

Abstract
Objectives
Flat epithelial atypia (FEA) is a relatively new diagnostic term with uncertain clinical significance for surgical management. Any implied risk of invasive breast cancer associated with FEA is contingent upon diagnostic reproducibility, yet little is known regarding its use.
Materials and Methods
Pathologists in the Breast Pathology Study interpreted one of four 60-case test sets, one slide per case, constructed from 240 breast biopsy specimens. An electronic data form with standardized diagnostic categories was used; participants were instructed to indicate all diagnoses present. We assessed participants’ use of FEA as a diagnostic term within: 1) each test set; 2) 72 cases classified by reference as benign without FEA; and 3) six cases classified by reference as FEA. 115 pathologists participated, providing 6,900 total independent assessments.
Results
Notation of FEA ranged from 0% to 35% of the cases interpreted, with most pathologists noting FEA on 4 or more test cases. At least one participant noted FEA in 34 of the 72 benign non-FEA cases. For the 6 reference FEA cases, participant agreement with the case reference FEA diagnosis ranged from 17% to 52%; diagnoses noted by participating pathologists for these FEA cases included columnar cell hyperplasia, usual ductal hyperplasia, atypical lobular hyperplasia, and atypical ductal hyperplasia.
Conclusions
We observed wide variation in the diagnosis of FEA among U.S. pathologists. This suggests that perceptions of diagnostic criteria and any implied risk associated with FEA may also vary. Surgical excision following a core biopsy diagnosis of FEA should be reconsidered and studied further.
Keywords: breast oncology, atypia, flat epithelial atypia, biopsy, observer variability
Introduction
Surgeons rely on the pathologist’s interpretation of a biopsy specimen to guide their management recommendations for women with abnormalities noted on mammography. This can be a difficult discussion, especially when carcinoma or atypia is part of the diagnosis. Many women and physicians are concerned about missing a carcinoma following a core biopsy diagnosis of atypia. Delay in diagnosis of breast cancer and failure to detect breast cancer are leading medical malpractice allegations,1 and may further encourage surgical management for atypical breast biopsy findings including flat epithelial atypia (FEA).
Up to 10% of core needle breast biopsies may include FEA, a type of proliferative intraductal epithelium associated with breast microcalcifications detected by radiologic imaging.2 Each year, 1.6 million breast biopsies are performed on women in the United States,3,4 suggesting a large number of women will be diagnosed with FEA. The World Health Organization (WHO) established the defining features of FEA in 2003.5 In the most recent WHO classification, FEA is defined as “a neoplastic alteration of the terminal-duct lobular units (TDLUs) characterized by replacement of the native epithelial cells by one to several layers of a single epithelial cell type showing low-grade (monomorphic) cytological atypia.”6 This WHO text description is accompanied by photomicrograph examples to assist distinguishing FEA from other epithelial proliferations with monomorphic cytological atypia.
Although earlier research posited the theory that pure FEA corresponds to a precursor stage of ductal carcinoma in situ (DCIS) or invasive carcinoma, most studies have shown that FEA rarely progresses to carcinoma.7–12 Nevertheless, a diagnosis of FEA includes the word “atypia” in its name, potentially causing concern to patients and clinicians. FEA has been associated with and may coexist with a family of indolent risk-associated proliferative lesions including atypical lobular hyperplasia (ALH), atypical ductal hyperplasia (ADH), lobular carcinoma in situ (LCIS), low-grade ductal carcinoma in situ (DCIS), and, less frequently, low-grade invasive carcinoma.6,13–15 Whether excisional biopsy should be offered when FEA is the only risk-associated lesion on core biopsy is not currently standardized.16–19 Uncertainty may encourage excisional biopsy.
The surgical outcomes after breast procedures are contingent on the reproducibility and accuracy of the pathological diagnosis. However, there is little data evaluating FEA as a diagnostic entity within a broad cross-section of practicing pathologists. In this analysis, we selected a spectrum of benign breast biopsy cases from the Breast Pathology (B-Path) study. Among this large cross-section of U.S. pathologists, we examine variability in diagnosis of FEA. We also identify and describe potential challenges associated with establishing a FEA diagnosis and the implications for surgical management.
Material and Methods
Data for this study originated from the B-Path Study, a large investigation examining diagnostic under- and over-interpretation of breast biopsy specimens by U.S. pathologists.20,21 The methods and test sets developed for the B-Path study are described elsewhere.22,23 In brief, each of four tests sets (A, B, C, and D) of breast biopsy specimens were created after sampling registries in Vermont and New Hampshire associated with the Breast Cancer Surveillance Consortium.24 Each test set was composed of 60 cases, one glass slide per case, randomized with stratification (N=240) to contain comparable pathological findings. Specimens were from excisional and core biopsies and from female patients ≥40 years of age. All study activities were approved by the Institutional Review Boards at Dartmouth College, Fred Hutchinson Cancer Research Center, Providence Health & Services Oregon, University of Vermont, and the University of Washington prior to data collection.
