

Abstract
Homocysteine (Hcy) is an important and independent risk factor for atherosclerotic diseases, such as coronary artery disease and ischemic cerebrovascular disease. Increased carotid artery intima-media thickness (IMT) is a non-invasive marker of systemic atherosclerosis. Allicin treatment may decrease serum Hcy levels and improve impaired endothelial function in rats with hyperhomocysteinemia (HHcy). The present study hypothesized that allicin has an anti-atherosclerotic effect in coronary heart disease and tested the effects of allicin treatment on carotid artery IMT and plasma Hcy levels in coronary heart disease patients with HHcy. Sixty-two coronary heart disease patients with HHcy were randomly divided into an allicin group and a control group. All patients underwent diagnostic assessment, plasma Hcy assay, blood lipid measurement and B-mode ultrasound of the carotid artery prior to and after treatment. Plasma Hcy levels were determined by high-performance liquid chromatography and fluorescence detection. Carotid artery IMT was calculated using an automated algorithm based on a validated edge-detection technique. After 12 weeks, significant decreases in carotid artery IMT, plasma Hcy levels, total cholesterol and triglycerides were observed in the allicin group (all P<0.05), and the decreases in the allicin group were significantly greater than those in the control group (all P<0.01). These findings suggested that reducing plasma Hcy levels may be useful for preventing the generation and development of atherosclerosis in patients with coronary heart disease. Allicin was able to decrease Hcy levels, total cholesterol and triglycerides as well as carotid artery IMT.
Keywords: allicin, coronary heart disease, hyperhomocysteinemia, B-mode ultrasonographic scanning, carotid artery intima-media thickness
Introduction
Cardiovascular and cerebrovascular diseases now have become the principal diseases that threaten human health and atherosclerosis is their principal pathogenic mechanism. Homocysteine (Hcy) has received much attention due to its role in the development of atherosclerosis. Numerous clinical studies and animal experiments have shown that hyperhomocysteinemia (HHcy) is an independent risk factor for vascular diseases, including ischemic heart disease, stroke and peripheral vascular disease (1,2). HHcy is a pathological condition characterized by an increase (>15 µmol/l) in the plasma concentration of total Hcy. Numerous studies have proposed that the atherogenic effects of HHcy are based on the induction of oxidative stress, endothelial dysfunction, thrombosis and activation of proinflammatory factors (3–8). Yet, the mechanisms by which Hcy promotes cardiovascular disease have remained to be fully elucidated. Carotid artery wall thickness is evaluated by measuring its intima-media thickness (IMT). Coronary artery IMT is an easily, reproducibly and non-invasively measured parameter for estimating the severity of carotid atherosclerosis and has been reported to be an independent predictor of coronary heart disease. Studies have demonstrated that allicin prevents atherosclerosis by exerting anti-aggregatory, anti-migratory (9) and anti-oxidant effects (10) as well as lowing blood pressure (11) and blood lipids (12). A previous study by our group reported that allicin obviously decreases the serum Hcy levels in rats with HHcy and also alleviates the injury of Hcy to endothelial cells (13). These results suggested that allicin may be useful as a drug for atherosclerosis. The present study hypothesized that allicin decreases plasma Hcy levels and exerts anti-atherosclerotic effects in coronary heart disease. The effect of allicin treatment on carotid artery IMT and plasma Hcy in coronary heart disease was assessed.
Materials and methods
Study design and subjects
Sixty-two patients (42 males and 20 females) between the age of 50 and 80 years diagnosed with coronary heart disease and HHcy at Qilu Hospital of Shandong University (Jinan, China) were consecutively recruited as outpatients and inpatients from August 2006 to September 2007. Levels indicative of atherosclerotic vascular disease were set according to the European Society of Hypertension-European Society of Cardiology guidelines (14). HHcy was defined as the plasma concentration of total Hcy exceeding 15 µmol/l. Exclusion criteria included overt liver and renal dysfunction, hematological system disease, major psychiatric illness, hypersensitivity constitution and hypersensitivity to the drug, pregnancy or lactation. All subjects were divided into two groups by simple randomization and were treated for 12 weeks by enteric-coated aspirin (100 mg/day), simvastatin (20 mg/day), isosorbide mononitrate tablets (20 mg twice daily) and metoprolol tartrate (from 12.5 mg twice daily gradually increased to the maximum tolerable dose), with the heart rate not lower than 55 beats/minute in the resting phase. One group was also administered allicin (40 mg thrice daily for 12 weeks; allicin group; n=32) and the other group did not receive any allicin (control group; n=30). The clinical characteristics of the subjects are shown in Table I. Conditions at baseline and at the end of the study were recorded and measurements of Hcy and lipids in blood samples as well as carotid artery IMT were undertaken. During the present study, all subjects maintained their normal living habits and did not change their medication. The purpose and potential risks of the study were explained to all patients and their voluntary written consent for participation in the study was obtained prior to enrolment. The present study was approved by the Committee on the Ethics of Clinical Experiments (Qilu Hospital of Shandong University, Jinan, China).
