

Abstract
Background
Solitary plasmacytoma of the liver is a very rare and aggressive form of plasma cell dyscrasia. To the best of our knowledge, very few cases have been reported without systemic disease. We reported a rare case of hepatic solitary plasmacytoma that successfully responded to fractionated stereotactic radiotherapy.
Case presentation
A 64-year-old white French man had monoclonal gammopathy of the immune globulin G lambda type; he developed a cholestasis and cytolysis with the discovery of a subscapular nodule. A biopsy showed plasma cells and, for several reasons, the decision was made to use the fractionated stereotactic radiotherapy strategy. After 20 months, he is asymptomatic and the immune globulin G component has completely disappeared.
Conclusion
We suggest considering Cyberknife® radiosurgery as an option for the treatment of hepatic solitary plasmacytoma.
Keywords: Solitary plasmacytoma, Liver, Radiosurgery
Background
Solitary plasmacytoma (SP) is a rare form of plasma cell dyscrasia with a single bone (SBP) or extramedullary location (EMP). It accounts for 3 to 5% of all plasma cell neoplasms [1]. Almost 85% of EMPs involve the head and neck mucosa, especially in the upper respiratory tract [2]. Gastrointestinal, lung, bladder, and testis involvement have also been reported. Only a few cases of hepatic SP have been reported to date [3, 4]. The presence of plasma cells in the liver or spleen is known to be associated with a more aggressive form of multiple myeloma [3] that usually requires a heavy treatment with chemotherapy or consolidation therapy with autologous hematopoietic stem cell transplantation.
Radiotherapy is the treatment of choice for EMP, with excellent response rates of approximately 86% [5]. Fractionated stereotactic radiotherapy has been used for approximately two decades to deliver ablative high-dose irradiations to small target volumes and low-dose irradiations to adjacent normal tissue. It plays an increasingly important role in the therapeutic arsenal of primary and secondary liver tumors but, to the best of our knowledge, its use has never been described in the treatment of hepatic plasmacytoma. We present a rare case of hepatic SP that successfully responded to a treatment with Cyberknife®.
Case presentation
A 64-year-old white French man had stable monoclonal gammopathy of the immune globulin G (IgG) lambda type (IgG = 1 g/L) with normal bone X-rays. He had no other significant comorbidities, except for diabetes and hypertension. Two years after the diagnosis of monoclonal gammopathy, he developed cholestasis 10N (10 x normal level) and cytolysis 4N (4 x normal value). Ultrasounds revealed a 4-cm subcapsular nodule involving segment VI of his liver. Magnetic resonance imaging (MRI) revealed multiple signal anomalies, with hemangiomas and benign cysts and a slightly hyperintense nodule on the T2-weighted image (Fig. 1a) and T1-weighted image, with arterial phase enhancement (Fig. 1b). Positron emission tomography-computed tomography (PET-CT) with 18fluorodeoxyglucose (18FDG) revealed an unusual hypermetabolic nodule, with maximum standardized uptake value (SUVmax) at 16. An ultrasound-guided biopsy showed numerous plasma cells (Fig. 1c) with a strong CD138 staining and low lambda light chain intensity (Fig. 1d). A full blood count revealed: hemoglobin 140 g/L, platelets 160 G/L, and leukocytes 5 G/L. All other laboratory parameters including renal function, albumin, beta-2-microglobulin, and calcium were within the normal range. A bone marrow examination and skeletal assessment were normal and a diagnosis of hepatic EMP was made. Surgery was deemed too difficult to perform because of the proximity of the kidney, and standard conformal irradiation was also contraindicated for the same reason and because the lesion was highly mobile due to breathing movements. However, our multidisciplinary team suggested the use of fractionated stereotactic radiotherapy in synchrony mode using implanted fiducials to limit liver toxicity in this patient with a single lesion without bone marrow involvement.
Fig. 1.