Reference Diagnosis on Test Cases
A panel of three experienced breast pathologists established a reference consensus interpretation for all 240 cases. Blinded to one another’s interpretations, the reference pathologists used a Breast Pathology Assessment Tool and Hierarchy for Diagnosis (BPATH-Dx) form to independently review each slide before meeting to establish a consensus reference diagnosis (Appendix A).25 Pathologists chose 1 or more diagnoses from 14 BPATH-Dx terms, which were grouped into 4 broad diagnostic categories with the following distribution: 30% benign (including normal breast tissue, non-proliferative fibrocystic changes, usual ductal hyperplasia [UDH], flat epithelial atypia [FEA], and atypical lobular hyperplasia [ALH]); 30% atypia (including atypical ductal hyperplasia [ADH] and intraductal papilloma with ADH); 30% DCIS; and 10% invasive carcinoma. ALH was included in the benign category exclusively for analytic reasons because lobular lesions were not a major focus of the main B-Path study.
Reference non-FEA Benign and Reference FEA Cases
Following reference consensus interpretation, there were six reference FEA cases that had FEA only or a combination of FEA and other lesions categorized as benign according to a consensus or majority of reference panel pathologists (Appendix B). FEA was the highest category lesion in all six cases. Three reference FEA cases (numbers 1, 2, and 5) were not reviewed during the consensus meetings because all three reference panel pathologists independently agreed on a benign proliferative diagnosis. In all three cases, two out of three reference pathologists (a majority) noted the presence of FEA on their independent interpretations. The remaining three reference FEA cases (numbers 3, 4, and 6) did not have definitive independent diagnostic agreement and were reviewed at consensus meetings, during which all three reference pathologists agreed on the presence of FEA and no higher-ranking diagnoses. A qualitative analysis of the consensus process for B-Path indicated that the most common reason underlying the need for consensus was differing opinions regarding whether a particular lesion, such as FEA, met diagnostic criteria.25
There were 72 benign non-FEA reference cases according to the consensus or majority of reference panel pathologists. The non-FEA cases comprised a spectrum of benign findings; individual slides may have included normal breast tissue, columnar cell change and hyperplasia (CCH), UDH, or ALH. Cases where only one reference pathologist indicated the presence of FEA were not excluded.
We considered the presence of other diagnoses in case selection because excision of proliferative lesions identified on core biopsy is often based on published associations with more severe disease on excisional biopsy (i.e., upstaging). For example, surgical excision is not routinely recommended for UDH, whereas many centers excise FEA if found on core needle biopsy.5,26,27 Excision for ALH on core biopsy is controversial; studies have shown that it may pose few risks, or its risk may depend on the extent of its presence.28–34 Thus, we included cases of FEA with UDH or ALH. We excluded cases of FEA with coexisting higher category lesions, including cases where the reference panel diagnosis noted ADH, intraductal papilloma with atypia (IPA), DCIS, or invasive cancer. It is not always standard practice for a pathologist to note all diagnostic lesions present on a slide, especially for lesions with lower risk relative to the primary diagnosis.
For the global assessment of the proportion of cases in each test set where the study participants noted FEA on the diagnostic form, we used all test set cases except those with invasive carcinoma. Random stratification of the 240 test cases into 4 test sets resulted in the following distribution of reference FEA cases: 3 in test set A, 2 in test set B, and 1 in test set C. FEA was not a random stratification variable for creating the test sets.
Participating Pathologist Recruitment and Characteristics
Pathologists with at least one year of experience interpreting breast specimens and who planned to continue practicing diagnostic breast pathology for at least one more year were recruited from eight states (AK, ME, MN, NH, NM, OR, VT, and WA). Pathology residents and fellows were excluded. After providing informed consent, all participants completed a web-based survey of demographic information and clinical practice characteristics.
Participating Pathologist Test Case Interpretation
Participating pathologists were randomly assigned with stratification on clinical expertise to independently interpret one of four test sets. Participants received one Hematoxylin and Eosin-stained (H&E) glass slide per case. All participants assigned to the same test set received the same slides. Pathologists were asked to assess cases and note all of the lesions present; there were no study-specific time constraints. Participants completed the same BPATH-Dx form for each case online that had been developed and used by the reference pathologists. We then determined the proportion of cases where FEA was identified out of 60 cases (a complete test-set) by each participant, the proportion of cases where FEA was identified among the subset of reference non-FEA benign cases, and, finally, the participants’ proportional agreement with the six reference FEA cases.
Results
Participating Pathologists’ Characteristics
Of 691 pathologists invited to join the B-Path study, 126 were randomly assigned to interpret the glass slide test sets. In total, 91% (115/126) independently interpreted all 60 cases in their assigned test set. Most (75.7%) did not have an academic affiliation, 51.3% had completed a fellowship in either surgical pathology or breast pathology, 21.7% reported being considered experts in breast pathology by their colleagues, and 59.1% worked in laboratory practices with fewer than ten pathologists.
Global use of FEA Diagnostic Term by Pathologists for the 60-Case Test Sets
Figure 1 shows the proportion of all test cases where participants and reference pathologists noted FEA during their initial independent interpretations. While the majority of pathologists noted FEA on 4 or more of the 60 test cases they interpreted, 9 (8%) participating pathologists identified FEA in ≥20% of the test cases, and 19 (17%) pathologists identified FEA in ≥15% of the cases. The reference pathologists also independently differed in the frequency with which they used the FEA diagnostic category (<5% to 20% of test cases).
Fig. 1.