Table I.
Clinical background of the subjects.
| Characteristics | Allicin group (n=32) | Control group (n=30) |
|---|---|---|
| Sex (% male) | 68.9 | 66.7 |
| Age (years) | 61.1±12.0 | 60.4±13.4 |
| Education (years) | 10.5±2.5 | 10.8±2.8 |
| Time since infarction (years) | 6.4±3.1 | 6.5±2.8 |
| CAD type | ||
| Angina pectoris | 24 (75.0) | 20 (66.7) |
| Myocardial infarction | 8 (25.0) | 10 (33.3) |
| Fasting blood glucose (mmol/l) | 5.79±1.72 | 5.72±1.61 |
| Serum triglycerides (mmol/l) | 3.03±1.76 | 3.09±1.60 |
| Serum cholesterol (mmol/l) | 5.60±1.20 | 5.55±1.28 |
| Serum homocysteine (mmol/l) | 19.92±2.11 | 20.05±2.15 |
| Major medical problems | ||
| Hypertension | 21 (65.6) | 17 (56.7) |
| Hyperlipemia | 11 (34.4) | 13 (43.3) |
| Hypercholesterolemia | 8 (25.0) | 7 (23.3) |
| Diabetes mellitus | 7 (21.9) | 9 (30.0) |
| Drugs for blood glucose | 7 (21.9) | 9 (30.0) |
| Drugs for blood pressure | 21 (65.6) | 17 (56.7) |
Values are expressed as the mean ± standard deviation or as n (%). All subjects were Chinese. There were no significant differences between the Allicin and Control groups with regard to any of the parameters. CAD, coronary artery disease.
Blood sampling
Blood samples were collected after overnight fasting. Serum was separated within 1 h and used for measuring of total cholesterol (TC) and triglyceride (TG). Hcy levels were determined in EDTA-treated plasma.
Plasma Hcy assay
In accordance to a previously published method (15), plasma Hcy was assayed at an excitation wavelength of 335 nm and an emission wavelength of 455 nm with a Waters 2695 high efficiency liquid chromatograph and a Waters 2475 fluorescence detector and a Millennium 32 chromatographic workstation (Waters Co., Milford, MA, USA). Standard Hcy and o-phthalaldehyde were obtained from Sigma-Aldrich (Merck KGaA, Darmstadt, Germany). All of the above parameters were detected at the Drug Testing Center of Qilu Hospital of Shandong University (Jinan, China).
Serum biochemical indices assay
Serum biochemical indices, including TC and TG, were determined with a Bayer 1650 supermatic biochemistry analyzer (Bayer AG, Leverkusen, Germany) at the Biochemistry Department of Shandong University (Jinan, China).
Ultrasound examination and IMT quantification
All measurements of carotid artery IMT were performed as part of a routine examination by the same technician, who was blinded to the subjects' clinical data. High-resolution B-mode carotid ultrasonography was performed using an 8–12 MHz transducer and an Aloka SSD-5500 ultrasound scanner (Aloka, Andover, Japan). The patients lied in the supine position with the head slightly tilted to either side at examination. Wall changes were carefully identified in the carotid arteries from different longitudinal and transverse views. The images were focused on the far wall of the artery. In all subjects, the common carotid artery, the internal and external carotid arteries and the carotid bulb were examined. Subsequent to identification of a region ~1.0 cm proximal to the carotid bifurcation, the IMT of the far wall was evaluated as the distance between the luminal-intimal interface and the medial-adventitial interface, measured thrice, and the average IMT value was used. Based on the data in healthy Chinese subjects, abnormal IMT was defined as an IMT of >1.0 mm.
