

Abstract
Aims and Objectives:
This study aims to evaluate the efficacy of tamsulosin and alfuzosin for the distal ureteral stone. This study assessed the spontaneous passage and expulsion of the stone.
Materials and Methods:
The study was conducted in the Department of Surgery at Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, from May 2013 to May 2014. A total number of 136 patients diagnosed as distal ureteric stone (US) of size <10 mm were included in this study. It was divided into two groups (I and II) out of which 36 cases were excluded. Group I received tablet tamsulosin 0.4 mg/day, and Group II received alfuzosin 10 mg/day. The efficacy of tamsulosin and alfuzosin as an adjunctive medical therapy was determined.
Results:
Both the drugs can be safely used for the distal USs. The stone expulsion rate was seen in 36 patients (72.0%) in Group I, and in 34 patients (68.0%) in Group II (P = 0.545). The passage of stones noticed by 32 patients in each Groups I and II (P = 1.000). The mean number of pain attacks was 2.91 ± 1.01 for Group I, and 1.8 ± 0.83 for Group II (P < 0.001 and P < 0.001). Thus, we propagate the use of alfuzosin significantly lower number of pain attacks. The drug-related side-effects were postural hypertension (four in Group I and one in Group II) and retrograde ejaculation (eight in Group I, and one in Group II). Thus, the difference was statistically significant in terms of retrograde ejaculation but insignificant for postural hypotension.
Conclusion:
There is no difference between both medications in term of efficacy (passing stones) for the management of distal ureteral stones. Both medications are safe and effective. In addition, alfuzosin was better tolerated than tamsulosin as it has fewer side effects.
Key words: Alfuzosin, medical therapy, pain, stones, ureter
INTRODUCTION
The lifetime risk of kidney stones is estimated to be between 5% and 10% with the recurrence rate as high as 50%.[1] Urinary tract stones are one of the common urological conditions worldwide. The prevalence is estimated to be 1%–5% in Asia, 5%–9% in Europe, and 13% in the USA.[2] A large number of patients presenting in a surgical emergency have symptoms and signs of ureteric colic. Spontaneous expulsion of distal ureteral stones of ≤10 mm diameter occurs in 25%–53% of cases.[3] The 2007 Guideline for the Management of Ureteral Calculi of the American Urological Association (AUA), and the European Association of Urology (EAU) guideline recommend watchful waiting with medical treatment for patients with a stone of <10 mm in diameter and with well-controlled pain. A meta-analysis performed by the AUA/EAU guidelines panel demonstrated that for stones ≤5 mm, 68% of stones would pass spontaneously. For stones >5 mm and ≤10 mm, 47% would pass spontaneously.[4] The medical and surgical therapy is used to manage the ureteric stones (USs). The most common methods are ureteroscopy (URS), shock wave lithotripsy (SWL), laser therapy, laparoscopic or open approach (transabdominal/retroperitoneal), or combinations of the above approaches. The choice of intervention depends on patient factors, anatomical considerations, surgeon preference, and stone location and characteristics.[4]
Nowadays, medical expulsive therapy (MET) has been used and is an excellent treatment modality for distal USs in spite of conservative treatment.[5] There are certain factors which influence the passage of USs such as stone size, configuration, location, smooth muscle spasm, submucosal edema, and anatomy.[6,7] Alpha blockers, calcium channel blockers are the most commonly used drugs for MET. Tamsulosin has been the most commonly studied α−1 blocker; however, alfuzosin is a combined α−1 A and α1 D selective adrenergic antagonist resulting in relaxation of distal ureteric smooth muscles to facilitate passage of stone and relieving pain. It is easily available and has less cardiac and ejaculatory side effects.[7] As some advised for conservative treatment but we do not recommend conservative treatment as it may cause complications and especially patient discomfort. Hence, in view, to reduce the complication rates, the MED therapy should be given. The aim of the present study was to compare tamsulosin and alfuzosin for their efficacy and safety as MET in patients with a symptomatic uncomplicated US that was located in one of the three sections of the ureter. We also assessed the effect of these two drugs in reducing the pain episodes in these patients.
