

Abstract
Background
Obstructive sleep apnea (OSA) is a highly prevalent condition, especially in obese children, and has been associated with increased risk for endothelial dysfunction and dislipidemia, which are precursors of atherosclerosis. Lipoprotein‐associated phospholipase A2 (Lp‐PLA2) is recognized as an independent risk factor for cardiovascular risk and atheromatous plaque activity. We hypothesized that Lp‐PLA2 levels would be elevated in children with OSA, particularly among obese children who also manifest evidence of endothelial dysfunction.
Methods and Results
One hundred sixty children (mean age 7.1±2.3 years), either nonobese with (n=40) and without OSA (n=40) or obese with (n=40) and without OSA (n=40) underwent overnight polysomnographic and postocclusive reperfusion evaluation and a fasting blood draw the morning after the sleep study. In addition to lipid profile, Lp‐PLA2 plasma activity was assessed using a commercial kit. Obese children and OSA children had significantly elevated plasma Lp‐PLA2 activity levels compared to controls. Furthermore, when both obesity and OSA were concurrently present or when endothelial function was present, Lp‐PLA2 activity was higher. Treatment of OSA by adenotonsillectomy resulted in reductions of Lp‐PLA2 activity (n=37; P<0.001).
Conclusions
Lp‐PLA2 plasma activity is increased in pediatric OSA and obesity, particularly when endothelial dysfunction is present, and exhibits decreases on OSA treatment. The short‐term and long‐term significance of these findings in relation to cardiovascular risk remain undefined.
Keywords: atherosclerosis, cholesterol, endothelial dysfunction, sleep apnea
Subject Categories: Atherosclerosis, Pediatrics, Endothelium/Vascular Type/Nitric Oxide, Biomarkers, Lipids and Cholesterol
Introduction
The increases in childhood obesity prevalence rates have now been reported globally and are currently viewed as both major short‐term and long‐term health hazards1, 2 due to the generation of a systemic inflammatory and oxidative stress burden.3, 4 However, the large variance in morbidity among overweight‐obese children suggests the need for biomarkers that identify the specific risk of any given child for cardiovascular morbidity.5, 6, 7
Obstructive sleep apnea (OSA) is also a highly prevalent condition in children, affecting up to 3% to 4% of all children.8 Children with OSA exhibit a highly collapsible upper airway that will lead to episodes of partial or complete airway obstruction during sleep, resulting in increased intrathoracic pressure swings and recurrent arousals as well as episodic oxyhemoglobin desaturations and elevations in carbon dioxide.9 The cumulative evidence derived from a large number of studies has further suggested that OSA is independently associated with increased inflammation and daytime somnolence,10, 11, 12 altered lipid homeostasis, and cardiovascular morbidity, including systemic and pulmonary vascular hypertension, left ventricular alterations in geometry and contractibility, as well as endothelial dysfunction.13, 14, 15 However, as in obese children, not every child suffering from OSA will manifest evidence of cardiovascular morbidity, even if the frequency of endothelial dysfunction increases with corresponding increases in OSA severity, particularly when obesity is concurrently present.16
Lipoprotein‐associated phospholipase A2 (Lp‐PLA2) is a calcium‐independent lipase primarily produced by monocytes and macrophages that catalyzes the hydrolysis of the sn‐2 acyl chain of the phospholipid substrates on the surface of low‐density lipoproteins, releasing lysophosphatidylcholine and oxidized fatty acids.17, 18 Lp‐PLA2 is recognized as an independent risk factor for cardiovascular disease (CVD) and atheromatous plaque activity in the general population,19 and elevations of Lp‐PLA2 have also been reported in children at significant CVD risk,20, 21 including obese children.22 However, the impact of OSA on Lp‐PLA2 activity has not been examined to date and could constitute a potential indicator for CVD risk in this patient population.
We hypothesized that OSA in children would be associated with increased plasma activity levels of Lp‐PLA2, particularly when concurrent obesity and endothelial dysfunction are present.
Materials and Methods
The research protocol was approved by the University of Chicago (protocol 09‐115‐B) human research ethics committee. Informed consent was obtained from the parents, and age appropriate assent was also obtained from the children. Children 4 to 11 years of age were recruited from the Sleep and ENT clinics at Comer Children's Hospital at the University of Chicago as well as by advertisement in the community. Children found to be hypertensive or using antihypertensive drug therapies were excluded (n=8). Furthermore, children with diabetes (fasting serum glucose ≥120 mg/dL; n=13), with a craniofacial, neuromuscular, or defined genetic syndrome, and children on chronic anti‐inflammatory therapy (n=14) or with any known acute or chronic illness were also excluded. In addition, children placed on sympathomimetic agents such as psychostimulants were not tested (n=21).
Overnight Polysomnographic Studies
All children underwent standard nocturnal polysomnography evaluation as previously described,23 with assessment of 8 standard EEG channels, bilateral EOG, EMG, 2‐lead ECG, oronasal airflow measurement using thermistor, nasal pressure transducer, end‐tidal CO2, chest and abdominal movement by respiratory inductance plethysmography, and pulse oximetry including pulse waveform using a commercially available data acquisition system (Polysmith; Nihon Kohden America Inc, Irvine, CA). The nocturnal polysomnography studies were scored as per the 2012 American Association of Sleep Medicine revised guidelines for the scoring of sleep and associated events.24 The proportion of time spent in each stage of sleep was calculated as a percentage of total sleep time (TST). A respiratory event was scored as an obstructive apnea if it was associated with a >90% fall in signal amplitude for >90% of the entire event compared to the baseline amplitude, the event lasted for at least 2 breaths, and there was continued or increased respiratory effort throughout the period of the event. A mixed apnea was scored if there was absent inspiratory effort in the initial part of the event, followed by resumption of inspiratory effort before the end of the event. A central apnea was scored if there was absent respiratory effort throughout the duration of the event, the event lasted for at least 2 missed breaths, and it was associated with an arousal/awakening or a ≥3% desaturation. A hypopnea was scored if the event was associated with a ≥50% fall in amplitude of the nasal pressure transducer, lasted for at least 2 breaths, and was associated with an arousal/awakening or ≥3% desaturation. The obstructive apnea‐hypopnea index (AHI) was calculated as the number of apneas and hypopneas per hour of TST. Arousals were classified as either spontaneous or respiratory, and corresponding indices were computed.