Percentage of B-Path test set cases interpreted as having FEA present on the glass slide, with results shown for each participating pathologist and the three reference pathologists, organized according to test seta
a. Each test set was composed of 60 cases. Cases may have been given other higher order interpretations along with the diagnosis of FEA. Cases with higher order interpretations and cases identified as FEA by only a single reference panel pathologist were not used as reference FEA cases.
Participating Pathologists’ Assessments of Reference non-FEA Benign Cases
One or more participants noted the presence of FEA on 34 of the 72 reference non-FEA benign cases (Table 1). Four of the 34 cases (11.8%) were independently noted to have FEA by 1 reference pathologist, even though they did not qualify as reference FEA cases based on consensus or the majority of reference pathologists. Six of the 34 cases were noted as having FEA by 20% or more of the participating pathologists. Common reference diagnoses for these 34 cases included CCH, UDH, and ALH.
Table 1.
Breast biopsy cases defined as benign with no FEA by the reference consensus panel, yet identified as FEA by one or more participating pathologists.
| Case Number | FEA was independently identified by at least one reference panel member | Reference panel diagnosisa | Number of Participants who identified FEA/ Number of Participants who independently interpreted the case (%) | |
|---|---|---|---|---|
| 7 | Yes | (CCH) | 18/27 | (66.7%) |
| 8 | No | (UDH, CCH) | 11/30 | (36.7%) |
| 9 | Yes | ALH, UDH, CCH | 8/30 | (26.7%) |
| 10 | Yes | ALH, UDH, CCH | 7/30 | (23.3%) |
| 11 | Yes | UDH | 6/29 | (20.7%) |
| 12 | No | Fibroadenoma | 6/30 | (20.0%) |
| 13 | No | (UDH, CCH) | 5/27 | (18.5%) |
| 14 | No | UDH, CCH | 4/27 | (14.8%) |
| 15 | No | (NPR) | 4/29 | (13.8%) |
| 16 | No | (CCH) | 4/30 | (13.3%) |
| 17 | No | CCH | 3/27 | (11.1%) |
| 18 | No | UDH | 3/29 | (10.3%) |
| 19 | No | UDH | 3/29 | (10.3%) |
| 20 | No | LCIS, IPW, UDH,CCH | 3/30 | (10.0%) |
| 21 | No | (UDH, CCH, Fib) | 3/30 | (10.0%) |
| 22 | No | (UDH) | 2/27 | (7.4%) |
| 23 | No | (UDH) | 2/29 | (6.9%) |
| 24 | No | ALH, UDH | 2/29 | (6.8%) |
| 25 | No | (UDH, CCH) | 2/29 | (6.9%) |
| 26 | No | (CCH, SCL) | 2/29 | (6.9%) |
| 27 | No | RSL | 2/29 | (6.9%) |
| 28 | No | ALH, UDH, RSL | 2/30 | (6.7%) |
| 29 | No | NPR | 2/30 | (6.7%) |
| 30 | No | UDH | 2/30 | (6.7%) |
| 31 | No | (CCH, RSL, ALH) | 1/27 | (3.7%) |
| 32 | No | (UDH) | 1/27 | (3.7%) |
| 33 | No | (UDH, CCH) | 1/27 | (3.7%) |
| 34 | No | NPR | 1/27 | (3.7%) |
| 35 | No | Fibroadenoma | 1/27 | (3.7%) |
| 36 | No | UDH | 1/29 | (3.4%) |
| 37 | No | (NPR) | 1/29 | (3.4%) |
| 38 | No | (NPR) | 1/29 | (3.4%) |
| 39 | No | NPR | 1/29 | (3.4%) |
| 40 | No | (NPR) | 1/30 | (3.3%) |
Parentheses indicate that the case did not go to consensus. When a case did not go to consensus, the reference diagnosis was determined based on which lesions were identified by two or more reference pathologists.
FEA = flat epithelial atypia; CCH = columnar cell change or hyperplasia; UDH = usual ductal hyperplasia; ALH = atypical lobular hyperplasia; NPR = non-proliferative changes only; LCIS = lobular carcinoma in situ; IPW = intraductal papilloma without atypia; Fib = fibroadenoma; RSL = radial scar/complex sclerosing lesion.
Participating Pathologists’ Assessments on the 6 Reference FEA Cases
The study pathologists who interpreted the 6 reference FEA cases provided a total of 175 individual interpretations (29 to 30 participants interpreted each case). Many participants listed multiple lesion types in their interpretations (Appendix B). Pathologists demonstrated the highest rate of agreement with the reference FEA diagnosis for case 1 (52%) and the lowest rate of agreement for case 6 (17%). Figure 2 shows common diagnoses by participants including CCH, UDH, ADH, and alternative benign lesions.
Fig. 2.

Frequency of diagnostic terms used by participating pathologists for reference FEA casesa
a. All six reference FEA cases had FEA only, or a combination of FEA and other lesions categorized as benign without atypia according to the reference panel. Percentages add up to >100% because participants could mark combinations of lesion types for a single case. See Appendix B for a table showing the reference diagnosis for each case and the number of participants who interpreted each lesion.
Discussion
We observed extensive and concerning variability in use of the FEA diagnostic term by practicing U.S. pathologists. Some pathologists identified FEA in more than 20% of the breast biopsy slides they interpreted, while others refrained from using the FEA term entirely. This variability likely represents a combination of differing thresholds for including a proliferative lesion in the FEA category, varied understanding or application of diagnostic criteria, and the challenge associated with assigning a categorical diagnosis to a continuum of histopathological features.