MATERIALS AND METHODS
This study was conducted in the Department of Surgery, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, India in an outpatient setting from May 2013 to May 2014. The study protocol was approved by the Ethics Committee of our hospital. All male and female patients presenting with acute ureteric colic had been completed for study participation. Patients with a single distal US <10 mm in size and age of 18 years and above of 50 years, were included for the study. Patients were excluded if they met any of the following criteria: (1) presence of multiple USs, (2) renal insufficiency (estimated by raised blood urea and serum creatinine levels), (3) moderate to severe hydronephrosis in solitary kidney, (4) pregnancy/lactation, (5) patients with a history of ureteric surgery or previous endoscopic procedures, (6) stone size of or >10 mm, and (7) bilateral USs.
Every case was assessed on ultrasonography (USG) and X-ray kidney, ureter, and bladder (KUB) was done. In addition, the patients underwent a series of measurements, including case history, physical examination, complete blood cell count, routine urinalysis, and serum creatinine measurement. All patients received the first treatment of diclofenac 75 mg by intramuscular injection, with a second dose after 30 min if necessary. If diclofenac gave inadequate pain relief, then injection drotin preferred by intramuscular or intravenous route. If the pain was resolved, the patient was dismissed and automatically enrolled in the study after providing informed written consent.
A total number of 136 patients were included in the study for the management of distal ureteric calculi out of that 36 cases were excluded as per the inclusion criteria. They were randomly divided into two groups at a ratio of 1:1, i.e., Group I (n = 50) received oral tamsulosin 0.4 mg/day and Group II (n = 50) received alfuzosin 10 mg orally/day for 21 days. Patients were asked to take the study medication once at the same time each day. Furthermore, they kept a diary to record the frequency of pain attacks, the date and time of stone passage, the presence and type of side-effects thought to be due to the medication and noted on every visit. The treatment was discontinued after the spontaneous stone expulsion, intervention, or at the end of the therapy (i.e., after day 21). They were advised to take plenty of fluids during the study and continue with their daily routine.
The patients were followed-up weekly for 3 weeks, with urinalysis and serum creatinine measurement. Abdominal USG and X-ray KUB was done to assess the stone status. For patients with a stone-free ureter on final USG but unnoticed stone expulsion, the date of last positive stone status was recorded. The absence of stone expulsion after day 21 was considered failed therapy. In these cases, further management was advised as per clinical status. Discontinuation of study medication and intervention before the end of the study due to uncontrollable pain, adverse events, urinary tract infections, acute renal failure, or the patient's desire for stone removal was also considered failed therapy. Patients who experienced stone expulsion before first medication, who withdrew their consent, were excluded from the analysis. The study medication was discontinued after spontaneous expulsion and at the end of study. The objective of this trial was evaluating the efficacy of MET with tamsulosin and alfuzosin. The primary end point was the proportion of patients having stone expulsion until day 21, as confirmed by ultrasound abdomen and X-ray KUB. Statistical analyses were performed with Student's t-test, ANOVA, Chi-square, and Fisher's exact test using the parameters of stone size, expulsion rate, time to expulsion, pain attacks, and side effects. The power used was 0.80, and the level of significance was 5%.