The diagnosis of OSA was defined by the presence of an AHI ≥1 per hour of TST. Control children were nonobese children who had AHI <1/hour of TST.
Endothelial Function Measurements
Endothelial function was assessed in a fasted state in the morning, using the hyperemic test after cuff‐induced occlusion of wrist arteries, as previously described.16, 25 In brief, a laser Doppler sensor (Periflux 5000 System; Perimed, Järfälla, Sweden) was placed over the volar aspect of the hand at the first finger distal metacarpal surface, and the hand was secured and immobilized.26 Once cutaneous blood flow readings became stable, a cuff placed at the forearm and connected to a computer‐controller was inflated to suprasystolic pressures, and blood flow signal declined to undetectable levels. The cuff was rapidly deflated, and the laser Doppler measured hyperemic responses. The time to maximal regional blood flow after occlusion release (Tmax) is representative of the postocclusion hyperemic response, an index of NO‐dependent endothelial function.27 A Tmax >45 seconds was considered as indicative of abnormal endothelial function28, 29 and represents 3 standard deviations above the mean. The intraobserver and interobserver variability of the test have been previously examined and are 8.9% and 13.8%, respectively.29
According to our recruitment strategies, 4 distinctly different groups of children were identified: Controls (CO), who were nonobese and either nonsnoring or snoring children with normal polysomnographic tests; obese children (OB), ie, BMI z‐score ≥1.65 with either normal polysomnographic tests or evidence of OSA; and nonobese snoring children with abnormal polysomnographic findings confirming the presence of OSA.
Plasma Assays
Blood samples were drawn into either EDTA‐containing tubes (purple top) or tubes without any additive. Samples were centrifuged within 30 minutes at 3000g for 10 minutes, and plasma was separated and either analyzed immediately or kept at −80°C. Levels of lipids including total cholesterol, high‐density lipoprotein (HDL) cholesterol, calculated low‐density lipoprotein (LDL) cholesterol, and triglycerides were assessed with a Flex reagent cartridge (Date Behring, Newark, DE). In addition, plasma samples were frozen at −80°C until assay. Plasma high‐sensitivity C‐reactive protein (hsCRP) was measured using a high‐sensitivity immunonephelometric method with a lowest detection limit of 0.0175 mg/dL (N High Sensitivity CRP; Dade Behring, Marburg, Germany).
Lp‐PLA2 Activity Assay
Plasma Lp‐PLA2 activity levels were assessed in duplicate using a commercially available kit (PLAQPRO™ Lp‐PLA2 Assay; Enzo, New York, NY; cat # ENZ‐KIT179‐0200). The assay is predicated on a colorimetric readout enzyme activity assay. During the test, Lp‐PLA2 in plasma samples hydrolyzed the SN2 position of the substrate, 1‐myristoyl‐2‐(4‐nitrophenylsuccinyl)‐phosphatidylcholine. The resulting colored reaction product, 4‐nitrophenol, is measured spectrophotometrically, and the rate of formation of 4‐nitrophenol is determined over successive time‐constrained measurements. The assay kit includes five Lp‐PLA2 calibrators for use in generating a standard curve fit of change in absorbance versus Lp‐PLA2 activity level in nanomoles per minute per milliliter. The activity of Lp‐PLA2 in subject samples is then interpolated from the standard calibration curve. The sensitivity of the assay was determined at 0.24 nmol/(min·mL); the intra‐assay variability of the assay was 8%, and the interassay variability was 12%.
Statistical Analysis
All analyses were conducted using SPSS software (version 21.0; SPPS Inc, Chicago, IL), and data are presented as mean±SD. The children were subdivided into 4 groups, based on the presence or absence of obesity (ie, BMI z‐score >1.65) and OSA. A priori assumptions on the presence of differences in Lp‐PLA2 activity levels between children with and without OSA were formulated such as to allow for 80% power and a 2‐sided confidence level at 0.01 and indicated the need for 90 to 120 subjects in the cohort. Significant differences between groups were analyzed using 2‐way analysis of variance. If the data were not normally distributed, they were logarithmically transformed. Pearson correlation analyses and linear stepwise regression analyses were conducted to examine potential associations between BMI z‐score, sleep variables, lipid profiles, hsCRP, Tmax, and Lp‐PLA2 plasma activity levels. All P‐values reported are 2‐tailed with statistical significance set at <0.05.
Results
A total of 196 children fulfilling entry criteria completed the overnight polysomnographic evaluation, underwent endothelial function testing, and provided a fasting blood sample after the sleep study. To allow for identical subgroup cohort sizes, children were prospectively and consecutively recruited into each of the 4 categorical groups, until a total of 40 children was reached (total recruitments were as follows: nonobese children without OSA 41; nonobese children with OSA 48; obese children without OSA 40; obese children with OSA, 67). In addition, a total of 32 children refused to participate in the study (7 parents declined to participate altogether, and 25 parents were not willing to participate in the blood draw portion of the study). The demographic, anthropometric, and polysomnographic characteristics of these 32 children were similar to those of the cohort, which are shown in Table 1.
Table 1.
