

Highlights
-
•
Levonorgestrel IUD was effective in treatment of recurrent APA.
-
•
No side effects were reported.
-
•
No impairments on a subsequent pregnancy were reported.
1. Introduction
Atypical polypoid adenomyoma (APA) is a rare benign mixed epithelial and mesenchymal tumor (Hendrickson et al., 2003). Histologically APA is characterized by a mixture of benign endometrial glands with structural atypia and a prominent cellular, smooth muscle stroma.
Although APA is considered a benign disease, it may recur, furthermore it is reported a frequent APA coexistence with endometrioid adenocarcinoma of the endometrium or with atypical endometrial hyperplasia and the possibility of APA progression to endometrioid adenocarcinoma of the endometrium (Yamagami et al., 2015, Inoue et al., 2014, Nomura et al., 2015).
APA is often diagnosed in childbearing and premenopausal patients, with the reported median age of 40 years (Yamagami et al., 2015, Longacre et al., 1996, Young et al., 1986, Di Spiezio Sardo et al., 2008). In post-menopause hysterectomy is the treatment of choice, while in patients who may want to preserve the fertility potential a conservative surgical procedure has been suggested (Matsumoto et al., 2013, Yamagami et al., 2015, Nomura et al., 2015, Di Spiezio Sardo et al., 2008).
We report the case of a patient who experienced 2 recurrences of APA after conservative hysteroscopic resections, submitted to hormonal treatment with levonorgestrel releasing intrauterine system for 12 months. Afterwards she was referred to our Fertility Center and conceived after induction of ovulation with clomiphene. She delivered a baby boy by caesarian section.
2. Case report
A 32-years old woman (gravida 0) was referred to the Department of Obstetrics and Gynecology of University of Milan, Italy (Macedonio Melloni Hospital), after an histological diagnosis of APA in November 2012. She complained of heavy menstrual bleeding with a mild anemia. Her physical examination was unremarkable. Transvaginal ultrasound (TVS) revealed the presence of a hyperechoic lesion in the uterine cavity suspicious for an endometrial polyp. Consequently, an operative hysteroscopy under general anesthesia with resectoscopic treatment of the lesion was performed with histological diagnosis of APA. The patient was then evaluated every 3 months by TVUS and diagnostic hysteroscopy with endometrial biopsy for the first 6 months. Afterwards the patient was followed up by TVUS every 6 months.
In March 2014, a suspicious endometrial polyp was diagnosed during her follow up with TVUS. Resection with operative hysteroscopy was then performed (Fig. 1) with final histology of recurrent APA.
Fig. 1.
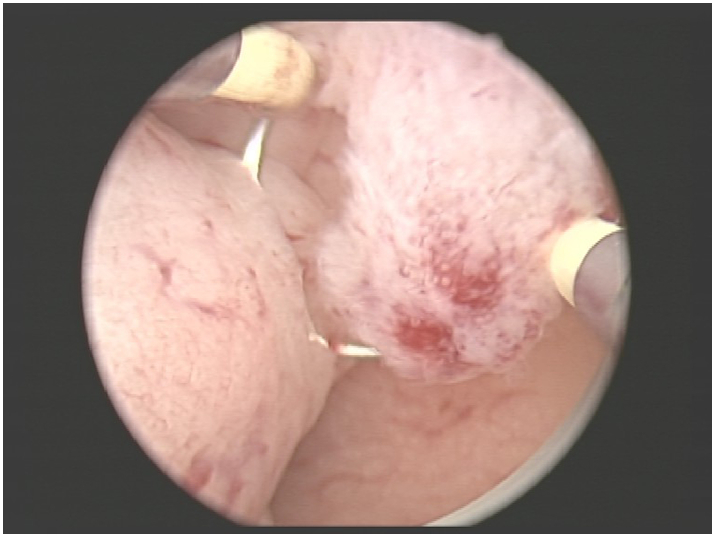
Macroscopic aspect of atypical polypoid adenomyoma during hysteroscopy.
She continued the follow up with diagnostic hysteroscopy with biopsies every four months and in September 2014 biopsies reveled APA recurrence, treated again by conservative hysteroscopic resection.
