

Abstract
Background: Achilles tendinopathy is a common injury for active patient populations and is challenging to treat. Acupuncture tendon–based therapy was first described in the Yellow Emperor's Classic of Internal Medicine. In modern times, specific techniques have been described poorly in the literature. The aim of this case report is to describe a new technique of acupuncture for the treatment of Achilles tendinopathy and provide 2 illustrative cases.
Cases: Treatments for the 2 patients were performed in a deployed military treatment facility. SERIN® 0.25 mm × 40 mm needles placed at BL 60, BL 61, KI 3, and KI 4, with needles directed into the Achilles tendon of each patient. Needles were inserted until a firm catch of the needle entering the tendon was discerned. Energy was placed from KI 3(–) → KI 4(+) and BL61 (–) → BL 60(+) at 30 Hz for 15 minutes.
Results: Both patients reported symptomatic reduction in Achilles tendinopathy pain and functional improvement following the described treatments.
Conclusions: This case series describes two cases of successful Achilles tendinopathy therapy using direct tendon needle insertion with electrostimulation. This novel technique may provide an effective adjunct to traditional therapies in the treatment of Achilles tendinopathy.
Keywords: : Achilles, Tendinopathy, Acupuncture, Electrostimulation, Electroacupuncture, Military
Introduction
Achilles tendinopathy is a common occurrence, with an estimated incidence of 5.6% in the general population and up to 9% in active runners.1 Achilles tendinopathy can be divided into two main categories: (1) midsubstance (area superior to the myotendinous junction) versus (2) insertional (myotendinous junction to the insertion on the calcaneus). Therapeutic interventions are guided by the type of tendinopathy. Midsubstance pathology is typically treated using a 12-week eccentric exercises program with an overall treatment efficacy rate of 60%–90%.2 Insertional pathology has proven to be more challenging to treat, with an effective treatment rate of only 30%. Recommended therapy consists of 4–6 weeks of pretherapy immobilization followed by an eccentric exercise program.2 While lacking significant data to support first-line use, acupuncture is a rising form of tendinopathy therapy. Within the past 7 years, studies have reported acupuncture's ability to strengthen damaged tendons by anti-inflammatory and mechanotransductor effects,3 promote cellular function,4 and increase blood flow/oxygenation to the tendon.5
The earliest record of treating the Achilles tendon with acupuncture was found in The Yellow Emperor's Classic of Internal Medicine.6 The text described use of the Hui technique, with needles placed directly into the tendon, followed by physical activity of the patient. This method has been adapted in current practice into the herringbone technique, wherein a series of 9–12 needles are placed into the distal 6 cm of the Achilles tendon. Needles are stimulated by hand every 5 minutes for a total therapy time of 30 minutes. This technique was described in a 2012 pilot study report in the Journal of the Acupuncture Association of Chartered Physiotherapists.6
The technique described in the 2 cases presented below utilizes the therapeutic effects of tendinous acupuncture described above with the addition of electrostimulation. These cases represent the care of 2 Uniformed Service members who were treated successfully while deployed oversees.
Cases
Case #1—Chronic Midsubstance Tendinopathy Post Achilles Repair
A 31-year-old male firefighter with a history of right Achilles tendon rupture, with surgical repair 1 year prior, presented with persistent Achilles tendon pain during ambulation and running, despite extensive clinic and home physical therapy. The patient underwent 3 sessions over 9 days. Electroacupuncture (EA), using needles inserted directly into the tendon was utilized for the last two treatments. Overall, his pain was reduced from a 10/10 to a 3/10. This patient's functionality was also improved, with the ability to ambulate without a limp and run with minimal discomfort. Treatments were stopped when the patient returned home from deployment. Follow-up occurred via e-mail 5 months after initial therapy. The patient reported that his pain was stable at 2–3/10, with short monthly spikes to 8–9/10. He is currently working to establish acupuncture care for himself, with the hope continuing therapy. “I was a skeptic, but after the treatment, I was able to walk without a limp. … ”—Patient #1
Details of needling
The treatments for this patient were as follows:
• First treatment—Tendinomuscular Meridian Treatment (TMM) was placed on the right Achilles tendon over the BL meridian with a red-handled 20-mm needle placed at the BL 67 Ting point to the depth of De Qi along with the SI 18 gathering point. Surface release was performed using 10 DBCtm Spring Ten needles. Needles were placed surrounding the distal 3 inches of the Achilles tendon and were removed at 12 minutes when erythema surrounding the surface-release needles had dissipated. The patient reported reduction of pain from a baseline of 10/10 to 5/10, with no pain on ambulation.
• Second and third treatments—Treatments #2 and #3 occurred at 2 days and 9 days, respectively, after treatment #1. SERIN® 0.25 mm × 40 mm needles were placed at BL 60, BL 61, KI 3, and KI 4, with the needles directed into the Achilles tendon. Needles were inserted until a firm catch of the needle entering the tendon was discerned. Energy was placed from KI 3(–) → KI 4(+) and BL 61(–) → BL 60(+) at 30 Hz for 15 minutes (Fig. 1). The patient was asked to continue the home physical therapy (stretching, towel exercises) that he had been doing, off and on, since his surgery 1 year prior.
FIG. 1.
