

Abstract
Background Tears of the dorsal radiocarpal capsule at the level of the scapholunate interosseous ligament (SLIL) have recently been described in association with predynamic scapholunate instability.
Purpose The aim of this anatomical study of the dorsal capsulo-scapholunate septum (DCSS) was to examine the connection of the dorsal capsule on the SLIL and dorsal intercarpal ligament (DICL).
Methods Fourteen fresh frozen wrists from seven adult cadavers were dissected through a dorsal approach. Any dorsal attachment of the DICL on the dorsal surface of the SLIL, that is, the DCSS, was identified and measured (height and width).
Results The DCSS was consistently found connecting the DICL, the dorsal radiocarpal capsule, and the dorsal aspect of the SLIL. It was formed by the confluence of three arches like intersecting ribs in gothic architecture. The mean dimensions of the DCSS were 5.8 mm in height and 4.0 mm in maximum width.
Conclusion The DCSS that connects the SLIL with the dorsal capsule and DICL could be a constant structure of dorsal wrist. Further investigation is required to study the histology of the DCSS and its biomechanical properties in isolation to know whether the DCSS can be considered a secondary stabilizer of the scapholunate ligament complex.
Clinical Relevance A better anatomical knowledge of scapholunate ligament complex could help understand and manage instability of the wrist.
Keywords: dorsal capsulo-scapholunate septum, dorsal wrist capsule, scapholunate instability, scapholunate ligament
The significant contribution of the dorsal intrinsic and extrinsic ligaments in stabilizing the scapholunate complex has been previously analyzed. The scapholunate interosseous ligament (SLIL), particularly the dorsal portion, is considered the primary stabilizer between the scaphoid and lunate. 1 Secondary stabilizers are thought to contribute to scaphoid stability after the SLIL was damaged. Berger and Garcia-Elias suggested that the scapho-triquetral ligament (proximal dorsal intercarpal ligament fibers [DICL]) played an important role in transverse stabilization of the proximal carpal row. 2 Several biomechanical studies emphasized the contribution of the DICL on scaphoid rotatory stability. 3 4 5 6 Van Overstraten described a ligamentous attachment that was called the dorsal capsulo-scapholunate septum (DCSS), between the dorsal part of the SLIL and the DICL. 7
Binder et al described a clinical case series of detachment of the DCSS from the dorsal portion of the SLIL, in which radiocarpal and midcarpal arthroscopy revealed Geissler grade 2 scapholunate instability despite an intact dorsal portion of the scapholunate ligament. 8 This led to the hypothesis that the dorsal tether between the scapholunate ligament and the dorsal wrist capsule could be related with the dorsal wrist pain and the predynamic scapholunate instability. An arthroscopic reanchoring procedure between the scapholunate ligament and dorsal capsule obtained excellent results. 8
Despite the awareness in the literature of an attachment between the scapholunate interval and dorsal capsule, 9 it has not previously been the focus of an anatomical study. The purpose of this study was to examine the anatomical features of the DCSS as well as its relationships to the SLIL and DICL.
Materials and Methods
Fourteen fresh frozen wrists from seven adult cadavers were dissected to assess the features of the dorsal attachment between the dorsal capsule and the SLIL. There were two males and five females. The mean age of the cadavers was 70 years old (60–80). The cadaver was placed in the supine position with the arm extended on an arm table. The wrist was placed in pronation. Each wrist was approached dorsally. The skin was incised longitudinally from the base of the middle proximal phalanx to the mid forearm. The extensor retinaculum was incised and retracted, and the extensor tendons were all excluded. Using loupe magnification, the dorsal capsule was exposed. A transverse incision was made 2 cm proximal to the wrist joint, and the capsule and wrist ligaments were elevated en bloc carefully by dissecting directly on the radius. Once the wrist joint was reached, the wrist was placed in full flexion to allow excellent visualization of the scapholunate interval. The synovial layer was removed. The DICL was carefully dissected to its attachments. The DCSS was identified between the scapholunate ligament and the dorsal capsule preventing passage of an instrument further distally. We measured the dimensions of the DCSS between the deep side of the DICL and the dorsal part of the SLIL. A metal ruler was utilized and each measurement was recorded to the whole millimeter.
