

Abstract
Background:
The ability to control skin blood flow decreases with advancing age and some clinical disorders, as in diabetes and in rheumatologic diseases. Feasible clinical strategies such as whole-body vibration exercise (WBVE) are being used without a clear understanding of its effects. The aim of the present study is to review the effects of the WBVE on blood flow kinetics and its feasibility in different populations.
Material and Methods:
The level of evidence (LE) of selected papers in PubMed and/or PEDRo databases was determined. We selected randomized, controlled trials in English to be evaluated.
Results:
Six studies had LE II, one had LE III-2 and one III-3 according to the NHMRC. A great variability among the protocols was observed but also in the assessment devices; therefore, more research about this topic is warranted.
Conclusion:
Despite the limitations, it is can be concluded that the use of WBVE has proven to be a safe and useful strategy to improve blood flow. However, more studies with greater methodological quality are needed to clearly define the more suitable protocols.
Keywords: blood flow, whole body vibration exercise, PubMed database, PEDRo database
Introduction
The ability to control skin blood flow decreases with advancing age (Tew et al., 2012). This fact could be due to loss of vascular tone as a consequence of the strong presence of increased production of oxygen free radicals, besides poor sympathetic vasoconstriction reflex (Camici et al., 2011; Camici et al., 2015; Holowatz et al., 2010). As a consequence, older adults would be less able to adequately thermoregulate and repair cutaneous wounds (Tew et al., 2012). In several clinical disorders, as in diabetes and in rheumatologic diseases, endothelial dysfunction occurs with an impairment of the microcirculation (Rajendram et al., 2013; Coelho et al., 2011; Widmer and Lerman 2014; Murray et al., 2004) and inhibition of blood flow restoration (Hadi et al., 2005), which may be also related to arterial stiffness (Zanoli et al., 2015). Moreover, Simmonds et al. (20130, have reported that impaired blood fluidity in humans of advanced age, includes enhanced plasma and whole blood viscosity, impaired red blood cell (RBC) deformability and enhanced RBC aggregation.
Physical activity, diet and smoking might interact with the pathways of the aging process, and to contribute to modulation of the expected changes in the cutaneous microcirculation associated with the (Tew et al., 2012). Physical activity, considered as a cornerstone in the primary and secondary disease prevention across different conditions, is a lifestyle factor related to the cutaneous microcirculation (Tew et al., 2012) which can improve circulation of blood with amelioration of the contraction in skeletal muscles, aiding supply of oxygen and ameliorating oxidative metabolism. The mechanisms underlying the increased blood flow during physical activity include (i) better adaptation of the vascular endothelial function by the likely effect of nitric oxide, (ii) excitation and signaling ATP, (iii) improve of the sympathetic reflexes (Holowatz et al., 2010; Nyberg and Hellsten 2016) and decrease of arterial stiffness (Endes et al., 2016). In order to reach these effects numerous activities (i.e. exercises that increase heart rate) have been suggested; however, some people, especially older adults or some clinical populations, are not able to easily perform these physical activities. Therefore, alternative procedures are required, and whole body vibration exercise (WBVE) has been used as a form of safe and accessible exercise for most people, and important revisions have been published (Collado-Mateo et al., 2015; Li et al., 2015; Rittweger 2010; Sá-Caputo et al., 2015). This kind of exercise is produced when mechanical vibrations generated in oscillating/vibratory platforms (OVP) are transmitted to a subject that is in contact with the base of the OVP (Rittweger 2010).
Three types of OVP can be identified (a) synchronous, the vibration is transferred to both feet synchronously, (b) alternated, in a side-alternating way, the right foot is the lowest while the left foot is the highest, and vice versa, (c) triplanar, with up and down, forward and back, and side-to-side movement of base of the platform (Rittweger 2010; Signorile 2011). The mechanical vibration produced in an OVP is a physical agent with an oscillatory motion about an equilibrium point (Rauch et al., 2010) and can be determined by biomechanical parameters: a) frequency, b) amplitude, c) the peak-to-peak displacement and d) the peak acceleration. The frequency is the number of cycles by the time, for example, by second, or Hertz (Hz). The peak-to-peak displacement is the measurement of the extension of the vibration between the lowest and the highest point in a cycle, in mm. The amplitude is the half of the peak-to-peak displacement, in mm. The peak acceleration of the mechanical vibration, which it is a combination of both frequency and amplitude, is expressed in multiples of Earth’s gravity (Rittweger 2010; Rauch et al., 2010; Cochrane 2011). Besides the biomechanical parameters, some other parameters must be also considered in the protocols related to the WBVE, such as the type of the platform, duration (work time), time of rest between bouts, periodicity of the sessions or even the position adopted by the subject in the base of the OVP (Rauch et al., 2010).
