

Abstract
Objective
To investigate whether sex impacts the trajectory of functional recovery following total knee arthroplasty (TKA).
Design
Retrospective analysis from a historical database containing data from three prospective clinical trials and a pilot study.
Setting
All studies were performed in a clinical laboratory setting.
Participants
Recruitment across studies was restricted to patients who underwent an elective unilateral TKA for the treatment of osteoarthritis and were between 50–85 years of age (N=301).
Intervention
Across all four studies patients received a TKA and physical therapy intervention. Measures of physical function and strength were assessed prior to TKA, 1, 3, and 6 months after TKA.
Main Outcome Measures
Statistical inference using a maximum likelihood model for repeated measures was done to estimate the changes in outcomes by sex from pre-surgical assessment compared to 1, 3, and 6 months after TKA. Muscle strength was assessed during maximal isometric quadriceps and hamstrings contractions. Muscle activation was assessed in the quadriceps muscle. Physical function outcomes included: Timed-Up-and-Go (TUG), Stair Climbing Test (SCT), and the Six-Minute Walk Test (6MWT).
Results
Women demonstrated less decline in quadriceps strength than men at 1, 3, and 6 months after TKA (p<0.04), whereas women demonstrated less decline in hamstrings strength 1 month after TKA (p<0.0001). Women demonstrated a greater decline than men on the TUG (p=0.001), SCT (p=0.004), and 6MWT (p=0.001) 1 month after TKA. Sex differences in physical function did not persist at 3 and 6 months following TKA.
Conclusions
Sex impacted early recovery of muscle and physical function within the first month after TKA. Women demonstrated better preservation of quadriceps strength, but demonstrated greater decline on measures of physical function compared to men.
Keywords: Sex Factors, Muscle Strength, Rehabilitation, Physical Function
INTRODUCTION
Osteoarthritis (OA) of the knee is a chronic disease that impacts approximately 9.3 million people in the United States,1 with the prevalence and severity being greater in women than men2,3 due to sex differences in the underlying physiological and psychosocial mechanisms of disease onset and severity. For example, in post-menopausal women the loss of ovarian hormones has been linked to impairments in knee joint function, though the exact physiologic mechanisms have yet to be discerned.4 From a psychosocial perspective, women with osteoarthritis have greater perceived disability compared to men,5 but often seek treatment later in the course of the disease.6 Thus, women and men with osteoarthritis exhibit different clinical presentations in terms of disease severity and functional limitations,7,8 which may impact the trajectory of recovery and the types of intervention strategies employed to prevent long-term disability.4 Importantly, women are at greater risk for developing disability in response to osteoarthritis due to longer duration of the osteoarthritic condition7,8 and increased life spans,3 both of which lead to an increased risk for costly institutionalization and poor quality of life.9,10
To alleviate the function-limiting symptoms associated with knee OA, 700,000 people voluntarily undergo total knee arthroplasty (TKA) annually, with ~60% (420,000) being women.11 By 2030, the number of people receiving a TKA is expected to dramatically increase 5-fold to 3.5 million per year or ~2.1 million women.11 Despite the pain relief reported following surgery, patients continue to demonstrate deficits in gait speed and stair climbing ability,12 with some evidence that women perform worse on functional outcomes compared to men.2,13–17 However, the reports on sex differences in functional outcomes following TKA are conflicting and show either no sex differences18 or that women perform worse after TKA compared to men 16–18 Quadriceps weakness in the surgical limb after TKA is a profound contributor to poor physical function. One month after TKA, quadriceps strength drops to 60% of pre-operative levels.19,20 Quadriceps weakness in the surgical limb has been associated with decreases in gait speed, balance, stair-climbing ability, and chair rise ability, as well as increased risk for falls.21–27 While, women demonstrate greater quadriceps weakness in the involved limb prior to surgery than men,2 the impact of pre-surgical quadriceps strength on the recovery of physical function and strength is unknown.
Previous studies have not explored the longitudinal trajectories of functional recovery for men and women compared to pre-surgical function and strength, specifically in the immediate post-operative period (e.g., 1 month), a time when rehabilitation interventions are likely to have the greatest impact.2,14,17,28,29 Sex differences in baseline measures of function and muscle strength have been established in OA.2 However, no studies have explored the absolute change in functional and strength measures from before to after TKA in men versus women, which may better elucidate sex-specific trajectories of recovery. A clearer understanding of the functional trajectory will guide future research designed to develop effective rehabilitation strategies that can be applied at a time post-surgery where they have the greatest impact on long-term recovery.
Therefore, the gap in knowledge of differences in the trajectory of functional recovery of men and women following TKA represents a barrier to developing sex-specific rehabilitation prescriptions that would reduce the risk for long-term disability. The purpose of this retrospective analysis was to determine the impact of sex on the longitudinal recovery (i.e., change from pre-operative to post-operative) of muscle and physical function following TKA, by pooling data from three prospective clinical trials and one pilot study.30–36 The current analyses were designed to estimate sex differences in functional recovery after TKA that would indicate the need for sex-specific tailoring of rehabilitation approaches.
METHODS
SUBJECTS
This analysis examined a historical database of patients who participated in one of three clinical trials or a pilot study spanning June 2006 to May 2015.31–33 Recruitment across all studies was restricted to patients who underwent an elective unilateral TKA for the treatment of OA and were between 50–85 years of age. Exclusion criteria in all studies included uncontrolled hypertension, uncontrolled diabetes, significant neurologic impairments, contralateral knee osteoarthritis (as defined by a pain level of greater than 4/10 with activity), the presence of other unstable lower-extremity orthopedic conditions, and a body mass index (BMI) greater than >40 kg/m2. This retrospective study on a convenience sample does not address whether the different interventions presented in each of the four studies were effective. Rather, the studies were selected and combined to answer a different question, a question regarding the trajectory of recovery and quantification of sex differences after TKA. All four studies have consistent eligibility criteria and were stratified by sex for randomization; therefore, the risk of selection bias is small.