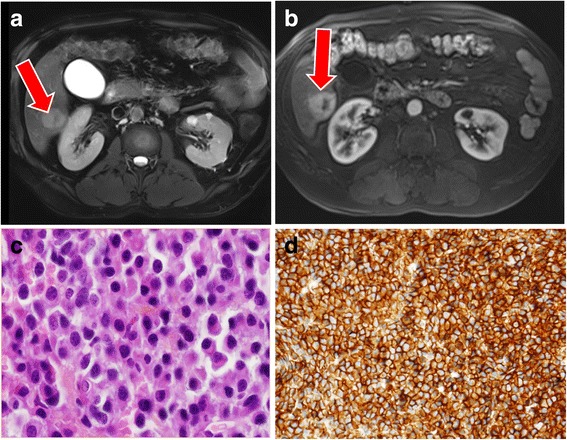
Magnetic resonance imaging images and tissue sections at diagnosis. a The lesion is hyperintense on the T2-weighted image (arrow) b and on the T1-weighted image with arterial phase enhancement with a centered hypointense signal in the probably necrotic tissue (arrow). c Diffuse proliferation of small monotonous round-to-ovoid cells with eccentric cytoplasms and round nuclei with d immunohistochemical analysis showing CD138 staining
In February 2015, our patient received 30 Gy in five consecutive fractions of 6 Gy, a dose that may be considered biologically equivalent to 40 Gy delivered in 2 Gy per fraction. The tolerance was excellent without acute toxicity. At month 3, 18FDG PET-CT revealed a stable disease, and subsequent assessments showed a partial response of 50% and 75% at month 12 and month 18, respectively (Fig. 2a). SUVmax also decreased to 8.2 at month 12 and 4.8 at month 18. Twenty months after irradiation, he is still asymptomatic with a normal biological liver function and IgG lambda M component has completely disappeared (Fig. 2b). No significant toxicity was observed during and after radiosurgery.
Fig. 2.
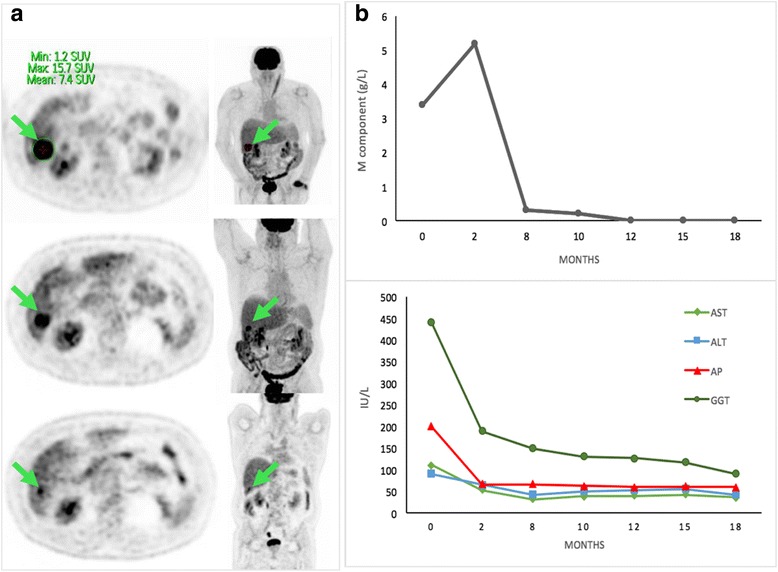
18Fluorodeoxyglucose positron emission tomography-computed tomography images and biologic graphics prior to and following therapy. a Images showing axial and coronal 18fluorodeoxyglucose positron emission tomography-computed tomography of the lesion in segment VI before radiosurgery, at month 12 with a 50% decrease and at month 18 with a 75% decrease. The arrow indicates the plasmacytoma lesion in both planes. All images show a partial remission of the metabolic activity of the nodule after Cyberknife® therapy compared to month 0. b The figures show reduced IgG M component with a maximum of 5.2 g of IgG/L and standardization from month 12 with normal immunofixation. The graphic below shows the concentration of liver enzymes, alkaline phosphatase, and gamma-glutamyltransferase. ALT alanine aminotransferase, AP alkaline phosphatase, AST aspartate aminotransferase, GGT gamma-glutamyltransferase, SUV standardized uptake value
Discussion
We describe a very good partial response of a very rare form of hepatic EMP with fractionated stereotactic radiotherapy. The diagnosis was made according to the recently updated recommendations [6], and differential diagnoses such as other neoplasms [7] were ruled out by histologic examination.