While in the elderly and in numerous clinical populations, WBVE have demonstrated improvements in numerous health outcomes including balance and gait (Ebersbach et al., 2008), walking function (Ness and Field-Fote 2009), cardiovascular fitness (Bogaerts et al., 2009), muscle strength (Gusi et al., 2006), or bone mineral density (Gusi et al., 2006), little is known about the effects on blood flow kinetics. It was reported that WBVE can acutely increase muscle blood flow (Kerschan-Schindl et al., 2001), leading to an enhancement of the mean blood velocity (Sañudo et al., 2013; Lythgo et al., 2009). It was also suggested the decrease of markers of systemic arterial stiffness (Figueroa et al., 2012). However, the characteristics of the protocols that can better enhance this outcome are largely unknown. Therefore, and considering that older adults or those with clinical disorders are not usually able to perform traditional exercises, WBVE, that have shown improvements in cardiovascular or thermoregulatory responses, could be suggested as an effective strategy to modulate blood flow with a low risk. But, it is important to verify its effects in these populations; and the aim of the current study is to review the effects of WBVE on blood flow kinetics and its feasibility in different populations.
Material and Methods
Search Strategy
Three reviewers independently accessed bibliographical databases (PubMed and/or PEDRo) through the Universidade do Estado do Rio de Janeiro on December 9th 2016 and all the publications were initially considered up to this date. The first search was performed in the PubMed database to verify the total number of publications (NP). The used keywords were (i) “whole body vibration” and “skin blood flow”, (ii) whole [Title] AND body [Title] AND vibration [Title] AND skin [Title] AND blood [Title] AND flow [Title], (iii) “whole body vibration” and “blood flow” and (iv) whole [Title] AND body [Title] AND vibration [Title] AND blood [Title] AND flow [Title]. Secondly, the keywords (i)“whole body vibration” and “skin blood flow” and (ii) “whole body vibration” and “blood flow” were searched in the database PEDRo to verify the number of publications. Personal files of the authors were also used in the searches.
Eligibility Criteria
For this review, the inclusion criteria were as follows: (a) randomized controlled trials (RCTs), (b) exercise interventions based on WBVE (c) assessment of skin blood flow, (d) clearly detailed parameters of exercise containing a description of at least frequency of the vibration and (e) to be written in English. Studies were excluded if they were based on segmental body vibration and they did not meet the minimum requirements regarding the description of training variables. In a second round, and in the absence of RCT’s, single group experimental studies were also considered (cross-over designs).
As the three reviewers carried out the searches for publications independently with the established keywords, data were independently abstracted and disagreements were discussed until a consensus was reached. Full papers were included for this narrative review if they met the search criteria and described a study using WBVE generated by an OVP used to verify the blood flow independently on the year of the publication.
Level of evidence of the selected papers
The levels of evidence (LE) included in the study were classified according to the National Health and Medical Research Councils (NHMRC, 2013) hierarchy of evidence (Table 1). Each article was assigned to a reviewer, cross-checked by a second reviewer and in case of disagreement, a third party was consulted until consensus was reached.
Table 1.
Designation* of levels of evidence according to the intervention research question (National Health and Medical Research Councils (NHMRC), Q5 2013).
| Level of Evidence (LE) | Description |
|---|---|
| I | Systematic review of level II studies |
| II | Randomized controlled trial |
| III-1 | Pseudo-randomized controlled trial (alternate allocation, as a crossover study or some other similar method) |
| III-2 | Comparative study with concurrent controls (Non-randomized experimental trial, cohort study, Case-Control study, interrupted time series with a control group). |
| III-3 | Comparative study without concurrent control (historical control. two or more single arm study, interrupted time series without a parallel control group |
| IV | Case series with either post-test or pre-test/post-test outcomes |
- adapted from NHMRC, 2013
Results
Considering the selected keywords, the literature searched in the PubMed and in PEDRo databases, twenty-three potentially relevant studies were identified. One additional study (Menéndez et al., 2016) was in the personal file of an author of this revision (Figure 1). A screening of the titles excluded fourteen articles and then the remaining 10 studies were analyzed concerning the eligibility criteria, and two of these were removed: a meta-analysis (Games et al., 2015) and a study based on segmental body vibration (Maloney-Hinds et al., 2008). Finally, eight publications with a total of 142 participants (59% male) with age ranging from 18 up to 79 years old were analyzed.
Figure 1.
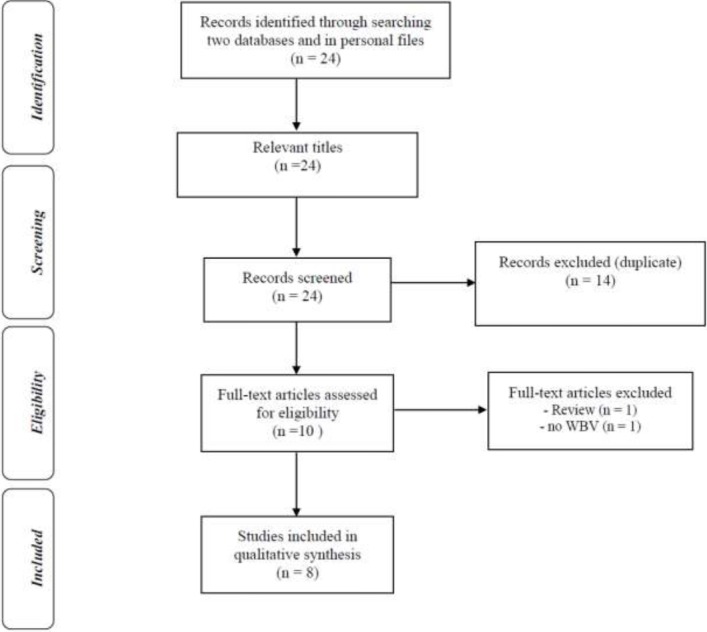
- Flow diagram indicating the steps to select the full papers analyzed in this revision using the keywords “whole body vibration” and “blood flow”.