OUTCOMES
Isometric Quadriceps and Hamstrings Muscle Strength & Quadriceps Activation
Maximal isometric hamstrings and quadriceps muscle torque of the surgical leg were assessed in all four studies as previously described31,32,36–40 at baseline (1–2 weeks before TKA), and at 1, 3, and 6 months after TKA. Patients were positioned and stabilized in the dynamometer with 60° of knee flexion. Voluntary activation of the quadriceps muscle was assessed using the doublet interpolation technique, in which a supramaximal stimulus (2-pulse, 600-μs pulse duration, 100-Hz electrical train) was applied during a maximum voluntary isometric contraction and again immediately afterwards while the quadriceps muscle was at rest.34,37–39 A value of 100% represents full voluntary muscle activation and anything less than 100% indicates incomplete motor unit recruitment or decreased motor unit discharge rates.37,38,41 Normalization of the torque from the superimposed doublet to the resting doublet allows for comparisons of quadriceps muscle activation across individuals and lower extremities. Isometric hamstrings torque was measured in 60°of knee flexion, although no activation testing was performed. Both quadriceps and hamstrings measures were performed twice, with a third trial performed if maximal torque differed by more than 5%.32 Torque data were reported as normalized to body weight.
Measures of Physical Function
Patients performed assessments of physical function at baseline (1–2 weeks before TKA), and at 1, 3, and 6 months after TKA. Measures of physical function included the Stair Climbing Test (SCT), Timed-Up-and-Go test (TUG), and Six-Minute Walk Test (6MWT). All measures were performed as previously described.30–32,36,40 Briefly, the SCT measures the total time to ascend, turn around, and descend a flight of stairs.42,43 The TUG measures the time it takes a patient to rise from an arm chair (seat height of 46 centimeters), walk 3 meters, turn, and return to sitting in the same chair without physical assistance (although assistive devices can be used if necessary).44 The 6MWT measures the total distance walked in meters in a period of 6 minutes.45
STATISTICAL ANALYSIS
Descriptive statistics were calculated for sex, age, and BMI by Study. Physical function measures (SCT, TUG, 6MWT) were described, by sex, pre-surgically and at 1, 3, and 6 months after TKA. Statistical inference was done to estimate the changes by sex in functional performance measures, muscle strength, and quadriceps muscle activation from pre-surgical values (i.e., baseline) to 1, 3, and 6 months after TKA using a maximum likelihood model for repeated measures. This method of analysis avoids case-wise deletion of records with missing data and provides unbiased estimates under the assumption that missing data are missing at random.46 The correlation structure was assumed to be autoregressive. Age and pre-surgical BMI were centered on the mean and included in all regressions. Age and BMI are considered important indicators of recovery following TKA.47 Across the four studies different interventions were administered; however indicators for Group, Study, and GroupxStudy were included in all analysis to control for differences in the interventions. For the analysis of the functional measures quadriceps and hamstrings strength values were entered as time-varying covariates because the strength loss or gain varied significantly during the stages of recovery. Differences between sexes in the change in outcomes across 1, 3, and 6 month time points compared to pre-surgical measures were estimated using linear contrasts. All analysis were done in SAS 9.3, SAS Inc., Cary, NC. A two-sided p value of 0.05 was designated for statistical significance.
RESULTS
Pre-Surgery Patient Characteristics
The combined study population (N=301; 55% females) had a mean age (±standard deviation [SD]) of 64.2±7.8 years and a mean BMI (±SD) of 30.1±4.9 kg/m2 (Table 1). Individual and combined study characteristics are shown in Table 1.
Table 1.
Population Characteristics for individual studies and the studies combined. Represented as a percent (sex) or means ±SD (age and BMI).
| Progressive Rehabilitation for TKA24,25 | Minimally Invasive TKA23,27 | Neuromuscular Electrical Stimulation21,22 | Neuromuscular Electrical Stimulation Pilot26 | Studies Combined | |
|---|---|---|---|---|---|
| Men, N (%) | 73 (45) | 22 (50) | 30 (45) | 9 (31) | 134 (45) |
| Women, N (%) | 89 (55) | 22 (50) | 36 (55) | 20 (69) | 167 (55) |
| Age, years, mean (SD) | 63.5 (7.4) | 64.3 (8.4) | 65.5 (8.5) | 65.4 (8.1) | 64.2 (7.8) |
| BMI, kg/m2, mean (SD) | 30.5 (4.8) | 30.9 (5.3) | 29.0 (5.0) | 29.0 (3.5) | 30.1 (4.9) |
Quadriceps and Hamstrings Strength & Quadriceps Activation
The unadjusted means (SD) and differences between sexes (95% confidence intervals) for surgical leg quadriceps and hamstrings strength are shown in Table 2. At 1, 3, and 6 months after TKA, women demonstrated less absolute quadriceps and hamstring strength compared to men (Table 2). The model was then adjusted for BMI, age, the baseline value of the outcome measure, Group, and Study. Adjusted means (standard error of estimate [SEE]) for the change from pre-surgical values by sex in all outcomes are shown in Table 3. Women demonstrated less decline in quadriceps strength than men at 1, 3, and 6 months after TKA (p<0.04; Table 3), whereas women demonstrated less decline in hamstrings strength at only the 1 month time point (p<0.0001; Table 3).
Table 2.