General Characteristics of Obese and Nonobese Children With and Without OSA
| Obese, No OSA (n=40) | Obese, OSA (n=40) | Nonobese, No OSA (n=40) | Nonobese, OSA (n=40) | |
|---|---|---|---|---|
| Age, y | 7.6±2.2 | 7.3±2.1 | 7.1±1.9 | 6.9±2.4 |
| Sex (male), % | 55.0 | 57.5 | 50.0 | 55.0 |
| Race (white), n | 6 | 6 | 12 | 10 |
| BMI z‐score | 2.28±0.11 | 2.37±0.42 | 0.21±0.80 | 0.07±0.88 |
| Systolic blood pressure, mm Hg | 115.1±9.4 | 122.2±9.6* | 106.8±8.7 | 111.8±8.6* |
| Diastolic blood pressure, mm Hg | 69.1±7.7 | 70.1±8.5* | 65.2±7.5 | 68.4±7.9 |
| Obstructive AHI, events/h | 0.91±0.22 | 18.3±14.6 | 0.48±0.30 | 18.3±13.6 |
| SpO2 nadir, % | 93.1±3.6 | 81.4±11.1 | 92.4±4.3 | 81.7±10.4 |
| Respiratory arousal index | 2.4±3.3 | 13.5±12.6 | 92.4±4.3 | 13.6±10.6 |
| LDL cholesterol, mg/dL | 91.1±24.9 | 101.5±26.2* | 85.7±15.1 | 91.9±19.7* |
| HDL cholesterol, mg/dL | 50.4±13.3 | 48.8±10.4 | 63.4±10.6 | 49.9±9.4* |
| Triglycerides, mg/dL | 90.7±50.2 | 96.0±48.9 | 74.8±32.3 | 75.5±31.1 |
| hsCRP, mg/L | 0.48±0.21 | 1.08±0.71* | 0.18±0.24 | 0.68±0.51* |
| Time to maximal hyperemic responses (Tmax), s | 40.5±8.5 | 49.5±8.8* | 29.9±6.5 | 42.1±9.6* |
| ED, n (%) | 6 (15%) | 26 (65%)* | 0 (0%) | 9 (22.5%)* |
| Lp‐PLA2 plasma activity, nmol/(min·mL) | 183.1±82.5 | 332.2±96.6* | 131.1±25.0 | 194.6±98.5* |
| Lp‐PLA2 plasma activity if ED present, nmol/(min·mL) | 334.7±47.2 | 390.4±64.5 | — | 338.2±93.8 |
| Lp‐PLA2 plasma activity if ED not present, nmol/(min·mL) | 156.3±52.7 | 224.1±26.0* | 131.1±25.0 | 152.8±47.7* |
BMI indicates body mass index; ED, endothelial dysfunction; HDL, high‐density lipid cholesterol; LDL, low‐density lipid cholesterol; Lp‐PLA2, lipoprotein‐associated phospholipase A2; SpO2, peripheral capillary oxygen saturation.
OSA vs no‐OSA: *P<0.05; ED=Tmax >45 s.
In general, there were no significant differences in age, sex, or ethnicity across the 4 subgroups. Primary sleep disturbance measures clinically used to characterize the severity of OSA were not significantly different in obese and nonobese children with OSA. Similarly, there were no differences in sleep measures in obese and nonobese children without OSA (Table 1).
However, obese children exhibited significantly higher BMI z‐scores and serum lipids and lower HDL cholesterol levels as well as higher hsCRP levels (Table 1). Similarly, children with OSA had significantly higher LDL cholesterol and lower HDL cholesterol levels as well as increased hsCRP (Table 1).
Plasma Lp‐PLA2 activity levels were significantly higher in obese children without OSA (183.1±82.5 nmol/[min·mL]) compared with non‐obese children without OSA (131.1±25.0 nmol/[min·mL], P<0.001). Lp‐PLA2 activity levels were significantly correlated with the BMI z score (r2 0.11; P<0.001; Figure 1), as well as with hsCRP (r 0.197; P<0.02). Nonobese and obese children with OSA exhibited increased Lp‐PLA2 activity levels compared to corresponding controls (Table 1). Furthermore, a significant linear correlation emerged between AHI and Lp‐PLA2 activity levels (r2 0.22; P=0.001; Figure 1). BMI z‐score, AHI, and hsCRP were also significantly associated with Tmax values (r2 0.09; P<0.001, r2 0.23; P<0.001, and r2 0.14; P<0.01, respectively; Figure 1). However, a remarkably strong association emerged between Tmax and Lp‐PLA2 activity (r2 0.70; P<0.001; Figure 1), whereas no significant associations were detected between LDL or HDL cholesterol or triglyceride concentrations and Tmax, Lp‐PLA2 activity, AHI, or BMI z‐scores. Notably, Lp‐PLA2 activity was markedly increased in all subjects with evidence of endothelial dysfunction (Table 1).
Figure 1.
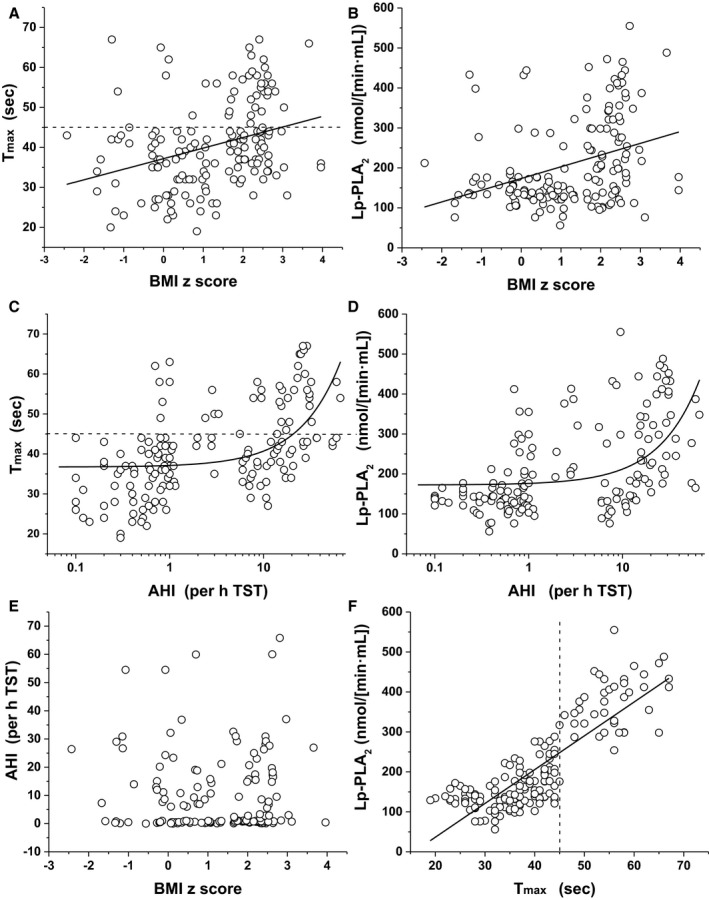
Scatterplots of Lp‐PLA2 plasma activity levels, BMI z‐score, obstructive apnea hypopnea index (AHI), and Tmax in children with and without obesity or OSA. A, Tmax vs BMI z‐score: r=0.319, P<0.001. B, Lp‐PLA2 vs BMI z‐score: r=0.350, P<0.001. C, Tmax vs AHI: r=0.489, P<0.001. D, Lp‐PLA2 vs AHI: r=0.483, P<0.001. E, AHI vs BMI z‐score, not significant. F, Lp‐PLA2 vs Tmax: r=0.837, P<0.001. Actual values rather than log‐transformed values were used in the linear fitting functions shown. AHI is displayed as log scale (C and D). Dotted lines indicate the cutoff used to define endothelial dysfunction, ie, Tmax >45 seconds. AHI indicates apnea hypopnea index; BMI, body mass index; Lp‐PLA 2, lipoprotein‐associated phospholipase A2; Tmax, time to peak reperfusion; TST, total sleep time.