Routine measurements of the DCSS included ( Fig. 1 ):
Fig. 1.
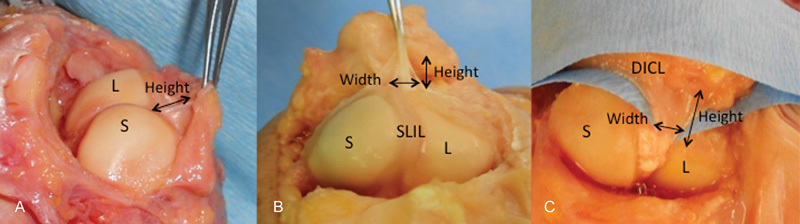
(A–C) Dorsal view of three cadaver wrists. The dorsal capsulo-scapholunate septum is extended between the dorsal aspect of the scapholunate interosseous ligament and the proximal transverse fibers of the dorsal intercarpal ligament. Width and height were measured in every wrist. DICL, dorsal intercarpal ligament; L, lunate; S, scaphoid; SLIL, scapholunate interosseous ligament.
Height: a stretched distance between the SLIL and the DICL
Width: a stretched transverse measurement at the mid-point of the DCSS
Photographs were taken of the structure with the wrist in flexion and the dorsal capsule elevated distally for better visualization.
Results
The DCSS was consistently observed in the 11 wrists from 6 specimens ( Table 1 ; Fig. 1 ), while three were excluded due to severe chondrocalcinosis in the bilateral wrists from one specimen and due to the pan-carpal arthritis without the intrinsic ligaments in the other wrist. Grossly the DCSS was seen as consisting of three arches ( Figs. 1 , 2 ). There were two transverse arches in series along the DICL and a third longitudinal one across the radiocarpal joint. The transverse arches extended between the scaphoid insertion and the triquetral insertion of the DICL. They formed two semi–hood-like structures that met the third arch over the dorsal part of the SLIL like gothic intersecting ribs. The third arch was larger than the previously mentioned and extended in the longitudinal plane. It demonstrated a wide diffuse attachment along the scapholunate ligament and then arched dorsally fanning out to a longer insertion into the dorsal capsule of the radiocarpal joint. A synovial layer surrounded the DCSS, creating a small dividing wall in the radiocarpal compartment ( Figs. 1 , 2 ).
Table 1. Measurements data of the DCSS in the 11 cadavers specimen.
| Cadaver | Sex | Wrist | Side | Height (mm) | Width (mm) |
|---|---|---|---|---|---|
| 1 | Female | 1 | Left | 4 | 5 |
| 2 | Female | 2 | Right | 6 | 3 |
| 3 | Left | 6 | 2 | ||
| 3 | Male | 4 | Right | 6 | 2 |
| 5 | Left | 6 | 2 | ||
| 4 | Female | 6 | Right | 8 | 7 |
| 7 | Left | 5 | 4 | ||
| 5 | Female | 8 | Right | 4 | 3 |
| 9 | Left | 8 | 5 | ||
| 6 | Female | 10 | Right | 6 | 3 |
| 1 | Left | 5 | 8 | ||
| Average (mm) | 5.82 | 4 |
Abbreviation: DCSS, dorsal capsulo-scapholunate septum.
Fig. 2.