Means (SD) of outcome measures by sex at baseline and 1, 3, and 6 months post-TKA. Differences between sexes (women-men) are represented as mean difference (95% confidence intervals [CI]) at baseline and 1, 3, and 6 months post-TKA. Quads=quadriceps muscle; Hams=hamstrings muscle. N indicates the number of patients (men and women) tested on each measure at each timepoint.
| Baseline | 1 month | 3 months | 6 months | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Men | Women | Differences Women-Men (95% CI) | Men | Women | Differences Women-Men (95% CI) | Men | Women | Differences Women-Men (95% CI) | Men | Women | Differences Women-Men (95% CI) | |
| Quads Strength (N-m/kg) | 1.54 (0.51) | 1.00 (0.40) | −0.54 (−0.64, 0.43) | 0.90 (0.36) | 0.65 (0.26) | −0.24 (−0.32, −0.17)* | 1.42 (0.47) | 1.03 (0.29) | −0.39 (−0.49, −0.30)* | 1.61 (0.46) | 1.17 (0.32) | −0.44 (−0.54, −0.34)* |
| N=299 | N=283 | N=272 | N=263 | |||||||||
| Hams Strength (N-m/kg) | 0.92 (0.28) | 0.61 (0.21) | −0.30 (−0.36, −0.25)* | 0.64 (0.24) | 0.43 (0.18) | −0.21 (−0.26, −0.16)* | 0.90 (0.25) | 0.61 (0.19) | −0.29 (−0.34, −0.23)* | 0.97 (0.26) | 0.65 (0.19) | −0.33 (−0.38, −0.27)* |
| N=299 | N=281 | N=272 | N=263 | |||||||||
| Quads Activation (%) | 74.23 (15.78) | 71.88 (17.47) | −2.35 (−6.34, 1.63) | 72.46 (19.82) | 74.74 (18.12) | 2.28 (−2.53, 7.08) | 82.76 (12.14) | 83.66 (12.03) | 0.89 (−2.18, 3.96) | 82.55 (12.80) | 84.91 (9.94) | 2.37 (−0.62, 5.36) |
| N=270 | N=245 | N=242 | N=233 | |||||||||
| TUG (s) | 8.38 (2.58) | 9.54 (3.46) | 1.17 (0.47, 1.87)* | 10.43 (3.39) | 12.27 (4.94) | 1.84 (0.85, 2.83)* | 7.55 (1.90) | 8.44 (2.29) | 0.90 (0.39, 1.40)* | 7.14 (1.62) | 7.90 (2.00) | 0.75 (0.31, 1.20)* |
| N=293 | N=278 | N=270 | N=258 | |||||||||
| SCT (s) | 15.10 (7.75) | 20.94 (11.86) | 5.84 (3.58, 8.10)* | 24.65 (15.08) | 32.55 (15.64) | 7.90 (4.24, 11.55)* | 12.60 (4.62) | 16.23 (7.15) | 3.63 (2.22, 5.05)* | 11.28 (3.53) | 14.52 (6.82) | 3.24 (1.93, 4.54)* |
| N=295 | N=277 | N=272 | N=257 | |||||||||
| 6MWT (m) | 466.73 (106.11) | 430.53 (114.04) | −36.20 (−61.73, −10.66)* | 398.57 (100.41) | 341.00 (98.59) | −57.57 (−81.73, −33.41)* | 500.73 (93.04) | 454.61 (94.86) | −46.12 (−68.72, −23.52)* | 525.14 (87.51) | 481.69 (92.01) | −43.45 (−65.63, −21.26)* |
| N=289 | N=269 | N=270 | N=255 | |||||||||
Indicates confidence intervals that exclude 0.
Table 3.
Changes in outcome measures from baseline means by sex (post-operative time point-baseline) (SEE). Negative values reflect a deficit from baseline; positive values reflect an improvement from baseline. Repeated measures maximum likelihood model adjusting for:
| Change from pre-surgery to 1 month after TKA | Change from pre-surgery to 3 months after TKA | Change from pre-surgery 6 months after TKA | ||||
|---|---|---|---|---|---|---|
| Men | Women | Men | Women | Men | Women | |
| Quadriceps Strength1 (N-m/kg) | −0.65 (0.03)* | −0.35 (0.03)*† | −0.13 (0.04)* | 0.03 (0.03)† | 0.06 (0.04) | 0.16 (0.03)*† |
| Hamstrings Strength1 (N-m/kg) | −0.28 (0.02)* | −0.18 (0.02)*† | −0.03 (0.02) | 0.00 (0.02) | 0.05 (0.02) | 0.03 (0.02) |
| Quadriceps Activation1 (%) | −1.30 (1.54) | 2.12 (1.42) | 8.39 (1.72)* | 11.08 (1.59)* | 8.08 (1.77)* | 12.02 (1.64)* |
| TUG2 (s) | −0.97 (0.27)* | −2.12 (0.23)*† | 0.89 (0.26)* | 0.97 (0.24)* | 0.00 (0.27)* | 1.33 (0.25)* |
| SCT2 (s) | −6.03 (1.00)* | −9.62 (0.84)*† | 2.83 (0.96)* | 4.42 (0.86)* | 2.99 (0.97)* | 5.32 (0.89)* |
| 6MWT2 (m) | −32.90 (7.36)* | −61.20 (6.06)*† | 34.82 (7.21)* | 21.67 (6.55)* | 45.44 (7.49)* | 37.50 (6.90)* |
Baseline of respective measure, BMI, age, Sex*Month, and Study*Group
Baseline of respective measure, BMI, age, Sex*Month, Study*Group, baseline quadriceps, and baseline hamstrings
Significantly different than baseline p <0.05.
Mean change from baseline in females is significantly different from male change from baseline: p <0.05.
There were no differences between men and women in unadjusted quadriceps muscle activation prior to surgery or any time after TKA (Table 2). Following adjustment for the same variables indicated for quadriceps strength, no differences between men and women were observed in the change in quadriceps activation compared to pre-surgical levels at any time point (p>0.102; Table 3).
