

Abstract
Background
It has been observed that married cancer patients have lower mortality rates than unmarried patients, but data for different racial/ethnic groups are scarce. The authors examined the risk of overall mortality associated with marital status across racial/ethnic groups and sex in data from the California Cancer Registry.
Methods
California Cancer Registry data for all first primary invasive cancers diagnosed from 2000 through 2009 for the 10 most common sites of cancer-related death for non-Hispanic whites (NHWs), blacks, Asians/Pacific Islanders (APIs), and Hispanics were used to estimate multivariable hazard ratios (HRs) and 95% confidence intervals (CIs) for marital status in relation to overall mortality by race/ethnicity and sex. The study cohort included 393,470 male and 389,697 female cancer patients and 204,007 and 182,600 deaths from all causes, respectively, through December 31, 2012.
Results
All-cause mortality was higher in unmarried patients than in married patients, but there was significant variation by race/ethnicity. Adjusted HRs (95% CIs) ranged from 1.24 (95% CI, 1.23-1.26) in NHWs to 1.11 (95% CI, 1.07-1.15) in APIs among males and from 1.17 (95% CI, 1.15-1.18) in NHWs to 1.07 (95% CI, 1.04-1.11) in APIs among females. All-cause mortality associated with unmarried status compared with married status was higher in US-born API and Hispanic men and women relative to their foreign-born counterparts.
Conclusions
For patients who have the cancers that contribute most to mortality, being unmarried is associated with worse overall survival compared with being married, with up to 24% higher mortality among NHW males but only 6% higher mortality among foreign-born Hispanic and API females. Future research should pursue the identification of factors underlying these associations to inform targeted interventions for unmarried cancer patients.
Keywords: marriage, mortality, nativity, neighborhood socioeconomic status, race/ethnicity
Introduction
Results from several studies have demonstrated a lower risk of mortality among married cancer patients compared with their unmarried counterparts. A large meta-analysis and a recent population-based study of data from the National Cancer Institute's (NCI) Surveillance, Epidemiology, and End Results (SEER) program indicate that never-married, divorced/separated, and widowed cancer patients had higher mortality than married patients, with relative risks ranging from 1.10 to 1.23.1,2 Being married is also associated with earlier cancer stage at diagnosis and receipt of definitive treatment.1,3-7 Proposed reasons for the beneficial effects of being married include having stronger social support and social networks, resulting in higher psychological well being and help with navigating the health care system ; having medical insurance8 ; and economic well being9 as well as improved behavioral and psychological function.1-4,7
Despite the considerable literature on marital status and cancer outcome and the well recognized racial/ethnic differences in cancer mortality and survival, 10,11 data on whether the impact of marriage varies across racial/ethnic groups are lacking. It is noteworthy that, in the United States, the proportion of adults who have never been married has risen from 10% in 1960 to 23% in 2012 among men and from 8% to 17% among women.12 urthermore, wide variations by race/ethnicity exist, with 36% of blacks, 26% of Hispanics, 19% of Asians/Pacific Islanders (APIs), and 16% of whites reporting never being married in 2012.
To address the lack of data on racial/ethnic differences in the association of marital status with mortality among patients with cancer, we assessed the risk of overall mortality associated with marital status across race/ethnicity and sex in data from the demographically diverse, population-based California Cancer Registry (CCR).
Materials and Methods
Case Selection
Data on all first primary invasive cancers for each patient from the 10 most common sites of cancer deaths for each sex were obtained from the CCR, which also comprises 4 NCI SEER program regions. For males, the sites were prostate, lung and bronchus (“lung”), colon, non-Hodgkin lymphoma (“NHL”), urinary bladder (“bladder”), liver and intrahepatic bile duct (“liver and IBD”), leukemia, pancreas, stomach, and esophagus. Additional sites for females included breast; corpus and uterus, not otherwise specified (NOS) (“uterus”); ovary; and brain and other nervous system (“brain”). We included cases diagnosed at ages ≥ 18 years from 2000 through 2009; and we excluded those diagnosed at autopsy or from death certificates (n = 9286) and those with invalid or unknown follow-up time (n = 4347), with unknown marital status (n = 36,937), and/or with unknown treatment status (n = 11,087).
CCR data on race, ethnicity, birthplace, and marital status at diagnosis are determined from medical records of reporting facilities and are primarily based on self-report. We also obtained CCR data on age and year of diagnosis, sex, disease stage at diagnosis, histology, primary and secondary sources of payment to the reporting hospital, and first course of treatment (surgery, radiation, and systemic hormone agents). Nativity is based on birthplace coded to as US or foreign born. Previous research indicates that birthplace is differentially missing in the cancer registry data between US and foreign born for Hispanics and APIs13,14; thus, we developed and validated a method to impute nativity using patients' Social Security numbers for the 23% of Hispanics and the 21% of APIs with missing registry birthplace. This imputation method assigns a foreign birthplace to Hispanic patients who received their Social Security numbers after age 24 years and to APIs after age 20 years.15,16 Patient residential address at diagnosis was geocoded and assigned to a census block group, then linked to a neighborhood socioeconomic status (nSES) index that incorporated data on education, occupation, employment, household income, poverty, rent and house values from the Census 2000 Summary File (for cases diagnosed 2000-2005) and from American Community Survey data from 2007 to 2011 (for cases diagnosed 2006-2009).17,18
Follow-Up and Vital Status
Follow-up for overall mortality was computed as the number of days between the date of diagnosis and the first occurrence of the following: date of death, date of last known contact, or end date of follow-up (December 31, 2012). We also considered cancer-specific deaths based on the underlying causes of death (coded to the International Classification of Diseases, 10th Revision), and follow-up was censored at the date of death for those who died from an underlying cause other than the primary cancer.
Statistical Analysis
Prior analyses of these data19 indicated significant differences in mortality by sex; therefore, all analyses presented here were conducted separately for males and females. Consistent with a recent review of mortality and marital status indicating that mortality risks did not vary across subcategories of unmarried status,20 we conducted analyses using marital status coded as married and unmarried (never married, separated, divorced, and widowed). We used chi-square tests to compare demographic and clinical characteristics by marital status and multivariable Cox proportional hazards regression models to estimate hazard rate ratios9 and 95% confidence intervals (CIs)21 for overall mortality and cancer-specific mortality, by sex and race/ethnicity. The proportional hazards assumption was tested for marital status and for each covariate using correlation tests of time versus scaled Schoenfeld residuals. The assumption of proportional hazards was violated for SEER summary stage and age at diagnosis. Thus, we computed stage-stratified and age-stratified Cox regression models, which allowed the baseline hazards to vary by both disease stage and age at diagnosis. The models were adjusted for cancer site, surgery, radiation, systemic hormone agents, nSES, and sources of medical payment. We modeled the top 10 cancer sites combined for each sex as well as each cancer site separately. Models that included all of the cancer sites combined excluded cases with leukemia, because stage and surgery were not applicable. We also conducted separate analyses by nativity among His-panics and APIs and for the 6 largest API ethnic groups: Chinese, Japanese, Filipino, Korean, South Asian, and Vietnamese. Greater than 40% of Hispanics had Spanish origin coded as “Hispanic, NOS,” so we did not analyze data for specific Hispanic origin. All statistical analyses were performed using SAS version 9.3 (SAS Institute, Cary, NC). Statistical tests were 2-sided with an a value .05. We did not obtain informed consent from the patients, because we analyzed deidentified cancer registry data.