After the 2nd recurrence of APA, due to her strong desire of childbearing, an adjuvant progestin intrauterine treatment was suggested. After a detailed informed consent was signed, a levonorgestrel releasing IUD was placed in December 2014. Diagnostic hysteroscopy was performed every 3–4 months starting from March 2015 confirming no sign of recurrence. No side effects related to IUD were observed.
After 12 months of treatment the IUD was removed and the patient was referred to our Fertility Center to shorten the time to pregnancy. Ovulation induction with clomiphene 50 mg starting from the 3rd day for 7 days was obtained. After just one cycle she conceived. The pregnancy course was uneventful, except for an observational hospitalization at 28th weeks for uterine contractile activity and reduction of the cervix length. The patient was discharged 2 days later with local progestin therapy. A baby boy weighing 3890 g was delivered by caesarian section for maternal request at 39 weeks. Placenta histology and uterine curettage carried out during cesarian section were normal.
Two months after the caesarian section the patient underwent a diagnostic hysteroscopy with biopsies for persistent mild vaginal bleeding and thickened endometrium, the specimens revealed only the presence of necrotic deciduas.
3. Discussion
The pathogenesis of APA is unknown. The presence of estrogen and progesterone receptors (Terada, 2011) suggests an hormonal influence and may support an hormonal treatment.
Hysteroscopic resection of the lesion and careful follow up has been proposed by some authors with encouraging results. Di Spiezio Sardo et al. (2008) proposed a four-step technique resection (step 1: the removal of the APA, step 2: the removal of endometrium sideward to the lesion, step 3: the removal of the myometrium under the lesion, step 4: random endometrial biopsies). Dilatation and curettage is an alternative treatment. However, hysteroscopic resection seems to reduce recurrence (Matsumoto et al., 2013).
Medical treatment by using medroxyprogesterone acetate was proposed by Nomura et al. (2015) in 18 patients (13 patients with APA, 4 patient with APA coexisting with endometrial adenocarcinoma, 1 patient with APA coexisting with atypical endometrial hyperplasia) diagnosed after dilatation and curettage. On 18 patients studied, 14 achieved a partial or complete response, 8 had a recurrence, 10 eventually underwent hysterectomy, 9 developed endometrial cancer. In patients under 35 years, 4 out of 5 had children (Table 1). Levonorgestrel IUD was suggested as maintenance therapy.
Table 1.
Outcome of treatment of APA with hormonal therapy in literature (MPA: medroxyprogesterone acetate; APA atypical polypoid adenomyoma; EC: endometrial carcinoma; AEH: atypical endometrial hyperplasia).
| Author | Journal | Treatment | N. patients | Histology | Response to therapy | APA Persistence | APA Recurrence | Final diagnosis of EC | Pregnancy |
|---|---|---|---|---|---|---|---|---|---|
| Nomura et al. (2015) | Arch Gynecol Obstet 2015 | MPA 200–600 mg/day for 6–9 months | 18 | APA (13) APA + EC (4) APA + AEH (1) |
14 | 4 | 8 | 9 | 4 |
| Yamagami et al. (2015) | J Obstet Gynecol Res 2015 | MPA 600 mg/day for 6 months | 3 | APA + EC (1) APA + AEH (2) |
3 | 0 | 1 | 0 | 3 |
Yamagami et al. (2015) treated 3 young patients with APA coexisting with endometrioid adenocarcinoma of the endometrium or with atypical endometrial hyperplasia with high dose of medroxyprogesterone acetate achieving pregnancy in all of them after complete hysteroscopic response to treatment (Table 1).
Several studies have reported the safety of progestins in young patients affected by endometrial adenocarcinoma at stage IA, grade 1, or atypical endometrial hyperplasia desiring to preserve their reproductive potential. Although no definitive consensus exists regarding the optimal progestin regimen and duration, levonorgestrel intrauterine system was suggested to reduce side effects of medroxyprogesterone acetate and megestrol acetate (Gunderson et al., 2012).