The implications for surgical management of CCH and ADH are generally different than those suggested for FEA. A diagnosis of CCH does not warrant further treatment whether diagnosed on a core or excisional biopsy, whereas women with ADH are considered at increased risk of developing breast cancer and typically undergo excisional biopsy following a core biopsy diagnosis to exclude low-grade DCIS. When the final diagnosis is ADH, some women consider heightened surveillance and risk reduction using hormonal or surgical treatments.35–37 Both ADH and FEA may have adjacent coexisting disease such as low-grade DCIS and low- grade invasive carcinomas, including tubular carcinomas. For this reason, some argue that FEA diagnosed on core biopsy should be followed by excisional biopsy to exclude an adjacent low-grade carcinoma. The counter argument is that the associated coexisting disease is relatively indolent and could be managed with surveillance.8–10,16,17,19 In addition, the intrinsic biologic risk for future breast cancer is considerably lower for FEA than for ADH.38
The surgical management of FEA is complicated by the potential magnitude of its prevalence in clinical practice. Previous research suggests that up to 10% of all core needle breast biopsies may have FEA noted by the interpreting pathologist.2 Our study corroborates these observations. Although studies have evaluated the incidence of breast cancer in women with FEA,39,40 their applicability relies on the reproducibility of FEA as a diagnostic entity. Other studies have found only moderate agreement (Kappa=0.47) for diagnoses of FEA.41
Pathologists with a special interest in breast pathology are better at distinguishing FEA from other lesions when tested immediately after a brief educational intervention.42,43 Thus, it is possible that the diagnosis of FEA can be improved through education. Figure 3 and Figure 4 describe some of the educational issues associated with a diagnosis of FEA.
Fig. 3. Images and discussion points for three cases classified as FEA by reference pathologists.
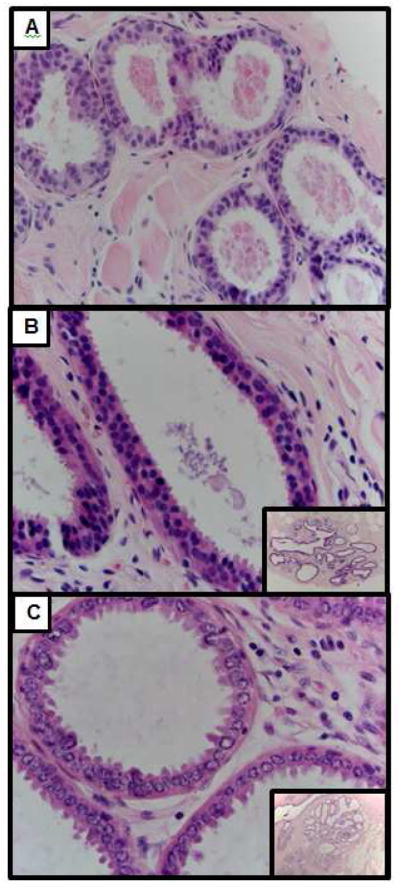
Fig. 3a) Case #1 Focus of FEA with intraluminal secretions. This lesion has round to ovoid monomorphic nuclei with some cellular stratification. In areas, the cells are oriented perpendicularly to the basement membrane reminiscent of columnar cell change, but in other areas, the cells lose this arrangement. Note the lack of slender, bland nuclei typical of columnar cell change and the presence of the more rounded nuclear contour of FEA. 2 of the 3 reference pathologists diagnosed this case as FEA. 52% of participating pathologists (N=29) interpreted this as FEA. Hematoxylin and eosin, 400X and 40X
Fig. 3b) Case #3 Focus of FEA in an enlarged TDLU. From low magnification (inset), note the dilated, hyperchromatic ducts that raise concern for FEA at scanning magnification. At higher magnification, the ducts are filled with rounded monomorphic cells that are not regularly oriented perpendicular to the basement membrane. There is cellular stratification and, although there are no prominent nucleoli or obvious chromatin margination, the cells resemble those seen in low grade ductal carcinoma in-situ. This lesion was interpreted as FEA by 34% of participating pathologists (N=29)
Fig. 3c) Case #5 Focus of FEA with prominent apical cytoplasmic snouting. From scanning magnification (inset), there are dilated ducts with round contours and hyperchromasia suggestive of FEA. At higher magnification, although there is no cellular stratification, the nuclei are round with a high nuclear to cytoplasmic ratio and prominent chromatin margination characteristic of FEA. 2 of the 3 reference pathologists diagnosed this case as FEA. This lesion was interpreted as FEA by 24% of participating pathologists (N=29)
Fig. 4. Images and discussion points for three cases classified as benign or ALH without FEA by reference pathologists. These cases were frequently interpreted as FEA by participating pathologists.
