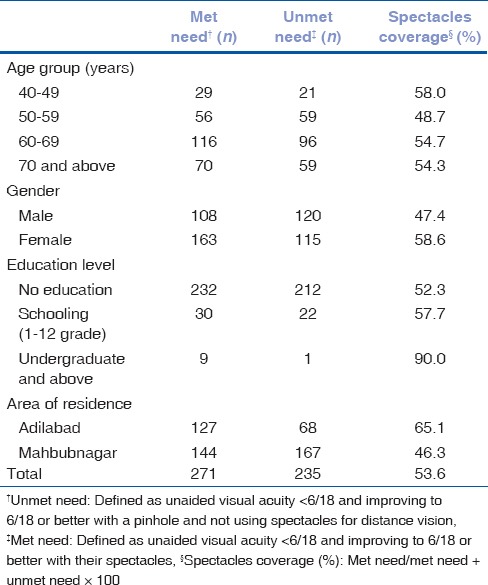
Table 3 shows the met need, unmet need, and spectacles coverage for refractive errors. The spectacles coverage was 53.6%. It was 65.1% in Adilabad and 46.3% in Mahbubnagar. Overall, the coverage for refractive errors was higher among women, those with higher levels of education, and those living in Adilabad district.
Table 3.
Spectacles coverage and sociodemographic variables
Previous spectacles use
Overall, 458 (7.8%; 95% CI: 7.1–8.5) participants reported the use of spectacles in the past. Previous spectacles use was similar in both Adilabad and Mahbubnagar districts, 7.3% (95% CI: 6.4–8.3) and 8.3% (95% CI: 7.3–9.3), respectively (P = 0.314) [Fig. 2]. “Scratched or broken spectacles” was the leading reason (47.6%; n = 218) quoted by the participants for discontinuation of spectacles; this was followed by “spectacles were for headache only and do not need to use them all the time” (27.1%; n = 124). The reasons for discontinuation of spectacles varied significantly between the districts (P = 0.02).
Figure 2.
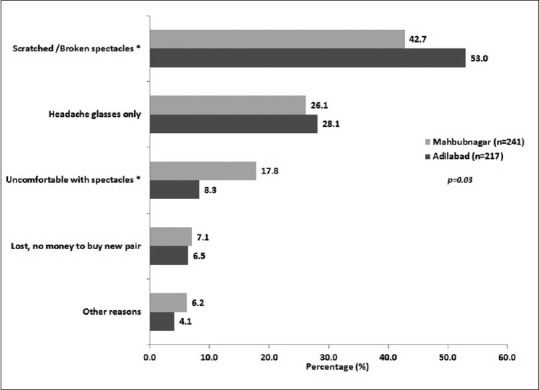
Reasons for discontinuation of spectacles in Mahbubnagar and Adilabad districts (n = 488)
Discussion
This research reported a comprehensive overview of prevalence and patterns of spectacles use from two large districts in the newly formed state of Telangana using a large representative sample with a high response rate. The Andhra Pradesh Eye Disease Study (APEDS) was the first study to report on spectacles use in South India.[16] In the APEDS, among those aged 15 years and older, the prevalence of current spectacles use was 17.1%. It was 8.2% in Mahbubnagar, 12.2% in Adilabad, and 17.1% in West Godavari district. In both, APEDS and the present study, the prevalence of current spectacles use was higher in Adilabad as compared to Mahbubnagar district. The prevalence estimates from APEDS are not directly comparable with the present study due to differences in the age groups studied and also time lapse of over one and half decades since APEDS. This higher prevalence of current spectacles use may indicate better availability and uptake of refraction services in Adilabad compared to Mahbubnagar.
Another study that was conducted in three districts Krishna (urban), Khammam (rural), and Warangal (rural) among similar age groups of 40 years and older and using a similar methodology found the prevalence of current spectacles use as 30.3% in the rural areas, which is comparable to the present study.[11] A low prevalence of spectacles use was found among fishing communities, and higher prevalence of spectacles use was found in elderly population in residential care in the state of Andhra Pradesh.[17,18] However, these are not population representative samples and they may not be directly comparable with the current study.