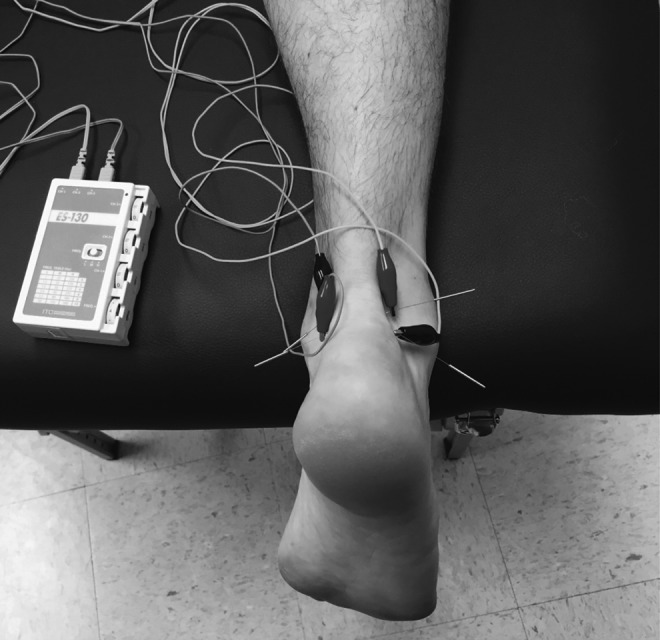
SERIN® 0.25 mm × 40 mm needles placed at BL 60, BL 61, KI 3, and KI 4 with needles directed into the Achilles tendon. Needles are inserted until a firm catch of the needle entering the tendon is discerned. Energy is placed from KI 3(–)→ KI 4(+) and BL 61(–) → BL 60(+) at 30 Hz for 12 minutes.
Results
Treatments produced progressive reduction of pain to a baseline pain level of 2–3/10. Function improved, with the patient able to return to running with minimal discomfort.
Case #2—Acute Midsubstance Achilles Tendinopathy
A 32-year-old male with a 3-week history of left Achilles tendon pain limiting daily activity presented to the clinic. This patient received two sessions of EA, using the same technique described in case #1, in addition to home physical therapy. His pain was reduced from 4/10 to 0/10, with a complete return to full activity and no pain at 2 months post-therapy. While not mentioned at his original appointment, through e-mail follow up the patient stated that his plantar fasciitis had also improved with the therapy, but he did not provide specific details. Due to the success achieved with the second and third therapies with Case #1, TMM was not utilized with the second case and treatment details are outlined below.
Details of needling
The treatments for this patient were as follows:
• First treatment—SERIN 0.25 mm × 40 mm needles were placed at BL 60, BL 61, KI 3, and KI 4, with needles directed into the Achilles tendon. Needles were inserted until a firm catch of the needle entering the tendon was discerned. Energy was placed from KI 3(–) → KI 4(+) and BL 61(–) → BL 60(+) at 30 Hz for 12 minutes. This patient reported a mild immediate reduction of pain from 4/10 to 3/10. He was provided with instructions on how to perform daily home physical therapy (stretching, towel exercises).
• Second treatment—Treatment occurred 8 days following the first therapy. This patient's interim history was notable for complete resolution of his pain until the day prior to the second treatment, when he had a reoccurrence of pain, which he rated as 1–2/10.
Results
The same treatment was repeated with complete resolution of this patient's pain.
Discussion
Achilles tendinopathy is a common musculoskeletal injury in active patient populations, such as the Military. For Military personal, a timely and effective recovery from injury is critical to mission success. This is especially important in the deployed setting, due to the complex physical demands required by the profession and the environment. These particular cases were treated while deployed overseas and working out of an Expeditionary Medical Support System canvas tent. This novel and simple treatment was highly effective, with rapid results for both acute and chronic Achilles tendinopathy and was performed easily in an austere environment. Further studies need to be performed to replicate results, establish treatment effectiveness for a more generalizable patient population, and consider the treatment effect on insertional Achilles tendinopathy.
Conclusions
This case report described 2 cases of successful Achilles tendinopathy therapy using direct tendon needle insertion with electrostimulation. This novel technique could be an effective adjunct to traditional therapies in the treatment of Achilles tendinopathy.
Author Disclosure Statement
No competing financial interests exist.
References
- 1.Li HY, Hua YH. Achilles tendinopathy: Current concepts about the basic science and clinical treatments. Biomed Res Int. 2016;2016:6492597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Childress MA, Beutler A. Management of chronic tendon injuries. Am Fam Physician. 2013;87(7):486–490 [PubMed] [Google Scholar]
- 3.Almeida M dos S, Oliveira LP, Vieira CP, Guerra F da R, Pimentel ER. Birefringence of collagen fibres in rat calcaneal tendons treated with acupuncture during three phases of healing. Acupunct Med. 2016;34(1):27–32 [DOI] [PubMed] [Google Scholar]
- 4.Speed C. Acupuncture's role in tendinopathy: New possibilities. Acupunct Med. 2015;33(1):7–8 [DOI] [PubMed] [Google Scholar]
- 5.Kubo K, Ikebukuro T, Tsunoda N, Kanehisa H. Noninvasive measures of blood volume and oxygen saturation of human Achilles tendon by red laser lights. Acta Physiol (Oxf). 2008;193(3):257–264 [DOI] [PubMed] [Google Scholar]
- 6.Kishmishian B, Selfe J, Richards J. A historical review of acupuncture to the Achilles tendon and the development of a standardized protocol for its use. J Acupunct Assoc Chartered Physiother. 2012;Spring:69–78 [Google Scholar]