Functional Performance Measures
The unadjusted means and differences between sexes for measures of physical function are shown in Table 2. Unadjusted sex differences in TUG, SCT, and 6MWT were statistically significant pre-surgically and at all post-operative time points, in which women performed TUG and SCT slower and ambulated less distance on the 6MWT compared to men (p<0.05; Table 2; Figure 1).
Figure 1.
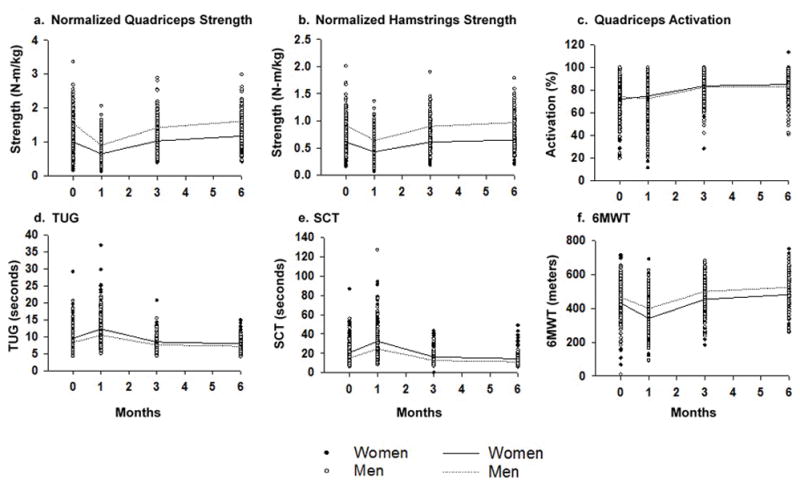
Unadjusted muscle and physical function measurements at baseline, 1, 3, and 6 months post. TKA for men and women. Measures assessed included: normalized quadriceps strength (a), normalized harmstrings strength (b), quadriceps activation (c). TUG (d) SCT (e), and 6MWT (f). Solid circles and solid lines represent women. Open circles and dotted lines represent men. Lines presented as group means.
The model was then adjusted for BMI, age, normalized pre-surgical quadriceps strength, normalized pre-surgical hamstrings strength, Group, and Study; Adjusted means (SEE) by sex for the change from pre-surgical values in all outcomes are shown in Table 3. Adjusted means (SEE) for the difference between sexes (men-women) in change from pre-surgical values are shown in Table 3. For adjusted change in TUG from prior to surgery to 1 month (men-women), women demonstrated a greater decline (1.15 [0.33] seconds slower than men) (p=0.001). Measurement of change in TUG times at 3 and 6 months compared to pre-surgical values were not statistically significant between sexes (p=0.83 and p=0.64, respectively). The adjusted change in SCT from before surgery to 1 month (men-women) showed that women demonstrated greater decline (3.59 [1.23] seconds slower than men) (p=0.004). SCT times at 3 and 6 months were not significantly different between sexes (p=0.22 and p=0.08, respectively). The adjusted change in 6MWT distance from before surgery to 1 month (men-women), revealed that women demonstrated a greater decline (28.3 [8.72] meters less than men) (p=0.001). No significant differences between men and women during the 6MWT were detected from before surgery to 3 or 6 months (p=0.18 and p=0.44, respectively).
DISCUSSION
The objective of this analysis was to determine whether sex affected the longitudinal recovery of muscle and physical function after TKA. One month following TKA, women demonstrated less decline in adjusted quadriceps and hamstrings strength compared to pre-surgical values, but performed worse on adjusted TUG, SCT, and 6MWT measures (all p < 0.05). At 3 and 6 month time points, women continued to demonstrate significantly less decline in quadriceps strength compared to men, but sex differences in physical performance and hamstrings strength were no longer apparent.
Previous examinations of sex differences after TKA for both subjective and performance measures of muscle and physical function, without a preoperative comparison, have shown conflicting results.14,15,17,18,48,49 In one study, women demonstrated greater improvement than men on Western Ontario and McMaster Universities Arthritis Index (WOMAC) function and pain scores after TKA.48 Meanwhile, several studies have shown that women score lower and improve less on the Knee Society Score (KSS) after TKA,14,16,18,50 while other investigations have indicated no sex differences in KSS.15,18,48 While many more studies have focused on subjective outcomes after TKA, far fewer have focused on performance measures of muscle and physical function that were utilized in the present analysis. A recent study by Pua et al. showed that after TKA, women demonstrate slower recovery of quadriceps strength and gait speed compared to men.49 However, the strength of the current analysis of sex differences is that we used pre-surgery measures to compare to post-operative time points. Use of change values from the pre-surgical time points adjusted for the well-established differences between sexes as a result of OA and allowed for a more complete evaluation of sex differences with respect to functional trajectories over time. Results from the current analysis indicate women demonstrate a paradoxically slower recovery of physical function during the first month after TKA, as measured by the TUG, SCT, and 6MWT, despite the fact that they experience less decline in quadriceps strength, as measured by isometric knee extensor torque. We acknowledge that, to date, minimal clinically important differences (MCID) have not been defined for TUG, SCT, and 6MWT in the TKA population, which limits our ability to state definitively the clinical significance of these results. However, in the study by Stevens-Lapsley et al., the NMES intervention demonstrated the following between group differences on functional performance from baseline to 3.5 weeks after TKA: 13.3 seconds (SCT), 2.7 seconds (TUG), and 102.4 meters (6MWT). The remaining differences between sexes, across the four combined studies, were not this large. Another explanation for the incongruent finding is that recovery of quadriceps strength and physical function occurs independently due to inherent sex differences in strength. Women demonstrate less absolute muscle strength compared to men51 and, therefore, their pre-surgical strength may be sufficiently low such that surgery does not affect greatly induce further loss compared to men(i.e., “floor effect”). Since men have greater strength before surgery, they may have more strength to lose acutely after TKA.