Statistical analysis
Values are expressed as the mean ± standard deviation and data were subjected to a test of normality. Statistical analyses were performed by using the SPSS statistical package, version 12.0 (SPSS Inc., Chicago, IL, USA). Student's t-test and the paired t-test were performed for statistical comparisons. P<0.05 was considered to indicate a statistically significant difference.
Results
Clinical characteristics
Characteristics of the study population are shown in Table I. No differences were found between the two groups with regard to age, sex, TC, TG, blood glucose, mean blood pressure, plasma Hcy, carotid artery IMT and morbidity duration of coronary heart disease. There were also no differences in the ratio of subjects using drugs for lowering blood glucose or blood pressure between the two groups.
Plasma Hcy levels
The Hcy levels are shown in Table II. The basal plasma Hcy concentration did not differ between the two groups. A significant decrease of Hcy was observed in the allicin group after 12 weeks (P<0.01) and the decrease in the allicin group was significantly larger than that in the control group (13.18±2.88 vs. 17.91±2.09 µmol/l; P<0.05).
Table II.
Effect of allicin on plasma Hcy and IMT.
| Hcy (µmol/l) | IMT (mm) | ||||
|---|---|---|---|---|---|
| Group | n | Before treatment | After treatment | Before treatment | After treatment |
| Allicin group | 32 | 19.92±2.11 | 13.18±2.88a,b | 1.28±0.13 | 1.13±0.10a,b |
| Control group | 30 | 20.05±2.15 | 17.91±2.09c | 1.28±0.08 | 1.23±0.08c |
Values are expressed as the mean ± standard deviation.
P<0.01, compared with before treatment in the same group
P<0.01, compared with control group
P<0.05, compared with before treatment in the same group. IMT, intima-media thickness; Hcy, homocysteine.
Carotid artery IMT
The IMTs are shown in Table II. After 12 weeks of allicin administration, the carotid artery IMT in the allicin group was significantly decreased compared with that in the control group (1.13±0.10 vs. 1.23±0.08 µmol/l; P<0.05). Compared with the baseline value, the IMT was significantly decreased after allicin treatment (P<0.01). The IMT was also significantly decreased in the control group (P<0.05), but that the decrease was greater in the allicin group (P<0.01). As shown in Figs. 1 and 2, after allicin treatment, the IMT was decreased from 1.4 to 1.0 mm.
Figure 1.
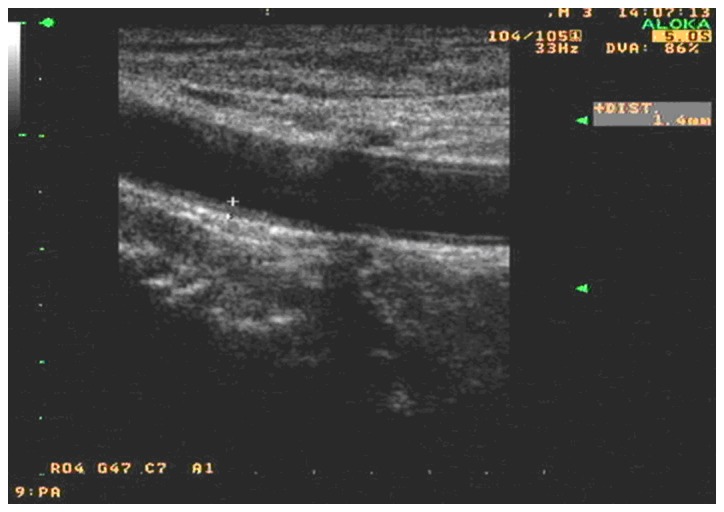
Carotid artery high resolution color Doppler ultrasonograph of a selected frame of a typical case prior to treatment.
Figure 2.