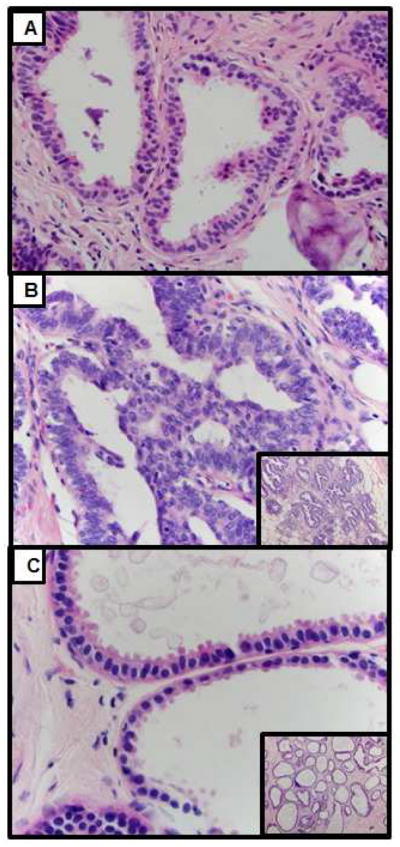
Fig. 4a) Case #7 Focus of columnar cell change and columnar cell hyperplasia in enlarged TLDUs with intraluminal calcifications. Although the nuclei of the cells lining the TLDUs in this lesion show mild pleomorphism, the cells are arranged perpendicularly to the basement membrane and do not have the round to ovoid monomorphic nuclei typical of FEA. The nuclear pleomorphism likely results from reaction to the intraluminal calcification. This lesion was interpreted as FEA by 67% of participating pathologists (N=27). Hematoxylin and eosin, 400X and 40X
Fig. 4b) Case #8 Focus of non-atypical proliferative change with enlarged terminal ductal lobular units (TLDUs) with irregular contours and usual ductal hyperplasia. Although from low power (see inset), the lesion is hyperchromatic, raising the possibility of FEA, at higher power, the cells are cytologically benign and are arranged in a haphazard pattern with poorly defined borders characteristic of usual ductal hyperplasia. Note the absence of low grade monomorphic round to ovoid nuclei typical of FEA. This lesion was interpreted as FEA by 37% of participating pathologists (N=30)
Fig. 4c) Case #10 Focus of columnar cell change in enlarged TDLUs. From low magnification (inset) the lesion has dilated ducts with round contours and mild hyperchromasia that is suggestive of FEA. However, at higher magnification, there is a single layer of non-atypical columnar to cuboidal cells with cytoplasmic snouts, intraluminal secretions and calcifications. The nuclei are arranged perpendicular to the basement membrane with evenly dispersed chromatin and no obvious nucleoli. These are features more consistent with columnar cell change rather than FEA. This lesion was interpreted as FEA by 23% of participating pathologists (N=30)
Our study evaluated interpretive variability among a large number of practicing U.S. pathologists within a spectrum of cases that were also evaluated by a reference panel. The reference panel members also demonstrated substantial variability in their interpretation of FEA; however, overall prevalence of FEA decreased following the consensus review process that included a discussion of diagnostic criteria. This observation suggests that educational interventions may refine understanding of the diagnostic criteria and potentially reduce the diagnostic prevalence. Open discussion and communication between radiologists, pathologists, and breast surgeons is perhaps more important than improving pathologist reproducibility. Our mutual goal is to segregate lesions associated with future risk of developing cancer from lesions associated with current risk for associated aggressive lesions that require early intervention and treatment. FEA and its associated family of indolent lesions, including ADH, ALH, low-grade DCIS, and small well-differentiated or tubular carcinomas are increasingly recognized as lesions that do not pose an immediate threat for women participating in breast screening.
Translating test set evaluation to clinical performance has limitations, and the issues requiring special consideration are described elsewhere.20,23,25 We also noted a difference among participants’ use of the BPATH-Dx form, with most checking multiple boxes, and some selecting a single, highest order diagnosis despite being instructed to check all applicable diagnostic boxes. We do not know how the order of slides within test sets (which was different for each participant), the oversampling of cases with atypia and DCIS, and the use of both excisional and core needle biopsies may have affected diagnoses. Participants tended to diagnose FEA more often on core biopsies, compared with excisional biopsies; however, the sample size was too small to draw any conclusions from this trend.
In summary, our findings show a high degree of variability in the use of FEA as a diagnostic entity among practicing U.S. pathologists and suggest that differences between FEA, CCH, UDH, and ALH should be discussed in greater detail during clinical case review. Our results emphasize the challenges that breast surgeons face when relying on pathologists’ reports and stress the need for cross-discipline understanding of diagnostic variability in potentially precancerous lesions.
Highlights
We observed wide variation in the diagnosis of FEA among U.S. pathologists.
Perceptions of diagnostic criteria and any implied risk for FEA may also vary.
FEA, CCH, UDH, and ALH should be compared in greater detail during case review.
Surgical excision following core biopsy diagnosis of FEA may not be necessary.
Educational interventions may refine understanding, reduce diagnostic variation.
Acknowledgments
This work relied on data from the B-Path study, which was supported by the National Cancer Institute of the National Institutes of Health under award numbers R01 CA140560, U54 CA163303, KO5 CA104699, and R01 CA172343 and by the National Cancer Institute-funded Breast Cancer Surveillance Consortium award number HHSN261201100031C. Laura Samples was supported by the University of Washington, School of Medicine Medical Student Research Training Program. The content is solely the responsibility of the authors and does not necessarily represent the views of the National Cancer Institute or the National Institutes of Health. The collection of cancer and vital status data used in this study was supported in part by several state public health departments and cancer registries throughout the U.S. For a full description of these sources, please see: http://www.breastscreening.cancer.gov/work/acknowledgement.html. We appreciate the time and efforts of all of the pathologists who participated in this study.