Numerous physiological factors may explain sex-specific differences in the recovery of muscle function 1 month after TKA. Sex differences in the adaptation of muscle’s intrinsic functionality (i.e., ability to produce force and velocity of contraction) might help explain the results of the current analysis, as men and women with advanced knee OA exhibit differences in single muscle fiber contractile properties prior to TKA compared to healthy controls.52 More specifically, in fast-twitch muscle fibers, men with knee OA showed greater single muscle fiber power output relative to women with knee OA.52 In contrast, the force-producing capacity of fast-twitch muscle fibers (both absolute and relative to fiber cross-sectional area) did not differ between men and women with knee OA, suggesting men were able to compensate for the loss of force generating capacity that occurs with OA by increasing contractile velocity to yield increased power production.52 Aside from the importance of muscle power output in determining lower extremity function in older adults,53 we have recently shown that contractile velocity in fast-twitch fibers is a strong determinant of the whole muscle rate of force development in men and women with knee OA.54 Rate of force development is a measure that we and others have shown is acutely reduced following TKA and predicts decreased function.55,56 Sex differences in myofilament adaptations could also help explain why women maintain isometric quadriceps strength compared to men after TKA. We have shown that sex differences in molecular function (i.e., slowed cross-bridge kinetics), as well as variation in single fiber power and velocity, contributed to the reduced quadriceps power.57 Thus, sex-specific adaptations of muscle myofilaments following TKA may partially explain the incongruity between recovery trajectories of muscle strength compared to physical function
Another possible account for the sex differences in recovery of muscle and physical function is altered movement patterns with functional activities, which can occur independently from recovery of muscle strength and activation. Quadriceps strength losses are pronounced at 1 month after TKA (~50–60% deficit) and are largely believed to result from neural activation deficits.31 However, sex differences in quadriceps activation were not observed in the current analysis, which is consistent with work by Petterson and colleagues also demonstrating that quadriceps activation deficits are comparable between men and women after TKA.17 Thus, differences in recovery of quadriceps strength between sexes are not explained by muscle activation deficits. However, the surgical TKA intervention imparts known changes in movement patterns and knee joint biomechanics, which have been suggested to demonstrate sex-specific patterns at one year after TKA.58 Such findings indicate neuromuscular and motor control may help account for the early (1 month) sex differences in physical function with women performing worse than men, despite the fact that women preserve more quadriceps strength early after TKA.
Non-physiological factors could also contribute to results of the current analysis. For example women, far more often than men, cite the importance of delaying surgery until they are unable to perform essential daily activities or surgical technology has advanced. 59 Women also cite more distrust with physicians who recommend and perform surgery, which impacts the timing at which they seek treatment.59 Thus, women tend to seek surgery later in the course of osteoarthritic disease because of perceptions that the surgery as “too risky” or would adversely disrupt their roles as primary caregiver for dependent spouses or other family members.59 Additionally, women are 3–4 times less likely to receive a recommendation for elective TKA compared to men,6,60,61 despite the longer duration of osteoarthritic symptoms in women and greater losses in function.6,59,60
STUDY LIMITATIONS
A limitation of this analysis is that the studied population may not be fully representative of the population of patients undergoing a TKA. The inclusion and exclusion criteria of the combined studies yielded a relatively healthy cohort of patients who had limited comorbidities and subsequent reduced risk for complications. Thus, sex differences in recovery of muscle strength and physical function after TKA may have a greater impact on the excluded, medically-complex population, who demonstrate limited mobility before surgery and are consequently at the highest risk for re-hospitalization, institutionalization, and long-term functional decline after TKA. A second limitation is the loss to follow-up, which increased over time in all four studies. It is unlikely that missingness is related to the outcomes; however, this assumption is not testable. Finally, unknown confounders may have affected the results. For example, participants who opted into the studies may present with demographic and clinical factors that are different from those who opt-out or are ineligible of research investigations.
CONCLUSION
The results of this study add greater clarification and insight into the functional trajectory of both men and women following TKA. In this cohort of patients undergoing elective TKA, sex was statistically significant in early recovery (within the first month after TKA); although these differences were not apparent during late recovery (3 and 6 months after TKA). Previous literature has shown Physical Therapy has the greatest impact within the first month after TKA. Thus, research initiatives should focus on this critical time period. In addition, developing effective rehabilitation strategies during the early post-surgical period has implications for payment reform and the commencement of bundled payments, as healthcare settings strive to decrease utilization (e.g., number of physical therapy visits), while increasing desirable outcomes (e.g., reduced long-term complications including disability and rehospitalization)62 Sex-specific approaches to rehabilitation may be necessary during the early post-operative phase as men lose significantly more strength during this time compared to women, while women demonstrate greater declines in function than men. Importantly, the discrepancy between strength loss and deficits in physical function during the 6 month recovery period in both sexes suggests that muscle activation is a crucial target for rehabilitation interventions. Improved evidence-based rehabilitation based on the physiologic and psychosocial mechanisms of functional impairment after TKA is of high importance to the healthcare field, because it has the potential to reduce the risk of long-term complications stemming from poor physical functioning and, subsequently, may decrease healthcare burden.