To further explore independent predictors of Tmax, we performed stepwise multiple regression analyses with age, sex, ethnicity, and BMI z‐score included as potential confounders. In model 1 (adjusted only for age, race, and sex), BMI z‐score, AHI, peripheral capillary oxygen saturation (SpO2) nadir, respiratory arousal indices, hsCRP, and Lp‐PLA2 activity were independently associated with Tmax (Table 2, P<0.001). In model 2 (adjusted for age, race, sex, and BMI z‐score), AHI, SpO2 nadir, respiratory arousal indices, hsCRP, and Lp‐PLA2 activity accounted for 12.7%, 10.7%, 6.1%, 3.8%, and 48.9% of the variance in Tmax, respectively. In addition, in the context of iterative variations on model 2, BMI z‐score contributed ~15.6% of the variance in Tmax after adjusting for age, sex, race, and sleep measures (Table 2), and hsCRP contributed a small, albeit significant, proportion (5.2%). However, when Lp‐PLA2 activity was included in the model, the association between Tmax and any other variable was markedly weakened and did not achieve statistical significance (standardized coefficient: 0.047; P>0.05). Based on the various iterative models described above, we used the residuals from these models in the comprehensive model aiming to establish the adjusted association between Tmax and OSA polysomnographic severity measures while adjusting for all other potential confounders and accounting for the interdependencies between BMI z‐score and other variables such as Lp‐PLA2 activity. In this comprehensive and adjusted model (model 3), which incorporates multiple risk factors, OSA severity accounted for 22% of the variance in Tmax (standardized coefficient: 0.243; P<0.001), with BMI z‐score accounting for 12% of the variance (standardized coefficient 0.117; P<0.01), and hsCRP did not contribute significantly to the variance in Tmax. There were no apparent interactions in the fully adjusted model between OSA and BMI z‐score severity on Tmax.
Table 2.
Multivariate Regression Analyses Among Sleep Measures, Lp‐PLA2 Activity, and Tmax Values in 160 Children
| Variables | Tmax | |
|---|---|---|
| Standardized Coefficients | P Value | |
| Age | 0.007 | 0.904 |
| Sex | 0.004 | 0.975 |
| Race | 0.002 | 0.972 |
| BMI z‐score | 0.118 | <0.01 |
| AHIa | 0.127 | <0.001 |
| SpO2 nadir | 0.108 | <0.01 |
| Respiratory arousal indexa | 0.068 | <0.05 |
| LDL cholesterol | 0.036 | 0.423 |
| HDL cholesterol | 0.057 | 0.217 |
| hsCRP | 0.147 | <0.01 |
| Lp‐PLA2 activitya | 0.489 | <0.00001 |
AHI indicates obstructive apnea‐hypopnea index; HDL, high‐density lipid cholesterol; hsCRP, high‐sensitivity C‐reactive protein; LDL, low‐density lipid cholesterol; Lp‐PLA2, lipoprotein‐associated phospholipase A2; SpO2, peripheral capillary oxygen saturation.
Data were log‐transformed. Data for age, sex, and race are not adjusted. Data for BMI z‐score are shown after adjusting for age, race, and gender only. All other data are shown after controlling for age, sex, race, and BMI z‐score.
A subset of 37 children (21 obese) who underwent adenotonsillectomy (T&A) as part of their treatment for the underlying sleep‐disordered breathing underwent a follow‐up overnight sleep study and Lp‐PLA2 activity assessments within 4 to 6 months after surgery. In 14 of these children, endothelial function was also evaluated. AHI decreased from 12.6±3.9 per hour TST before treatment to 3.6±2.6 per hour TST following T&A (P<0.001; Figure 2). In parallel, significant reductions in Lp‐PLA2 activity levels occurred (pre‐T&A 221.3±116.4 nmol/[min·mL] vs post‐T&A 140.1±35.0 nmol/[min·mL]; P<0.001; Figure 2), with overall improvements in Tmax being apparent among the 14 children tested (pre‐T&A 43.4±9.3 seconds vs post‐T&A 36.2±4.6 seconds; P<0.001; Figure 2).
Figure 2.