Appendix A. BPATH-Dx Histology Form for Data Collection on Each Case Used by Participating Pathologists. Originally published in K Allison et al (2014).19


Appendix B. Participating pathologists’ interpretations of reference FEA cases*
| Case Number | Reference Panel diagnosis** | Core or excisional | N (Practicing Pathologists Interpreting a case) | Number of Pathologists who Agree with the Reference Diagnosis of FEA | If pathologist does not diagnose the case as FEA, what other diagnosis is given? (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alternative Benign (RS, SA, IPW, FA, ALH, NP) | IPA | ADH | DCIS | ||||||||||||
| RS | SA | IPW | FA | ALH | NP | ||||||||||
| 1 | (FEA) | Needle Core | 29 | 15 (52%) | 7 (24%) | 1 (3%) | 3(10%) | 6(21%) | |||||||
| 2 | (FEA) | Needle Core | 29 | 11 (38%) | 20 (69%) | 4 (14%) | 2 (7%) | 1 (3%) | 2 (7%) | 1 (3%) | |||||
| 3 | FEA, CCH | Needle Core | 29 | 10 (34%) | 17 (59%) | 1 (3%) | 4 (14%) | 1 (3%) | 1 (3%) | ||||||
| 4 | FEA, ALH | Excisional | 29 | 8 (28%) | 13 (45%) | 1 (3%) | 2 (7%) | 1 (3%) | 8 (28%) | ||||||
| 5 | (UDH, FEA) | Excisional | 29 | 7 (24%) | 15 (52%) | 10(34%) | 5 (17%) | 5 (17%) | 1 (3%) | 2 (7%) | |||||
| 6 | FEA, UDH, CCH | Excisional | 30 | 5 (17%) | 11 (37%) | 17(57%) | 8 (27%) | 3 (10%) | 1 (3%) | 1 (3%) | 6(20%) | ||||
Diagnostic Category Appreciations: FEA: Flat Epithelial Atypia, CCH: Columnar Cell Hyperplasia, UDH: Usual Ductal Hyperplasia, RS: Radial Scar/Complex Sclerosing lesion, SA: Sclerosing Adenosis, IPW: Intraductal Hyperplasia Without Atypia, FA: Fibroadenoma, ALH: Atypical Lobular Hyperplasia, NP: Non-Proliferative, ADH: Atypical Ductal Hyperplasia, DCIS: Ductal Carcinoma In Situ
Percentages add up to >100% because participants could mark combinations of lesion types for a single case
Parentheses indicate that the case did not go to consensus. When a case did not got to consensus, the reference diagnosis was determined based on which lesions were identified by two or more reference pathologists.
See Figure 2 for a bar graph of data specified in this appendix B.
Footnotes
Author Contributions:
LSS: Participated in study design and implementation. Drafted manuscript. MHR: Participated in study design, analysis, and manuscript preparation. Provided expert pathologist feedback at all stages of the process. PDF: Statistician. Analyzed data, developed figures and tables, provided manuscript feedback. Drafted components of the methods section. KHA: Participated in study design and conception. Provided expert pathologist feedback. Edited manuscript. HDN: Participated in study design, conception and manuscript preparation. TRM: Participated in study design, data collection, data analysis and manuscript preparation. DLW: Participated in overall study design, conception and implementation. Participated in manuscript writing and editing. JGE: Participated in overall study design, conception and implementation. Participated in manuscript writing and editing. All authors read and approved the final manuscript.
Compliance with Ethical Standards
The authors have no conflicts of interest to disclose. All participants provided informed consent.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Ward CJ, VLG Risk Management and Medico-Legal Issues in Breast Cancer. Clin Obstet Gynecol. 2016;59(2):439–446. doi: 10.1097/GRF.0000000000000203. [DOI] [PubMed] [Google Scholar]
- 2.Prowler VL, Joh JE, Acs G, et al. Surgical excision of pure flat epithelial atypia identified on core needle breast biopsy. Breast. 2014;23(4):352–356. doi: 10.1016/j.breast.2014.01.013. [DOI] [PubMed] [Google Scholar]
- 3.Silverstein M. Where's the outrage? J Am Coll Surg. 2009;208(1):78–79. doi: 10.1016/j.jamcollsurg.2008.09.022. [DOI] [PubMed] [Google Scholar]
- 4.Silverstein M, Recht A, Lagios MD, et al. Special report: Consensus conference III. Image-detected breast cancer: state-of-the-art diagnosis and treatment. J Am Coll Surg. 2009;209(4):504–520. doi: 10.1016/j.jamcollsurg.2009.07.006. [DOI] [PubMed] [Google Scholar]
- 5.Tavassoli FA, Devilee P. Pathology and genetics of tumours of the breast and female genital organs. IARC; 2003. [Google Scholar]
- 6.Schnitt SJ, CL, Lakhani SR, Simpson PT, Eusebi V. Flast epithelial atypia. In: Lakhani RD, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ, editors. WHO Classificatoin of Tumours of the Breast. Vol. 87. International Agency for Research on Cancer (IARC); Lyon: 2012. [Google Scholar]
- 7.Ceugnart L, Doualliez V, Chauvet M-P, et al. Pure flat epithelial atypia: is there a place for routine surgery? Diagn Interv Imaging. 2013;94(9):861–869. doi: 10.1016/j.diii.2013.01.011. [DOI] [PubMed] [Google Scholar]