Results
Characteristics of the Study Population
Among the 393,470 male patients included in our analyses, 204,007 deaths were observed during a total of 1,801,907 person-years of follow-up; and, among the 389,697 female patients, 182,600 deaths were observed during 1,903,874 person-years of follow-up. The proportion of unmarried males at the time of diagnosis was 46% for blacks, 29.8% for Hispanics, 29.7% for NHWs, and 19.1% for APIs; the corresponding proportions of unmarried females were 68%, 47.3%, 49.4%, and 37.8%, respectively. Table 1 indicates that unmarried males were more likely to live in lower SES neighborhoods, have public insurance, present with distant-stage disease, and receive less surgery and radiation than married males overall and within racial/ethnic groups. Among Hispanic and API males, there was a higher proportion of US-born than foreign-born unmarried patients than married patients. Similar to males, differences in socioeconomic factors, stage distribution, and treatment were observed for married compared with unmarried females overall and by race/ethnicity (Table 2). Unlike males, however, unmarried and married Hispanic and API females were similar in their distribution of nativity.
Table 1. Demographic and Clinical Characteristics (%) of Male Patients According to Race/Ethnicity and Marital Status, California, Diagnosis Years 2000 Through 2009.
| Characteristic | Percentage | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||
| All (N = 393,470 | NHW, N = 258,306 | Black, N = 31,059 | Hispanic, N = 59,468 | API, N = 38,121 | ||||||
|
|
|
|
|
|
||||||
| Unmarried, n = 118,126 | Married, n = 275,344 | Unmarried, n = 76,805 | Married, n = 181,501 | Unmarried, n = 14,283 | Married, n = 16,776 | Unmarried, n = 17,715 | Married, n = 41,753 | Unmarried, n = 7273 | Married, n = 30,848 | |
| Total percentage | 30 | 70 | 29.7 | 70.3 | 46 | 54) | 29.8 | 70.2 | 19.1 | 80.9 |
| Age at diagnosis, y | ||||||||||
| 18–29 | 1.6 | 0.2 | 0.9 | 0.1 | 0.8 | 0.1 | 4.5 | 0.6 | 3.3 | 0.2 |
| 30–39 | 1.9 | 1 | 1.3 | 0.6 | 1.6 | 0.8 | 4.2 | 2.3 | 3.5 | 1.4 |
| 40–49 | 6.9 | 4.7 | 6.1 | 3.8 | 8.6 | 6.7 | 9.2 | 7.3 | 7.3 | 5.7 |
| 50–59 | 20.6 | 18.7 | 20 | 18.1 | 27.4 | 25.2 | 19.3 | 20.1 | 16.5 | 17.2 |
| 60–69 | 27.6 | 32.5 | 27.8 | 32.6 | 32.3 | 37 | 25.4 | 32.3 | 21.7 | 30.3 |
| 70–79 | 24.9 | 29.7 | 25.4 | 30.5 | 20.7 | 22.7 | 24.4 | 27.6 | 27.1 | 31.3 |
| 80–89 | 14 | 12.1 | 15.5 | 13.2 | 7.5 | 6.9 | 11.2 | 8.9 | 17.2 | 12.7 |
| ≥90 | 2.6 | 1.1 | 3 | 1.2 | 1.1 | 0.5 | 1.8 | 0.8 | 3.3 | 1.1 |
| Neighborhood (block group) SES (statewide quintiles) | ||||||||||
| Q1 (low) | 19.6 | 12.1 | 13 | 7 | 35.6 | 22.7 | 36.4 | 30.3 | 17 | 11.6 |
| Q2 | 21.1 | 17.3 | 19.6 | 14.9 | 25.2 | 23.8 | 24.3 | 24.8 | 20.6 | 17.5 |
| Q3 | 21.1 | 20.6 | 22.2 | 20.7 | 18.7 | 21.8 | 18.5 | 19.8 | 20.7 | 20 |
| Q4 | 20.2 | 22.8 | 22.9 | 24.8 | 13.5 | 19 | 13 | 14.7 | 21.7 | 23.6 |
| Q5 (high) | 18.1 | 27.3 | 22.3 | 32.5 | 7 | 12.6 | 7.9 | 10.4 | 20 | 27.4 |
| Health insurance | ||||||||||
| None | 3.6 | 1.4 | 2.6 | 0.8 | 5.2 | 1.9 | 6.2 | 3 | 4.6 | 2.3 |
| Private only | 36.3 | 49.5 | 39 | 51 | 30.8 | 54.9 | 29.7 | 46.1 | 32.9 | 42.4 |
| Medicare or Medicare and private | 14 | 18.7 | 16.9 | 22.2 | 7.6 | 12 | 8.5 | 11.8 | 9.1 | 11.2 |
| Any public, Medicaid, or military | 41.3 | 27.2 | 36.6 | 22.9 | 51.8 | 28.5 | 50.5 | 35.3 | 49.1 | 41.2 |
| Unknown | 4.8 | 3.2 | 4.8 | 3.2 | 4.7 | 2.7 | 5.1 | 3.8 | 4.3 | 2.8 |
| Cancer site | ||||||||||
| Prostate | 37.2 | 48.9 | 36.4 | 49.5 | 46 | 59.6 | 34.9 | 48.4 | 26.9 | 36.1 |
| Lung | 21.4 | 15.6 | 23.3 | 16.4 | 21.5 | 14 | 14.2 | 11 | 21.4 | 19.2 |
| Colon | 10.4 | 9.8 | 10.4 | 9.6 | 9.3 | 9.4 | 11 | 10.1 | 12.5 | 11.3 |
| Bladder | 4.6 | 4.1 | 5.6 | 4.8 | 2.2 | 1.9 | 3.1 | 2.7 | 3.1 | 2.6 |
| NHL | 7.4 | 6.1 | 7.3 | 6.1 | 4.8 | 3.6 | 10.3 | 7.1 | 7.4 | 6 |
| Leukemia | 4.5 | 3.7 | 4.5 | 3.9 | 2.8 | 2.3 | 6 | 4 | 4.9 | 2.8 |
| Liver and IBD | 5.2 | 3.5 | 3.7 | 2 | 5 | 2.7 | 9.1 | 5.9 | 11.5 | 10.5 |
| Pancreas | 3.7 | 3.5 | 3.8 | 3.4 | 3.4 | 3.1 | 3.7 | 3.9 | 4.2 | 3.6 |
| Esophagus | 2.4 | 1.7 | 2.6 | 2 | 1.9 | 1 | 2.1 | 1.5 | 1.8 | 1.2 |
| Stomach | 3.1 | 3.2 | 2.3 | 2.2 | 3.1 | 2.5 | 5.5 | 5.5 | 6.4 | 6.6 |
| Stage | ||||||||||
| Local | 42.7 | 52.4 | 43 | 53.4 | 44.3 | 56.4 | 40.2 | 49.7 | 37.4 | 45.4 |
| Regional | 17.8 | 18.8 | 17.5 | 18.4 | 18.2 | 18.3 | 18.3 | 19.7 | 20 | 21.1 |
| Distant | 28.4 | 20.9 | 28.4 | 20.4 | 28.5 | 19.3 | 28.8 | 21.9 | 30.1 | 25.5 |
| Unknown/NA | 11.1 | 7.9 | 11 | 7.8 | 9 | 5.9 | 12.7 | 8.7 | 12.5 | 8 |
| Surgery | ||||||||||
| No | 60.4 | 52.8 | 59.2 | 51.3 | 65.6 | 56.8 | 59.5 | 53.2 | 61.1 | 56.3 |
| Yes | 35 | 43.5 | 36.3 | 44.8 | 31.7 | 40.9 | 34.5 | 42.9 | 34.1 | 40.8 |
| NA | 4.5 | 3.7 | 4.5 | 3.9 | 2.8 | 2.3 | 6 | 4 | 4.9 | 2.8 |
| Radiation | ||||||||||
| No | 75.9 | 73 | 75.3 | 72.1 | 74 | 71.8 | 79 | 75.6 | 77.6 | 74.4 |
| Yes | 24.1 | 27 | 24.7 | 27.9 | 26 | 28.2 | 21 | 24.4 | 22.4 | 25.6 |
| Nativity | ||||||||||
| US born | 51.1 | 42 | 23.6 | 15.8 | ||||||
| Foreign born | 48.9 | 58 | 74.8 | 82.7 | ||||||
| Unknown | 1.6 | 1.5 | ||||||||
Abbreviations: API, Asian/Pacific Islander; IBD, intrahepatic bile duct; NA, not applicable; NHL, non-Hodgkin lymphoma; Q, quintile; SES, socioeconomic status.