Table 2 shows the included studies with the outcomes assessed and the main findings, and the level of evidence. The level of evidence of the studies included in this review was III-1 according to the NHMRC in six studies (Lythgo et al., 2009; Menéndez et al., 2016; Herrero et al., 2011a; Herrero et al., 2011b; Lohman et al., 2012; Johnson et al., 2014), and II in another two studies (Sañudo et al., 2013; Lohman et al., 2007). While in all studies the effects of WBV on blood flow were investigated, the populations analyzed varied (i) Johnson et al. (2014) and Sanudo et al. (2013) assessed patients with diabetes, (ii) Lohman et al., 2012 were elderly non-diabetic (iii) Herrero et al., 2011a used patients with Friedreich’s ataxia (iv) Herrero et al., 2011b and Menéndez et al., 2016 used patients with spinal cord injury and (v) Lythgo et al. (2009) and Lohman et al. (2007) used healthy adults.
Table 2.
Selected studies with the level of evidence and aim, some anthropometric characteristics with the clinical conditions of the participants, outcomes and findings.
| Study | Sample size and Population | Age (years old) | Aims | Outcomes | Findings | Level of evidence |
|---|---|---|---|---|---|---|
| Menéndez et al., 2016 | Ten SCI patients (8 males and 2 females) | 46.3±12 | To analyze the acute effects of isolated and simultaneous application of WBV and ES on popliteal artery BV and ST of the calf in subjects with SCI. | Doppler Ultrasound was used. popliteal artery was imaged, MBV and PBV velocities were determined. ST over the left gastrocnemius was measured using an infrared thermometer. | Simultaneous WBV+ES seems to produce a greater increase in MBV and PBV of the popliteal artery than the isolated (WBV or ES) or consecutive application of both stimuli. Although an increase was found only WBV. | II |
| Johnson et al., 2014 | Ten DM patients (3 males and 7 females) | 71±8 | To determine the effects of low-frequency, low-amplitude WBV on whole blood NO concentrations and SBF in individuals with symptoms of distal symmetric polyneuropathy. | Blood draws for NO analysis and laser Doppler imager scans of SBF were performed before, immediately after, and following a 5-min recovery of each of the treatments. | WBV significantly increased SBF compared to the sham condition. | II |
| Sañudo et al.,2013 | Forty T2DM (21 males and 19 females), | 67±11 | To examine the effect of a 12-week WBV training program on leg blood flow and body composition in people with T2DM. | Doppler Ultrasound was used. Femoral artery diameter, maximum systolic velocity, maximum DV, time averaged mean, pulsatility index and RI, Vmed, and peak blood velocities | Significant increases in the blood flow, Vmed, and DV after WBV compared with the control group. Within-group analysis showed significant differences in Vmed (17%), PBV (12.6%), and DV (0.7%) in the WBV | II |
| Lohman et al.,2012 | Ten elderly healthy subjects (3 females and 7 males) | From 55 up to 73 | To determine the effects of WBV (active and passive-no vibration) and/or moist heat onSBF and ST in elderly, non-diabetic individuals following short-term exposure. | SBF and skin temperature were measured using a MOOR Laser Doppler before, immediately and after 10 min of the intervention | Mean SBF increased (450%) after no WBV (passive) combined with moist heat and persisted 10 min after the intervention (379%). Significant increments in ST were also observed. | III-3 |
| Herrero et al., 2011a | Ten FA patients (7 males and 3 females) | 38.1±10 | To investigate the effects of WBV onBFV and muscular activity after vibrationprotocols in FA patients. | Femoral artery BFV was determined using an ultrasound system, VL and VM EMG, and rate of perceived exertion were registered. | PBV increased after 1, 2 and 3 min of WBV with 30 Hz, as well as the rate of perceived exertion. EMG amplitude of VL and VM was increased. | II |
| Herrero et al., 2011b | Eight SCI patients (6 males and 2 females) | 36.1±5 | To investigate the effects of WBV on muscular activity and BFV after vibration treatments in patients with SCI. | Femoral arteryBFV was registered using an ultrasound system. EMG (VL and VM) was registered at baseline and during WBV. | PBV increased after 1, 2 and 3 min of WBV with 30 Hz (with 20 Hz only after 2 and 3 min; no changes with 10 Hz). EMG increased with all frequencies. | II |
| Lythgo et al., 2009 | Nine male healthy young adult | 22±4 | To investigate the effect of WBV on legBF. | Blood draws for NO analysis and laser Doppler imager scans of SBF were performed before, immediately after, and following a 5-min recovery of each of the treatments. | Four-fold increase (33%) in MBV with 10-30 Hz and a two-fold increase (27%) in PBV with 20-30 Hz. Amplitude was additive to frequency but only achieved significance at 30 Hz. Compared with the standing condition, squatting alone produced increases in mean and PBV. | III-2 |
| Lohman et al., 2007 | Forty-five healthy subjects (22 females and 23 males). | From 18 up to 43 | To determine the effects of short-duration, high-intensity, isometric weight bearing exercise (vibration exercise [VE]) and vibration only on SBF. | SBF was measured using a laser Doppler imager at three time intervals: 1) initial base line, 2) immediately following intervention, and 3) 10-minutes following intervention. | MBV significantly increased at both post-intervention time intervals with 30 Hz. | II |
BF – Blood flow, BFV - Blood flow velocity, DM - diabetes mellitus, DV - diastolic velocity, EMG - Electromyography activity, ES – electromyostimulation, FA - Friedreich’s ataxia, MBV - meanblood velocity, NO – nitric oxide, PBV - Peak blood velocity, RI - resistance index, SBF- skin blood flow, SCI - spinal cord injury, ST – skin temperature, T2DM - type 2 diabetes mellitus, VL - vastus lateralis, VM - vastus medialis, Vmed - mean velocity, WBV- whole body vibration.