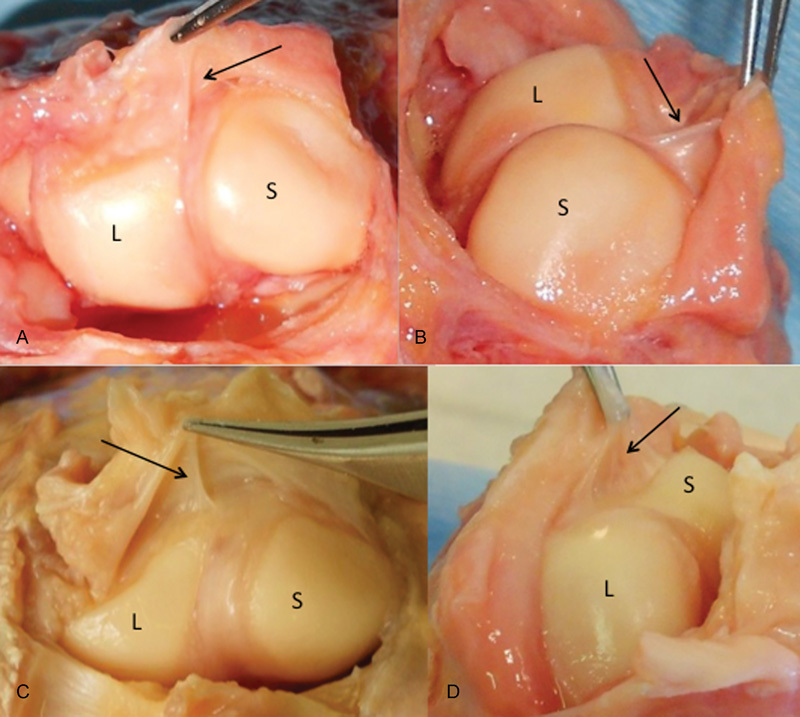
(A–D) Dorsal view of two cadaver wrists. The three arches of the DCSS are well seen when the DICL is held at stretch.
The height indicated an average of 5.8 mm (4.0–8.0 mm). The width was found to be an average of 4.0 mm (2.0–8.0 mm) ( Table 1 , Fig. 1 ).
Discussion
The SLIL binds the scaphoid and lunate together in a nearly seamless interval when viewed by arthroscopy from the radiocarpal compartment. 10 The SLIL is C-shaped and has strong confluent attachments along the dorsal, proximal and volar margins of the scaphoid and lunate. The dorsal component is known to be the thickest, strongest, and the most critical part of the SLIL in stabilization of the scapholunate interval. 11 Buijze et al highlighted the inconsistencies within current literature in describing the scaphoid ligament attachments, probably due to anatomic variations. 12 The dorsodistal part of the SLIL merges with the DICL, whereas proximally it merges with the membranous region of the dorsal carpal capsule. 12
Viegas et al examined the anatomical and mechanical properties of the dorsal radiocarpal ligament (DRCL) and DICL. 9 The DICL comprised two sections consisting of a thinner distal portion extending between the dorsal tubercle of the triquetrum to the trapezoid and the capitate, and a thicker proximal section extending from the triquetrum to the trapezium with attachment on the lunate in 90% of cases as well as on the scaphoid. The DRCL and DICL formed a “V” with two arms that had the ability to vary their length throughout the range of motion of the wrist. They concluded that the integrity of the dorsal ligamentous structures was important in maintaining carpal stability, alignment, and normal carpal kinetics, therefore preventing volar intercalated segmental instability (VISI) and dorsal intercalated segmental instability (DISI) deformities. 9 Insertions of the DICL were found on the triquetrum, trapezoid, scaphoid, and SLIL. 2 13 14
Several biomechanical studies also described contribution of the DICL on scaphoid rotatory stability. 3 4 5 6 Elsaidi et al evaluated the role of the dorsal capsuloligamentous structures in preventing scapholunate instability and emphasized the importance of the dorsal capsular insertion and the dorsal intercarpal complex ligament insertion onto the scaphoid and scapholunate ligaments. 6 They demonstrated that arthroscopic sectioning of the palmer extrinsic ligaments and sequential sectioning of the three components of the SLIL did not result in flexion deformity of the scaphoid as long as the dorsal capsuloligamentous insertions on to the scapholunate ligament and dorsum of the scaphoid remained intact. After sectioning of the SLIL, the DICL and the dorsal capsular attachments to the scaphoid may act as a tether to prevent rotatory subluxation of the scaphoid. 6
Mitsuyasu et al observed that disruption of the DICL from the scaphoid and sectioning of the scapholunate ligament changed the scaphoid position and widened the scapholunate interval significantly under loading. 15 However, the lunate was unchanged in its position with/without load until the DICL was detached from the lunate. This suggests that the DICL may relate with scapholunate instability. Several studies demonstrated the clinical significance of the dorsal capsuloligamentous insertions to the scaphoid to the scaphoid stability. 16 17 18 19 20