- 8.Mooney KL, Bassett LW, Apple SK. Upgrade rates of high-risk breast lesions diagnosed on core needle biopsy: a single-institution experience and literature review. Mod Pathol. 2016 doi: 10.1038/modpathol.2016.127. [DOI] [PubMed] [Google Scholar]
- 9.Rageth CJ, O'Flynn EA, Comstock C, et al. First International Consensus Conference on lesions of uncertain malignant potential in the breast (B3 lesions) Breast Cancer Res Treat. 2016;159(2):203–213. doi: 10.1007/s10549-016-3935-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Said SM, Visscher DW, Nassar A, et al. Flat epithelial atypia and risk of breast cancer: A Mayo cohort study. Cancer. 2015;121(10):1548–1555. doi: 10.1002/cncr.29243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Schnitt SJ. Benign breast disease and breast cancer risk: morphology and beyond. Am J Surg Pathol. 2003;27(6):836–841. doi: 10.1097/00000478-200306000-00017. [DOI] [PubMed] [Google Scholar]
- 12.Sohn V, Porta R, Brown T. Flat epithelial atypia of the breast on core needle biopsy: an indication for surgical excision. Mil Med. 2011;176(11):1347–1350. doi: 10.7205/milmed-d-11-00088. [DOI] [PubMed] [Google Scholar]
- 13.Biggar M. Columnar cell change with atypia (flat epithelial atypia) on breast core biopsy–Outcomes following open excision. ANZ J Surg. 2013;83(1):7–16. doi: 10.1111/tbj.12039. [DOI] [PubMed] [Google Scholar]
- 14.Fraser JL, Raza S, Chorny K, Connolly JL, Schnitt SJ. Columnar alteration with prominent apical snouts and secretions: a spectrum of changes frequently present in breast biopsies performed for microcalcifications. Am J Surg Pathol. 1998;22(12):1521–1527. doi: 10.1097/00000478-199812000-00009. [DOI] [PubMed] [Google Scholar]
- 15.Goldstein NS, O'Malley BA. Cancerization of small ectatic ducts of the breast by ductal carcinoma in situ cells with apocrine snouts: a lesion associated with tubular carcinoma. Am J Clin Pathol. 1997;107(5):561–566. doi: 10.1093/ajcp/107.5.561. [DOI] [PubMed] [Google Scholar]
- 16.Calhoun BC. Management of flat epithelial atypia on breast core biopsy may be individualized based on correlation with imaging studies. Mod Pathol. 2014 doi: 10.1038/modpathol.2014.159. [DOI] [PubMed] [Google Scholar]
- 17.Saladin C, Haueisen H, Kampmann G, et al. Lesions with unclear malignant potential (B3) after minimally invasive breast biopsy: evaluation of vacuum biopsies performed in Switzerland and recommended further management. Acta Radiol. 2016;57(7):815–821. doi: 10.1177/0284185115610931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Uzoaru I, Morgan BR, Liu ZG, et al. Flat epithelial atypia with and without atypical ductal hyperplasia: to re-excise or not. Results of a 5-year prospective study. Virchows Arch. 2012;461(4):419–423. doi: 10.1007/s00428-012-1312-1. [DOI] [PubMed] [Google Scholar]
- 19.Yu CC, Ueng SH, Cheung YC, et al. Predictors of underestimation of malignancy after image-guided core needle biopsy diagnosis of flat epithelial atypia or atypical ductal hyperplasia. Breast J. 2015;21(3):224–232. doi: 10.1111/tbj.12389. [DOI] [PubMed] [Google Scholar]
- 20.Elmore JG, Longton G, Carney PA, et al. Diagnostic Concordance Among Pathologists Interpreting Breast Biopsy Specimens. JAMA. 2015;313(11):1122–1132. doi: 10.1001/jama.2015.1405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Elmore JG, Nelson HD, Pepe MS, et al. Variability in Pathologists' Interpretations of Individual Breast Biopsy Slides: A Population Perspective. Ann Intern Med. 2016;164(10):649–655. doi: 10.7326/M15-0964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Feng S, Weaver DL, Carney PA, et al. A framework for evaluating diagnostic discordance in pathology discovered during research studies. Arch Pathol Lab Med. 2014;138(7):955–961. doi: 10.5858/arpa.2013-0263-OA. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Oster NV, Carney PA, Allison KH, et al. Development of a diagnostic test set to assess agreement in breast pathology: practical application of the Guidelines for Reporting Reliability and Agreement Studies (GRRAS) BMC Womens Health. 2013;13(1):3. doi: 10.1186/1472-6874-13-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Breast Cancer Surveillance Consortium. [Accessed March 27, 2017];2016 http://www.bcsc-research.org/
- 25.Allison KH, Reisch LM, Carney PA, et al. Understanding diagnostic variability in breast pathology: lessons learned from an expert consensus review panel. Histopathology. 2014;65(2):240–251. doi: 10.1111/his.12387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Dupont WD, Page DL. Risk factors for breast cancer in women with proliferative breast disease. N Engl J Med. 1985;312(3):146–151. doi: 10.1056/NEJM198501173120303. [DOI] [PubMed] [Google Scholar]