Among the devices used for the blood flow assessment in the selected studies, (a) Light stimulated emission (Laser) Doppler image scans were selected in three studies (Lohman et al., 2007; Lohman et al., 2012; Johnson et al., 2014) and (b) an ultrasound system was used in other five (Sanudo et al., 2013; Menéndez et al., 2016; Herrero et al., 2011a; Herrero et al., 2011b) and Lythgo et al. (2009). Considering the findings in general, in all the studies an improvement of the blood flow was observed due to the mechanical vibration, except in the work published by Lohman et al. (2012) that used a single session with elevated frequency (50 Hz) in elderly healthy subjects. In patients with diabetes (Johnson et al., 2014) WBV, immediately after, and following a 5-min recovery, significantly increased the skin blood flow (SBF) compared to the sham condition. When in this population a 12-week WBV training program was studied, Sañudo et al. (2013) observed significant increases in the blood flow, mean velocity (V med), and maximum diastolic velocity (DV) after WBV. Within-group analysis showed significant differences in V med, Peak blood velocity (PBV), and DV in the WBV group. The assessment of the effect of the WBVE in patients with FA (Herrero et al., 2011a) demonstrated an increment of the PBV and the mean blood velocity after 1, 2 and 3 min of WBV. In patients with SCI, Herrero et al. (2011b) also verified that PBV increased after 1, 2 and 3 min of WBV; and Menéndez et al. (2016) have also observed an increase in MBV and PBV of the popliteal artery with WBV, however these effects were better when was used simultaneously WBV and electrostimulation. Lythgo et al. (2009) reported an increase in mean blood velocity with 10-30 Hz and an increase in peak blood velocity with 20-30 Hz in healthy young adult. Lohman et al. (20120 described that WBV alone not modify the blood velocity in elderly healthy subjects. Lohman et al., 2007 observed in healthy subjects that the mean blood velocity increased due to 30 Hz WBV.
The type of the oscillating/vibratory platform, the protocol description (frequency, amplitude or peak to peak displacement, number of sessions/sets and the time of exercise/rest) and the position of the subject on the base of the platform are shown in Table 3. Two types of OVP were used in the studies, alternating and synchronous (Lohman et al., 2007; Lohman et al., 2012). The frequency used in the protocols varied from 5 up to 50 Hz and the amplitude from 2 up to 6 mm. In general, the individuals were on the base of the platform in squat position with knees bent 30 to 40° (Johnson et al., 2014), 60º (Herrero et al., 2011a; Herrero et al., 2011b), 50° (Lythgo et al., 2009) and 25°, 80°, or 100° (Lohman et al., 2007). However, in the Menéndez et al. (2016) study, the patients were seated on wheelchairs. Regarding the length of the sessions varied from a single session up 24 sessions. The working time in the sessions varied from 30 up to 180 seconds.
Table 3.
Description of the whole body vibration exercise protocols.
