

Abstract
Background:
This research aims to evaluate the role of tamsulosin in the medical expulsion therapy for distal ureteral stones, including her effects in stone expulsion time, expulsion rates, stone size, pain episodes and analgesic dosage usage.
Material and methods:
The 104 patients with distal ureteral calculi were examined, with the size of the stones 4-10 mm. They were randomly divided into two groups: study group (n=52), received tamsulosin 0.4 mg in morning, for 28 days, analgesic (diclofenac 75 mg), high fluid intake and Control group (n=52) received analgesic (diclofenac 75 mg), high fluid intake.
Results:
There is no significant difference between groups, based on sex (P=0.835) and age (P=0.987). Average size of the stones was 6.5 mm (SD ± 1.6 mm), with no significant difference (P=0.996). Stone expulsion rate is 90.4% in the study group and 71.2% from the control group, with statistical significance (P=0.023). The average time of the expulsion of stones in the study group was 9.6 days (SD ± 7.1 days), control group 13.7 days (SD ± 7.3 days), with statistical significance, (P=0.034). Average dose of analgesics in the study group was 63.7 mg (SD ± 45.2 mg), control group is 109.2 (SD ± 53.3), with statistical significance (P=0.019).
Conclusion:
Our study reveals that tamsulosin is efficient for the treatment of distal ureteral stones. Tamsulosin decrease the number of ureteral colic episodes, by acting as a spasmolytic, increase and hasten stone expulsion rates, reduce days of stone expulsion, decrease analgesic dose usage.
Keywords: Tamsulosin, ureteral stones, expulsion therapy
1. INTRODUCTION
The minimal invasive therapies for ureteral stone are now the accepted gold standards. Many advances in endourological techniques and instrumentation have largely diverted the management of ureteral stones by open surgeries to either minimal invasive methods, like ESWL (Extracorporeal wave lithotripsy) ureterorenoscopic removal of stones, or to watchful waiting. Nevertheless, these techniques are not risk-free, are quite expensive and are not widely available in the developing countries. Minimally invasive interventional (e.g., ESWL and ureteroscopy) as well as expectant (watchful waiting) treatment exist for the management of lower ureteric calculi. But the choice of the ideal method to be taken up largely depend on the type of equipment available, type and size of stone, needs of the patient and the skills of the surgeon (1).
Recent studies have reported excellent results relating to medical expulsive therapy (MET) for distal ureteral calculi, in terms of stone expulsion and control of ureteral colic pain, using drugs (e.g., nifedipine and prednisolone) that can modulate the function of the ureter obstructed by the stone. Recently, an a1A receptor blocker to be used in this regard is tamsulosin.
Most of the work on the efficiency of tamsulosin in lower ureteral calculi expulsion has been done in affluent western countries with variable results. The disease spectrum in a developing country like ours, is different from that in developed countries, mainly because of delay in diagnosis, delay in investigations and lack of awareness which tend to modify the outcome in case of ureteral stones or of any disease for that matter. More so, advanced interventional facilities in this part of the world are not easily available. A prospective study was thus planned to compare the tamsulosin group with a control group in our setup to evaluate the efficiency of tamsulosin for lower ureteral calculi expulsion within a few days without the need for hospitalization, common endoscopic treatment or shock wave lithotripsy (1,2,3).
2. MATERIALS AND METHODS
A prospective randomized controlled study was conducted in the Department of Urology, University Clinical Centre of Kosova. The study protocol was approved by the Ethical Committee of the Faculty of Medicine, University of Prishtina, and the research was conducted in accordance with Declaration of Helsinki guidelines. Written informed consent was obtained from all study participants before inclusion in the study.
From the 104 patients, the youngest was 18 years of age, while the oldest was 65 years of age. This study included patients with a diagnosis of a symptomatic, unilateral, solitary lower ureteral stones (stone present at the level of ischial spine or below), proved either on a skiagram or sonography of the KUB (Kidney-Ureter-Bladder) with size ≥4 mm and ≤10 mm (in major axis). Prior to study, complete hemogram, blood urea, serum creatinine, complete urine examination, urine culture sensitivity, was done for participating patients.
Stone presence and its characteristics were diagnosed by kidney-ureter-bladder X-ray (KUB), abdominal ultrasonography and intravenous urography (IVU), or computed tomography when necessary. All patients with active urinary tract infection, fever, acute renal failure, chronic renal failure, history of urinary surgery or endoscopic treatment, uncorrected distal obstruction and marked hydronephrosis, diabetes, history of hypersensitivity to α-blockers and pregnant women, were excluded.