All three studies, the APEDS study,[16] a rapid assessment study,[11] and the current study, consistently found higher odds for spectacles use among older age groups, those with any education, and among women. These higher odds may be related to increasing visual demand due to activities such as reading among the older individuals and among those who are educated, in addition to routine household tasks that are common among women.
We found that the bifocals were the most common type of spectacles similar to an earlier study.[11] A very small proportion of people were using single vision glasses for near vision correction. It is possible that the service providers tend to prescribe bifocals even if there is no refractive error for distance. As one could assume, bifocals may need repeated visits to the service providers, once to order for the and then again to pick up the spectacles after they are made as these are not readily available. The cost in terms of time and cost of travel to the service provider for the second time could increase the overall cost for the spectacles. Dispensing of readymade single vision glasses for near could be encouraged as these are likely to be less expensive and can be dispensed on the same day. It is also possible that people tend to prefer bifocals instead single vision glasses as they need to remove them for different tasks. This needs further investigation.
Two population-based studies reported on the prevalence of previous spectacles use in Andhra Pradesh (which included Telangana).[11,16] The APEDS study reported a 9.2% prevalence of previous spectacles use.[16] It was 6.5% in Mahbubnagar, 9.9% in Adilabad, and 12.6% in West Godavari.[16] As mentioned earlier, that APEDS study included all those aged 15 years and older. Another study that had comparable age groups and methodology reported 8.7% prevalence of previous spectacles use, which is comparable to this study.[11] Although “scratched/broken” spectacles are the most common reasons for discontinuation of spectacles, over one-fourth of them reported that “spectacles are for headache only and one is not needed to wear them all the time,” in both the districts. A similar reason was also reported from APEDS study which included the two districts as this study.[16] As spectacles dispensing services are not regulated, it appears that the spectacles could have been over prescribed. There also could be a “placebo effect” where people are relieved of their headache after using these spectacles with no power or minimal power. The reason “uncomfortable with my spectacles” continues to be the important reasons across the studies, a possible reflection on quality of refraction and spectacles dispensing in these districts and calls for sustained efforts for improvement on this front.[11,16]
The private eye clinics continue as the leading service providers in both districts consistent with the earlier studies.[11,16] As reported in our previous paper, the cost of procuring spectacles would be higher if a person had to go to the nearby towns for their spectacles as private clinics are located in larger towns only.[11] About 36% and 16% of the current spectacles users in Adilabad and Mahbubnagar district, respectively, procured their spectacles from LVPEI secondary centres and vision centres. Overall, one out of every four current spectacles users procured their spectacles either from vision centres or secondary centres compared to smaller number in earlier studies.[11] This is a healthy trend given that people have to pay less to procure their spectacles at these centres. The comprehensive eye examination including intraocular pressure measurement is conducted in these centres that provide opportunistic screening for other serious eye conditions, unlike local optical shops and eye camps. Moreover, as the vision centres are located in smaller villages, the cost of procuring the spectacles might have been lower. The cost savings of the vision centre model and the satisfaction of the users of the facility have been reported.[19,20,21] A widespread replication of this model may be the way forward to reach out to larger populations in rural areas.