This study demonstrated the consistent presence of the DCSS that attached the dorsal aspect of the SLIL to the DICL. The height of the DCSS indicated an average of 5.8 mm and the width was an average of 4.0 mm. From these anatomical features, the DCSS can stabilize the proximal carpal row. 2 9
A recent biomechanical study demonstrated the role of the dorsal capsular attachment of the SLIL in predynamic scapholunate stability. 7 In this study, sectioning of the DCSS from the SLIL resulted in an increased arthroscopic grade of scapholunate instability, 3 21 but it did not affect the significant scapholunate gap or angle.
The limitations of our study included (1) the small number of specimen and (2) the absence of biomechanical or histologic assessment. We cannot eliminate anatomical variations consisting in an absent or thinner DCSS. Moreover, we dissected both wrists of the same cadavers, which diminishes the number of possible variations encountered.
In conclusion, the DCSS that connects the SLIL with the dorsal capsule and DICL could be a constant structure in the dorsal wrist and may play a role in carpal stability. A clinical study exploring the integrity of the DCSS in cases of predynamic scapholunate instability would contribute to a better understanding of its importance.
Acknowledgments
The authors thank all the staff of the anatomy laboratory of the Ecole de Chirurgie du Fer à Moulin (Paris) for its precious help.
Footnotes
Conflict of Interest None. Note This work was performed in the anatomy laboratory of the Ecole de Chirurgie du Fer à Moulin, Paris.
References
- 1.Berger R A. The gross and histologic anatomy of the scapholunate interosseous ligament. J Hand Surg Am. 1996;21(02):170–178. doi: 10.1016/S0363-5023(96)80096-7. [DOI] [PubMed] [Google Scholar]
- 2.Berger R A, Garcia-Elias M. New York, NY: Springer-Verlag; 1991. General anatomy of the wrist; pp. 1–22. [Google Scholar]
- 3.Geissler W B. New York, NY: Springer; 2005. Management of scapholunate instability; pp. 86–93. [Google Scholar]
- 4.North E R, Thomas S. An anatomic guide for arthroscopic visualization of the wrist capsular ligaments. J Hand Surg Am. 1988;13(06):815–822. doi: 10.1016/0363-5023(88)90253-5. [DOI] [PubMed] [Google Scholar]
- 5.Van Overstraeten L. Montpellier, France: Sauramps Medical; 2009. Anatomie arthroscopique et lésions des ligaments extrinsèques; pp. 105–116. [Google Scholar]
- 6.Elsaidi G A, Ruch D S, Kuzma G R, Smith B P.Dorsal wrist ligament insertions stabilize the scapholunate interval: cadaver study Clin Orthop Relat Res 2004;(425152–157. [DOI] [PubMed] [Google Scholar]
