

Abstract
Group-based training through CrossFit has recently exploded in popularity. Anecdotally, participants often make lifestyle changes and experience improved fitness. Participation factors were mapped to the Integrated Theory of Health Behavior Change and “sense of community” constructs. Key informant interviews were conducted with 6 CrossFit gym owners/coaches. Data were thematically coded with NVivo 10. Results revealed key factors that both facilitated and restricted participation in CrossFit. Findings provide implications for future theory application and highlight how to improve initiation and adherence by capitalizing on community building and taking steps to reduce intimidation and cost, facilitate realistic goals, and ensure social support.
Keywords: exercise, physical fitness, health behavior, CrossFit, theory
BACKGROUND
Current aerobic and muscle strengthening guidelines are met by less than 21% of United States adults,1 and many exercise programs have high drop-out rates.2 To improve the health of the public, it is important to understand the theoretical implications of exercise programs that work. As an exercise program experiencing 2300% growth in the past 10 years,3 this article explores participation in group-based CrossFit exercise through the perspective of coaches.
CrossFit is a strength and conditioning exercise program for all ages. CrossFit is defined as “constantly varied functional movements performed at high intensity” and is focused on developing “a broad, general, and inclusive fitness” (www.crossfit.com/what-is-crossfit). CrossFit also has an explicit aim of community building. CrossFit workouts incorporate functional aerobic and resistance exercises, with self-selected intensity and universal scalability.4 To have a CrossFit affiliated gym, CrossFit-certified trainers apply and pay a yearly fee.
The Integrated Theory of Health Behavior Change (ITHBC) blends concepts from the Health Belief Model, Theory of Reasoned Action, and Social Cognitive Theory and assumes behavior change is dynamic, iterative and requires desire, motivation, and self-reflection.5 The ITHBC includes three categories of the inner self: knowledge and beliefs, self-regulation of skill and abilities, and social facilitation, which lead to proximal and distal health outcomes.5 The ITHBC has been used to examine post-pregnancy weight loss6 and osteoporosis prevention,7 but has never been applied to an exercise program.
In addition, the sense of community (SOC) consists of community members feeling that they belong, matter to each other, and that their needs will be met due to their commitment to be together.8 In sport settings, key SOC factors have included administrative consideration, common interest, competition, equity of administrative decisions, leadership opportunities, social spaces, and voluntary action.9 Previous research found strong SOC among CrossFit participants, although competition was not studied.10 This phenomenological qualitative study11 mapped key factors influencing participation in CrossFit from the perspective of head coaches to the ITHBC and SOC.
METHODS
Participants (N=6) were head coaches/owners from six Midwest CrossFit affiliates. Participants were white and college educated with 4 ±3 years coaching experience; average age was 39 ± 8 years. Purposive selection ensured representation of a variety of settings, including one of the first CrossFit affiliates, a university, a military base, a YMCA, a stand-alone gym, and a home business that used CrossFit methodology. Participants completed written informed consent and the study was approved by the university Institutional Review Board.
Sixty-minute interviews were audio recorded, transcribed verbatim, and verified by each key informant. Questions were designed to examine key social and behavioral factors associated with CrossFit participation. Key informants were asked four questions regarding CrossFit culture and community, four questions regarding CrossFit participation, four questions regarding the effects of CrossFit participation, and four questions about coaching CrossFit participants.
Using NVivo 10, the ITHBC and SOC concepts were applied by a primary coder. A second coder verified the analysis and any disagreements in coding were resolved via discussion.
RESULTS
Key informants’ statements regarding participation in CrossFit addressed each construct of the ITHBC as highlighted in Figure 1. Identified factors both facilitated and served as barriers to participation for knowledge and beliefs, social facilitation, and self-regulation skill and ability; however, only positive factors were identified for proximal and distal outcomes, since those constructs assumed participation in the behavior (CrossFit).
Figure 1.