Table 2. Demographic and Clinical Characteristics (%) of Female Patients According to Race/Ethnicity and Marital Status, California, Diagnosis Years 2000 Through 2009.
| Characteristic | Percentage | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||
| All, N = 389,697 | NHW, N = 260,529 | Black, N = 24,693 | Hispanic, N = 60,132 | API, N = 41,253 | ||||||
|
|
|
|
|
|
||||||
| Unmarried, n = 191,059 | Married, n = 198,638 | Unmarried, n = 128,640 | Married, n = 131,889 | Unmarried, n = 16,789 | Married, n = 7904 | Unmarried, n = 28,413 | Married, n = 31,719 | Unmarried, n = 15,602 | Married, n = 25,651 | |
| Total percentage | 49 | 51 | 49.4 | 50.6 | 68 | 32 | 47.3 | 52.7 | 37.8 | 62.2 |
| Age at diagnosis, y | ||||||||||
| 18–29 | 1.3 | 0.7 | 0.8 | 0.4 | 1 | 0.7 | 3.2 | 1.9 | 2.3 | 0.8 |
| 30–39 | 3 | 4.9 | 1.9 | 3.3 | 4 | 5.8 | 6.1 | 9.7 | 4.4 | 6.8 |
| 4CM9 | 9.5 | 16.6 | 7.6 | 13.7 | 13.7 | 18.3 | 14.3 | 23.4 | 11.3 | 22.2 |
| 50–59 | 16.5 | 25.6 | 15.1 | 24.9 | 21.8 | 26.3 | 18.8 | 26 | 17.4 | 28.3 |
| 60–69 | 20.1 | 25.1 | 19.9 | 26.6 | 23 | 26.6 | 20.1 | 21.3 | 18.5 | 22 |
| 70–79 | 24.6 | 19.4 | 25.9 | 21.8 | 20.8 | 16.8 | 21.3 | 13.7 | 24.4 | 15 |
| 80–-89 | 20.6 | 7.4 | 23.5 | 8.9 | 12.8 | 5.1 | 13.2 | 3.7 | 18.3 | 4.7 |
| ≥90 | 4.5 | 0.5 | 5.2 | 0.6 | 2.8 | 0.4 | 2.9 | 0.2 | 3.5 | 0.3 |
| Neighborhood (block group) SES (statewide quintile) | ||||||||||
| Q1 (low) | 16 | 10.9 | 10.5 | 6.5 | 33 | 23.1 | 32.9 | 28.3 | 12.7 | 8.6 |
| Q2 | 20 | 16.4 | 18.2 | 14.1 | 26.5 | 24.1 | 25 | 24.4 | 18.7 | 15.5 |
| Q3 | 21.8 | 20.4 | 22.6 | 20.5 | 20 | 22.5 | 19.7 | 20.1 | 20.9 | 19.4 |
| Q4 | 22.2 | 23.5 | 24.9 | 25.4 | 13.6 | 18.5 | 13.8 | 16 | 24.6 | 25 |
| Q5 (high) | 20 | 28.8 | 23.9 | 33.5 | 6.8 | 11.8 | 8.6 | 11.3 | 23.1 | 31.6 |
| Health insurance | ||||||||||
| None | 1.9 | 1.4 | 1.2 | 0.8 | 2.5 | 1.6 | 4.3 | 3 | 2.6 | 2.2 |
| Private only | 41.4 | 61.2 | 43.4 | 62.1 | 40.3 | 62.1 | 34.1 | 57 | 39.8 | 61.5 |
| Medicare or Medicare and private | 17.4 | 13.8 | 21.3 | 17.1 | 10.3 | 10.1 | 8.5 | 7.2 | 9.6 | 6.3 |
| Any public, | 34.9 | 20.5 | 29.5 | 16.9 | 44 | 24.1 | 48.9 | 29.3 | 44.1 | 27.4 |
| Medicaid, or military | ||||||||||
| Unknown | 4.4 | 3.1 | 4.7 | 3.1 | 3 | 2 | 4.2 | 3.6 | 3.8 | 2.7 |
| Cancer site | ||||||||||
| Breast | 39.1 | 50.6 | 38.8 | 50.6 | 40.1 | 50.3 | 40.1 | 51.1 | 38 | 50.4 |
| Lung | 19.1 | 12.5 | 21.2 | 14.1 | 19.7 | 12.9 | 11.5 | 7.3 | 15.5 | 10.8 |
| Colon | 12 | 9 | 11.9 | 8.6 | 13.9 | 12.7 | 10.6 | 8.4 | 13.8 | 10.3 |
| Uterus | 8.2 | 8.9 | 8 | 8.7 | 7.5 | 7.5 | 9.7 | 10 | 8.1 | 9.1 |
| NHL | 5.6 | 5.3 | 5.3 | 5.2 | 4.2 | 4 | 7.4 | 6.4 | 5.7 | 4.8 |
| Ovary | 5 | 4.8 | 4.8 | 4.7 | 3.7 | 3.5 | 6.4 | 5.5 | 5.6 | 4.7 |
| Pancreas | 4.3 | 3.1 | 4 | 3 | 5.2 | 4.1 | 4.8 | 3.4 | 4.5 | 3 |
| Leukemia | 3.1 | 2.7 | 3.1 | 2.6 | 2.4 | 2.5 | 3.8 | 3.3 | 2.6 | 2.1 |
| Liver and IBD | 1.9 | 1.4 | 1.1 | 0.7 | 2.1 | 1.3 | 3.4 | 2.2 | 4.9 | 3.6 |
| Brain | 1.7 | 1.8 | 1.7 | 1.8 | 1.1 | 1.1 | 2.3 | 2.4 | 1.4 | 1.1 |
| Stage | ||||||||||
| Local | 40 | 47.7 | 40.8 | 48.7 | 34.9 | 41.5 | 38.9 | 44.9 | 40.6 | 48.1 |
| Regional | 26.3 | 28 | 25.4 | 26.9 | 28.9 | 31.4 | 28.3 | 31.1 | 27.2 | 29.4 |
| Distant | 24.8 | 19 | 24.7 | 19.3 | 28.7 | 21.9 | 23.3 | 18 | 24.3 | 18 |
| Unknown/NA | 9 | 5.3 | 9.1 | 5.2 | 7.5 | 5.2 | 9.4 | 6.1 | 8 | 4.6 |
| Surgery | ||||||||||
| No | 32.8 | 20.4 | 33.1 | 20.6 | 36.5 | 24 | 29.5 | 19 | 31.5 | 20.2 |
| Yes | 64.1 | 76.9 | 63.8 | 76.8 | 61.1 | 73.5 | 66.8 | 77.7 | 65.9 | 77.7 |
| Unknown | 3.1 | 2.7 | 3.1 | 2.6 | 2.4 | 2.5 | 3.6 | 3.3 | 2.6 | 2.1 |
| Radiation | ||||||||||
| No | 72.9 | 64.8 | 72.5 | 63.4 | 72.4 | 68 | 73.5 | 66.9 | 75.5 | 67.8 |
| Yes | 27.1 | 35.2 | 27.5 | 36.6 | 27.6 | 32 | 26.5 | 33.1 | 24.5 | 32.2 |
| Nativity | ||||||||||
| US born | 47.4 | 45.8 | 18.8 | 17.2 | ||||||
| Foreign born | 52.6 | 54.2 | 78.7 | 79.7 | ||||||
| Unknown | 2.4 | 3.2 | ||||||||
Abbreviations: API, Asian/Pacific Islander; IBD, intrahepatic bile duct; NA, not applicable; NHL, non-Hodgkin lymphoma; Q, quintile; SES, socioeconomic status.