RESULTS
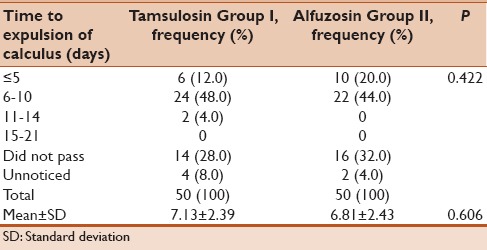
A total of 136 patients were enrolled, and 100 patients completed the study. Group I (50 patients) consisted of 35 men and 15 women, Group II (50 patients) consisted of 36 men and 14 women. Our study was comparable in terms of gender distribution. This was important for the analysis of the side effects thought to be due to the medication, especially retrograde ejaculation. The mean age group in tamsulosin Group I was 36.18 years with the standard deviation of 10.22 whereas the alfuzosin Group II had a mean age of 35.20 years with 10.94 as standard deviation. This was comparable in both groups and was statistically insignificant (P = 0.644). The mean stone size was 6.5 ± 1.78 mm for Group I and 6.26 ± 1.85 mm for Group II. The 32 (64%) patients noticed passage of stone in each of Group I and Group II. The 18 patients did not notice passage of stone in Group I, but 4 patients eventually passed the stone as confirmed on X-ray KUB and USG. Furthermore, in the alfuzosin group also 18 (36%) patients did not notice the passage of stone but two patients had expelled the stone as confirmed radiologically at follow-up. The P value was 1.000 [Table 1]. The calculus expulsion was seen in 36 (72%) patients and 34 (68%) patients in Group I, Group II, respectively (P = 0.545) [Table 2]. The patients had comparable variables in terms of the stone size [Table 3]. The mean time for stone expulsion observed in Group I was 7.13 days with a standard deviation of 2.39 and the mean time in Group II was 6.81 days with a standard deviation of 2.43 [Table 4]. This difference was statistically insignificant.
Table 1.
Patient noticed passage of stones
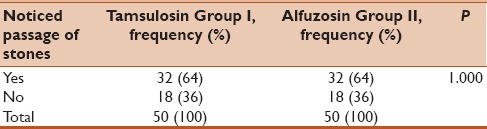
Table 2.
The results of expulsion of the stones
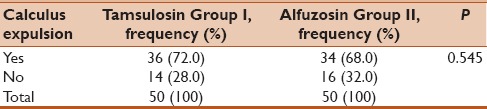
Table 3.
The patients had comparable variables in terms of the stone size
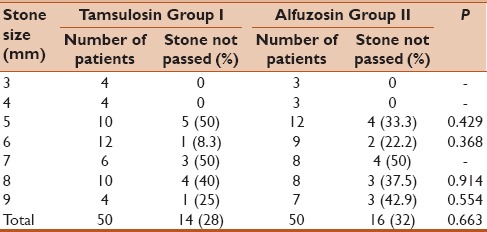
Table 4.
Time to expulsion of calculus (days)
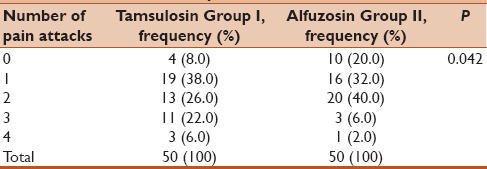
The number of pain attacks was considerably lower in Group II as compared to the Group I. This difference was significant as observed by a P value of 0.042 [Table 5]. The side effects observed with the two medications was postural hypotension and retrograde ejaculation. In tamsulosin group, four patients experienced postural hypotension (8.0%) whereas just one patient had postural hypotension (2.0%) so P value was 0.362. In terms of retrograde ejaculation, eight patients developed retrograde ejaculation in tamsulosin group (16.0%) whereas only one patient developed this in the alfuzosin group (2.0%). Thus, the difference was statistically significant in terms of retrograde ejaculation as side effect but insignificant for postural hypotension with P value of 0.031 and 0.362, respectively. None of the side effects required discontinuation of the study medication. Thus, we propagate the use of alfuzosin for MET as there are significantly lower number of pain attacks and less number of side effects in terms of retrograde ejaculation which may be quite bothersome in patients especially sexually active males.
Table 5.