Spectacles coverage is one of the important impact indicators for primary eye care programs and has been widely reported from the population-based studies ranging from 21.1% in Los Angeles Latinos Eye Study[22] to 66% in Iran.[23] It was 40.5% in Bangladesh.[24] However, due to the difference in age groups studied, the definitions used, the results cannot be directly compared. A recent study from Andhra Pradesh (that included Telangana) reported 38% spectacles coverage for refractive errors compared to 54% in the present study.[11] This higher spectacles coverage can be attributed to an increase in reach as well as quality of refraction services in the region which implies that more and more people are having their “need” for spectacles met; in other words, more people with significant refractive errors are being corrected now. It is interesting to note higher spectacles coverage despite a similar prevalence of spectacles use.[11] We have earlier reported that the prevalence of spectacles use does not directly relate to spectacles coverage.[11]
This is the first study to report on the amount paid for procuring spectacles which indicate the actual willingness of people to pay for spectacles. Overall, 80% of those who are using spectacles now paid < Rs. 600 (equivalent to 10 US$) which is approximately equal to 2–3 days of wages in this region. This does not include indirect expenses which may be higher if a person was to purchase spectacles in private clinics which are typically available in towns instead of local vision centres. This information can be used as a “bench” mark to set up a pricing system for spectacles in the region.
We reported on prevalence and patterns of spectacles use from a large population representative sample with a good response rate and hence can be generalized to the two districts of Adilabad and Mahbubnagar. The information on spectacles use was collected from the participants but not verified through retinoscopy and lensometry which could be a limitation in the study. In conclusion, the study revealed good spectacles coverage in the two districts studies which can be improved further to reach the goal of elimination of refractive errors as a cause of visual impairment in this region.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Bourne RR, Stevens GA, White RA, Smith JL, Flaxman SR, Price H, et al. Causes of vision loss worldwide, 1990-2010: A systematic analysis. Lancet Glob Health. 2013;1:e339–49. doi: 10.1016/S2214-109X(13)70113-X. [DOI] [PubMed] [Google Scholar]
- 2.Resnikoff S, Kocur I, Etya'ale DE, Ukety TO. Vision 2020 – The right to sight. Ann Trop Med Parasitol. 2008;102(Suppl 1):3–5. doi: 10.1179/136485908X337409. [DOI] [PubMed] [Google Scholar]
- 3.Rao GN. VISION 2020. The right to sight. Indian J Ophthalmol. 2000;48:3. [PubMed] [Google Scholar]
- 4.Dandona L, Dandona R, Srinivas M, Giridhar P, Vilas K, Prasad MN, et al. Blindness in the Indian state of Andhra Pradesh. Invest Ophthalmol Vis Sci. 2001;42:908–16. [PubMed] [Google Scholar]
- 5.Dandona R, Dandona L, Srinivas M, Giridhar P, Prasad MN, Vilas K, et al. Moderate visual impairment in India: The Andhra Pradesh Eye Disease Study. Br J Ophthalmol. 2002;86:373–7. doi: 10.1136/bjo.86.4.373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Marmamula S, Khanna RC, Shekhar K, Rao GN. A population-based cross-sectional study of barriers to uptake of eye care services in South India: The Rapid Assessment of Visual Impairment (RAVI) project. BMJ Open. 2014;4:e005125. doi: 10.1136/bmjopen-2014-005125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Marmamula S, Keeffe JE, Raman U, Rao GN. Population-based cross-sectional study of barriers to utilisation of refraction services in South India: Rapid Assessment of Refractive Errors (RARE) Study. BMJ Open. 2011;1:e000172. doi: 10.1136/bmjopen-2011-000172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rao GN. An infrastructure model for the implementation of VISION 2020: The right to sight. Can J Ophthalmol. 2004;39:589. doi: 10.1016/s0008-4182(04)80023-1. [DOI] [PubMed] [Google Scholar]