Marital Status and All-Cause Mortality by Race/Ethnicity and Nativity
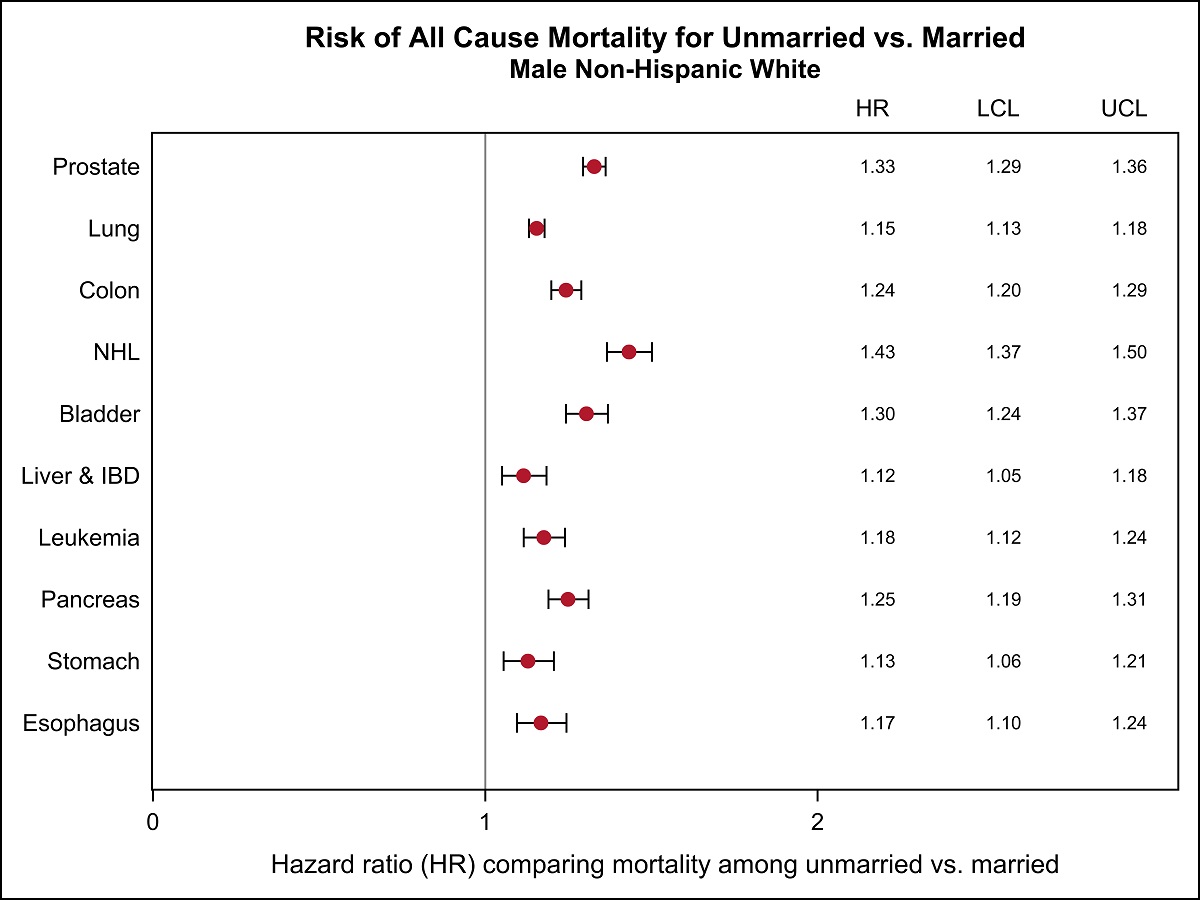
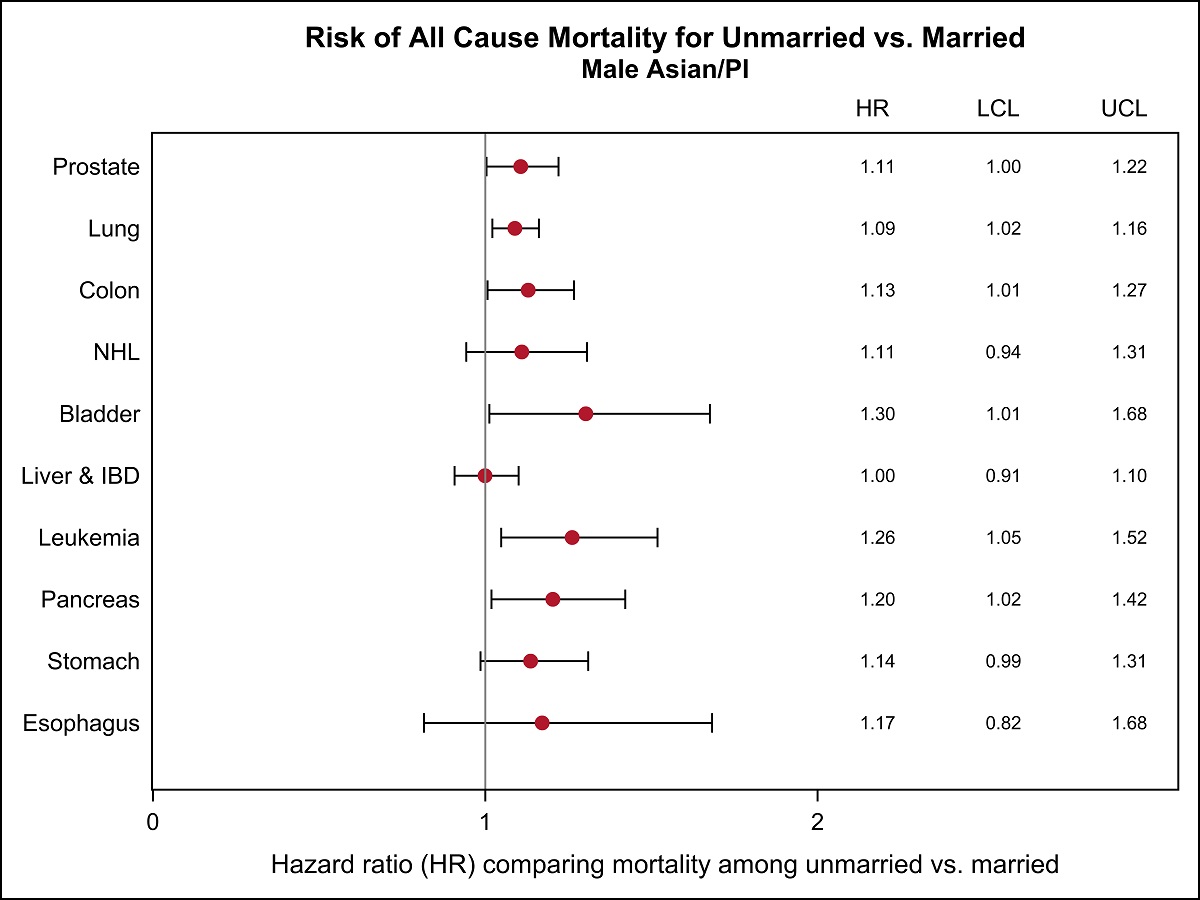
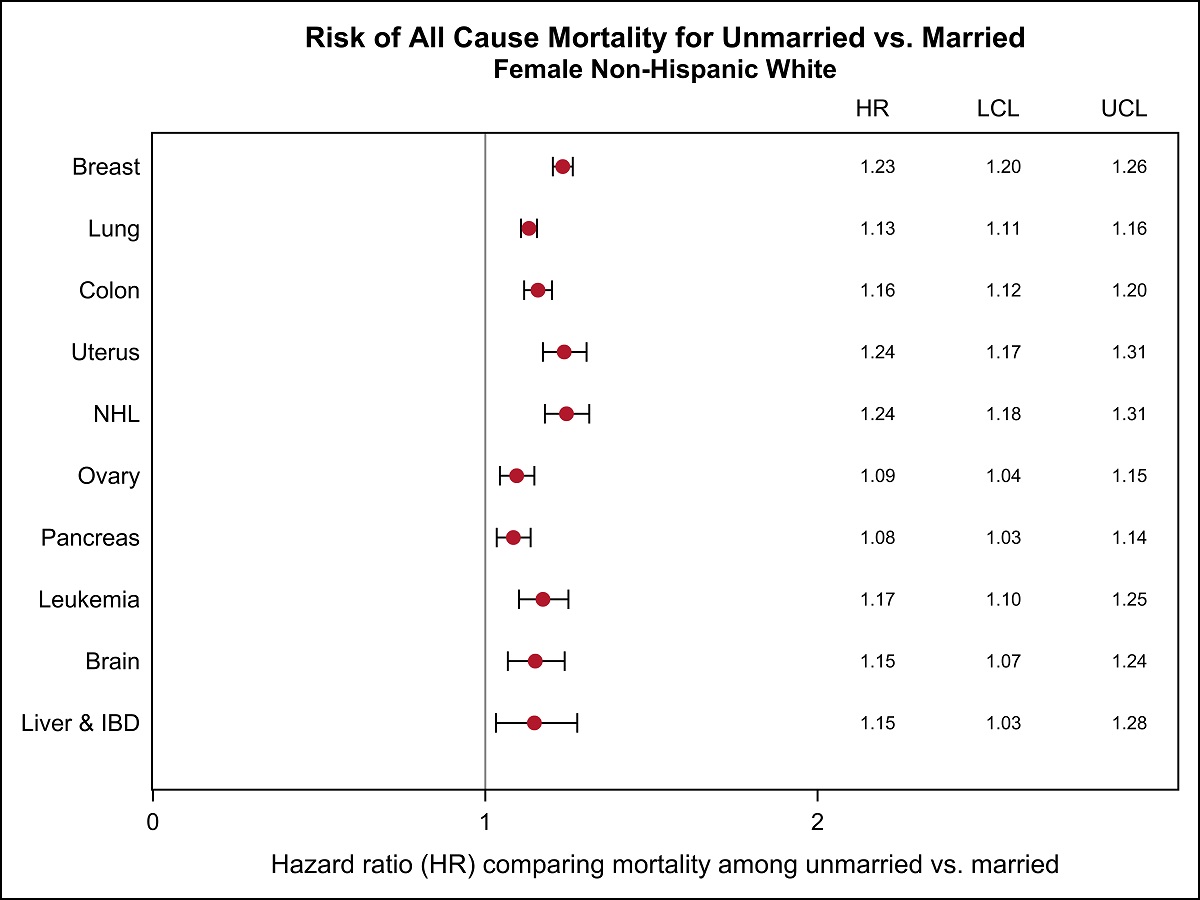
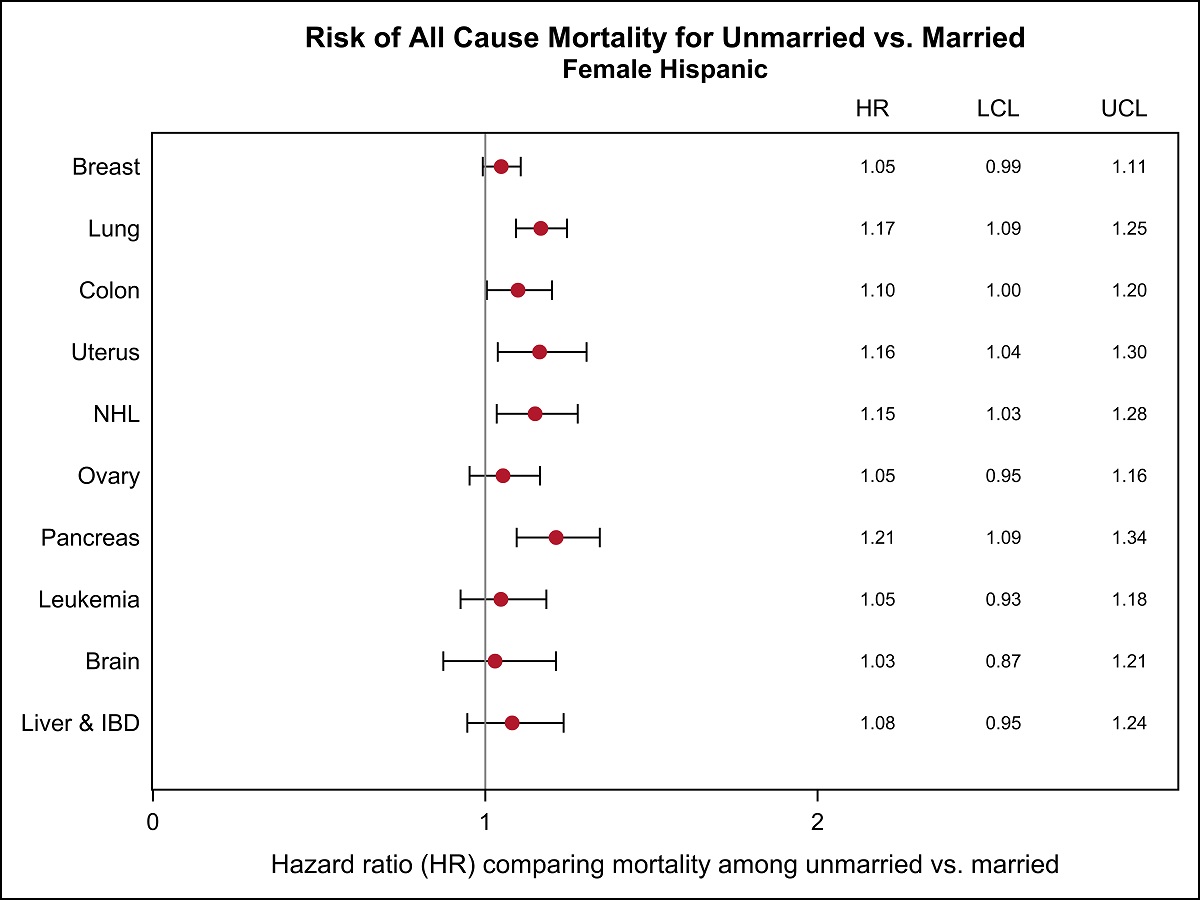
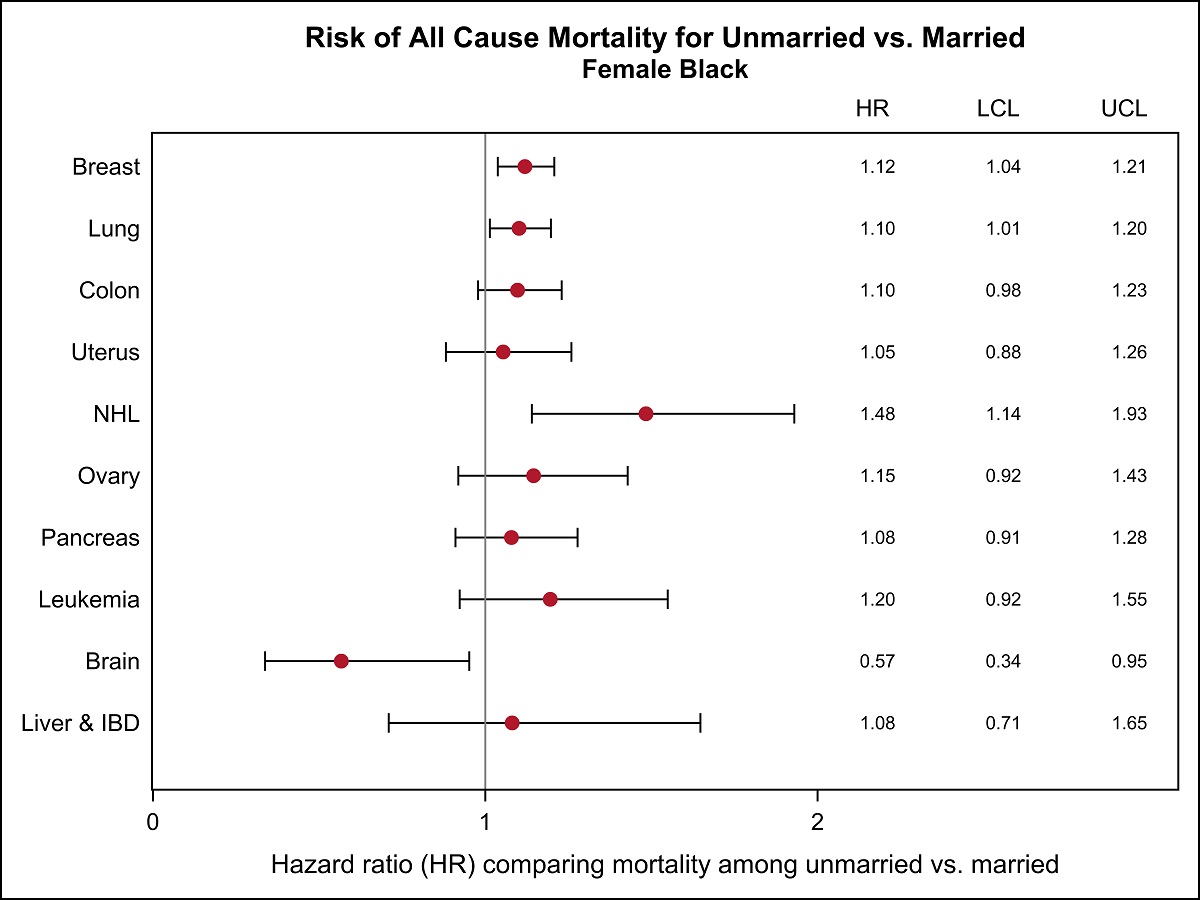
Among males, all-cause mortality was significantly higher in unmarried patients compared with married patients (Table 3). However, the magnitude of the association varied across racial/ethnic groups (P < 6.2 × 10−9), with the largest adjusted hazard ratios (HRs) observed in NHWs (HR, 1.24; 95% CI, 1.23-1.26) and the smallest observed in APIs (HR, 1.11; 95% CI, 1.07-1.15). The association was significantly stronger in US-born versus foreign-born API males (P = .0024), whereas no significant difference by nativity was observed for Hispanic males. The association of marital status with all-cause mortality for females also varied across racial/ethnic groups (P < .0001) and was highest in NHWs (HR, 1.17; 95% CI, 1.15-1.18) and lowest in APIs (HR, 1.07; 95% CI, 1.04-1.11). The HR for marital status and all-cause mortality was significantly higher in US-born versus foreign-born Hispanic women and in API men and women. For all racial/ethnic groups except APIs, the risk of all-cause mortality associated with marital status was statistically significantly lower in females than it was in males (based on nonoverlapping CIs). Given the appreciable attenuation that occurred between the crude and adjusted HRs, we built a series of nested models to assess which factors or set of factors contributed to the attenuation in the HRs for each racial/ethnic and sex group. These data indicated that, regardless of the racial/ethnic or