The number of pain attacks
DISCUSSION
In worldwide urinary tract stones are one of the most usual urological problems. The approximated incidence is to be 1%–5% in Asia, 5%–9% in Europe, and 13% in the USA.[8] The annual incidence of stone occurrence is probably to be 1500–2000 cases/million persons.[9] However, the success rate of conservative management of USs lies mainly on the stone size and position.[3] When patients present with colic symptoms, 60% of stones are located at the ureterovesical junction, but 23.4% are located between the ureteropelvic junction and the iliac vessels. In these cases, extracorporeal SWL (ESWL) is preferred over conservative therapy.[10] ESWL has its own drawbacks such as pain and long sittings and then it was combined with the antagonist such as tamsulosin has shown better results in ureteral stones. Alpha-1 androgen receptor antagonists reduce the tension of ureteral smooth muscle, peristaltic movements, and amplitude of the ureter. As a result, the increased intraureteral pressure gradient created around the stone facilitates its expulsion by the urinary flow.[11]
With the α 1-adrenoceptors, stimulation of phospholipase C starts ureteral contraction, which in turn causes the formation of second messengers (inositol triphosphate [IP3] and diacylglycerol [DAG]). IP3 is involved in the mobilization of calcium from the sarcoplasmic reticulum, whereas DAG increases calcium influx across the cell membrane through the activation of protein kinase C.[12] Thus, the histologic characteristics of the three smooth muscle layers in the lower ureter and the more dense innervation of the lower ureter than the upper and mid ureter have become subjects of research interest. Impacted ureteral calculi cause partial or complete obstruction which activates the α1-receptors by increasing the contraction and the frequency of ureteral peristalsis. Hence, blockage of α1-receptors decreases basal tone prevents peristaltic amplitude and frequency, and lower intraluminal pressure. They studied the role of tamsulosin and alfuzosin for the lower USs and stated that both drugs increase the stone expulsion rate (82.3% vs. 70.5%), reduces expulsion time (12.3 vs. 14.5), and decrease the requirement of analgesics.[13] Another authors compared the three groups for stone expulsion by tamsulosin, alfuzosin group, and a control group. The rate of expulsion of stone was 86.2%, 76.6%, and 50% in Groups I, II, and III, respectively.[14] Another study declared expulsion rate 85% with tamsulosin which was more than with alfuzosin (75%) or in the control group (44%).[2] In our study, the stone expulsion was 72.0% in Group I whereas 68.0% was seen in Group II [Table 6].
Table 6.
Comparison of different studies

Other study used alfuzosin for upper USs, with a spontaneous passage rate of 72.7% versus 21.4% for the control. The mean stone size was 5.49 ± 1.31 mm for Group I (an oral dose of 0.2 mg tamsulosin once), 5.73 ± 1.57 mm for Group II (an oral dose of 0.2 mg tamsulosin twice daily), 5.81 ± 1.26 mm for Group III (a daily oral dose of 10 mg alfuzosin), and 5.59 ± 1.44 mm for Group IV (received trospium chloride only). In their study, calculi passed through the ureter spontaneously in 32 patients (78%) in Group I, 23 patients in Group II (77%), 27 patients in Group III (75%), and 16 patients (47%) in Group IV. Comparison between the two tamsulosin doses and the 10 mg alfuzosin dose showed no significant differences in expulsion rate or expulsion time for lower ureteric calculi.[15] In the present study, 18 patients did not notice passage of stone in tamsulosin and alfuzosin group, respectively, but 4 patients eventually passed the stone as confirmed on X-ray KUB and USG. In the alfuzosin group also, 18 patients did not notice the passage of stone, but 2 patients had expelled the stone as confirmed radiologically at follow-up.