References
- 1.Lawrence RC, Felson DT, Helmick CG, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis and rheumatism. 2008;58(1):26–35. doi: 10.1002/art.23176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Logerstedt DS, Zeni J, Jr, Snyder-Mackler L. Sex Differences in Patients With Different Stages of Knee Osteoarthritis. Archives of physical medicine and rehabilitation. 2014 doi: 10.1016/j.apmr.2014.07.414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Weinstein AM, Rome BN, Reichmann WM, et al. Estimating the burden of total knee replacement in the United States. J Bone Joint Surg Am. 2013;95(5):385–392. doi: 10.2106/JBJS.L.00206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Stevens-Lapsley JE, Kohrt WM. Osteoarthritis in women: effects of estrogen, obesity and physical activity. Womens Health (Lond Engl) 2010;6(4):601–615. doi: 10.2217/whe.10.38. [DOI] [PubMed] [Google Scholar]
- 5.Tonelli SM, Rakel BA, Cooper NA, Angstom WL, Sluka KA. Women with knee osteoarthritis have more pain and poorer function than men, but similar physical activity prior to total knee replacement. Biol Sex Differ. 2011;2:12. doi: 10.1186/2042-6410-2-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Borkhoff CM, Hawker GA, Kreder HJ, Glazier RH, Mahomed NN, Wright JG. The effect of patients’ sex on physicians’ recommendations for total knee arthroplasty. CMAJ. 2008;178(6):681–687. doi: 10.1503/cmaj.071168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Srikanth VK, Fryer JL, Zhai G, Winzenberg TM, Hosmer D, Jones G. A meta-analysis of sex differences prevalence, incidence and severity of osteoarthritis. Osteoarthritis and cartilage/OARS, Osteoarthritis Research Society. 2005;13(9):769–781. doi: 10.1016/j.joca.2005.04.014. [DOI] [PubMed] [Google Scholar]
- 8.D’Ambrosia RD. Epidemiology of osteoarthritis. Orthopedics. 2005;28(2 Suppl):s201–205. doi: 10.3928/0147-7447-20050202-04. [DOI] [PubMed] [Google Scholar]
- 9.Murtaugh CM, Kemper P, Spillman BC. The risk of nursing home use in later life. Medical care. 1990;28(10):952–962. doi: 10.1097/00005650-199010000-00009. [DOI] [PubMed] [Google Scholar]
- 10.Crimmins EM, Hayward MD, Saito Y. Differentials in active life expectancy in the older population of the United States. J Gerontol B Psychol Sci Soc Sci. 1996;51(3):S111–120. doi: 10.1093/geronb/51b.3.s111. [DOI] [PubMed] [Google Scholar]
- 11.Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780–785. doi: 10.2106/JBJS.F.00222. [DOI] [PubMed] [Google Scholar]
- 12.Noble PC, Gordon MJ, Weiss JM, Reddix RN, Conditt MA, Mathis KB. Does total knee replacement restore normal knee function? Clin Orthop Relat Res. 2005;(431):157–165. doi: 10.1097/01.blo.0000150130.03519.fb. [DOI] [PubMed] [Google Scholar]
- 13.Singh JA, O’Byrne MM, Harmsen WS, Lewallen DG. Predictors of moderate-severe functional limitation 2 and 5 years after revision total knee arthroplasty. J Arthroplasty. 2010;25(7):1091–1095. 1095.e1091–1094. doi: 10.1016/j.arth.2009.07.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Parsley BS, Bertolusso R, Harrington M, Brekke A, Noble PC. Influence of gender on age of treatment with TKA and functional outcome. Clin Orthop Relat Res. 2010;468(7):1759–1764. doi: 10.1007/s11999-010-1348-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ritter MA, Wing JT, Berend ME, Davis KE, Meding JB. The clinical effect of gender on outcome of total knee arthroplasty. J Arthroplasty. 2008;23(3):331–336. doi: 10.1016/j.arth.2007.10.031. [DOI] [PubMed] [Google Scholar]
- 16.Dalury DF, Mason JB, Murphy JA, Adams MJ. Analysis of the outcome in male and female patients using a unisex total knee replacement system. J Bone Joint Surg Br. 2009;91(3):357–360. doi: 10.1302/0301-620X.91B3.21771. [DOI] [PubMed] [Google Scholar]
- 17.Petterson SC, Raisis L, Bodenstab A, Snyder-Mackler L. Disease-specific gender differences among total knee arthroplasty candidates. J Bone Joint Surg Am. 2007;89(11):2327–2333. doi: 10.2106/JBJS.F.01144. [DOI] [PubMed] [Google Scholar]
- 18.Pun SY, Ries MD. Effect of gender and preoperative diagnosis on results of revision total knee arthroplasty. Clin Orthop Relat Res. 2008;466(11):2701–2705. doi: 10.1007/s11999-008-0451-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mizner RL, Petterson SC, Stevens JE, Vandenborne K, Snyder-Mackler L. Early quadriceps strength loss after total knee arthroplasty. The contributions of muscle atrophy and failure of voluntary muscle activation. J Bone Joint Surg Am. 2005;87(5):1047–1053. doi: 10.2106/JBJS.D.01992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Stevens JE, Mizner RL, Snyder-Mackler L. Quadriceps strength and volitional activation before and after total knee arthroplasty for osteoarthritis. J Orthop Res. 2003;21(5):775–779. doi: 10.1016/S0736-0266(03)00052-4. [DOI] [PubMed] [Google Scholar]
- 21.Rantanen T, Guralnik JM, Izmirlian G, et al. Association of muscle strength with maximum walking speed in disabled older women. Am J Phys Med Rehabil. 1998;77(4):299–305. doi: 10.1097/00002060-199807000-00008. [DOI] [PubMed] [Google Scholar]
- 22.Skelton DA, Greig CA, Davies JM, Young A. Strength, power and related functional ability of healthy people aged 65–89 years. Age Ageing. 1994;23(5):371–377. doi: 10.1093/ageing/23.5.371. [DOI] [PubMed] [Google Scholar]