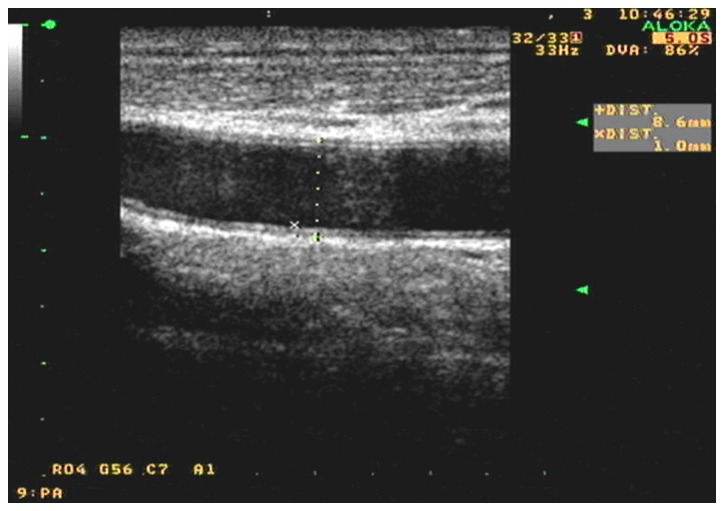
Carotid artery high resolution color Doppler ultrasonograph of a selected frame after allicin treatment of the same typical case as in Fig. 1.
Serum biochemical index levels
The levels of serum biochemical indices are shown in Table III. At baseline, the biochemical indices did not differ between the two groups. However, after 12 weeks of allicin treatment, significant decreases in TC and TG were observed (P<0.01). Furthermore, the decreases in the allicin group were significant larger than those in the control group (P<0.05).
Table III.
Levels of serum biochemical indices (mmol/l).
| Allicin group | Control group | |||
|---|---|---|---|---|
| Index | Before treatment | After treatment | Before treatment | After treatment |
| TC | 5.60±1.20 | 4.81±1.00a,b | 5.55±1.28 | 5.33±0.78c |
| TG | 3.53±1.76 | 1.93±0.91a,b | 3.09±1.60 | 2.54±0.79c |
Values are expressed as the mean ± standard deviation.
P<0.01, compared with before treatment in the same group
P<0.01, compared with control group
P<0.05, compared with before treatment in the same group. TC, total cholesterol; TG, triglycerides.
Discussion
Atherosclerosis, initiated at sites of endothelial cell injury, is the pathological basis of cardiovascular and cerebrovascular diseases, such as coronary heart disease, cerebral apoplexy and post-angioplasty restenosis. Characteristic features of atherosclerotic lesions include infiltration of monocytic cells, cholesterol deposition, elaboration of extracellular matrix as well as proliferation and migration of vascular smooth muscle cells. HHcy is an independent risk factor of arteriosclerosis (16,17) and has been associated with an increased relative risk of cardiovascular events (18). In 587 coronary disease patients followed up for four years, a mortality rate of 3.8% was observed among those with homocysteinemia (Hcy, <9 µmol/l), and a mortality rate of 24.7% among those with Hcy levels of >15 µmol/l (19). The rate of HHcy among patients with atherosclerotic diseases is up to 40%. In the clinic, HHcy is classified into three categories according to the plasma Hcy concentration: Mild (15–30 µmol/l), moderate (30–100 µmol/l) and severe (>100 µmol/l). The present study identified that coronary heart diseases were closely associated with mild HHcy. Few of the patients with coronary heart diseases had moderate HHcy, but none of them had severe HHcy. In the allicin group, a significant decrease of plasma Hcy levels was observed after 12 weeks of treatment, which was significantly larger than the decrease in the control group, suggesting that the use of allicin may decrease Hcy levels in patients with coronary heart disease. Hcy, a sulfur-containing amino acid, is an intermediate product of methionine metabolism and causes multifold effects through the reactivity of its sulfhydryl group. Laboratory studies have suggested a role of Hcy in activating pathways attributed to atherogenesis and thrombosis (20), including endothelial dysfunction, inflammation, oxidative stress, lipid peroxidation (21), endoplasmic reticulum stress (22), stimulation of vascular smooth muscle cell proliferation and apoptosis (23). Garlic consumption has been inversely correlated with multiple risk factors associated with cardiovascular diseases, including increased platelet aggregation (9,24), reactive oxygen species (25), high blood pressure (11), high cholesterol (12,26), proliferation and migration of vascular smooth muscle cells (27,28), and apoptosis of heart cell (29). Allicin, diallyl trisulfide (CH2=CH-CH2-S-S-S-CH2-CH=CH2), is an organosulfur compound considered responsible for most of the pharmacological activities of garlic. Therefore, it is hypothesized that allicin has certain lowering effects on Hcy. A previous study by our group reported that allicin obviously decreases the serum Hcy levels in rats with HHcy and also alleviates Hcy-induced injury to endothelial cells (30). Another study suggested that garlic and garlic-derived organic polysulfides induce H2S production in a thiol-dependent manner (31). H2S is an endogenous cardioprotective vascular cell-signaling molecule. It can not only activate KATP channels, but also react with S-nitrosothiol species to release NO as a reducing agent and nucleophile, causing vascular smooth muscle cell relaxation. Whether H2S generation from allicin is able to decrease Hcy in HHcy patients requires further investigation. The decrease of Hcy levels in coronary heart disease patients with HHcy after treatment with allicin was confirmed in the present study.