A study observed a total of nine randomized controlled trials combining the results of those using calcium channel blockers and alpha antagonists to treat ureteral stones. This study showed patients who were having calcium channel blockers or alpha antagonists had a 65% greater likelihood of stone passage (P < 0.0001), with a number needed to treat of four patients.[16]
Al-Ansari et al.[17] assessed the efficacy of tamsulosin on the spontaneous passage rate of distal USs. An additional benefit to the use of a-blockers in patients with USs, especially those who are candidates for surgical intervention, is the emerging role of these drugs in relieving symptoms related to an indwelling JJ stent, as reported by other studies.[2] However, the expectant approach may result in complications, such as infection of the urinary tract, hydronephrosis, and renal function defects. ESWL and URS, with or without intracorporeal lithotripsy, are the routinely used methods to treat ureteral stones. Studies have stated that compared to ESWL, URS achieves a greater stone-free state but with a higher complication rate and a longer hospital stay.[18] Recent studies suggested that alfuzosin is much effective for the distal ureteral stones, fewer side effects and more expulsion rate and the reduction in time to stone passage. The studies observed that alfuzosin improves patient discomfort, and decreases the time to stone passage. Several studies evaluated different alpha blockers for MET and they stated that although all alpha blockers improve stone passage compared to placebo, alfuzosin was better tolerated.[19]
A study retrospectively investigated stone passage with tamsulosin-based MET along with parameters on CT imaging including transverse stone diameter, longitudinal stone diameter, ureteral diameter (proximal to stone), and ureter-to-stone diameter ratio. They noted that each of these factors was inversely associated with the successful stone passage, regardless of stone position within the ureter (P < 0.001). Stone expulsion rates appeared to drastically decrease at the 5 mm mark measured longitudinally with 70% and 84.3% passage of 4–5 mm upper and lower ureteral stones, respectively, and 42.9% and 44.8% passage of 5–6 mm upper and lower ureteral stones, respectively.[20] In tamsulosin group, four patients experienced postural hypotension whereas just one patient had postural hypotension. In terms of retrograde ejaculation, eight patients developed retrograde ejaculation in tamsulosin group whereas only one patient developed this in the alfuzosin group. Thus, the difference was statistically significant in terms of retrograde ejaculation as side effect but insignificant for postural hypotension. None of the side effects required discontinuation of the study medication. Thus, we propagate the use of alfuzosin for MET as there are significantly lower number of pain attacks and less number of side effects in terms of retrograde ejaculation which may be quite bothersome in patients especially sexually active males.
Highlights of our study:
It is beneficial for the patient who does not want to go for surgery
It is effective in those cases who are unfit for surgery like pregnancy, cardiac problem
It is cost-effective, easy to take, less side effects, no radiation exposure
If patient is already compromised or hydronephrotic kidney then again side effects may be there
No requirement of hospital stay.
CONCLUSION
The use of tamsulosin 0.4 mg or alfuzosin 10 mg for distal USs was safe and effective. There are increased overall stone expulsion rate, reduced stone expulsion time, and fewer pain episodes. The study observed that alfuzosin was better tolerated than tamsulosin as it has less side effects and pain attacks were also less.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Wood KD, Gorbachinsky I, Gutierrez J. Medical expulsive therapy. Indian J Urol. 2014;30:60–4. doi: 10.4103/0970-1591.124209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ibrahim AK, Mahmood IH, Mahmood NS. Efficacy and safety of tamsulosin vs. alfuzosin as medical expulsive therapy for ureteric stones. Arab J Urol. 2013;11:142–7. doi: 10.1016/j.aju.2013.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Segura JW, Preminger GM, Assimos DG, Dretler SP, Kahn RI, Lingeman JE, et al. Ureteral stones clinical guidelines panel summary report on the management of ureteral calculi. The American Urological Association. J Urol. 1997;158:1915–21. doi: 10.1016/s0022-5347(01)64173-9. [DOI] [PubMed] [Google Scholar]