sex group, attenuation was greatest with the inclusion of age and disease stage at diagnosis and cancer site and was less marked when we included nSES, insurance, or treatment (data not shown). For both sexes, although the CIs became quite broad for some racial/ethnic groups, we observed similar patterns of relative risk estimates for each of the 10 common cancers by racial/ethnic group (Supporting Figure 1; see online Supporting Information). Results for cancer-specific mortality were similar to those observed for all-cause mortality (data not shown). Furthermore, when patients with unknown marital status were included in models, the HR for unmarried status did not change (data not shown).
Table 3. Crude and Adjusted Hazard Ratios and 95% Confidence Intervals for All-Cause Mortality Associated With Marital Status (Unmarried vs Married) Stratified by Sex and Nativity.
| Variable | Males: HR (95% CI) | ||||
|---|---|---|---|---|---|
|
| |||||
| All Races, N = 377,932 | NHW, N = 247,722 | Black, N = 30,281 | Hispanic, N = 56,754 | API, N = 36,901 | |
| Overall, crude | 1.57 (1.56–1.59) | 1.63 (1.61–1.65) | 1.64 (1.59–1.69) | 1.56 (.52–1.59) | 1.37 (1.32–1.41) |
| Overall, adjusteda | 1.22 (1.21–1.24) | 1.24 (1.23–1.26) | 1.20 (1.16–1.24) | 1.20 (1.17–1.23) | 1.11 (1.07–1.15) |
| Pheterogeneity for raceb | 6.2 × 10−9 | ||||
| By nativity | |||||
| US born, crude | — | — | — | 1.59 (1.54–1.65) | 1.49 (1.38–1.610 |
| US born, adjusteda | — | — | — | 1.21 (1.17–1.26) | 1.21 (1.11–1.32) |
| Foreign born, crude | — | — | — | 1.52 (1.46–1.57) | 1.39 (1.34–1.44) |
| Foreign born, adjusteda | — | — | — | 1.17 (1.13–1.21) | 1.09 (1.05–1.13) |
| Pheterogeneity for nativityb | — | — | — | .085 | .0024 |