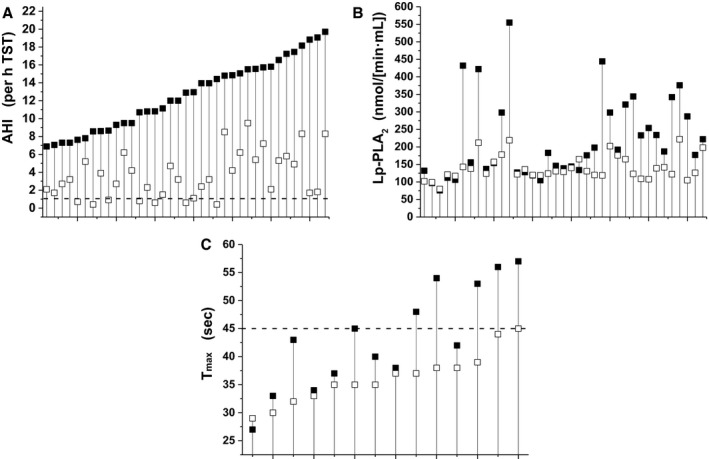
Individual changes in AHI (A), Lp‐PLA2 (B) and Tmax (C) before and after adenotonsillectomy. AHI indicates apnea hypopnea index; Lp‐PLA2, lipoprotein‐associated phospholipase A2; Tmax, time to peak reperfusion.
Discussion
This study shows that both obese children with and without OSA and nonobese children with OSA are at risk for increased Lp‐PLA2 activity when compared to nonobese children without OSA and that a very strong association is present between Lp‐PLA2 plasma activity levels and Tmax values. In addition, significant, albeit weaker, associations emerged between Lp‐PLA2 activity and BMI z‐scores as well as with the 3 major polysomnographic measures traditionally used to characterize OSA, namely AHI, SpO2 nadir, and respiratory arousal index. Furthermore, reduction in AHI consequent to T&A resulted in improved Tmax and reductions in Lp‐PLA2. Taken together, these findings suggest that assessment of plasma Lp‐PLA2 activity levels may provide a reliable biomarker for children at risk for atherosclerosis, ie, when obesity or OSA is present.
Several methodological considerations deserve mention. First, in the context of the prospective recruitment protocol, careful standardization of fasting blood sampling procedures after the overnight sleep study should dispel any concerns about potential circadian variability in Lp‐PLA2 activity because all samples were obtained at the same time. Furthermore, overall sleep duration in the night preceding the blood sample was available from the polysomnogram, and no major differences were apparent across the 4 subgroups. Second, Lp‐PLA2 activity assays were all performed concomitantly, which should reduce assay variability. We opted for Lp‐PLA2 activity because such assessment has been viewed as superior to the measurement of Lp‐PLA2 concentrations in plasma, which are apparently fraught with both pre‐ and postanalytical problems.30
In the context of cardiovascular morbidity associated with OSA or obesity, our findings corroborate those of previous studies, whereby significant, albeit small, increments in systemic blood pressure are detectable in children with either of these 2 conditions.31, 32, 33, 34, 35, 36, 37, 38 Furthermore, current results confirm the increased frequency of children with abnormal endothelial function, particularly when obesity and OSA are concurrently present.25, 39, 40, 41 The concept that delayed postocclusive hyperemic responses represent alterations in endothelial integrity and attest to the incipient processes involved in atherogenesis has gained widespread acceptance as providing a valid and reliable indication of risk for cardiovascular disease.
Endothelial dysfunction has now been repeatedly reported in both adult and pediatric patients with OSA. The bioavailability of nitric oxide is a critical component underlying the adequacy of the postocclusive hyperemic responses,27 and the presence of activated endothelium by proatherogenic factors such as LDL cholesterol is key in promoting atherosclerosis induction and progression. The vast majority of Lp‐PLA2 circulates bound to LDL cholesterol, with the remainder being bound to HDL cholesterol and remnant lipoprotein particles. When an LDL particle enters the intimal space, it may be oxidized by several enzymes, at which stage Lp‐PLA2 begins to hydrolyze oxidized phospholipid (oxPL) on the LDL particles, forming some of the major molecular triggers of the inflammation cascade, namely oxidized fatty acids and lysophosphatidylcholine. Oxidized fatty acids and lysophosphatidylcholine stimulate expression of adhesion molecules and inflammatory cytokines by endothelial cells, promoting the adhesion and migration monocytes/macrophages to the subendothelial space where they become activated and transform into foam cell macrophages.42 Evidence for some of these events has been previously reported in pediatric OSA, further attesting to the systemic and widespread impact of the disease on the vasculature.43, 44, 45 Furthermore, Lp‐PLA2 activity can also directly decrease the ability of the endothelium to generate nitric oxide.46 Thus, Lp‐PLA2 plasma activity levels as reported in the children with OSA may in fact provide a reliable indicator of the presence or absence of reduced nitric oxide bioavailability in the endothelium, an important correlate of disrupted vascular integrity, or even suggest the presence of atherosclerotic processes and local inflammation in the vascular system. We therefore view the significant reductions in Lp‐PLA2 activity with treatment of OSA as indicative of reversibility of the aforementioned processes, particularly in view of the strong associations between Lp‐PLA2 activity and Tmax, and also the parallel improvements in Tmax and Lp‐PLA2 activity, especially among those with pre‐T&A evidence of endothelial dysfunction. However, we should also remark that our study does not elucidate why some children exhibit reductions in endothelial function while others do not despite the presence of OSA or obesity of similar severity. Furthermore, we cannot infer whether Lp‐PLA2 activity levels reflect a mechanism involved in Tmax changes or simply represent a correlate of Tmax. We hypothesize that based on the known biological activity of Lp‐PLA2, both obesity and OSA may induce increases in Lp‐PLA2 activity that, in turn, adversely affects endothelial integrity.47 In this context we should emphasize that significant associations between Lp‐PLA2 and endothelial function, as measured by flow‐mediated vasodilation in adults, have not been consistently identified.48, 49, 50 Indeed, Garg and colleagues reported no evidence of such association in a large cohort of adult subjects participating in the Multi‐Ethnic Study of Atherosclerosis.50 However, the same group reported more recently that Lp‐PLA2 was positively associated with cardiovascular disease risk, irrespective of the presence or absence of coronary artery calcium or of carotid‐intima‐media thickening in the Multi‐Ethnic Study of Atherosclerosis cohort.51 Notwithstanding such discrepant findings, the remarkably strong association between Lp‐PLA2 and Tmax in our pediatric cohort as well as the decreases in Lp‐PLA2 following treatment of OSA suggest that the signal to noise regarding the putative link between Lp‐PLA2 and endothelial function is substantially higher, probably due to the absence of coexisting confounders in the pediatric age range. Furthermore, differences in the actual information provided by flow‐mediated vasodilation (ie, macrovascular) and Tmax (microvascular) may also account for some of such discrepancies between children and adults.26
In addition to genetic variability in a wide range of genes and pathways pathogenetically involved in atherosclerosis,52, 53 we note that obese children with OSA are more likely to consume fat‐rich and energy‐dense items in their diets that may further predispose them to generation of an adverse vascular milieu.12, 54 The previously observed increases in circulating LDL cholesterol levels and reciprocal decreases in HDL cholesterol in OSA children and obese children,55, 56 which were also documented in the present study, would further support this assumption and potentially explain some of the variance in both Tmax and Lp‐PLA2 levels in the cohort.