- 23.Moreland JD, Richardson JA, Goldsmith CH, Clase CM. Muscle weakness and falls in older adults: a systematic review and meta-analysis. J Am Geriatr Soc. 2004;52(7):1121–1129. doi: 10.1111/j.1532-5415.2004.52310.x. [DOI] [PubMed] [Google Scholar]
- 24.Brown M, Sinacore DR, Host HH. The relationship of strength to function in the older adult. J Gerontol A Biol Sci Med Sci. 1995;50(Spec No):55–59. doi: 10.1093/gerona/50a.special_issue.55. [DOI] [PubMed] [Google Scholar]
- 25.Connelly DM, Vandervoort AA. Effects of detraining on knee extensor strength and functional mobility in a group of elderly women. J Orthop Sports Phys Ther. 1997;26(6):340–346. doi: 10.2519/jospt.1997.26.6.340. [DOI] [PubMed] [Google Scholar]
- 26.Moxley Scarborough D, Krebs DE, Harris BA. Quadriceps muscle strength and dynamic stability in elderly persons. Gait Posture. 1999;10(1):10–20. doi: 10.1016/s0966-6362(99)00018-1. [DOI] [PubMed] [Google Scholar]
- 27.Mizner RL, Petterson SC, Snyder-Mackler L. Quadriceps strength and the time course of functional recovery after total knee arthroplasty. J Orthop Sports Phys Ther. 2005;35(7):424–436. doi: 10.2519/jospt.2005.35.7.424. [DOI] [PubMed] [Google Scholar]
- 28.Singh JA, Gabriel S, Lewallen D. The impact of gender, age, and preoperative pain severity on pain after TKA. Clin Orthop Relat Res. 2008;466(11):2717–2723. doi: 10.1007/s11999-008-0399-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bade MJ, Stevens-Lapsley JE. Restoration of physical function in patients following total knee arthroplasty: an update on rehabilitation practices. Curr Opin Rheumatol. 2012;24(2):208–214. doi: 10.1097/BOR.0b013e32834ff26d. [DOI] [PubMed] [Google Scholar]
- 30.Stevens-Lapsley JE, Balter JE, Wolfe P, et al. Relationship between intensity of quadriceps muscle neuromuscular electrical stimulation and strength recovery after total knee arthroplasty. Phys Ther. 2012;92(9):1187–1196. doi: 10.2522/ptj.20110479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Stevens-Lapsley JE, Balter JE, Wolfe P, Eckhoff DG, Kohrt WM. Early neuromuscular electrical stimulation to improve quadriceps muscle strength after total knee arthroplasty: a randomized controlled trial. Phys Ther. 2012;92(2):210–226. doi: 10.2522/ptj.20110124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Stevens-Lapsley JE, Bade MJ, Shulman BC, Kohrt WM, Dayton MR. Minimally invasive total knee arthroplasty improves early knee strength but not functional performance: a randomized controlled trial. J Arthroplasty. 2012;27(10):1812–1819. e1812. doi: 10.1016/j.arth.2012.02.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bade M, Strussel T, Dennis D, et al. High-Intensity versus Low-Intensity Rehabilitation after Total Knee Arthroplasty: A Randomized Controlled Trial. American Physical Therapy Association Combined Sections Meeting; 2016; Anaheim CA. [Google Scholar]
- 34.Loyd B, Bade M, Paxton R, et al. Poor quadriceps activation 72 hours after total knee replacement is related to poor functional performance at 1 month. American Physical Therapy Association Combined Sections Meeting; 2016; Anaheim, CA. [Google Scholar]
- 35.Stevens-Lapsley JE, Balter JE, Kohrt WM, Eckhoff DG. Quadriceps and hamstrings muscle dysfunction after total knee arthroplasty. Clin Orthop Relat Res. 2010;468(9):2460–2468. doi: 10.1007/s11999-009-1219-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Dayton MR, Bade MJ, Muratore T, Shulman BC, Kohrt WM, Stevens-Lapsley JE. Minimally invasive total knee arthroplasty: surgical implications for recovery. J Knee Surg. 2013;26(3):195–201. doi: 10.1055/s-0032-1327449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Behm DG, St-Pierre DM, Perez D. Muscle inactivation: assessment of interpolated twitch technique. J Appl Physiol (1985) 1996;81(5):2267–2273. doi: 10.1152/jappl.1996.81.5.2267. [DOI] [PubMed] [Google Scholar]
- 38.Behm D, Power K, Drinkwater E. Comparison of interpolation and central activation ratios as measures of muscle inactivation. Muscle Nerve. 2001;24(7):925–934. doi: 10.1002/mus.1090. [DOI] [PubMed] [Google Scholar]
- 39.Mintken PE, Carpenter KJ, Eckhoff D, Kohrt WM, Stevens JE. Early neuromuscular electrical stimulation to optimize quadriceps muscle function following total knee arthroplasty: a case report. J Orthop Sports Phys Ther. 2007;37(7):364–371. doi: 10.2519/jospt.2007.2541. [DOI] [PubMed] [Google Scholar]
- 40.Bade MJ, Stevens-Lapsley JE. Early high-intensity rehabilitation following total knee arthroplasty improves outcomes. J Orthop Sports Phys Ther. 2011;41(12):932–941. doi: 10.2519/jospt.2011.3734. [DOI] [PubMed] [Google Scholar]
- 41.Stevens JE, Pathare NC, Tillman SM, et al. Relative contributions of muscle activation and muscle size to plantarflexor torque during rehabilitation after immobilization. J Orthop Res. 2006;24(8):1729–1736. doi: 10.1002/jor.20153. [DOI] [PubMed] [Google Scholar]