- 9.Rao GN. The Barrie Jones Lecture-Eye care for the neglected population: Challenges and solutions. Eye (Lond) 2015;29:30–45. doi: 10.1038/eye.2014.239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rao GN, Khanna RC, Athota SM, Rajshekar V, Rani PK. Integrated model of primary and secondary eye care for underserved rural areas: The L V Prasad Eye Institute experience. Indian J Ophthalmol. 2012;60:396–400. doi: 10.4103/0301-4738.100533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Marmamula S, Khanna RC, Narsaiah S, Shekhar K, Rao GN. Prevalence of spectacles use in Andhra Pradesh, India: Rapid Assessment of Visual Impairment project. Clin Exp Ophthalmol. 2014;42:227–34. doi: 10.1111/ceo.12160. [DOI] [PubMed] [Google Scholar]
- 12.Marmamula S, Khanna RC, Kunkunu E, Rao GN. Population-based assessment of prevalence and causes of visual impairment in the state of Telangana, India: A cross-sectional study using the Rapid Assessment of Visual Impairment (RAVI) methodology. BMJ Open. 2016;6:e012617. doi: 10.1136/bmjopen-2016-012617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Marmamula S, Narsaiah S, Shekhar K, Khanna RC, Rao GN. Visual impairment in the South Indian state of Andhra Pradesh: Andhra Pradesh – Rapid Assessment of Visual Impairment (AP-RAVI) project. PLoS One. 2013;8:e70120. doi: 10.1371/journal.pone.0070120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Turner AG, Magnani RJ, Shuaib M. A not quite as quick but much cleaner alternative to the Expanded Programme on Immunization (EPI) Cluster Survey design. Int J Epidemiol. 1996;25:198–203. doi: 10.1093/ije/25.1.198. [DOI] [PubMed] [Google Scholar]
- 15.StataCorp. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP; 2011. [Google Scholar]
- 16.Dandona R, Dandona L, Kovai V, Giridhar P, Prasad MN, Srinivas M. Population-based study of spectacles use in Southern India. Indian J Ophthalmol. 2002;50:145–55. [PubMed] [Google Scholar]
- 17.Marmamula S, Madala SR, Rao GN. Prevalence of uncorrected refractive errors, presbyopia and spectacles coverage in marine fishing communities in South India: Rapid Assessment of Visual Impairment (RAVI) project. Ophthalmic Physiol Opt. 2012;32:149–55. doi: 10.1111/j.1475-1313.2012.00893.x. [DOI] [PubMed] [Google Scholar]
- 18.Marmamula S, Ravuri LV, Boon MY, Khanna RC. Spectacles coverage and spectacles use among elderly population in residential care in the South Indian state of Andhra Pradesh. Biomed Res Int 2013. 2013 doi: 10.1155/2013/183502. 183502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kovai V, Rao GN, Holden B. Key factors determining success of primary eye care through vision centres in rural India: Patients' perspectives. Indian J Ophthalmol. 2012;60:487–91. doi: 10.4103/0301-4738.100558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kovai V, Rao GN, Holden B, Krishnaiah S, Bhattacharya SK, Marmamulla S, et al. An estimate of patient costs and benefits of the new primary eye care model utilization through vision centres in Andhra Pradesh, India. Asia Pac J Public Health. 2010;22:426–35. doi: 10.1177/1010539510370779. [DOI] [PubMed] [Google Scholar]
- 21.Kovai V, Rao GN, Holden B, Sannapaneni K, Bhattacharya SK, Khanna R. Comparison of patient satisfaction with services of vision centres in rural areas of Andhra Pradesh, India. Indian J Ophthalmol. 2010;58:407–13. doi: 10.4103/0301-4738.67056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Varma R, Wang MY, Ying-Lai M, Donofrio J, Azen SP Los Angeles Latino Eye Study Group. The prevalence and risk indicators of uncorrected refractive error and unmet refractive need in Latinos: The Los AngelesLatino Eye Study. Invest Ophthalmol Vis Sci. 2008;49:5264–73. doi: 10.1167/iovs.08-1814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Fotouhi A, Hashemi H, Raissi B, Mohammad K. Uncorrected refractive errors and spectacles utilisation rate in Tehran: The unmet need. Br J Ophthalmol. 2006;90:534–7. doi: 10.1136/bjo.2005.088344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bourne RR, Dineen BP, Huq DM, Ali SM, Johnson GJ. Correction of refractive error in the adult population of Bangladesh: Meeting the unmet need. Invest Ophthalmol Vis Sci. 2004;45:410–7. doi: 10.1167/iovs.03-0129. [DOI] [PubMed] [Google Scholar]