In summary, we have shown that both obesity and OSA in children lead to increases in plasma activity levels of Lp‐PLA2 and that the latter are strongly associated with measures of endothelial function. These findings may afford clinical diagnostic opportunities by taking advantage of LP‐PLA2 as a biomarker of underlying atherosclerosis and vascular dysfunction in children and could potentially enable risk‐reduction interventions targeting LP‐PLA2.
Sources of Funding
This work was supported by NIH grants HL65270 and HL130984.
Disclosures
None.
(J Am Heart Assoc. 2017;6:e004923. DOI: 10.1161/JAHA.116.004923.)
References
- 1. Lakshman R, Elks CE, Ong KK. Childhood obesity. Circulation. 2012;126:1770–1779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Katzmarzyk PT, Shen W, Baxter‐Jones A, Bell JD, Butte NF, Demerath EW, Gilsanz V, Goran MI, Hirschler V, Hu HH, Maffeis C, Malina RM, Müller MJ, Pietrobelli A, Wells JC. Adiposity in children and adolescents: correlates and clinical consequences of fat stored in specific body depots. Pediatr Obes. 2012;7:e42–e61. [DOI] [PubMed] [Google Scholar]
- 3. Berends LM, Ozanne SE. Early determinants of type‐2 diabetes. Best Pract Res Clin Endocrinol Metab. 2012;26:569–580. [DOI] [PubMed] [Google Scholar]
- 4. Park MH, Falconer C, Viner RM, Kinra S. The impact of childhood obesity on morbidity and mortality in adulthood: a systematic review. Obes Rev. 2012;13:985–1000. [DOI] [PubMed] [Google Scholar]
- 5. Canas JA, Sweeten S, Balagopal PB. Biomarkers for cardiovascular risk in children. Curr Opin Cardiol. 2013;28:103–114. [DOI] [PubMed] [Google Scholar]
- 6. Weiss R, Bremer AA, Lustig RH. What is metabolic syndrome, and why are children getting it? Ann NY Acad Sci. 2013;1281:123–140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Choi J, Joseph L, Pilote L. Obesity and C‐reactive protein in various populations: a systematic review and meta‐analysis. Obes Rev. 2013;14:232–244. [DOI] [PubMed] [Google Scholar]
- 8. Marcus CL, Brooks LJ, Draper KA, Gozal D, Halbower AC, Jones J, Schechter MS, Ward SD, Sheldon SH, Shiffman RN, Lehmann C, Spruyt K; American Academy of Pediatrics . Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130:e714–e755. [DOI] [PubMed] [Google Scholar]
- 9. Tan HL, Gozal D, Kheirandish‐Gozal L. Obstructive sleep apnea in children: a critical update. Nat Sci Sleep. 2013;5:109–123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Gozal D, Serpero LD, Kheirandish‐Gozal L, Capdevila OS, Khalyfa A, Tauman R. Sleep measures and morning plasma TNF‐α levels in children with sleep‐disordered breathing. Sleep. 2010;33:319–325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Gozal D, Kheirandish‐Gozal L. Obesity and excessive daytime sleepiness in prepubertal children with obstructive sleep apnea. Pediatrics. 2009;123:13–18. [DOI] [PubMed] [Google Scholar]
- 12. Spruyt K, Sans Capdevila O, Serpero LD, Kheirandish‐Gozal L, Gozal D. Dietary and physical activity patterns in children with obstructive sleep apnea. J Pediatr. 2010;156:724–730, 730.e1‐730.e3. [DOI] [PubMed] [Google Scholar]
- 13. Gozal D, Kheirandish‐Gozal L. Childhood obesity and sleep: relatives, partners, or both? Ann NY Acad Sci. 2012;1264:135–141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Bhattacharjee R, Kheirandish‐Gozal L, Pillar G, Gozal D. Cardiovascular complications of obstructive sleep apnea syndrome: evidence from children. Prog Cardiovasc Dis. 2009;51:416–433. [DOI] [PubMed] [Google Scholar]
- 15. Kheirandish‐Gozal L, Bhattacharjee R, Gozal D. Autonomic alterations and endothelial dysfunction in pediatric obstructive sleep apnea. Sleep Med. 2010;11:714–720. [DOI] [PubMed] [Google Scholar]
- 16. Bhattacharjee R, Kim J, Alotaibi WH, Kheirandish‐Gozal L, Capdevila OS, Gozal D. Endothelial dysfunction in children without hypertension: potential contributions of obesity and obstructive sleep apnea. Chest. 2012;141:682–691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Asano K, Okamoto S, Fukunaga K, Shiomi T, Mori T, Iwata M, Ikeda Y, Yamaguchi K. Cellular source(s) of platelet‐activating‐factor acetylhydrolase activity in plasma. Biochem Biophys Res Commun. 1999;261:511–514. [DOI] [PubMed] [Google Scholar]
- 18. Burke JE, Dennis EA. Phospholipase A2 biochemistry. Cardiovasc Drugs Ther. 2009;23:49–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Bhatti S, Hakeem A, Cilingiroglu M. Lp‐PLA(2) as a marker of cardiovascular diseases. Curr Atheroscler Rep. 2010;12:140–144. [DOI] [PubMed] [Google Scholar]
- 20. Öngen B, Kalkan Uçar S, Levent E, Azarsız E, Koloğlu T, Çoker M, Sözmen E, Sağın FG. Lipoprotein‐associated phospholipase A2: a new marker to determine cardiovascular risk in hypercholesterolemic dyslipidaemic children. Ann Clin Biochem. 2016. Available at: http://journals.sagepub.com/doi/abs/10.1177/0004563216671338. Accessed January 14, 2017. [DOI] [PubMed] [Google Scholar]