| Study | Type of the OVP | Frequency (Hz) | Amplitude/PPD (mm) | Position | Sessions/sets | Sets/Time series/ rest between series |
|---|---|---|---|---|---|---|
| Menéndez et al., 2016 | Not informed | 10 | PPD 5 | Seated on wheelchairs with the feet on the OVP | Single session. | 10 × 1min/1min |
| Johnson et al., 2014 | Alternating | 26 | Amplitude 2 | Squat with knees flexed 30 to 40°. | Single session. | 10 × 30 s/1min |
| Sañudo et al., 2013 | Alternating | 12-16 | PPD 4 | Eight different dynamic and static exercises (lunge, step up and down, squat, calf raises, left and right pivot, shoulder abduction with elastic bands, shoulder abduction with elastic bands while squatting, arm swinging with elastic bands | 3 sessions/wk – 12 wks. | 8 × 30-60 s / 30 s |
| Lohman et al., 2014 | Synchronous | 50 | PPD 5-6 | Subject stands supported with one foot on the vibration platform for 10 min. | Single session. | 10 bouts × 60s/ 2 s |
| Herrero Et al., 2011a | Alternating | 10-30 | PPD 5 | Subject was laid down and fixed to a tilt table with straps (60º knee flexion -0º the full knee extension). Tilt table was placed at 45º and the subject was kept in that position for a period of 10 min before the WBV. | Eight sessions in 3 wks. | 3 min continuous (constant) or fragmented (three bouts 60s exposures, separated by 60 s rests). |
| Herrero et al., 2011b | Alternating | 10-30 | PPD 5 | Same as above (Herrero et al,33) | Eight sessions in 3 wks. | 3 min continuous (constant) or fragmented (three bouts 60s exposures, separated by 60 s rests). |
| Lythgo et al., 2009 | Alternating | 5-30 | Amplitude 2.5-4.5 | Squat position (50° of knee flexion). | Single session. | 14 × 1-min and 2 × 1 min bouts where no vibration was applied. |
| Lohman et al., 2007 | Synchronous | 30 | Amplitude 5-6 | Isometric hold with Knees bent at 25°, 80° or at 100° | Single session. | 3 × 60 s (180 s). |
min – minute, PPD – peak-to-peak displacement, s – second, WBV- whole body vibration, WBVT- Whole body vibration training, wks - weeks
Discussion
The normal circulation of the blood is crucial for health and body homeostasis. Some lifestyle factors (physical activity, diet, and smoking) might contribute to modulate positively or negatively the expected changes in the cutaneous microcirculation associated with the age. In addition, in various clinical disorders, as in diabetes and in rheumatologic diseases, endothelial commitment occurs with undesirable effect of the microcirculation (Tew et al., 2012; Murray et al., 2004) and inhibition of blood flow restoration (Hadi et al., 2005). In consequence, it is desirable to assess suitable and safe strategies that would improve or to restore the blood flow. In the current study, the effects of WBVE on blood flow were reviewed.
As reported, different activities such as regular aerobic exercise and endurance training improve the arterial function decreasing the arterial stiffness (Seals et al., 2008; Liu et al., 2015). However, when the effects of vibration are considered, several mechanisms may underline the increase of blood flow observed after WBV exposure (Games et al., 2015). In a meta-analysis Games et al., 2013 suggested that metabolic, humoral, and neuronal factors would potentially play relevant roles to justify the physiological basis of the increase of the blood flow due to the WBVE. This is of importance as WBVE is known to increase the contraction in skeletal muscles and this is one of the main mechanisms to improve the blood circulation (Tew et al., 2012).
As a type of physical activity, WBVE would enhance the supply of oxygen and ameliorate the oxidative metabolism (Kang et al., 2016). In addition, vibration might reduce the viscosity of blood and thereby increase the mean speed of blood flow in the popliteal artery (Kerschan-Schindl et al., 2001) which may be of importance in many populations. The results of the review indicated that in six of the seven studies analyzed, the WBVE has improved the blood flow both in healthy people and in some clinical populations (Sañudo et al., 2013; Herrero et al., 2011a; Herrero et al., 2011b; Johnson et al., 2014), although differences between studies deserve to be analyzed.
Effects on healthy people
In healthy young people, only acute effects have been assessed. WBVE, in comparison with the standing condition, showed improvements in mean blood cell velocity (Lythgo et al., 2009; Lohman et al., 2007) and peak blood cell velocity (Sañudo et al., 2013). These effects were not observed in older adults with 50 Hz WBV (Lohman et al., 2012). Although the mechanisms by which WBVE can increase the blood flow are unclear, it would be plausible to consider two possibilities (i) the heightened muscle activity and muscle metabolic demand would result from the activation of muscle spindle reflexes (Cardinale 2005) and/or (ii) the reduction in the blood viscosity (Kerschan-Schindl et al., 2001). Another possible explanation to these results may be related to a possible decrease of the resistance in the blood vessels as it was previously reported (Sañudo et al., 2013; Lythgo et al., 2009), although this hypothesis must be tested in future studies. Despite this, it seems that these findings are not related to the type of the platform, due to Lythgo et al. (2009) have used an alternating platform while Lohman et al. (2007) and Lohman et al. (2012) have used the synchronous type. However, chronic effects on blood flow after WBVE are still unknown.
Effects on clinical populations
In patients with diabetes, increments in the blood flow speed and maximum diastolic velocity after WBV were observed (Sañudo et al., 2013; Johnson et al., 2014). Johnson et al. (2014) with a single session, also observed a significant increase in the skin blood flow. These findings are of clinical importance due to endothelial dysfunction with capillary alterations and impairment of the blood flow in this population group (Rajendran et al., 2013; Coelho et al., 2011; Widmer and Lerman 2014; Murray et al., 2004). After 12-week WBV training changes on leg blood flow were accompanied by positive changes in body composition (Sañudo et al., 2013). However, both studies used an alternating platform, thus the effects of synchronous must be contrasted.
In patients with several neuromuscular disorders, including Friedreich’s ataxia (Bourke and Keane, 2011) and those with spinal cord injury (Kam et al., 2009), cardiomyopathies can occur. WBVE have also been considered a feasible strategy to increase blood flow in patients with Friedreich’s ataxia (Herrero et al., 2011) and those with spinal cord injury (Menéndez et al., 2016; Herrero et al., 2011). Changes in Peak and mean blood flow velocity were observed after 1, 2 and 3 min of WBVE. However, these improvements seem to be dependent on the frequency used. In addition, the electromyography activity of some muscles increased due to the WBV. This would be in line with Cardinale and Wakeling (2005) that have suggested that the heightened muscle activity and muscle metabolic demand would result from the activation of muscle spindle reflexes. Therefore, these biological responses would contribute to improve the blood flow in the patients with Friedreich’s ataxia and with spinal cord injury. By contrast, as reviewed by Games et al. (2013), lower frequencies (5-25 Hz) produce a better effect on peripheral blood flow than those produced with higher frequencies (30-50 Hz).