|
| |||||
| Variable | Females: HR (95% CI)c | ||||
|
| |||||
| All Races, N = 378,447 | NHW, N = 253,102 | Black, N = 24,098 | Hispanic, N = 58,008 | API, N = 40,309 | |
|
| |||||
| Overall, crude | 1.80 (1.78–1.82) | 1.83 (1.81–1.85) | 1.54 (1.48–1.60) | 1.63 (1.59–1.68) | 1.75 (1.69–1.81) |
| Overall, adjusteda | 1.15 (1.14–1.16) | 1.17 (1.15–1.18) | 1.09 (1.05–1.13) | 1.11 (1.08–1.14) | 1.07 (1.04–1.11) |
| Pheterogeneity for raceb | <1.0 3 10−30 | ||||
| By nativity | |||||
| US born, crude | — | — | — | 1.64 (1.58–1.70) | 1.88 (1.73–2.05) |
| US born, adjusteda | — | — | — | 1.17 (1.13–1.22) | 1.20 (1.09–1.32) |
| Foreign born, crude | — | — | 1.63 (1.57–1.69) | 1.74 (1.68–1.80) | |
| Foreign born, adjusteda | — | — | — | 1.06 (1.02–1.10) | 1.06 (1.02–1.10) |
| Pheterogeneity for nativityb | — | — | — | 1.5 3 10−8 | 4.6 3 10−6 |
Abbreviations: API, Asian/Pacific Islander; CI, confidence interval; HR, hazard ratio; NHW, non-Hispanic white.
Adjusted HRs were estimated from Cox proportional hazard models stratified by stage (localized, regional, distant, unknown) and age at diagnosis (in years) and were adjusted for: cancer site (prostate, lung, colon, non-Hodgkin lymphoma, bladder, liver and intrahepatic bile duct, pancreas, stomach, and esophagus), race/ethnicity (NHW, black, Hispanic, API, other/unknown for the all races model only), first course of treatment (yes or no for surgery, radiation, hormone therapy), insurance status (no insurance, private insurance only, Medicare only/Medicare and private insurance, any public/Medicaid/military insurance, unknown), and neighborhood socioeconomic status (quintiles). The analysis excluded 15,538 leukemia cases in males.