Lipid dysbolism is involved in the development of atherosclerosis. However, evidence linking allicin to blood lipids remains inconclusive. In the present study, significant decreases in TC and TG were observed in the allicin group compared with those in the control group. The possible mechanisms of allicin in reducing blood lipids are as follows: A displacement reaction of allicin with an enzyme containing an SH moiety may take place, which interferes the synthesis of lipids. Allicin may increase lipoidase activity and accelerate the hydrolysis of triglycerides. In the metabolic processes, allicin requires NADPH, which is also the sine qua non substrate in the biosynthesis of cholesterol and triglycerides. Allicin reacts with oxidized glutathione, causing a deficiency of glutathione, which affects the metabolism of insulin in the liver and indirectly affects the metabolism of lipids.
Due to its simplicity, reproducibility, cost-effectiveness and non-invasiveness, IMT measurement of carotid arteries has been widely adopted as a method for assessing systemic atherosclerosis and cardiovascular risk in adults. IMT has been reported to be an independent predictor of coronary heart disease (32–34). In carotid atherosclerosis patients, an increase in the IMT by 0.1 mm is associated with an 11% increase in the risk of acute myocardial infarction (35). The increased thickness of the carotid artery IMT is a signal of the total body vascular intima. Several biological mechanisms of the increased thickness of the vascular intima associated with HHcy include impaired endothelial function, dysregulation of cholesterol and triglyceride biosynthesis and stimulation of vascular smooth muscle cell proliferation. The oxidant stress hypothesis is frequently used to explain the damaging effects of Hcy on vascular cells. Due to the reactive sulfhydryl group (−SH), Hcy, as most thiols (RSH), can undergo oxidation to the disulfide (RSSR) at physiological pH in the presence of O2: 2RSH + O2 → RSSR + [O2−] + 2H → H2O2. By inducing oxidative stress, the free radicals can injure the vascular endothelium. Allicin is able to quench oxygen and hydroxyl radicals to alleviate oxidative stress in a dose-effect manner. Nutritional deficiencies in B vitamin cofactors, including folic acid, vitamin B6 (pyridoxal phosphate) and/or B12 (methylcobalamin) are required for Hcy metabolism. Of note, dietary enrichment in B vitamins can decrease the levels of Hcy but does not attenuate these adverse effects of HHcy. Therefore, only decreasing the Hcy levels is insufficient. The present findings indicated that the carotid artery IMT in the allicin group was significantly decreased compared with that in the control group, which showed the beneficial effect of allicin in atherosclerosis. It is therefore indicated that the beneficial effects may be associated with the anti-oxidative effects of allicin.
In conclusion, the present study indicated that allicin may be useful for the prevention of atherosclerosis, at least in part by decreasing Hcy levels, regulating lipid metabolism and decreasing the carotid artery IMT. Medication prescribed for patients with coronary heart disease may also modify Hcy levels. However, certain studies have indicated that vitamin therapy, such as folic acid and B vitamins, lowered Hcy levels but failed to rescue cardiovascular or neurovascular disease outcomes (36–39). Therefore, allicin may be a prospective drug for the prevention of cardiovascular and cerebrovascular diseases.
Acknowledgements
The present study was supported by Shandong University and by the Tackle Key Problems in Science and Technology Article of Shandong, China (grant no. Y2006C55). The authors would like to thank the Ultrasound and Central Laboratory departments of Qilu Hospital of Shandong University (Jinan, China) for technical assistance.