- 42.Kennedy DM, Stratford PW, Wessel J, Gollish JD, Penney D. Assessing stability and change of four performance measures: a longitudinal study evaluating outcome following total hip and knee arthroplasty. BMC Musculoskelet Disord. 2005;6:3. doi: 10.1186/1471-2474-6-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Almeida GJ, Schroeder CA, Gil AB, Fitzgerald GK, Piva SR. Interrater reliability and validity of the stair ascend/descend test in subjects with total knee arthroplasty. Archives of physical medicine and rehabilitation. 2010;91(6):932–938. doi: 10.1016/j.apmr.2010.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi: 10.1111/j.1532-5415.1991.tb01616.x. [DOI] [PubMed] [Google Scholar]
- 45.Parent E, Moffet H. Comparative responsiveness of locomotor tests and questionnaires used to follow early recovery after total knee arthroplasty. Archives of physical medicine and rehabilitation. 2002;83(1):70–80. doi: 10.1053/apmr.2002.27337. [DOI] [PubMed] [Google Scholar]
- 46.Verbeke GMG. Linear Mixed Models in Practice: A SAS Oriented Approach. New York, NY: Springer Publishing; 1997. [Google Scholar]
- 47.Hoogeboom TJ, van Meeteren NL, Schank K, Kim RH, Miner T, Stevens-Lapsley JE. Risk factors for delayed inpatient functional recovery after total knee arthroplasty. BioMed research international. 2015;2015:167643. doi: 10.1155/2015/167643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.MacDonald SJ, Charron KD, Bourne RB, Naudie DD, McCalden RW, Rorabeck CH. The John Insall Award: gender-specific total knee replacement: prospectively collected clinical outcomes. Clin Orthop Relat Res. 2008;466(11):2612–2616. doi: 10.1007/s11999-008-0430-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Pua YH, Seah FJ, Seet FJ, Tan JW, Liaw JS, Chong HC. Sex differences and impact of body mass index on the time course of knee range-of-motion, knee strength, and gait speed after total knee arthroplasty. Arthritis Care Res (Hoboken) 2015 doi: 10.1002/acr.22584. [DOI] [PubMed] [Google Scholar]
- 50.Cherian JJ, O’Connor MI, Robinson K, Jauregui JJ, Adleberg J, Mont MA. A Prospective, Longitudinal Study of Outcomes Following Total Knee Arthroplasty Stratified by Gender. J Arthroplasty. 2015;30(8):1372–1377. doi: 10.1016/j.arth.2015.03.032. [DOI] [PubMed] [Google Scholar]
- 51.Frontera WR, Hughes VA, Lutz KJ, Evans WJ. A cross-sectional study of muscle strength and mass in 45- to 78-yr-old men and women. J Appl Physiol (1985) 1991;71(2):644–650. doi: 10.1152/jappl.1991.71.2.644. [DOI] [PubMed] [Google Scholar]
- 52.Callahan DM, Miller MS, Sweeny AP, et al. Muscle disuse alters skeletal muscle contractile function at the molecular and cellular levels in older adult humans in a sex-specific manner. J Physiol. 2014;592(Pt 20):4555–4573. doi: 10.1113/jphysiol.2014.279034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Korhonen MT, Cristea A, Alen M, et al. Aging, muscle fiber type, and contractile function in sprint-trained athletes. J Appl Physiol (1985) 2006;101(3):906–917. doi: 10.1152/japplphysiol.00299.2006. [DOI] [PubMed] [Google Scholar]
- 54.Callahan DM, Tourville TW, Slauterbeck JR, et al. Reduced rate of knee extensor torque development in older adults with knee osteoarthritis is associated with intrinsic muscle contractile deficits. Exp Gerontol. 2015;72:16–21. doi: 10.1016/j.exger.2015.08.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Maffiuletti NA, Bizzini M, Widler K, Munzinger U. Asymmetry in quadriceps rate of force development as a functional outcome measure in TKA. Clin Orthop Relat Res. 2010;468(1):191–198. doi: 10.1007/s11999-009-0978-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Winters JD, Rudolph KS. Quadriceps rate of force development affects gait and function in people with knee osteoarthritis. Eur J Appl Physiol. 2014;114(2):273–284. doi: 10.1007/s00421-013-2759-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Miller MS, Bedrin NG, Callahan DM, et al. Age-related slowing of myosin actin cross-bridge kinetics is sex specific and predicts decrements in whole skeletal muscle performance in humans. J Appl Physiol (1985) 2013;115(7):1004–1014. doi: 10.1152/japplphysiol.00563.2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Astephen Wilson JL, Dunbar MJ, Hubley-Kozey CL. Knee joint biomechanics and neuromuscular control during gait before and after total knee arthroplasty are sex-specific. J Arthroplasty. 2015;30(1):118–125. doi: 10.1016/j.arth.2014.07.028. [DOI] [PubMed] [Google Scholar]
- 59.Karlson EW, Daltroy LH, Liang MH, Eaton HE, Katz JN. Gender differences in patient preferences may underlie differential utilization of elective surgery. Am J Med. 1997;102(6):524–530. doi: 10.1016/s0002-9343(97)00050-8. [DOI] [PubMed] [Google Scholar]
- 60.Hawker GA, Wright JG, Coyte PC, et al. Differences between men and women in the rate of use of hip and knee arthroplasty. The New England journal of medicine. 2000;342(14):1016–1022. doi: 10.1056/NEJM200004063421405. [DOI] [PubMed] [Google Scholar]
- 61.Hawker GA, Wright JG, Coyte PC, et al. Determining the need for hip and knee arthroplasty: the role of clinical severity and patients’ preferences. Medical care. 2001;39(3):206–216. doi: 10.1097/00005650-200103000-00002. [DOI] [PubMed] [Google Scholar]
- 62.Services DoHaH, editor. Comprehensive Care for Joint Replacement Payment Model for Acute Care Hospitals Furnishing Lower Extremity Joint Replacement Services. 802015 [PubMed] [Google Scholar]