Total 104 symptomatic cases of lower ureteric stones were divided randomly into a study group I (Tamsulosin) and control group II.
Study group I (Tamsulosin): The 52 patients in this group were given Tabl. Tamsulosin 0.4 mg in the morning, half hour after breakfast for a maximum period of 28 days or until spontaneous passage of stone, (which ever was earlier). High fluid intake and analgesic (Caps. diclofenac 75 mg), were given on demand during the study period.
Group II (Control): The 52 patients included in this group were advised of high fluid intake along with analgesic (Caps diclofenac 75 mg), on demand during the study period.
The patients were followed up with a weekly sonography KUB and fortnightly X-ray KUB and final evaluation was done after completion of four weeks. Successful results were defined by complete stone passage. The failure was considered if the patient failed to pass the stone at the end of four weeks.
2.1. Statistical analysis.
Processing of date is done with the statistical package InStat 3. The obtained data has been presented through tables. The index of the structures has been calculated from the statistical parameters, arithmetical average and standard deviation. Testing of the quantitative data has been performed with X2-test, or the Fisher test. Testing of the quantitative data is done with the T-test. Verification of tests is done with degree of reliability 99.7% (P<0.01) and with reliability of 95% (P<0.005).
3. RESULTS
Our study comprised 104 patients, with the youngest patient being 18 years of age and the oldest 65 years of age. Accordingly, the average age was 35.5 years.
In the first group, there were 65.4% male, while in the second group this figure was 67.3%. With χ2-test we have not reached difference, with important statistical significance, between gender structures, according to groups (χ2=0.04, P=0.835). Based on the age-groups, biggest numbers of patients were of the age 30-39 years old, with 33.7%; then 20-29 years old, with 27.9%; 40-49 years old, with 20.2%; 50-59 years old, with 10.6%; younger than 29 years old were 6.7% and 60 and older, were 1.0%. We have reached similar structure with the distribution of cases according to groups and age-group. We have reached similar structure with the χ2-test, too, which means that we have not reached difference in statistical significance (χ2=0.334, P=0.987), (Table 1).
Table 1.
Age and sex distribution
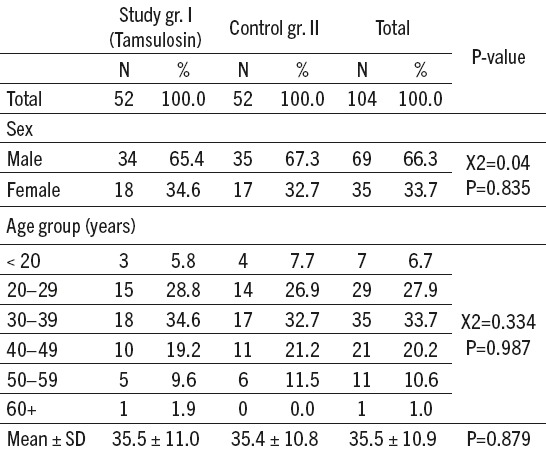
Average age of the patients included in the research was 35.5 years (SD ± 10.9 years old). Average age in the first group was 35.5 years old (SD ± 11.0), while the average age of the patients of the second group was 35.5 years old (SD ± 10.8 years old). With the T-test we have not reached difference with the important statistical significance (P>0.05), (Table 1).
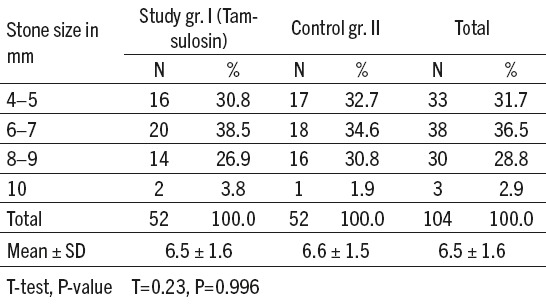
As to the size of stones, the biggest number of stones was of the size 6-7 mm, with 35.5%; then 4-5 mm, with 31.7%; 8-9 mm, with 28.8%; and 10 mm, with 2.9%. With the distribution of the cases according to groups and size of stones, we have reached similar structure (Table 2). Average size of the stones of the patients included in the research was 6.5 mm (SD ± 1.6 mm). Avarage size of the stones of the patient of the first group was 6.5 mm (SD ± 1.6 mm), whereas the average size of the stones included in the second group was 6.6mm (SD ± 1.5). With T-test we have not reached difference with important statistical significance (T=0.23, P=0.996), (Table 2).