References
- 1.Fallon UB, Ben-Shlomo Y, Elwood P, Ubbink JB, Smith GD. Homocysteine and coronary heart disease in the caerphilly cohort: A 10 year follow up. Heart. 2001;85:153–158. doi: 10.1136/heart.85.2.153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Suhara T, Fukuo K, Yasuda O, Tsubakimoto M, Takemura Y, Kawamoto H, Yokoi T, Mogi M, Kaimoto T, Ogihara T. Homocysteine enhances endothelial apoptosis via upregulation of Fas-mediated pathways. Hypertension. 2004;43:1208–1213. doi: 10.1161/01.HYP.0000127914.94292.76. [DOI] [PubMed] [Google Scholar]
- 3.Lauricella AM, Quintana IL, Kordich LC. Effects of homocysteine thiol group on fibrin networks: Another possible mechanism of harm. Thromb Res. 2002;107:75–79. doi: 10.1016/S0049-3848(02)00191-3. [DOI] [PubMed] [Google Scholar]
- 4.Dardik R, Varon D, Tamarin I, Zivelin A, Salomon O, Shenkman B, Savion N. Homocysteine and oxidized low density lipoprotein enhance platelet adhesion to endothelial cells under flow conditions: Distinct mechanisms of thrombogenic modulation. Thromb Haemost. 2000;83:338–344. [PubMed] [Google Scholar]
- 5.Maron BA, Loscalzo J. The treatment of hyperhomocysteinemia. Annu Rev Med. 2009;60:39–54. doi: 10.1146/annurev.med.60.041807.123308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Eberhardt RT, Forgione MA, Cap A, Leopold A, Rudd MA, Trolliet M, Heydrick S, Stark R, Klings ES, Moldovan NI, et al. Endothelial dysfunction in a murine model of mild hyperhomocyst(e)inemia. J Clin Invest. 2000;106:483–491. doi: 10.1172/JCI8342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Heydrick SJ, Weiss N, Thomas SR, Cap AP, Pimentel DR, Loscalzo J, Keaney JF., Jr L-Homocysteine and L-homocystine stereospecifically induce endothelial nitric oxide synthase-dependent lipid peroxidation in endothelial cells. Free Radic Biol Med. 2004;36:632–640. doi: 10.1016/j.freeradbiomed.2003.12.001. [DOI] [PubMed] [Google Scholar]
- 8.Dayal S, Lentz SR. Role of redox reactions in the vascular phenotype of hyperhomocysteinemic animals. Antioxid Redox Signal. 2007;9:1899–1909. doi: 10.1089/ars.2007.1806. [DOI] [PubMed] [Google Scholar]
- 9.Patumraj S, Tewit S, Amatyakul S, Jariyapongskul A, Maneesri S, Kasantikul V, Shepro D. Comparative effects of garlic and aspirin on diabetic cardiovascular complications. Drug Deliv. 2000;7:91–96. doi: 10.1080/107175400266650. [DOI] [PubMed] [Google Scholar]
- 10.Kanth V Rajani, Uma Maheswara Reddy P, Raju TN. Attenuation of streptozotocin- induced oxidative stress in hepatic and intestinal tissues of Wistar rat by methanolic-garlic extract. Acta Diabetol. 2008;45:243–251. doi: 10.1007/s00592-008-0051-x. [DOI] [PubMed] [Google Scholar]
- 11.Varmaghany S, Torshizi MA Karimi, Rahimi S, Lotfollahian H, Hassanzadeh M. The effects of increasing levels of dietary garlic bulb on growth performance, systolic blood pressure, hematology, and ascites syndrome in broiler chickens. Poult Sci. 2015;94:1812–1820. doi: 10.3382/ps/pev148. [DOI] [PubMed] [Google Scholar]
- 12.Ashraf R, Aamir K, Shaikh AR, Ahmed T. Effects of garlic on dyslipidemia in patients with type 2 diabetes mellitus. J Ayub Med Coll Abbottabad. 2005;17:60–64. [PubMed] [Google Scholar]
- 13.Liu DS, Gao W, Liang ES, Wang SL, Lin WW, Zhang WD, Jia Q, Guo RC, Zhang JD. Effects of allicin on hyperhomocysteinemia-induced experimental vascular endothelial dysfunction. Eur J Pharmacol. 2013;714:163–169. doi: 10.1016/j.ejphar.2013.05.038. [DOI] [PubMed] [Google Scholar]
