

Abstract
This study has been conducted in an effort to establish more suitable and accurate scoring model we use in everyday practice. Among the specific outcome prediction models, in 1989 Parsonnet et al elaborated a method of uniform risk stratification for evaluation of the results of cardiac surgery procedures. We have tested two forms of the Parsonnet score, Initial and Modified Parsonnet score, in our patients.
In the first half of the year 2007, 145 patients were operated in Sarajevo Heart center. All operated patients in that period, have participated in this study. The overall hospital mortality was 4,13 (6 deaths). This study shows that the initial and modified Parsonnet’s scores are predictive for operative mortality in adult cardiac surgery patients.
Keywords: mortality prediction, Parsonnet score, scoring systems
INTRODUCTION
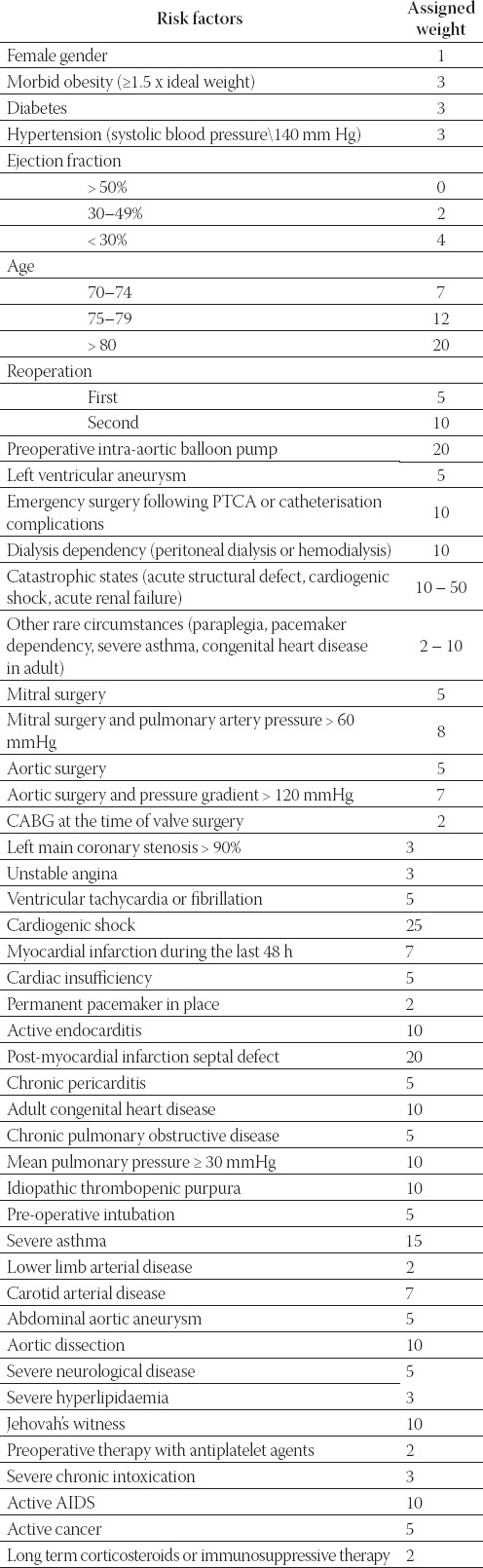
In the early 1980s, CABG (coronary artery bypass grafting) operations were characterized by operative mortality rates typically in the range of 1 to 2%, A few years later, however, the severity of illness of CABG patients began a progressive rise that is still being seen today. Predictably, CABG operative mortality rates reached the 5 to 6% range (1). This rise in operative mortality was understood by cardiovascular specialists, but others were unaware of the changes that had produced these higher mortality rates, and surgeons were challenged to justify the increase in CABG mortality. It soon became apparent that databases would be essential for proper investigation of these issues. To truly analyze patient risk factors in a meaningful way required statistical risk models designed to generate a predicted operative mortality based on preoperative clinically significant factors. In 1989, Parsonnet proposed a preoperative score for adult cardiac surgery (’’initial Parsonnet’s score’’). This score is simple, additive and grades the severity of illness of patients into five groups (Table 1, (2)). This useful score has been rapidly taken up by several cardiac surgery teams, and other authors have confirmed its predictive value on hospital mortality and morbidity (3, 4). Two risk factors of the “initial Parsonnet’s score” are however imprecise and their weights are arbitrarily chosen by the surgeon (catastrophic states, other rare circumstances, Table 1). Thus, the reliability of the initial Parsonnet’s score decreases when these 2 risk factors are present. This original score was later modified, including thirty new risk factors according to the SUMMIT system (5, 6). These 30 new risk factors take the place of the 2 imprecise risk factors of the initial score, and this new score is referred to as the “modified Parsonnet’s score” (Table 2). We wanted to assess the predictive value of the different Parsonnet’s scores and their risk in our patients (7, 8).