- 27.Lakhani SR Cancer IAfRo, Organization WH. WHO classification of tumours of the breast. International Agency for Research on Cancer; 2012. [Google Scholar]
- 28.Brem RF, Lechner MC, Jackman RJ, et al. Lobular neoplasia at percutaneous breast biopsy: Variables associated with carcinoma at surgical excision. AJR Am J Roentgenol. 2008;190(3):637–641. doi: 10.2214/AJR.07.2768. [DOI] [PubMed] [Google Scholar]
- 29.Cangiarella J, Guth A, Axelrod D, et al. Is surgical excision necessary for the management of atypical lobular hyperplasia and lobular carcinoma in situ diagnosed on core needle biopsy?: a report of 38 cases and review of the literature. Arch Pathol Lab Med. 2008;132(6):979–983. doi: 10.5858/2008-132-979-ISENFT. [DOI] [PubMed] [Google Scholar]
- 30.Crisi GM, Mandavilli S, Cronin E, Ricci A., Jr Invasive mammary carcinoma after immediate and short-term follow-up for lobular neoplasia on core biopsy. Am J Surg Pathol. 2003;27(3):325–333. doi: 10.1097/00000478-200303000-00005. [DOI] [PubMed] [Google Scholar]
- 31.Esserman LE, Lamea L, Tanev S, Poppiti R. Should the extent of lobular neoplasia on core biopsy influence the decision for excision? Breast J. 2007;13(1):55–61. doi: 10.1111/j.1524-4741.2006.00363.x. [DOI] [PubMed] [Google Scholar]
- 32.Hwang H, Barke LD, Mendelson EB, Susnik B. Atypical lobular hyperplasia and classic lobular carcinoma in situ in core biopsy specimens: routine excision is not necessary. Mod Pathol. 2008;21(10):1208–1216. doi: 10.1038/modpathol.2008.134. [DOI] [PubMed] [Google Scholar]
- 33.Menon S, Porter GJ, Evans AJ, et al. The significance of lobular neoplasia on needle core biopsy of the breast. Virchows Arch. 2008;452(5):473–479. doi: 10.1007/s00428-008-0607-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Rendi MH, Dintzis SM, Lehman CD, Calhoun KE, Allison KH. Lobular In-Situ Neoplasia on Breast Core Needle Biopsy: Imaging Indication and Pathologic Extent Can Identify Which Patients Require Excisional Biopsy. Ann Surg Oncol. 2012;19(3):914–921. doi: 10.1245/s10434-011-2034-3. [DOI] [PubMed] [Google Scholar]
- 35.Chae BJ, Lee A, Song BJ, Jung SS. Predictive factors for breast cancer in patients diagnosed atypical ductal hyperplasia at core needle biopsy. World J Surg Oncol. 2009;7:77. doi: 10.1186/1477-7819-7-77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hartmann LC, Degnim AC, Santen RJ, Dupont WD, Ghosh K. Atypical Hyperplasia of the Breast — Risk Assessment and Management Options. N Engl J Med. 2015;372(1):78–89. doi: 10.1056/NEJMsr1407164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Verschuur-Maes AH, van Deurzen CH, Monninkhof EM, van Diest PJ. Columnar Cell Lesions on Breast Needle Biopsies: Is Surgical Excision Necessary?: A Systematic Review. Ann Surg. 2012;255(2):259–265. doi: 10.1097/SLA.0b013e318233523f. [DOI] [PubMed] [Google Scholar]
- 38.Boulos FI, Dupont WD, Simpson JF, et al. Histologic associations and long-term cancer risk in columnar cell lesions of the breast: a retrospective cohort and a nested case-control study. Cancer. 2008;113(9):2415–2421. doi: 10.1002/cncr.23873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Khoumais NA, Scaranelo AM, Moshonov H, et al. Incidence of Breast Cancer in Patients with Pure Flat Epithelial Atypia Diagnosed at Core-Needle Biopsy of the Breast. Ann Surg Oncol. 2013;20(1):133–138. doi: 10.1245/s10434-012-2591-0. [DOI] [PubMed] [Google Scholar]
- 40.Neal L, Sandhu NP, Hieken TJ, et al. Diagnosis and management of benign, atypical, and indeterminate breast lesions detected on core needle biopsy. Mayo Clin Proc. 2014;89(4):536–547. doi: 10.1016/j.mayocp.2014.02.004. [DOI] [PubMed] [Google Scholar]
- 41.Gomes DS, Porto SS, Balabram D, Gobbi H. Inter-observer variability between general pathologists and a specialist in breast pathology in the diagnosis of lobular neoplasia, columnar cell lesions, atypical ductal hyperplasia and ductal carcinoma in situ of the breast. Diagn Pathol. 2014;9:121. doi: 10.1186/1746-1596-9-121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Haupt B, Schwartz MR, Xu QS, Ro JY. Columnar cell lesions: a consensus study among pathology trainees. Hum Pathol. 2010;41(6):895–901. doi: 10.1016/j.humpath.2009.12.003. [DOI] [PubMed] [Google Scholar]
- 43.O'Malley FP, Mohsin SK, Badve S, et al. Interobserver reproducibility in the diagnosis of flat epithelial atypia of the breast. Mod Pathol. 2006;19(2):172–179. doi: 10.1038/modpathol.3800514. [DOI] [PubMed] [Google Scholar]