- 14.European Society of Hypertension-European Society of Cardiology Guidelines Committee, corp-author. 2003 European society of hypertension-European society of cardiology guidelines for the management of arterial hypertension. J Hypertens. 2003;21:1011–1053. doi: 10.1097/00004872-200306000-00001. [DOI] [PubMed] [Google Scholar]
- 15.Guo J, Xiao F, Tang ZY. Determination of homocysteine in plasma by high performance liquid chromatography. Chin J Lab Med. 2000:217–219. (In Chinese) [Google Scholar]
- 16.Wald DS, Law M, Morris JK. Homocysteine and cardiovascular disease: Evidence on causality from a meta-analysis. BMJ. 2002;325:1202. doi: 10.1136/bmj.325.7374.1202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Homocysteine Studies Collaboration: Homocysteine and risk of ischemic heart disease and stroke: A meta-analysis. JAMA. 2002;288:2015–2022. doi: 10.1001/jama.288.16.2015. [DOI] [PubMed] [Google Scholar]
- 18.Mudd SH, Skovby F, Levy HL, Pettigrew KD, Wilcken B, Pyeritz RE, Andria G, Boers GH, Bromberg IL, Cerone R, et al. The natural history of homocystinuria due to cystathionine beta-synthase deficiency. Am J Hum Genet. 1985;37:1–31. [PMC free article] [PubMed] [Google Scholar]
- 19.Nygård O, Nordrehaug JE, Refsum H, Ueland PM, Farstad M, Vollset SE. Plasma homocysteine levels and mortality in patients with coronary artery disease. N Eng J Med. 1997;337:230–236. doi: 10.1056/NEJM199707243370403. [DOI] [PubMed] [Google Scholar]
- 20.de Koning AB Lawrence, Werstuck GH, Zhou J, Austin RC. Hyperhomocysteinemia and its role in the development of atherosclerosis. Clin Biochem. 2003;36:431–441. doi: 10.1016/S0009-9120(03)00062-6. [DOI] [PubMed] [Google Scholar]
- 21.Blom HJ, Kleinveld HA, Boers GH, Demacker PN, Har-Lemmers HL, Te Poele-Pothoff MT, Trijbels JM. Lipid peroxidation and susceptibility of low-density lipoprotein to in vitro oxidation in hyperhomocysteinaemia. Eur J Clin Invest. 1995;25:149–154. doi: 10.1111/j.1365-2362.1995.tb01541.x. [DOI] [PubMed] [Google Scholar]
- 22.Zhou J, Austin RC. Contributions of hyperhomocysteinemia to atherosclerosis: Causal relationship and potential mechanisms. Biofactors. 2009;35:120–129. doi: 10.1002/biof.17. [DOI] [PubMed] [Google Scholar]
- 23.Skurk C, Walsh K. Death receptor induced apoptosis: A new mechanism of homocysteine-mediated endothelial cell cytotoxicity. Hypertension. 2004;43:1168–1170. doi: 10.1161/01.HYP.0000127811.48554.12. [DOI] [PubMed] [Google Scholar]
- 24.Ohaeri OC, Adoga GI. Anticoagulant modulation of blood cells and platelet reactivity by garlic oil in experimental diabetes mellitus. Biosci Rep. 2006;26:1–6. doi: 10.1007/s10540-006-9004-1. [DOI] [PubMed] [Google Scholar]
- 25.Kanth V Rajani, Uma Maheswara Reddy P, Raju TN. Attenuation of streptozotocin-induced oxidative stress in hepatic and intestinal tissues of Wistar rat by methanolic-garlic extract. Acta Diabetol. 2008;45:243–251. doi: 10.1007/s00592-008-0051-x. [DOI] [PubMed] [Google Scholar]
- 26.Zhu MW, Tang SL. Curative effects of allicin on 59 hyperlipidemia patients. Chin General Practice. 2002:496–497. (In Chinese) [Google Scholar]
- 27.Tan B, Hu YS, Hang H, Yu ZL, Li YJ. Protecting function of Thera-Garlicin on injury of blood vessel endothelium in rats with diabetes mellitus. Modern J Integrated Traditional Chin Western Med. 2006:3335–3336. (In Chinese) [Google Scholar]