Table 2.
Stone size distribution
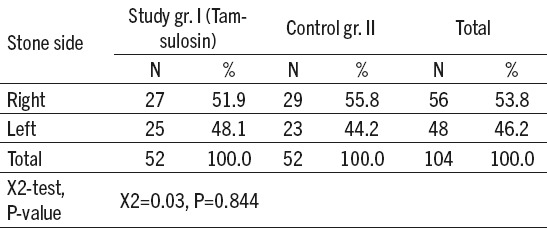
In 53.8% of the cases, stones were located on the right side and in 46.2%, in the left side. On both groups, the stones were more often localized on the right side (X²=0.03, P=0.844), (Table 3).
Table 3.
Stone side distribution by group
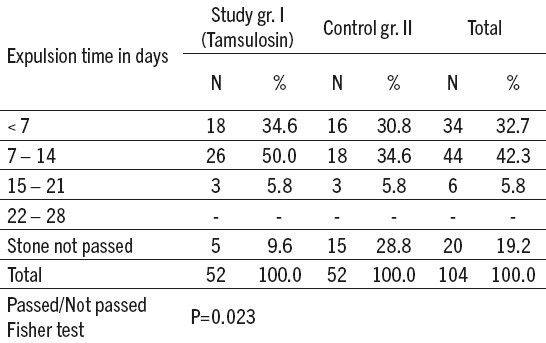
The time of expulsion of stones in less than seven days was in 32.7% of patients involved in the research; in the first group it was 34.6% and in the second group this figure was 30.8%. From 7 to 14 days, it was on the 42.3% of the patients involved in the research; in the first group 50.0% and in the second group 34.6%. The time period from 15 to 21 days was among 5.8% of the patients involved in the research; in the first group this figure was 5.8% and in the second group this figure was 5.8%; while more than 21 days we did not have any patient. A stone expulsion rate of 90.4% (47 out of 52 patients) was observed for Group I and 71.2% (37 out of 52 patients) in Group II. Group I showed a statistically significant advantage in terms of the stone expulsion rate (Fisher test, P=0.023), (Table 4).
Table 4.
Expulsion time by group
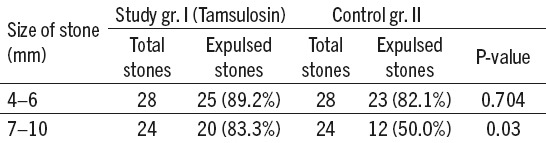
From 28 stones of the size 4-6 mm of the first group, 25 or 89.2% were expulsed, whereas from the second group this figure was 23 or 82.1%. This difference has no important statistical significance (Fisher test, P=0.704). From the 24 stones of the size 7-10 mm of the first group, 20 or 83.3% were expulsed, whereas in the second group, from 24, 12 or 50% were expulsed. This means that we have reached difference with important statistical significance (Fisher test, P=0.03), (Table 5).
Table 5.
Expulsion by stone size
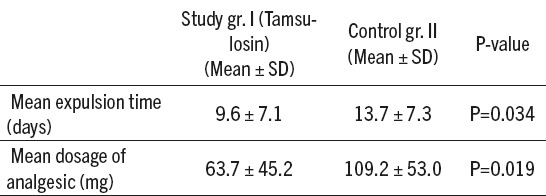
The average time of the expulsion of stones in the first group was 9.6 days (SD ± 7.1 days), and in the control group 13.7 days (SD ± 7.3 days). With T-test we have reached difference with important statistical significance, based on the timing of expulsion of stones according to groups (P=0.034). Average dose of analgesics among in the first group was 63.7 mg (SD ± 45.2 mg), control group II is 109.2 (SD ± 53.3). With T-test we have reached difference with important statistical significance among doses of analgesics used according to groups (P=0.019), (Table 6).
Table 6.