TABLE 1.
Initial Parsonnet score
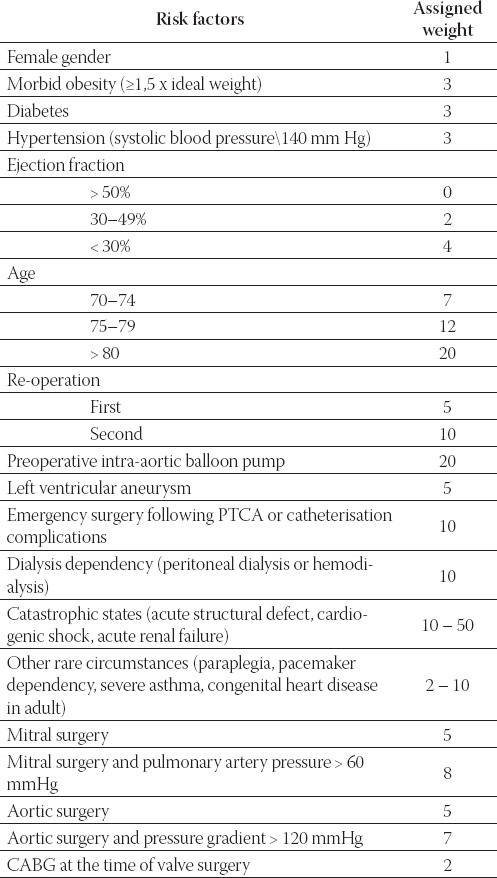
TABLE 2.
Modified Parsonnet score
MATERIALS AND METHODS
Patients
Data on 145 patients have been collected. After validation of the data, during preoperative preparation, we have bolded all patient’s co morbidities and in the same time from medical documentation as well as different examinations, that have been already performed. Afterward, collected data we putted into two Parsonnet model equitation and compared results.
Tested patients 145 (109 male age/medium 59,02±18 and 36 female age/medium 61,94 ± 20) (Graph 2, Table 3)
GRAPH 1.
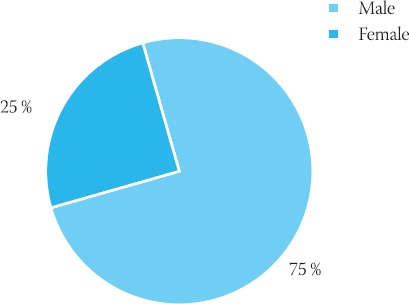
Distribution by gender
GRAPH 2.
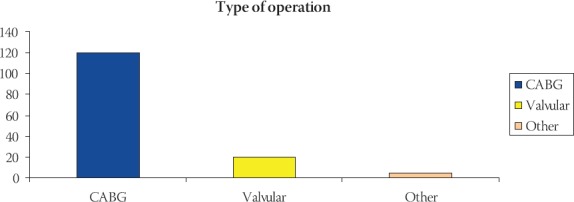
Type of the performed operations in studied group
TABLE 3.
Demographic data
TABLE 4.
Observed mortality by modified Parsonnet score

TABLE 5.
Observed mortality by initial Parsonnet score

RESULTS
This study has been conducted in the time period between January - July 2007, and it included 145 patients all of which underwent open heart surgery. The overall hospital mortality was 4,13 (6 deaths). This mortality also includes all emergency procedures. For coronary artery surgery it was 1,8, and for valvular surgery 2,1%. The two Parsonnet’s scores are predictive for operative mortality. The predictive value of the modified Parsonnet’s score is better than the initial Parsonnet’s score.