- 7.Van Overstraeten L, Camus E J, Wahegaonkar A et al. Anatomical description of the dorsal capsulo-scapholunate septum (DCSS). Arthroscopic staging of scapholunate instability after DCSS sectioning. J Wrist Surg. 2013;00:1–6. doi: 10.1055/s-0033-1338256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Binder A C, Kerfant N, Wahegaonkar A L, Tandara A A, Mathoulin C L. Dorsal wrist capsular tears in association with scapholunate instability: results of an arthroscopic dorsal capsuloplasty. J Wrist Surg. 2013;2(02):160–167. doi: 10.1055/s-0032-1333426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Viegas S F, Yamaguchi S, Boyd N L, Patterson R M. The dorsal ligaments of the wrist: anatomy, mechanical properties, and function. J Hand Surg Am. 1999;24(03):456–468. doi: 10.1053/jhsu.1999.0456. [DOI] [PubMed] [Google Scholar]
- 10.Kuo C E, Wolfe S W. Scapholunate instability: current concepts in diagnosis and management. J Hand Surg Am. 2008;33(06):998–1013. doi: 10.1016/j.jhsa.2008.04.027. [DOI] [PubMed] [Google Scholar]
- 11.Berger R A.Arthroscopic anatomy of the wrist and distal radioulnar joint Hand Clin 19991503393–413., vii [PubMed] [Google Scholar]
- 12.Buijze G A, Lozano-Calderon S A, Strackee S D, Blankevoort L, Jupiter J B. Osseous and ligamentous scaphoid anatomy: Part I. A systematic literature review highlighting controversies. J Hand Surg Am. 2011;36(12):1926–1935. doi: 10.1016/j.jhsa.2011.09.012. [DOI] [PubMed] [Google Scholar]
- 13.Mizuseki T, Ikuta Y. The dorsal carpal ligaments: their anatomy and function. J Hand Surg [Br] 1989;14(01):91–98. doi: 10.1016/0266-7681(89)90025-9. [DOI] [PubMed] [Google Scholar]
- 14.Savelberg H H, Kooloos J G, Huiskes R, Kauer J M. Stiffness of the ligaments of the human wrist joint. J Biomech. 1992;25(04):369–376. doi: 10.1016/0021-9290(92)90256-z. [DOI] [PubMed] [Google Scholar]
- 15.Mitsuyasu H, Patterson R M, Shah M A, Buford W L, Iwamoto Y, Viegas S F. The role of the dorsal intercarpal ligament in dynamic and static scapholunate instability. J Hand Surg Am. 2004;29(02):279–288. doi: 10.1016/j.jhsa.2003.11.004. [DOI] [PubMed] [Google Scholar]
- 16.Blatt G. Capsulodesis in reconstructive hand surgery. Dorsal capsulodesis for the unstable scaphoid and volar capsulodesis following excision of the distal ulna. Hand Clin. 1987;3(01):81–102. [PubMed] [Google Scholar]
- 17.Lavernia C J, Cohen M S, Taleisnik J. Treatment of scapholunate dissociation by ligamentous repair and capsulodesis. J Hand Surg Am. 1992;17(02):354–359. doi: 10.1016/0363-5023(92)90419-p. [DOI] [PubMed] [Google Scholar]
- 18.Wintman B I, Gelberman R H, Katz J N. Dynamic scapholunate instability: results of operative treatment with dorsal capsulodesis. J Hand Surg Am. 1995;20(06):971–979. doi: 10.1016/S0363-5023(05)80145-5. [DOI] [PubMed] [Google Scholar]
- 19.Mathoulin C L, Dauphin N, Wahegaonkar A L.Arthroscopic dorsal capsuloligamentous repair in chronic scapholunate ligament tears Hand Clin 20112704563–572., xi [DOI] [PubMed] [Google Scholar]
- 20.Wahegaonkar A L, Mathoulin C L. Arthroscopic dorsal capsulo-ligamentous repair in the treatment of chronic scapho-lunate ligament tears. J Wrist Surg. 2013;2(02):141–148. doi: 10.1055/s-0033-1341582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Messina J C, Van Overstraeten L, Luchetti R, Fairplay T, Mathoulin C L. The EWAS classification of scapholunate tears: an anatomical arthroscopic study. J Wrist Surg. 2013;2(02):105–109. doi: 10.1055/s-0033-1345265. [DOI] [PMC free article] [PubMed] [Google Scholar]