- 4.Preminger GM, Tiselius HG, Assimos DG, Alken P, Buck C, Gallucci M, et al. 2007 guideline for the management of ureteral calculi. J Urol. 2007;178:2418–34. doi: 10.1016/j.juro.2007.09.107. [DOI] [PubMed] [Google Scholar]
- 5.Sameer, Lal S, Charak KS, Chakravarti S, Kohli S, Ahmad S. Efficacy of nifedipine and alfuzosin in the management of distal ureteric stones: A randomized, controlled study. Indian J Urol. 2014;30:387–91. doi: 10.4103/0970-1591.139572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Porpiglia F, Destefanis P, Fiori C, Fontana D. Effectiveness of nifedipine and deflazacort in the management of distal ureter stones. Urology. 2000;56:579–82. doi: 10.1016/s0090-4295(00)00732-9. [DOI] [PubMed] [Google Scholar]
- 7.Dellabella M, Milanese G, Muzzonigro G. Efficacy of tamsulosin in the medical management of juxtavesical ureteral stones. J Urol. 2003;170:2202–5. doi: 10.1097/01.ju.0000096050.22281.a7. [DOI] [PubMed] [Google Scholar]
- 8.Ramello A, Vitale C, Marangella M. Epidemiology of nephrolithiasis. J Nephrol. 2000;13(Suppl 3):S45–50. [PubMed] [Google Scholar]
- 9.Amato M, Lusini ML, Nelli F. Epidemiology of nephrolithiasis today. Urol Int. 2004;72(Suppl 1):1–5. doi: 10.1159/000076582. [DOI] [PubMed] [Google Scholar]
- 10.Eisner BH, Reese A, Sheth S, Stoller ML. Ureteral stone location at emergency room presentation with colic. J Urol. 2009;182:165–8. doi: 10.1016/j.juro.2009.02.131. [DOI] [PubMed] [Google Scholar]
- 11.Cho HJ, Shin SC, Seo DY, Min DS, Cho JM, Kang JY, et al. Efficacy of alfuzosin after shock wave lithotripsy for the treatment of ureteral calculi. Korean J Urol. 2013;54:106–10. doi: 10.4111/kju.2013.54.2.106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sigala S, Dellabella M, Milanese G, Fornari S, Faccoli S, Palazzolo F, et al. Evidence for the presence of alpha1 adrenoceptor subtypes in the human ureter. Neurourol Urodyn. 2005;24:142–8. doi: 10.1002/nau.20097. [DOI] [PubMed] [Google Scholar]
- 13.Agrawal M, Gupta M, Gupta A, Agrawal A, Sarkari A, Lavania P. Prospective randomized trial comparing efficacy of alfuzosin and tamsulosin in management of lower ureteral stones. Urology. 2009;73:706–9. doi: 10.1016/j.urology.2008.11.013. [DOI] [PubMed] [Google Scholar]
- 14.Ahmed AF, Al-Sayed AY. Tamsulosin versus alfuzosin in the treatment of patients with distal ureteral stones: Prospective, randomized, comparative study. Korean J Urol. 2010;51:193–7. doi: 10.4111/kju.2010.51.3.193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cha WH, Choi JD, Kim KH, Seo YJ, Lee K. Comparison and efficacy of low-dose and standard-dose tamsulosin and alfuzosin in medical expulsive therapy for lower ureteral calculi: Prospective, randomized, comparative study. Korean J Urol. 2012;53:349–54. doi: 10.4111/kju.2012.53.5.349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hollingsworth JM, Rogers MA, Kaufman SR, Bradford TJ, Saint S, Wei JT, et al. Medical therapy to facilitate urinary stone passage: A meta-analysis. Lancet. 2006;368:1171–9. doi: 10.1016/S0140-6736(06)69474-9. [DOI] [PubMed] [Google Scholar]
- 17.Al-Ansari A, Al-Naimi A, Alobaidy A, Assadiq K, Azmi MD, Shokeir AA. Efficacy of tamsulosin in the management of lower ureteral stones: A randomized double-blind placebo-controlled study of 100 patients. Urology. 2010;75:4–7. doi: 10.1016/j.urology.2009.09.073. [DOI] [PubMed] [Google Scholar]
- 18.Aboumarzouk OM, Kata SG, Keeley FX, McClinton S, Nabi G. Extracorporeal shock wave lithotripsy (ESWL) versus ureteroscopic management for ureteric calculi. Cochrane Database Syst Rev. 2012;5:CD006029. doi: 10.1002/14651858.CD006029.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bensalah K, Pearle M, Lotan Y. Cost-effectiveness of medical expulsive therapy using alpha-blockers for the treatment of distal ureteral stones. Eur Urol. 2008;53:411–8. doi: 10.1016/j.eururo.2007.09.012. [DOI] [PubMed] [Google Scholar]
- 20.Lee SR, Jeon HG, Park DS, Choi YD. Longitudinal stone diameter on coronal reconstruction of computed tomography as a predictor of ureteral stone expulsion in medical expulsive therapy. Urology. 2012;80:784–9. doi: 10.1016/j.urology.2012.06.032. [DOI] [PubMed] [Google Scholar]