The effect of Tamsulosin on stone expulsion time and analgesic dose
4. DISCUSSION
Many minimally invasive interventional (e.g., ESWL and ureteroscopy), as well as expectant (watchful waiting) treatment, exist for the management of lower ureteric calculi. But the choice of the ideal method to be taken largely depends on the type of equipment available, type and size of stone, needs of the patient and the skills of the surgeon (3). The stone burden remains the primary factor in deciding the appropriate treatment for a patient with ureteral calculi (4). α1D receptors are found in abundance in the detrusor and the intramural part of the ureter. α1A and α1D adrenergic receptors are present more densely in the distal 1/3 of ureter (including intramural part) than other adrenergic receptors. When stimulated, they inhibit the basal tone, peristaltic wave frequency and the ureteral contractions even in the intramural part of lower ureter. α1 antagonists have a crucial impact in spontaneous painless elimination of the stones smaller than 8 mm located in the uretero-bladder junction (5).
According to Smaller, more distal and right sided stones are more likely to pass spontaneously (6). However, the expectant approach may result in complications, such as infection of the urinary tract, hydronephrosis and renal function defects (7). Spontaneous passage depends upon stone size, shape, location and associated ureteral edema (which is likely to depend on the length of time that a stone has not progressed). Ureteral calculi 4–5 mm in size have a 40–50% chance of spontaneous passage. In contrast, calculi >6 mm have less than 5% chance of spontaneous passage. Majority of stones that pass do so within a 6 weeks period after the onset of symptoms (8).
In our study we have not reached significant difference between groups, according to their gender or age. In the present study, average size of the stones of the patients included in the research was 6.5 mm (SD ± 1.6 mm). Avarage size of the stones of the patients of the first group was 6.5 mm (SD ± 1.6 mm), whereas the avarage size of the stones of patients included in the second group was 6.6mm (SD ± 1.5). With T-test we have not reached a difference with important statistical signigicance (T=0.23, P=0.996), (Table 2). In 53.8% of the cases, stones were located on the right side and in 46.2%, in the left side. In both groups, the stones were more often localized on the right side (X²=0.03, P=0.844).
Cervenakov et al, concluded that the treatment by α1 blockers considerably decreased not only lower urinary tract symptoms (LUTS) but also helped to accelerate the passing of minor calculi from the terminal parts of the ureters of 80.4% of patients. They also suggested that α1 blockers potentiate the spasm analgesic action of drugs used in standard methods of treatment (9).
Dellabella et al, used tamsulosin as a spasmolytic drug during episodes of ureteral colic due to juxta vesical calculi, observed an increased stone expulsion rate and with a decrease in stone expulsion time, the need for hospitalization and endoscopic procedures, and provided particularly good control of colic pain, the expulsion rate was 90 % (10).
In the present study, a stone expulsion rate of 90.4 % (47 out of 52 patients) was observed for Group I and 71.2% (37 out of 52 patients) in group II. Group I showed a statistically significant advantage in terms of the stone expulsion rate (Fisher test, P=0.023). The average time of the expulsion of stones in the first group was 9.6 days (SD ± 7.1 days), and in the control group 13.7 days (SD ± 7.3 days). With T-test we have reached difference with important statistically significant, based on the timing of expulsion of stones according to groups (P=0.034).
In our study, the main amount of analgesic dosage (in mg) was 63.7 mg (SD ± 45.2 mg), in group I, while the control group II is 109.2 (SD ± 53.3). With T-test we have reached difference with important statistically significant among doses of analgesics used according to groups (P=0.019).
From 28 stones of the size 4-6 mm of the first group, 25 or 89.2% were expulsed while from the second group have been 23 or 82.1%. This difference has no important statistical significance (Fisher test, P=0.704). From the 24 stones of the size 7-10 mm of the first group, 20 or 83.3% were expulsed, whereas in the second group, from 24, 12 or 50% were expulsed. This means that we have reached difference with important statistically significant (Fisher test, P= 0.03).
They may work on the obstructed ureter by inducing an increase in the intraureteral pressure gradient around the stone, that is, an increase in the urine bolus above the stone (and consequently an increase in intraureteral pressure above the stone), as well as decreased peristalsis below the ureter (and consequently a decrease in intraureteral pressure below the stone) in association with the decrease in basal and micturition pressures even at the bladder neck, thereby an increased chance of stone expulsion. Furthermore, the decreased frequency of phasic peristaltic contractions in the obstructed ureteral tract induced by tamsulosin might determine a decrease in or the absence of the algogenic stimulus (10,11,12,13).