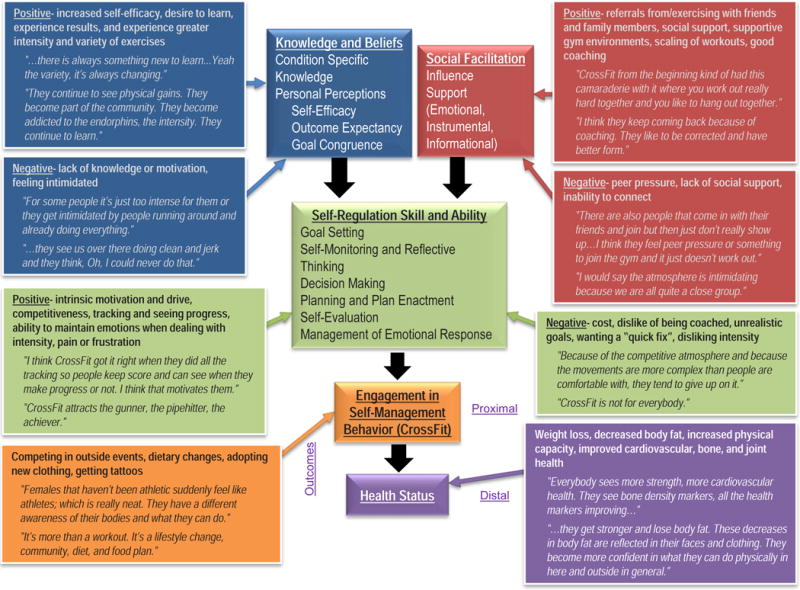
Coaches’ Key Informant Interview Data Regarding CrossFit Participation Mapped to the Integrated Theory of Health Behavior Change
When coding data for SOC constructs (Figure 2), key informants’ statements reflected administrative consideration, common interest, competition, leadership opportunities, social spaces, and voluntary action. However, they did not mention factors that reflected equity of administrative decisions. In addition, statements from two coaches were coded as inclusion, tolerance, and empowerment, which McMillan & Chavis10 explained as individuals defining themselves within the community when feeling empowered; and statements from three coaches were coded as social support, which is regarded as a result of SOC.12
Figure 2.
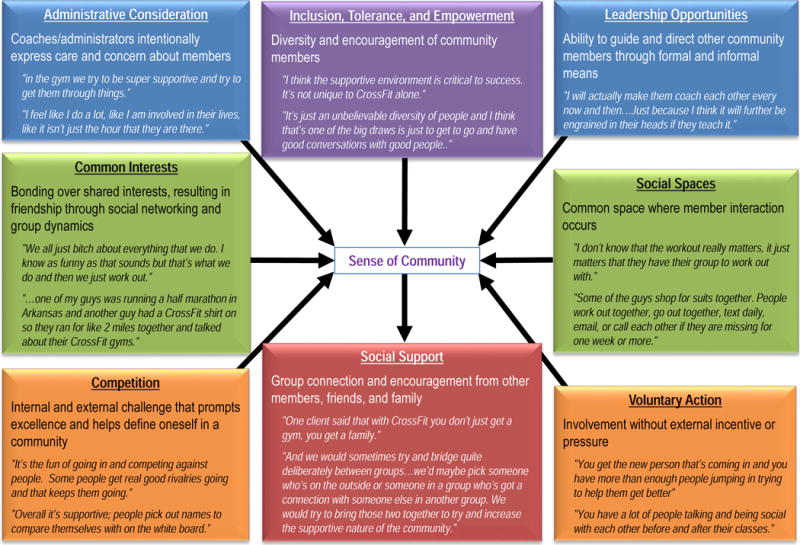
Coaches’ Key Informant Interview Data Regarding CrossFit Participation Mapped to Sense of Community Factors
DISCUSSION
Study results show how key reasons for participation in CrossFit from the perspective of coaches can be mapped to ITHBC theory5 and relevant SOC concepts.8–10,12 Results suggest that while coaches thought participants experienced positive physical and psychological outcomes, environmental and social factors also were important for both exercise initiation and adherence. Findings could help practitioners increase exercise participation by capitalizing on community building and taking steps to reduce intimidation and cost, facilitate realistic goals, and ensure social support. This study adds to the growing body of knowledge for participation in CrossFit exercise programs4,10 and has community-wide public health implications as there are over 12,000 CrossFit affiliates located worldwide (map.crossfit.com).