- 28.Baluchnejadmojarad T, Roghani M, Homayounfar H, Hosseini M. Beneficial effect of aqueous garlic extract on the vascular reactivity of streptozotocin-diabetic rats. J Ethnopharmacol. 2003;85:139–144. doi: 10.1016/S0378-8741(02)00372-0. [DOI] [PubMed] [Google Scholar]
- 29.Lin YL, Yang SF. Effect of allicin on apoptosis and MAPK of heart cell in diabetic rats. J Lialaoning Univ TCM. 2011;13:56–58. [Google Scholar]
- 30.Wang SL, Liu DS, Guo RC, Zhang WD. Effect of garlicin on the serum homocysteine level in rats. J Shandong Univ. 2006:389–391. (In Chinese) [Google Scholar]
- 31.Benavides GA, Squadrito GL, Mills RW, Patel HD, Isbell ST, Patel RP, Darley-Usmar VM, Doeller JE, Kraus DW. Hydrogen sulfide mediates the vasoactivity of garlic; Proc Natl Acad Sci USA; 2007; pp. 17977–17982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Adams MR, Nakagomi A, Keech A, Robinson J, McCredie R, Bailey BP, Freedman BS, Celermajer DS. Carotid intima-media thickness is only weakly correlated with the extent and severity of coronary artery disease. Circulation. 1995;92:2127–2134. doi: 10.1161/01.CIR.92.8.2127. [DOI] [PubMed] [Google Scholar]
- 33.Chambless LE, Heiss G, Folsom AR, Rosamond W, Szklo M, Sharrett AR, Clegg LX. Association of coronary heart disease incidence with carotid arterial wall thickness and major risk factors: The Atherosclerosis Risk in Communities (ARIC) Study, 1987–1993. Am J Epidemiol. 1997;146:483–494. doi: 10.1093/oxfordjournals.aje.a009302. [DOI] [PubMed] [Google Scholar]
- 34.Burke GL, Evans GW, Riley WA, Sharrett RA, Howard G, Barnes RW, Rosamond W, Crow RS, Rautaharju PM, Heiss G. Arterial wall thickness is associated with prevalent cardiovascular disease in middle-aged adults. The Atherosclerosis Risk in Communities (ARIC) Study. Stroke. 1995;26:386–391. doi: 10.1161/01.STR.26.3.386. [DOI] [PubMed] [Google Scholar]
- 35.Karpe F, Boquist S, Tang R, Bond GM, de Faire U, Hamsten A. Remnant lipoproteins are relatedto intima-media thickness of the carotid artery independently of LDL cholesterol and plasma triglycerides. J Lipid Res. 2001;42:17–21. [PubMed] [Google Scholar]
- 36.Albert CM, Cook NR, Gaziano JM, Zaharris E, MacFadyen J, Danielson E, Buring JE, Manson JE. Effect of folic acid and B vitamins on risk of cardiovascular events and total mortality among women at high risk for cardiovascular disease: A randomized trial. JAMA. 2008;299:2027–2036. doi: 10.1001/jama.299.17.2027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ebbing M, Bleie Ø, Ueland PM, Nordrehaug JE, Nilsen DW, Vollset SE, Refsum H, Pedersen EK, Nygård O. Mortality and cardiovascular events in patients treated with homocysteine-lowering B vitamins after coronary angiography: A randomized controlled trial. JAMA. 2008;300:795–804. doi: 10.1001/jama.300.7.795. [DOI] [PubMed] [Google Scholar]
- 38.Lonn E, Yusuf S, Arnold MJ, Sheridan P, Pogue J, Micks M, McQueen MJ, Probstfield J, Fodor G, Held C, et al. Homocysteine lowering with folic acid and B vitamins in vascular disease. N Engl J Med. 2006;354:1567–1577. doi: 10.1056/NEJMoa060900. [DOI] [PubMed] [Google Scholar]
- 39.Toole JF, Malinow MR, Chambless LE, Spence JD, Pettigrew LC, Howard VJ, Sides EG, Wang CH, Stampfer M. Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke, myocardial infarction, and death: The vitamin intervention for stroke prevention (VISP) randomized controlled trial. JAMA. 2004;291:565–575. doi: 10.1001/jama.291.5.565. [DOI] [PubMed] [Google Scholar]