The likelihood ratio test for interaction was computed based on cross-product terms.
Models for females include sites in the breast, lung, colon, uterus, non-Hodgkin lymphoma, ovary, pancreas, brain, and liver and intrahepatic bile duct. The analysis excluded 11,250 leukemia cases in females.
Associations Among Api Ethnic Groups
Next, we assessed the association between marital status and all-cause mortality by API ethnic subgroup (Table 4). Among males, the association was strongest for Japanese (adjusted HR, 1.17; 95% CI, 1.05-1.31) and was lowest and imprecise for Vietnamese. Among females, Koreans had the highest risk of overall mortality associated with being unmarried (adjusted HR, 1.24; 95% CI, 1.06-1.44), whereas no association was observed for South Asian or Japanese women.
Table 4. Crude and Adjusted Hazard Ratios and 95% Confidence Intervals for All-Cause Mortality Associated With Marital Status (Unmarried vs Married) by Sex and Asian and Pacific Islander Ethnicity.
| API Group | Males | Females | ||||
|---|---|---|---|---|---|---|
|
|
|
|||||
| No. | Crude HR (95% CI) | Adjusted HR (95% CI)a | No. | Crude HR (95% CI) | Adjusted HR (95% CI)a | |
| Chinese | 10,752 | 1.35 (1.26–1.44) | 1.11 (1.03–1.19) | 10,656 | 1.87 (1.76–1.99) | 1.08 (1.01–1.16) |
| Japanese | 4147 | 1.30 (1.19–1.43) | 1.17 (1.05–1.31) | 5084 | 1.53 (1.41–1.66) | 1.02 (0.93–1.13) |
| Filipino | 9662 | 1.40 (1.31–1.50) | 1.12 (1.04–1.21) | 11,868 | 1.71 (1.61–1.81) | 1.12 (1.05–1.20) |
| Korean | 3225 | 1.46 (1.31–1.63) | 1.16 (1.01–1.32) | 2931 | 1.99 (1.77–2.23) | 1.24 (1.06–1.44) |
| South Asian | 1831 | 1.51 (1.25–1.82) | 1.15 (0.88–1.50) | 2039 | 1.73 (1.47–2.04) | 0.98 (0.77–1.24) |
| Vietnamese | 4255 | 1.33 (1.22–1.46) | 1.09 (0.99–1.21) | 3621 | 1.72 (1.55–1.90) | 1.08 (0.96–1.22) |
Abbreviations: API, Asian/Pacific Islander; HR, hazard ratio; CI, confidence interval.
Adjusted HRs were estimated from Cox proportional hazard models stratified by stage (localized, regional, distant, unknown) and age at diagnosis (in years) and were adjusted for: cancer site (males: prostate, lung, colon, non-Hodgkin lymphoma, bladder, liver and intrahepatic bile duct, pancreas, stomach, esophagus; females: breast, lung, colon, uterus, non-Hodgkin lymphoma, ovary, pancreas, brain, and liver and intrahepatic bile duct), first course of treatment (yes or no for surgery, radiation, hormone therapy), insurance status (no insurance, private insurance only, Medicare only/Medicare and private insurance, any public/Medicaid/military insurance, unknown), neighborhood socioeconomic status (quintiles), and nativity (US born, foreign born). Leukemia cases were excluded.
Discussion
Studies of cancer patients in various settings have reported beneficial effects of marriage on cancer-specific and overall mortality,1-4 but data are lacking on differences by race/ethnicity. Our results indicate that unmarried patients experience a higher risk of all-cause mortality than married patients, with significant variation across racial/ethnic groups. We also observed stronger associations for US-born versus foreign-born Hispanic and API patients. Our results further support the well recognized heterogeneity within the aggregated API race group,22 demonstrating variation in the association of marital status and all-cause mortality within API ethnic subgroups for both sexes. Although the adjusted HRs are generally modest, it is important to note that the proportion of unmarried individuals is high, ranging from 19.1% for API males to 68% for black females. Thus, the public health implications are not trivial given these percentages of unmarried patients as well as the rising rates of never married individuals in the United States.12
Differences in the association of marital status with mortality by race/ethnicity and nativity may be attributable to differences in the relative contributions of the hypothesized marital status pathways, including social support and help with navigating the health care system,2 economic well being,9 and medical insurance coverage,8 among others. The results from our analyses demonstrate that only a modest attenuation of HRs resulted from the inclusion of insurance coverage and nSES in the multivariate models. Larger attenuation occurred with the inclusion of age and disease stage in the models.
In the context of cancer survival, various levels of acculturation and English language proficiency also are likely important factors influencing the associations we observed. We observed that the association between marital status and overall mortality was stronger in US-born versus foreign-born APIs and Hispanics, although the HR was imprecise for Hispanic males. These results suggest that factors responsible for the adverse effects of not being married tend to have a greater effect on overall mortality as immigrant groups acculturate to the United States. It is plausible that social support outside of marriage diminishes as individuals acculturate to the United States. Conceptually, acculturation and English language proficiency should be factors relevant among foreign born but less so among US born, suggesting that there are different contributing factors in the marital status-survival association between US-born and foreign-born patients. Further research to identify factors underlying these associations would help to inform interventions targeted toward ensuring that unmarried cancer patients have the same opportunity for survival after cancer diagnosis as their married counterparts.
The strengths of this study include racial/ethnic diversity and a large and representative study population. However, limitations to our data also must be considered. Cancer registry-recorded race, ethnicity, and birthplace may be subject to some misclassification; although, because this information is usually based on self-report (extracted from patient medical records),23 it is generally accurate for most racial/ethnic groups.13,14,24-26 However, because registry birthplace data are incomplete in a biased manner, we used a validated approach to impute nativity. Although marital status was assessed at the time of diagnosis, we lack data on changes in marital status after cancer diagnosis and on cohabitation without marriage, which may differ by race/ethnicity. In addition, information is not available on comorbidities, specific treatment modalities, and other factors that are potential mediators or con-founders in the marital status relationship with survival (ie, psychological and cultural factors, social networks and support, health behaviors, etc). Consequently, our study does not provide specific information regarding why patients from different racial/ethnic groups who are not married at the time of diagnosis have lower survival than married individuals, although it provides patterns of association that can be further evaluated in future studies. There is the possibility of self-selection, as reported in the literature, whereby individuals who are physically, emotionally, or psychologically healthier and/or of higher SES may be more likely to marry than those who are not.20,21,27
Conclusions
Not being married at the time of cancer diagnosis was associated with higher mortality compared with being married, but the association varied by race/ethnicity, sex, and nativity, with up to 24% higher mortality among NHW males but only 6% higher mortality among foreign-born Hispanic and API females. Given the rising proportion of unmarried individuals in the United States and the variation by race/ethnicity,12 the contribution of marital status to the overall burden of cancer mortality will likely continue to rise. Future research should focus on identifying the factors underlying these associations to inform targeted interventions for unmarried cancer patients.
Supplementary Material
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgments
Funding Support: This work was supported by the Stanford Cancer Institute and by the National Cancer Institute's Surveillance, Epidemiology, and End Results program under contract HHSN261201000140C awarded to the Cancer Prevention Institute of California (principal investigator, Sally L. Glaser) and by the Specialized Cancer Center Support Grant to the University of California, San Diego Moores Cancer Center (CA023100-29). Incidence data collection was supported by the California Department of Public Health as part of the statewide cancer reporting program mandated by California Health and Safety Code Section 103885; the National Cancer Institute's Surveillance, Epidemiology, and End Results program under contract HHSN261201000140C awarded to the Cancer Prevention Institute of California, contract HHSN261201000035C awarded to the University of Southern California, and contract HHSN261201000034C awarded to the Public Health Institute; and the Centers for Disease Control and Prevention's National Program of Cancer Registries, under agreement U58DP003862-01 awarded to the California Department of Public Health.