Data were limited to a single geographic region and only represented the perspective of six gym owners/coaches. However, Guest and associates12 indicate that saturation may be reached with as few as six key informant interviews, which is sufficient in phenomenological inquiries such as this study. Factors identified by the key informants may differ from those perceived as important by CrossFit participants and non-participants, as well as other coaches. However, using open-ended interview questions allowed key informants to articulate their thoughts and opinions on what affects CrossFit participation.
Implications for Advancing Theory in Health Promotion and Community Health
This study provides a novel application of the ITHBC and SOC to an exercise setting. Future research could further investigate practical applications of these theoretical concepts in intervention settings and with multiple stakeholders, including participants and non-participants via focus groups. It would be useful to examine how ITHBC and SOC constructs integrate to facilitate exercise behaviors and how coaches and health promoters can harness key factors that increase participation and limit factors that serve as barriers by helping set reasonable goals, monitoring progress, facilitating supportive communities, and providing education.10,12
Acknowledgments
We would like to acknowledge Andrea Sweetwood, BS, for her assistance with initial data coding.
Funding Disclosure: This research was funded by Kansas State University Start-up Funds awarded to Dr. Heinrich. Work on this manuscript was partially supported by a NIH/NIDDK grant (R01DK099516) awarded to Dr. Heinrich.
Footnotes
Conflict of Interest Statement:
All authors declare no conflicts of interest and do not represent the views of CrossFit, Inc.
References
- 1.Centers for Disease Control and Prevention. Adult participation in aerobic and muscle-strengthening physical activities – United States, 2011. MMWR. 2013;62(17):326–330. [PMC free article] [PubMed] [Google Scholar]
- 2.Marcus BH, Williams DM, Dubbert PM, et al. Physical activity intervention studies: what we know and what we need to know: a scientific statement from the American Heart Association. Circ. 2006;114:2739–2752. doi: 10.1161/CIRCULATIONAHA.106.179683. [DOI] [PubMed] [Google Scholar]
- 3.Beers E. Virtuosity goes viral. CrossFit J. 2014 Jun;30:1–10. Accessed May 2015 at http://library.crossfit.com/free/pdf/CFJ_2014_06_10000_Beers3.pdf. [Google Scholar]
- 4.Heinrich K, Patel PM, O’Neal JL, Heinrich BS. High-intensity compared to moderate-intensity training for exercise initiation, enjoyment, adherence, and intentions: an intervention study. BMC Public Health. 2014;14:789. doi: 10.1186/1471-2458-14-789.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ryan P. Integrated theory of health behavior change: background and intervention development. Clin Nurse Spec. 2009;23:161–170. doi: 10.1097/NUR.0b013e3181a42373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ryan P, Weiss M, Traxel N, Brondino M. Testing the integrated theory of health behavior change for postpartum weight management. J Adv Nurs. 2011;67:2047–2059. doi: 10.1111/j.1365-2648.2011.05648.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ryan P, Maierle D, Csuka ME, Thomson A, Szabo A. Computer-based intervention to enhance self-management of calcium and vitamin D intake in women. West J Nurs Res. 2013;35(8):986–1010. doi: 10.1177/0193945913483369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.McMillan DW, Chavis DM. Sense of community: a definition and theory. J Community Psychol. 1986;14:6–23. [Google Scholar]
- 9.Warner S, Kerwin S, Walker M. Examining sense of community in sport: developing the multidimensional ‘SCS’ scale. J Sport Manage. 2013;27:349–362. [Google Scholar]
- 10.Pickett AC, Goldsmith A, Damon Z, Walker M. The influence of sense of community on the perceived value of physical activity: a cross-context analysis. Lesiure Sci. 2016;38(1):1–16. [Google Scholar]
- 11.Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18:59–82. doi: 10.1177/1525822X05279903. [DOI] [Google Scholar]
- 12.Sarason SB. The psychological sense of community: prospects for a community psychology. San Francisco, CA: Jossey-Bass; [Google Scholar]