- 21. Ragab SM, Safan MA, Obeid OM, Sherief AS. Lipoprotein‐associated phospholipase A2 (Lp‐PLA2) and tumor necrosis factor‐α (TNF‐α) and their relation to premature atherosclerosis in β‐thalassemia children. Hematology. 2015;20:228–238. [DOI] [PubMed] [Google Scholar]
- 22. Sakka S, Siahanidou T, Voyatzis C, Pervanidou P, Kaminioti C, Lazopoulou N, Kanaka‐Gantenbein C, Chrousos GP, Papassotiriou I. Elevated circulating levels of lipoprotein‐associated phospholipase A2 in obese children. Clin Chem Lab Med. 2015;53:1119–1125. [DOI] [PubMed] [Google Scholar]
- 23. Montgomery‐Downs HE, O'Brien LM, Gulliver TE, Gozal D. Polysomnographic characteristics in normal preschool and early school‐aged children. Pediatrics. 2006;117:741–753. [DOI] [PubMed] [Google Scholar]
- 24. Berry RB, Budhiraja R, Gottlieb DJ, Gozal D, Iber C, Kapur VK, Marcus CL, Mehra R, Parthasarathy S, Quan SF, Redline S, Strohl KP, Davidson Ward SL, Tangredi MM; American Academy of Sleep Medicine . Rules for scoring respiratory events in sleep: update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2012;8:597–619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Gozal D, Kheirandish‐Gozal L, Serpero LD, Sans Capdevila O, Dayyat E. Obstructive sleep apnea and endothelial function in school‐aged nonobese children: effect of adenotonsillectomy. Circulation. 2007;116:2307–2314. [DOI] [PubMed] [Google Scholar]
- 26. Hansell J, Henareh L, Agewall S, Norman M. Non‐invasive assessment of endothelial function—relation between vasodilatory responses in skin microcirculation and brachial artery. Clin Physiol Funct Imaging. 2004;24:317–322. [DOI] [PubMed] [Google Scholar]
- 27. Kheirandish‐Gozal L, Khalyfa A, Gozal D, Bhattacharjee R, Wang Y. Endothelial dysfunction in children with obstructive sleep apnea is associated with epigenetic changes in the eNOS gene. Chest. 2013;143:971–977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Gozal D, Kheirandish‐Gozal L, Bhattacharjee R, Spruyt K. Neurocognitive and endothelial dysfunction in children with obstructive sleep apnea. Pediatrics. 2010;126:e1161–e1167. [DOI] [PubMed] [Google Scholar]
- 29. Khalyfa A, Kheirandish‐Gozal L, Khalyfa AA, Philby MF, Alonso‐Álvarez ML, Mohammadi M, Bhattacharjee R, Terán‐Santos J, Huang L, Andrade J, Gozal D. Circulating plasma extracellular microvesicle miRNA cargo and endothelial dysfunction in OSA children. Am J Respir Crit Care Med. 2016;194:1116–1126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Donato LJ, Meeusen JW, Callanan H, Saenger AK, Jaffe AS. Advantages of the lipoprotein‐associated phospholipase A2 activity assay. Clin Biochem. 2016;49:172–175. [DOI] [PubMed] [Google Scholar]
- 31. Kim S, Lewis JR, Baur LA, Macaskill P, Craig JC. Obesity and hypertension in Australian young people: results from the Australian Health Survey 2011 to 2012. Intern Med J. 2016. DOI: 10.1111/imj.13298. Available at: http://onlinelibrary.wiley.com/doi/10.1111/imj.13298/full. Accessed January 14, 2017. [DOI] [PubMed] [Google Scholar]
- 32. Yan W, Li X, Zhang Y, Niu D, Mu K, Ye Y, Liu F. Reevaluate secular trends of body size measurements and prevalence of hypertension among Chinese children and adolescents in past two decades. J Hypertens. 2016;34:2337–2343. [DOI] [PubMed] [Google Scholar]
- 33. Steinberger J, Daniels SR, Hagberg N, Isasi CR, Kelly AS, Lloyd‐Jones D, Pate RR, Pratt C, Shay CM, Towbin JA, Urbina E, Van Horn LV, Zachariah JP; American Heart Association Atherosclerosis, Hypertension, and Obesity in the Young Committee of the Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Epidemiology and Prevention; Council on Functional Genomics and Translational Biology; and Stroke Council . Cardiovascular health promotion in children: challenges and opportunities for 2020 and beyond: a scientific statement from the American Heart Association. Circulation. 2016;134:e236–e255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Vlahandonis A, Nixon GM, Davey MJ, Walter LM, Horne RS. Improvement of sleep‐disordered breathing in children is associated with a reduction in overnight blood pressure. Sleep Med. 2013;14:1295–1303. [DOI] [PubMed] [Google Scholar]
- 35. Horne RS, Yang JS, Walter LM, Richardson HL, O'Driscoll DM, Foster AM, Wong S, Ng ML, Bashir F, Patterson R, Nixon GM, Jolley D, Walker AM, Anderson V, Trinder J, Davey MJ. Elevated blood pressure during sleep and wake in children with sleep‐disordered breathing. Pediatrics. 2011;128:e85–e92. [DOI] [PubMed] [Google Scholar]
- 36. Bixler EO, Vgontzas AN, Lin HM, Liao D, Calhoun S, Fedok F, Vlasic V, Graff G. Blood pressure associated with sleep‐disordered breathing in a population sample of children. Hypertension. 2008;52:841–846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Li AM, Au CT, Sung RY, Ho C, Ng PC, Fok TF, Wing YK. Ambulatory blood pressure in children with obstructive sleep apnoea: a community based study. Thorax. 2008;63:803–809. [DOI] [PubMed] [Google Scholar]
- 38. Amin R, Somers VK, McConnell K, Willging P, Myer C, Sherman M, McPhail G, Morgenthal A, Fenchel M, Bean J, Kimball T, Daniels S. Activity‐adjusted 24‐hour ambulatory blood pressure and cardiac remodeling in children with sleep disordered breathing. Hypertension. 2008;51:84–91. [DOI] [PubMed] [Google Scholar]