Radiation therapy is the best option for patients with localized EMP over systemic chemotherapy. Recommendations include a radiotherapy dose of 40 Gy in 20 fractions for tumors <5 cm and up to 50 Gy in 25 fractions for tumors ≥5 cm with at least a 2-cm margin encompassing the primary tumor [8]. Other alternatives exist like surgery or combined chemotherapy treatment, but are not justified outside clinical trials. Hepatic plasmacytomas without systemic disease have been treated either by chemotherapy (melphalan/steroids or vincristine, adriamycin, and dexamethasone combinations) or by radiotherapy [9]. Only a few cases of SP treated by fractionated stereotactic radiotherapy have been reported, and our case is the first reported with a hepatic localization. Wong et al. reported a plasmacytoma of the clivus extending to the foramen magnum treated by fractionated stereotactic radiotherapy with a complete and durable response on MRI at 12 months [10]. Theiler et al. reported the case of a 49-year-old man with SP of the bone, with radiotherapy as first-line treatment and radiosurgery for the treatment of local relapse with disappearance of bone lesion [11]. Other cases reported Cyberknife® success in plasmacytoma in neurological localizations such as cavernous sinus [12], cranial [13], and spine cord [14]. To the best of our knowledge, this is the first case of successful fractionated stereotactic radiotherapy use in hepatic SP. The absence of toxicity observed in this unusual observation suggests that other patients with similar presentations could benefit from this treatment modality.
Conclusions
This case shows that stereotactic radiotherapy could be highly effective in localized liver plasmacytoma. The Cyberknife® technology, which combines high precision and surrounding tissue protection, could be an alternative to conventional radiotherapy in some cases [11, 12]. Due to the lack of guidelines and clinical trials, the indication of fractionated stereotactic radiotherapy for the treatment of plasmacytoma should be further studied. In our case, the radiographic response was almost complete, safety was satisfactory, and our patient is still asymptomatic after 20 months. We suggest considering fractionated stereotactic radiotherapy as an option for the treatment of hepatic SP.
Acknowledgements
Not applicable.
Funding
Not applicable.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Authors’ contributions
TC collected the data and wrote the manuscript; IB and LB treated the patient and approved the manuscript; EG wrote and approved the manuscript; JPB and FA provided and analyzed tissue sections; MSR, MB, OH, and EP contributed essential tools. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Thomas Chalopin, Email: tomchalopin@yahoo.fr.
Isabelle Barillot, Email: i.barillot@chu-tours.fr.
Jean-Paul Biny, Email: prologue37@gmail.com.
Flavie Arbion, Email: f.arbion@chu-tours.fr.
Marie Besson, Email: m.besson@chu-tours.fr.
Maria Santiago-Ribeiro, Email: M.SANTIAGORIBEIRO@chu-tours.fr.
Eric Piver, Email: piver_e@med.univ-tours.fr.
Olivier Herault, Email: olivier.herault@univ-tours.fr.
Emmanuel Gyan, Email: emmanuel.gyan@univ-tours.fr.
Lotfi Benboubker, Email: l.benboubker@chu-tours.fr.