Despite these encouraging results, the effects should be taken with caution due to the variability of the frequencies (5 up to 50 Hz) and the amplitudes (2 up to 6 mm) used in the protocols, but also the types of the platform used (alternating or synchronous). Another important aspect that should make us call into question the obtained results is the methodological quality of the studies. The level of evidence of six of the eight studies that fulfilled the inclusion criteria in this current narrative revision was II, one was III-2 and one was III-3 according to the NHMRC. This is indicative of moderate methodological study quality and therefore, this finding demonstrates the importance of further research with a higher methodological quality (RCTs).
Another aspect that should not be overlooked is the use of various devices in the analysis of the outcome variables. It is crucial to use devices that enable a reliable and valid assessment of the blood flow. In this review, studies used laser Doppler image scans (used in four of the seven articles) and the ultrasound device (used in three of the seven studies). Briefly, the image is obtained due to the fact that the observed wavelength of electromagnetic radiation is influenced by the relative motion between the source and observer, as in the case of the red blood cells in the circulation. This phenomenon is also verified with the sound/ultrasound waves in the Doppler ultrasound. These considerations indicate the relevance of the images obtained with devices with convenient laser or ultrasound after the use of procedures that might alter the blood flow, as the WBVE. In this case, the velocity of the red blood cells would be increased.
Considering the sports and the findings described in this current systematic review, it is possible to suggest that WBV exercise would be an important option of aerobic exercise to improve the performance of athletes of any sport modality due to the possibility to improve the blood flow.
The current study has several limitations that must be considered in the interpretation of the findings. Caution should be taken when generalizing the results due to the methodological variations concerning to biomechanical parameters, type of the oscillating/vibratory platform, or the variability of the protocols used. In addition, although we tried to retrieve the articles involving WBVE and blood flow with the selected keywords, it is not sure that all studies on this topic have been identified, including articles that were not published in English and articles published in journals that were not indexed in the PubMed and PEDRo databases. In addition, six of the eight of the publications had high methodological quality (RCTs) and this must also be considered due to the evidence of the findings could be affected. Therefore, studies with a higher methodological quality and focusing specifically on certain types of population would be desirable.
Despite the limitations and although the idea that WBVE is a potential strategy for the improvement of the blood flow is a bit far-fetched, and it was not well corroborated yet; it can be concluded that the use of WBVE has proven to be a safe and useful strategy to improve the blood flow. These findings may have clinical relevance and should also be considered by professionals as a therapeutic strategy. Nevertheless, methodological flaws and differences among protocols indicate the need of more research in this area.
Acknowledgments
The authors thank the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) for the support to this project.
References
- Bogaerts A.C, Delecluse C, Claessens A.L, Troosters T, Boonen S, Verschueren S.M. Effects of whole body vibration training on cardiorespiratory fitness and muscle strength in older individuals (a 1-year randomised controlled trial) Age Ageing. 2009;38:448–454. doi: 10.1093/ageing/afp067. [DOI] [PubMed] [Google Scholar]
- Bourke T, Keane D. Friedreich’s Ataxia:a review from a cardiology perspective. Ir J Med Sci. 2011;180:799–805. doi: 10.1007/s11845-011-0744-y. [DOI] [PubMed] [Google Scholar]
- Camici G.G, Savarese G, Akhmedov A, Lüscher T.F. Molecular mechanism of endothelial and vascular aging:implications for cardiovascular disease. Eur Heart J. 2015;36:3392–33403. doi: 10.1093/eurheartj/ehv587. [DOI] [PubMed] [Google Scholar]
- Camici G.G, Shi Y, Cosentino F, Francia P, Lüscher T.F. Anti-aging medicine:molecular basis for endotelial cell-targeted strategies –a mini-review. Gerontology. 2011;57:101–108. doi: 10.1159/000314227. [DOI] [PubMed] [Google Scholar]
- Cardinale M, Wakeling J. Whole body vibration exercise:are vibrations good for you? Br J Sports Med. 2005;39:585–589. doi: 10.1136/bjsm.2005.016857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cochrane D. Vibration exercise:the potential benefits. Int J Sports Med. 2011;32:75–99. doi: 10.1055/s-0030-1268010. [DOI] [PubMed] [Google Scholar]