5. CONCLUSION
Our study reveals that tamsulosin is efficient for the treatment of distal ureteral stones. The use of tamsulosin in our patients decreased the number of ureteral colic episodes and the intensity of pain during spontaneous passage at the lower ureteral calculi, increased and hastened stone expulsion rates, decreased days of stone expulsion and reduced analgesic dose usage. Tamsulosin should be considered for uncomplicated distal ureteral calculi before ureteroscopy or extracorporeal lithotripsy. Tamsulosin may have benefits of reducing the number of interventional procedures. Tamsulosin should therefore be offered as part of medical expulsive therapy, as one of the primary treatment modalities for distal ureteral stones.
Footnotes
• Conflict of interest: none declared.
REFERENCES
- 1.Lotan Y, Gettman MT, Roehrborn CG, Cadeddu JA, Pearle MS. Management of ureteral calculi: A cost comparison and decision making analysis. J Urol. 2002;167:162. [PubMed] [Google Scholar]
- 2.Russell RC, Williams NS, Bulstrode CJ. The kidneys and ureters. Bailey and Love’s Short Practice of Surgery. 4th ed. New York: Edward Arnold; 2004. pp. 1321–33. [Google Scholar]
- 3.Finlayan B, Ackermann D. Overview of surgical management of urolithiasis with special reference toLithotripsy. J Urol. 1989;141:7789. doi: 10.1016/s0022-5347(17)41008-1. [DOI] [PubMed] [Google Scholar]
- 4.Eisenberger F, Fuchs G, Miller K, et al. World J Urol. 1985;3:41. doi:10.1007/BF00326887. [Google Scholar]
- 5.Pricop C, Novac C, Negru D, Iiie C, Pricop A, Tanase A. Can selective alpha blockers help the spontaneous passage of the stones located in the uretero bladder junction. Rev Med ChirSoc Med Nat. 2004;108:128–33. [PubMed] [Google Scholar]
- 6.Ueno A, Kawamura T, Ogawa A, Takayasu H. Relation of spontaneous passage of ureteral calculi to size. Urology. 1977;10:544. doi: 10.1016/0090-4295(77)90097-8. [DOI] [PubMed] [Google Scholar]
- 7.Miller OF, Kane CJ. Time to stone passage for observed ureteral calculi: A guide for patient education. J Urol. 1999;162:688–91. doi: 10.1097/00005392-199909010-00014. [DOI] [PubMed] [Google Scholar]
- 8.Marshall LS. Urinary stones disease. In: Amend WJ Jr, Barbour S, Baskin LS, Berger TG, Bloom AL, Bretan PN Jr, et al., editors. Smith’s Urology. New York: McGraw Hill; 2004. pp. 256–90. [Google Scholar]
- 9.Cervenakov I, Fillo J, Mardiak J, Kopecny M, Smirala J, Lepies P. Speedy elimination of ureterolithiasis in lower part of ureters with the alpha 1 blockers-tamsulosin. Int J UrolNephrol. 2002:34–25. doi: 10.1023/a:1021368325512. [DOI] [PubMed] [Google Scholar]
- 10.Dellabella M, Milanese G, Muzzonigro G. Efficacy of tamsulosin in the medical management of juxtavesical ureteral stones. J Urol. 2003;170:2202–5. doi: 10.1097/01.ju.0000096050.22281.a7. [DOI] [PubMed] [Google Scholar]
- 11.Resim S, Ekerbices H, Cifti A. Effect of tamsulosin on the number and intensity of ureteral colic in patients with lower ureteral calculus. Int J Urol. 2005;12:615–20. doi: 10.1111/j.1442-2042.2005.01116.x. [DOI] [PubMed] [Google Scholar]
- 12.Kupeli B, Irkilata L, Gurocak S, Tun CL, Kirac M, Karaoglan V, et al. Does tamsulosin enhance lower ureteral stone clearance with or without shock wave lithotripsy? Urology. 2004;64:1111–5. doi: 10.1016/j.urology.2004.07.020. [DOI] [PubMed] [Google Scholar]
- 13.Prcic A, Begic E, Hiros M. Actual Contribution of Free to Total PSA Ratio in Prostate Diseases Differentiation. Med Arch. 2016;70(4):288–292. doi: 10.5455/medarh.2016.70.288-292. doi:10.5455/medarh.2016.70.288-292. [DOI] [PMC free article] [PubMed] [Google Scholar]