References
- 1.Dimopoulos MA, Hamilos G. Solitary bone plasmacytoma and extramedullary plasmacytoma. Curr Treat Options Oncol. 2002;3:255–9. doi: 10.1007/s11864-002-0015-2. [DOI] [PubMed] [Google Scholar]
- 2.Finsinger P, Grammatico S, Chisini M, Piciocchi A, Foa R, Petrucci MT. Clinical features and prognostic factors in solitary plasmacytoma. Br J Haematol. 2016;172(4):554–60. doi: 10.1111/bjh.13870. [DOI] [PubMed] [Google Scholar]
- 3.Petrucci MT, Tirindelli MC, De Muro M, Levi A, Mandelli F. Extramedullary Liver Plasmacytoma: a rare presentation. Leuk Lymphoma. 2003;44(6):1075–6. doi: 10.1080/1042819031000067882. [DOI] [PubMed] [Google Scholar]
- 4.Husaric S, Pasic J, Alic E, Kuljanin M. Solitary extramedullary plasmacytoma of the liver. Acta Med Acad. 2013;42(1):85–6. doi: 10.5644/ama2006-124.76. [DOI] [PubMed] [Google Scholar]
- 5.Knobel D, Zouhair A, Tsang RW, Poortmans P, Belkacemi Y, Bolla M, Oner FD, Landmann C, Castelain B, Ozsahin M. Prognostic factors in solitary plasmacytoma of the bone: a multicenter Rare Cancer Network study. BMC Cancer. 2006;6:118. doi: 10.1186/1471-2407-6-118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rajkumar SV, Dimopoulos MA, Palumbo A, Blade J, Merlini G, Mateos MV, Miguel JFS. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538–48. doi: 10.1016/S1470-2045(14)70442-5. [DOI] [PubMed] [Google Scholar]
- 7.Ng P, Slater S, Radvan G, Price A. Hepatic plasmacytomas : Case report and review of imaging features. Australas Radiol. 1999;43(1):98–101. doi: 10.1046/j.1440-1673.1999.00603.x. [DOI] [PubMed] [Google Scholar]
- 8.Soutar R, Lucraft H, Jackson G, Reece A, Bird J, Low E, Samson D. Guidelines on the diagnosis and management of solitary plasmacytoma of bone and solitary extramedullary plasmacytoma. Br J Haematol. 2004;124:717–26. doi: 10.1111/j.1365-2141.2004.04834.x. [DOI] [PubMed] [Google Scholar]
- 9.Ozsahin M, Tsang RW, Poortmans P, Belkacemi Y, Bolla M, Dincbas FO, Landmann C, Castelain B, Buijsen J, Curschmann J, Kadish SP, Kowalczyk A, Anacak Y, Hammer J, Nguyen TD, Studer G, Cooper R, Sengoz M, Scandolaro L, Zouhair A. Outcomes and patterns of failure in solitary plasmacytoma: a multicenter Rare Cancer Network study of 258 patients. Int J Radiat Oncol Biol Phys. 2006;64:210–7. doi: 10.1016/j.ijrobp.2005.06.039. [DOI] [PubMed] [Google Scholar]
- 10.Wong ET, Lu XQ, Devulapalli J, Mahadevan A. Cyberknife radiosurgery for basal skull plasmacytoma. J Neuroimaging. 2006;16:361–3. doi: 10.1111/j.1552-6569.2006.00062.x. [DOI] [PubMed] [Google Scholar]
- 11.Theiler G, Schwetz V, Gstettner C, Wowra B, Fürweger C, Steiner J, Schmidt HH. Cyberknife radiosurgery leading to long-lasting complete remission in locally relapsed solitary plasmacytoma of the bone. Ann Hematol. 2015;94:1251–3. doi: 10.1007/s00277-015-2365-4. [DOI] [PubMed] [Google Scholar]
- 12.Peker S, Abacioglu U, Bayrakli F, Kilic T, Pamir MN. Gamma knife radiosurgery for cavernous sinus plasmacytoma in a patient with breast cancer history. Surg Neurol. 2005;63:174–6. doi: 10.1016/j.surneu.2003.12.013. [DOI] [PubMed] [Google Scholar]
- 13.Alafaci C, Grasso G, Conti A, Caffo M, Salpietro FM, Tomasello F. Cyberknife radiosurgery for cranial plasma cell tumor. Turk Neurosurg. 2014;24:272–5. doi: 10.5137/1019-5149.JTN.7049-12.0. [DOI] [PubMed] [Google Scholar]
- 14.Chang UK, Lee DH, Kim MS. Stereotactic radiosurgery for primary malignant spinal tumors. Neurol Res. 2014;36:597–606. doi: 10.1179/1743132814Y.0000000381. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.