To our knowledge, this is the first report of conservative treatment of recurrent APA with a local hormonal therapy with levonorgestrel IUD. Firstly, no side effects were reported. Secondly, there was no impairment on a subsequent pregnancy. Although a larger case series is necessary to confirm the efficacy and safety of this treatment, this case supports the effectiveness of levonorgestrel IUD in treatment of recurrent APA in young women who desire to preserve fertility.
Follow up should be performed for a long time. Recurrence with endometrial cancer has been diagnosed up to 8 years after treatment by Inoue et al. (2014). Standard follow up should include TVUS and diagnostic hysteroscopy in case of suspicious lesions.
Conflict of interest statement
The authors declare no conflicts of interest.
References
- Di Spiezio Sardo A., Mazzon I., Gargano V., Di Carlo C., Guida M., Mignogna C. Hysteroscopic treatment of atypical polypoid adenomyoma diagnosed incidentally in a young infertile woman. Fertil. Steril. 2008;89 doi: 10.1016/j.fertnstert.2007.02.061. 456.e9–12) [DOI] [PubMed] [Google Scholar]
- Gunderson C.C., Fader A.N., Carson K.A., Bristow R.E. Oncologic and reproductive outcomes with progestin therapy in women with endometrial hyperplasia and grade 1 adenocarcinoma: a systematic review. Gynecol. Oncol. 2012;25(2):477–482. doi: 10.1016/j.ygyno.2012.01.003. [DOI] [PubMed] [Google Scholar]
- Hendrickson M.R., Tavassoli F.A., Kempson R.L., McCluggage W.G., Haller U., Kubick-Huch R.A. Adenomyoma including atypical polypoid adenomyoma. In: Tavassoli F.A., Devilee P., editors. World Health Organization Classification of Tumors. Pathology and Genetics of Tumours of the Breast and Female Genital Organs. IARC Press; Lyon: 2003. p. 24. [Google Scholar]
- Inoue K., Tsubamoto H., Hori M., Ogasawara T., Takemura T. A case of endometrioid adenocarcinoma developing 8 years after conservative management for atypical polypoid adenomyoma. Gynecol. Oncol. Rep. 2014;8:21–23. doi: 10.1016/j.gynor.2014.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Longacre T.A., Chung M.H., Rouse R.V., Hendrickson M.R. Atypical polypoid adenomyofibromas (atypical polypoid adenomyomas) of the uterus. A clinicopathologic study of 55 cases. Am. J. Surg. Pathol. 1996;20:1–20. doi: 10.1097/00000478-199601000-00001. [DOI] [PubMed] [Google Scholar]
- Matsumoto T., Hiura M., Baba T., Ishiko O., Shiozawa T. Clinical management of atypical polypoid adenomyoma of the uterus. A clinicopathological review of 29 cases. Gynecol. Oncol. 2013;129:54–57. doi: 10.1016/j.ygyno.2012.12.040. [DOI] [PubMed] [Google Scholar]
- Nomura H., Sugiyama Y., Tanigawa T., Matoda M., Kanao H. Long term outcome of fertility sparing treatment of atypical polypoid adenomyoma with medroxyprogesterone acetate. Arch. Gynecol. Obstet. 2015;293:177–181. doi: 10.1007/s00404-015-3824-9. [DOI] [PubMed] [Google Scholar]
- Terada T. Atipical polypoid adenomyoma of the uterus: an immunohistochemical study on 5 cases. Ann. Diagn. Pathol. 2011;15:338–341. doi: 10.1016/j.anndiagpath.2011.03.008. [DOI] [PubMed] [Google Scholar]
- Yamagami W., Susumu N., Ninomiya T., Nakadaira N., Iwasa N. Hysteroscopic transcervical resection is useful to diagnose myometrial invasion in atypical polypoid adenomyoma coexisting with atypical endometrial hyperplasia or endometrial cancer with suspicious myometrial invasion. J. Obstet. Gynaecol. Res. 2015;5:768–775. doi: 10.1111/jog.12645. [DOI] [PubMed] [Google Scholar]
- Young R.H., Treger T., Scully R.E. Atypical polypoid adenomyomas of the uterus. A report of 27 cases. Am. J. Clin. Pathol. 1986;86:139–145. doi: 10.1093/ajcp/86.2.139. [DOI] [PubMed] [Google Scholar]