- Coelho S, Guimaraes M, Fernandes T. Endotelium in Turner syndrome with capillaroscopy. J Vasc Bras. 2011;10:119–123. [Google Scholar]
- Collado-Mateo D, Adsuar J.C, Olivares P.R, Del Pozo-Cruz B, Parraca J.A, Del Pozo-Cruz J, Gusi N. Effects of Whole-Body Vibration Therapy in Patients with Fibromyalgia:A Systematic Literature Review. Evid Based Complement Alternat Med. 2015;2015:719082. doi: 10.1155/2015/719082. doi:10.1155/2015/719082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ebersbach G, Edler D, Kaufhold O, Wissel J. Whole body vibration versus conventional physiotherapy to improve balance and gait in Parkinson’s disease. Arch Phys Med Rehabil. 2008;89:399–403. doi: 10.1016/j.apmr.2007.09.031. [DOI] [PubMed] [Google Scholar]
- Endes S, Schaffner E, Caviezel S, Dratva J, Autenrieth C.S, Wanner M, Martin B, Stolz D, Pons M, Turk A, Bettschart R, Schindler C, Künzli N, Probst-Hensch N, Schmidt-Trucksäss A. Physical activity is associated with lower arterial stiffness in older adults:results of the SAPALDIA 3 Cohort Study. Eur J Epidemiol. 2016;31:275–285. doi: 10.1007/s10654-015-0076-8. [DOI] [PubMed] [Google Scholar]
- Figueroa A, Gil R, Wong A, Hooshmand S, Park S.Y, Vicil F, Sanchez-Gonzalez M.A. Whole-body vibration training reduces arterial stiffness, blood pressure and sympathovagal balance in young overweight/obese women. Hypertens Res. 2012;35:667–672. doi: 10.1038/hr.2012.15. [DOI] [PubMed] [Google Scholar]
- Games K.E, Sefton J.M, Wilson A.E. Whole-body vibration and blood flow and muscle oxygenation:a meta-analysis. J Athl Train. 2015;50:542–549. doi: 10.4085/1062-6050-50.2.09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gusi N, Raimundo A, Leal A. Low-frequency vibratory exercise reduces the risk of bone fracture more than walking:a randomized controlled trial. BMC Musculoskelet Disord. 2006;30:87–92. doi: 10.1186/1471-2474-7-92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hadi H.A, Carr C.S, Al Suwaidi J. Endothelial dysfunction:cardiovascular risk actors, therapy, and outcome. Vasc Health Risk Manag. 2005;1:183–98. [PMC free article] [PubMed] [Google Scholar]
- Herrero A.J, Martín J, Martín T, García-López D, Garatachea N, Jiménez B, Marín P.J. Whole-body vibration alters blood flow velocity and neuromuscular activity in Friedreich’s ataxia. Clin Physiol Funct Imaging. 2011;31:139–144. doi: 10.1111/j.1475-097X.2010.00992.x. [DOI] [PubMed] [Google Scholar]
- Herrero A.J, Menéndez H, Gil L, Martín J, Martín T, García-López D, Gil-Agudo A, Marín P.J. Effects of whole-body vibration on blood flow and neuromuscular activity in spinal cord injury. pinal Cord. 2011;49:554–559. doi: 10.1038/sc.2010.151. [DOI] [PubMed] [Google Scholar]
- Holowatz L, Thompson-Torgerson C, Kenney W. Aging and the control of human skin blood flow. Front Biosci (Landmark Ed) 2010;15:718–739. doi: 10.2741/3642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson P.K, Feland J.B, Johnson A.W, Mack G.W, Mitchell U.H. Effect of whole body vibration on skin blood flow and nitric oxide production. J Diabetes Sci Technol. 2014;8:889–994. doi: 10.1177/1932296814536289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kam A, Sankaran R, Gowda K, Linassi G, Shan R.L. Cardiomyopathy presenting as severe fatigue in a person with chronic spinal cord injury. J Spinal Cord Med. 2009;32:204–208. doi: 10.1080/10790268.2009.11760773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kang J, Bushi J.A, Ratamess N.A, Faigenbaum A.D, Klei S, Maconi D, Kreckel M. Acute effects of whole-body vibration on energy metabolism during aerobic exercise. J Sports Med Phys Fitness. 2016;56:834–842. [PubMed] [Google Scholar]
- Kerschan-Schindl K, Grampp S, Henk C, Resch H, Preisinger E, Fialka-Moser V, Imhof H. Whole-bod vibration exercise leads to alterations in muscle blood volume. Clin Physiol. 2001;21:377–382. doi: 10.1046/j.1365-2281.2001.00335.x. [DOI] [PubMed] [Google Scholar]
- Li X, Wang X.Q, Chen B.L, Huang L.Y, Liu Y. Erratum to “Whole-Body Vibration Exercise for Knee Osteoarthritis:A Systematic Review and Meta-Analysis”. Evid Based Complement Alternat Med. 2015;2015:636435. doi: 10.1155/2015/636435. doi:10.1155/2015/636435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu H.B, Yuan W.X, Qin K.R, Hou J. Acute effect of cycling intervention on carotid arterial hemodynamics:basketball athletes versus sedentary controls. Biomed Eng Online. 2015;14 doi: 10.1186/1475-925X-14-S1-S17. doi:10.1186/1475-925X-14-S1-S17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lohman E.B, Petrofsky J.S, Maloney-Hinds C, Betts-Schwab H, Thorpe D. The effect of whole body vibration on lower extremity skin blood flow in normal subjects. Med Sci Monit. 2007;13:71–76. [PubMed] [Google Scholar]