- 39. Kheirandish‐Gozal L, Etzioni T, Bhattacharjee R, Tan HL, Samiei A, Molero Ramirez H, Abu Eta B, Pillar G. Obstructive sleep apnea in children is associated with severity‐dependent deterioration in overnight endothelial function. Sleep Med. 2013;14:526–531. [DOI] [PubMed] [Google Scholar]
- 40. Kato M, Roberts‐Thomson P, Phillips BG, Haynes WG, Winnicki M, Accurso V, Somers VK. Impairment of endothelium‐dependent vasodilation of resistance vessels in patients with obstructive sleep apnea. Circulation. 2000;102:2607–2610. [DOI] [PubMed] [Google Scholar]
- 41. Bhattacharjee R, Alotaibi WH, Kheirandish‐Gozal L, Capdevila OS, Gozal D. Endothelial dysfunction in obese non‐hypertensive children without evidence of sleep disordered breathing. BMC Pediatr. 2010;10:8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Lavi S, Lavi R, McConnell JP, Lerman LO, Lerman A. Lipoprotein‐associated phospholipase A(2): review of its role as a marker and a potential participant in coronary endothelial dysfunction. Mol Diagn Ther. 2007;11:219–226. [DOI] [PubMed] [Google Scholar]
- 43. Loffredo L, Zicari AM, Occasi F, Perri L, Carnevale R, Angelico F, Del Ben M, Martino F, Nocella C, Savastano V, Cesoni Marcelli A, Duse M, Violi F. Endothelial dysfunction and oxidative stress in children with sleep disordered breathing: role of NADPH oxidase. Atherosclerosis. 2015;240:222–227. [DOI] [PubMed] [Google Scholar]
- 44. Kim J, Gozal D, Bhattacharjee R, Kheirandish‐Gozal L. TREM‐1 and pentraxin‐3 plasma levels and their association with obstructive sleep apnea, obesity, and endothelial function in children. Sleep. 2013;36:923–931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Khalyfa A, Kheirandish‐Gozal L, Capdevila OS, Bhattacharjee R, Gozal D. Macrophage migration inhibitory factor gene polymorphisms and plasma levels in children with obstructive sleep apnea. Pediatr Pulmonol. 2012;47:1001–1011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Tektaş AK, Uslu S, Yalçin AU, Sahin G, Temiz G, Kara M, Temel HE, Demirkan ES, Colak E, Colak O. Effects of lipoprotein‐associated phospholipase A2 on arginase/nitric oxide pathway in hemodialysis patients. Ren Fail. 2012;34:738–743. [DOI] [PubMed] [Google Scholar]
- 47. Bhattacharjee R, Kim J, Kheirandish‐Gozal L, Gozal D. Obesity and obstructive sleep apnea syndrome in children: a tale of inflammatory cascades. Pediatr Pulmonol. 2011;46:313–323. [DOI] [PubMed] [Google Scholar]
- 48. Macphee C, Benson GM, Shi Y, Zalewski A. Lipoprotein associated phospholipase A2: a novel marker of cardiovascular risk and potential therapeutic target. Expert Opin Investig Drugs. 2005;14:671–679. [DOI] [PubMed] [Google Scholar]
- 49. Garza CA, Montori VM, McConnell JP, Somers VK, Kullo IJ, Lopez‐Jimenez F. Association between lipoprotein‐associated phospholipase A2 and cardiovascular disease: a systematic review. Mayo Clin Proc. 2007;82:159–165. [DOI] [PubMed] [Google Scholar]
- 50. Garg PK, McClelland RL, Jenny NS, Criqui M, Liu K, Polak JF, Jorgensen NW, Cushman M. Association of lipoprotein‐associated phospholipase A(2) and endothelial function in the Multi‐Ethnic Study of Atherosclerosis (MESA). Vasc Med. 2011;16:247–252. [DOI] [PubMed] [Google Scholar]
- 51. Garg PK, McClelland RL, Jenny NS, Criqui MH, Greenland P, Rosenson RS, Siscovick DS, Jorgensen N, Cushman M. Lipoprotein‐associated phospholipase A2 and risk of incident cardiovascular disease in a multi‐ethnic cohort: the Multi Ethnic Study of Atherosclerosis. Atherosclerosis. 2015;241:176–182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Chatsuriyawong S, Gozal D, Kheirandish‐Gozal L, Bhattacharjee R, Khalyfa AA, Wang Y, Hakonarson H, Keating B, Sukhumsirichart W, Khalyfa A. Genetic variance in nitric oxide synthase and endothelin genes among children with and without endothelial dysfunction. J Transl Med. 2013;11:227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Kheirandish‐Gozal L, Gozal D. Genotype‐phenotype interactions in pediatric obstructive sleep apnea. Respir Physiol Neurobiol. 2013;189:338–343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Beebe DW, Miller N, Kirk S, Daniels SR, Amin R. The association between obstructive sleep apnea and dietary choices among obese individuals during middle to late childhood. Sleep Med. 2011;12:797–799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Gozal D, Capdevila OS, Kheirandish‐Gozal L. Metabolic alterations and systemic inflammation in obstructive sleep apnea among nonobese and obese prepubertal children. Am J Respir Crit Care Med. 2008;177:1142–1149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Koren D, Gozal D, Bhattacharjee R, Philby MF, Kheirandish‐Gozal L. Impact of adenotonsillectomy on insulin resistance and lipoprotein profile in nonobese and obese children. Chest. 2016;149:999–1010. [DOI] [PMC free article] [PubMed] [Google Scholar]