From the tables below we can realize that modified Parsonnet score create groups in the manner that low risk group contain more observed patients and that low risk and medium risk group contain 68% observed patients, meanwhile excluded mortality in large number of patients, unlike initial Parsonnet score does. The biggest group formed by initial Parsonnet score was high risk group which contain 101 patients or 69,65% observed patients. It means that initial Parsonnet score overestimate risk factors and predict high mortality in most number of patients.
DISCUSSION
Operative mortality is an easily defined, readily measured outcome, and its value to patients is undeniable. Most studies that have attempted to define effective care have focused on mortality as an outcome for the preceding reasons. For most of the history of cardiac surgery, quality generally was equated with operative mortality (i.e., outcome measure). As the new millennium got underway, a distinct change in the landscape of quality assessment occurred. The narrow focus on operative mortality gave way to a broader analysis that also included operative morbidity (9, 10).
CONCLUSION
This study shows that the initial and modified Parsonnet’s scores are predictive for operative mortality of the cardiac surgery in adults. However, these scores remain imperfect:
-many risk factors are non-significant
-the initial Parsonnet’s score has only a moderate predictive value
-use of modified Parsonnet’s score is too complex and many of its risk factors are subjective or not well defined. Establishment of a new score seems to be necessary. Ideally it has to be as predictive as the modified Parsonnet’s score and as objective and simple to use as the initial Parsonnet’s score.
REFERENCES
- 1.Ceraci JM, Johnson ML, Gordon HS, et al. Mortality after cardiacbypass surgery: Prediction from administrative versus clinical data. Med. Care. 2005;43:149. doi: 10.1097/00005650-200502000-00008. [DOI] [PubMed] [Google Scholar]
- 2.Parsonnet V, Dean D, Berstein AD. A method of uniform stratification of risk for evaluating the results of surgery in acquíred adult heart disease. Circulation. 1989;79(2):3–12. [PubMed] [Google Scholar]
- 3.Nashef S, Carey F, Silcock MM, Oomen PK, Levy RD, Jones MT. Risk stratification for open heart surgery: trial of the Parsonnet system in a British hospital. Br. Med J. 1992;305:1066–1067. doi: 10.1136/bmj.305.6861.1066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Roques F, De Vincentis C, Guibaud JP, Nashef S, Roques X, Deville C, Baudet E. Is the parsonnet system a standard for risk assesment in adult heart surgery? results of a thousand patients. EACTS Congress Barcelona September. 1993:193. Abstract Book 1993. [Google Scholar]
- 5.Clark RE. It is time for a national cardiothoracic surgical data base. Ann. Thorac. Surg. 1989;48:755–756. doi: 10.1016/0003-4975(89)90665-6. [DOI] [PubMed] [Google Scholar]
- 6.Hattler BG, Madia C, Johnson C, Armitage JM, Hardesty RL, Kormos RL, Payne DN, Griffith BP. Risk stratification using the Society of Thoracic Surgeons programme. Ann. Thorac. Surg. 1994;52:1348–1352. doi: 10.1016/0003-4975(94)91911-9. [DOI] [PubMed] [Google Scholar]
- 7.Hammermeister ICE, Burchfiel C, Jonhson R, Grover FL. Identification of patients at greatest risk for developing major complications at cardiac surgery. Circulation. 1990;82:380–389. [PubMed] [Google Scholar]
- 8.Kirklin JK, Naftel DC, Blackstone FH, Kirklin JW, Brown RC. Risk factors for mortality after primary combined valvular and coronary artery surgery. Circulation. 1989;79(6 Pt 2):185–190. [PubMed] [Google Scholar]
- 9.Scott WC, Miller DC, Haverich A, Dawkins K, Mitchell S, Jamieson SW, Oyer PE, Stinson EB, Baldwin JC, Shumway NE. Determinants of operative morality for patients undergoing aortic valve replacement. J. Thorac. Cardiovasc. Surg. 1985;89:400–413. [PubMed] [Google Scholar]
- 10.Paiement B, Pelletier C, Dyrda I, Maille JG, Boulanger M, Taillefer J, Sahab P, Delorme M, Dupont E. A simple classification of the risk in cardiac surgery. Can. Anaesth. Soc. J. 1983;30:61–68. doi: 10.1007/BF03007718. [DOI] [PubMed] [Google Scholar]