Footnotes
Conflict of Interest Disclosures: Christina A. Clarke reports grants from Genentech outside the submitted work.
References
- 1.Aizer AA, Chen MH, McCarthy EP, et al. Marital status and survival in patients with cancer. J Clin Oncol. 2013;31:3869–3876. doi: 10.1200/JCO.2013.49.6489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pinquart M, Duberstein PR. Associations of social networks with cancer mortality: a meta-analysis. Crit Rev Oncol Hematol. 2010;75:122–137. doi: 10.1016/j.critrevonc.2009.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Inverso G, Mahal BA, Aizer AA, Donoff RB, Chau NG, Haddad RI. Marital status and head and neck cancer outcomes. Cancer. 2015;121:1273–1278. doi: 10.1002/cncr.29171. [DOI] [PubMed] [Google Scholar]
- 4.Wang L, Wilson SE, Stewart DB, Hollenbeak CS. Marital status and colon cancer outcomes in US Surveillance, Epidemiology and End Results registries: does marriage affect cancer survival by gender and stage? Cancer Epidemiol. 2011;35:417–422. doi: 10.1016/j.canep.2011.02.004. [DOI] [PubMed] [Google Scholar]
- 5.Chang SM, Barker FG., 2nd Marital status, treatment, and survival in patients with glioblastoma multiforme: a population based study. Cancer. 2005;104:1975–1984. doi: 10.1002/cncr.21399. [DOI] [PubMed] [Google Scholar]
- 6.Aizer AA, Paly JJ, Zietman AL, et al. Multidisciplinary care and pursuit of active surveillance in low-risk prostate cancer. J Clin Oncol. 2012;30:3071–3076. doi: 10.1200/JCO.2012.42.8466. [DOI] [PubMed] [Google Scholar]
- 7.Osborne C, Ostir GV, Du X, Peek MK, Goodwin JS. The influence of marital status on the stage at diagnosis, treatment, and survival of older women with breast cancer. Breast Cancer Res Treat. 2005;93:41–47. doi: 10.1007/s10549-005-3702-4. [DOI] [PubMed] [Google Scholar]
- 8.Ayanian JZ, Kohler BA, Abe T, Epstein AM. The relation between health insurance coverage and clinical outcomes among women with breast cancer. N Engl J Med. 1993;329:326–331. doi: 10.1056/NEJM199307293290507. [DOI] [PubMed] [Google Scholar]
- 9.Waite LJ, Lehrer EL. The benefits from marriage and religion in the United States: a comparative analysis. Popul Dev Rev. 2003;29:255–276. doi: 10.1111/j.1728-4457.2003.00255.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kish JK, Yu M, Percy-Laurry A, Altekruse SF. Racial and ethnic disparities in cancer survival by neighborhood socioeconomic status in Surveillance, Epidemiology, and End Results (SEER) Registries. J Natl Cancer Inst Monogr. 2014;2014:236–243. doi: 10.1093/jncimonographs/lgu020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Trinh QD, Nguyen PL, Leow JJ, et al. Cancer-specific mortality of Asian Americans diagnosed with cancer: a nationwide population-based assessment [serial online] J Natl Cancer Inst. 2015;107 doi: 10.1093/jnci/djv054. djv054. [DOI] [PubMed] [Google Scholar]
- 12.Wang W, Parker K. Record Share of Americans Have Never Married: As Values, Economics and Gender Patterns Change. Washington, DC: Pew Research Center; 2014. [Google Scholar]
- 13.Gomez SL, Glaser SL, Kelsey JL, Lee MM. Bias in completeness of birthplace data for Asian groups in a population-based cancer registry (United States) Cancer Causes Control. 2004;15:243–253. doi: 10.1023/B:CACO.0000024244.91775.64. [DOI] [PubMed] [Google Scholar]
- 14.Gomez SL, Glaser SL. Quality of cancer registry birthplace data for Hispanics living in the United States. Cancer Causes Control. 2005;16:713–723. doi: 10.1007/s10552-005-0694-7. [DOI] [PubMed] [Google Scholar]
- 15.Gomez SL, Quach T, Horn-Ross PL, et al. Hidden breast cancer disparities in Asian women: disaggregating incidence rates by ethnicity and migrant status. Am J Public Health. 2010;100(suppl 1):S125–S131. doi: 10.2105/AJPH.2009.163931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Keegan TH, John EM, Fish KM, Alfaro-Velcamp T, Clarke CA, Gomez SL. Breast cancer incidence patterns among California Hispanic women: differences by nativity and residence in an enclave. Cancer Epidemiol Biomarkers Prev. 2010;19:1208–1218. doi: 10.1158/1055-9965.EPI-10-0021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Yang J, Schupp CW, Harrati A, Clarke C, Keegan THM, Gomez SL. Developing an area-based socioeconomic measure from American Community Survey data. Fremont, CA: Cancer Prevention Institute of California; 2014. [Google Scholar]
- 18.Yost K, Perkins C, Cohen R, Morris C, Wright W. Socioeconomic status and breast cancer incidence in California for different race/ethnic groups. Cancer Causes Control. 2001;12:703–711. doi: 10.1023/a:1011240019516. [DOI] [PubMed] [Google Scholar]
- 19.Gomez SL, Hurley S, Canchola AJ, et al. Effects of marital status and economic resources on survival after cancer: a population-based study. Cancer. 2016;122:1618–1625. doi: 10.1002/cncr.29885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Rendall MS, Weden MM, Favreault MM, Waldron H. The protective effect of marriage for survival: a review and update. Demography. 2011;48:481–506. doi: 10.1007/s13524-011-0032-5. [DOI] [PubMed] [Google Scholar]
- 21.Manzoli L, Villari P, M Pirone G, Boccia A. Marital status and mortality in the elderly: a systematic review and meta-analysis. Soc Sci Med. 2007;64:77–94. doi: 10.1016/j.socscimed.2006.08.031. [DOI] [PubMed] [Google Scholar]
- 22.Gomez SL, Glaser SL, Horn-Ross PL, et al. Cancer research in Asian American, Native Hawaiian, and Pacific Islander populations: accelerating cancer knowledge by acknowledging and leveraging heterogeneity. Cancer Epidemiol Biomarkers Prev. 2014;23:2202–2205. doi: 10.1158/1055-9965.EPI-14-0624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gomez SL, Le GM, West DW, Satariano WA, O'Connor L. Hospital policy and practice regarding the collection of data on race, ethnicity, and birthplace. Am J Public Health. 2003;93:1685–1688. doi: 10.2105/ajph.93.10.1685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Clegg LX, Reichman ME, Hankey BF, et al. Quality of race, Hispanic ethnicity, and immigrant status in population-based cancer registry data: implications for health disparity studies. Cancer Causes Control. 2007;18:177–187. doi: 10.1007/s10552-006-0089-4. [DOI] [PubMed] [Google Scholar]
- 25.Gomez SL, Glaser SL. Quality of birthplace information obtained from death certificates for Hispanics, Asians, and Pacific Islanders. Ethn Dis. 2004;14:292–295. [PubMed] [Google Scholar]
- 26.Gomez SL, Glaser SL. Misclassification of race/ethnicity in a population-based cancer registry (United States) Cancer Causes Control. 2006;17:771–781. doi: 10.1007/s10552-006-0013-y. [DOI] [PubMed] [Google Scholar]
- 27.Kravdal O. The poorer cancer survival among the unmarried in Norway: is much explained by comorbidities? Soc Sci Med. 2013;81:42–52. doi: 10.1016/j.socscimed.2013.01.012. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.