- Lohman E.B, Sackiriyas K.S, Bains G.S, Calandra G, Lobo C, Nakhro D, Malthankar G, Paul S. A comparison of whole body vibration and moist heat on lower extremity skin temperature and skin blood flow in healthy older individuals. Med Sci Monit. 2012;18:415–424. doi: 10.12659/MSM.883209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lythgo N, Eser P, de Groot P, Galea M. Whole-body vibration dosage alters leg blood flow. Clin Physiol Funct Imaging. 2009;29:53–59. doi: 10.1111/j.1475-097X.2008.00834.x. [DOI] [PubMed] [Google Scholar]
- Maloney-Hinds C, Petrofsky J, Zimmerman G. The effect of 30 Hz vs. 50 Hz passive vibration and duration of vibration on skin blood flow in the arm. Med Sci Monit. 2008;14:112–116. [PubMed] [Google Scholar]
- Menéndez H, Ferrero C, Martín-Hernández J, Figueroa A, Marín P.J, Herrero A.J. Acute effects of simultaneous electromyostimulation and vibration on leg blood flow in spinal cord injury. Spinal Cord. 2016;54:383–389. doi: 10.1038/sc.2015.181. [DOI] [PubMed] [Google Scholar]
- Murray A, Herrick A, King T. Laser Doppler imaging:a developing technique for application in the rheumatic diseases. Rheumatology (Oxford) 2004;43:1210–1218. doi: 10.1093/rheumatology/keh275. [DOI] [PubMed] [Google Scholar]
- Ness L, Field-Fote E. Whole-body vibration improves walking function in individuals with spinal cord injury:a pilot study. Gait Posture. 2009;30:436–440. doi: 10.1016/j.gaitpost.2009.06.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [Accessed January 31, 2016];NHMRC additional levels of evidence and grades for recommendations for developers of guidelines. 2013 http://www.nhmrc.gov.au/files nhmrc/file/guidelines/levels grades05.pdf .
- Nyberg M, Hellsten Y. Reduced blood flow to contracting skeletal muscle in ageing humans:is it all an effect of sand through the hourglass? J Physiol. 2016;594:2297–22305. doi: 10.1113/JP270594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rajendran P, Rengarajan T, Thangavel J, Nishigaki Y, Sakthisekaran D, Sethi G, Nishigaki I. The vascular endothelium and human diseases. Int J Biol Sci. 2013;9:1057–1069. doi: 10.7150/ijbs.7502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rauch F, Sievanen H, Boonen S, Cardinale M, Degens H, Felsenberg D, Roth J, Schoenau E, Verschueren S, Rittweger J. International Society of Musculoskeletal and Neuronal Interactions. Reporting whole-body vibration intervention studies:recommendations of the International Society of Musculoskeletal and Neuronal Interactions. J Musculoskelet Neuronal Interact. 2010;10:193–198. [PubMed] [Google Scholar]
- Rittweger J. Vibration as an exercise modality:how it may work, and what its potential might be. Eur J Appl Physiol. 2010;108:877–904. doi: 10.1007/s00421-009-1303-3. [DOI] [PubMed] [Google Scholar]
- Sá-Caputo D.C, Costa-Cavalcanti R, Carvalho-Lima R.P, Arnóbio A, Bernardo R.M, Ronikeile-Costa P, Kutter C, Giehl P.M, Asad N.R, Paiva D.N, Pereira H.V, Unger M, Marin P.J, Bernardo-Filho M. Systematic review of whole body vibration exercises in the treatment of cerebral palsy:Brief report. Dev Neurorehabil. 2015;24:1–7. doi: 10.3109/17518423.2014.994713. [DOI] [PubMed] [Google Scholar]
- Sañudo B, Alfonso-Rosa R, Del Pozo-Cruz B, Del Pozo-Cruz J, Galiano D, Figueroa A. Whole body vibration training improves leg blood flow and adiposity in patients with type 2 diabetes mellitus. Eur J Appl Physiol. 2013;113:2245–2252. doi: 10.1007/s00421-013-2654-3. [DOI] [PubMed] [Google Scholar]
- Seals D.R, Walker A.E, Pierce G.L, Lesniewski L.A. Habitual exercise and arterial aging. J Appl Physiol. 2008;105:1323–1332. doi: 10.1152/japplphysiol.90553.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Signorile J. Whole body vibration, part two:What’s the most effective protocol? Journal on active aging. 2011;68:l73. [Google Scholar]
- Simmonds M, Meiselman H, Baskurt O. Blood rheology and aging. J Geriatr Cardiol. 2013;10:291–301. doi: 10.3969/j.issn.1671-5411.2013.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tew G, Saxton J, Hodges G. Exercise training and the control of skin blood flow in older adults. J Nutr Health Aging. 2012;16:237–241. doi: 10.1007/s12603-011-0156-8. [DOI] [PubMed] [Google Scholar]
- Widmer R, Lerman A. Endothelial dysfunction and cardiovascular disease. Glob Cardiol Sci Pract. 2014;2014:291–308. doi: 10.5339/gcsp.2014.43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zanoli L, Rastelli S, Inserra G, Castellino P. Arterial structure and function in inflammatory bowel disease. World J Gastroenterol. 2015;21:11304–1111. doi: 10.3748/wjg.v21.i40.11304. [DOI] [PMC free article] [PubMed] [Google Scholar]