

Abstract
Tuberculosis (TB) in prisons is a major problem. The prisons in Chhattisgarh, India, are overcrowded, and there are no formal efforts to engage them in TB control. In 2014, the International Union Against Tuberculosis and Lung Disease and the state TB programme advocated with state prison authorities to implement an enhanced case-finding strategy in the prisons. Sensitisation meetings (one/quarter/prison) to improve awareness among prisoners about TB symptoms and services were coupled with improved access to diagnosis. Patients with presumptive TB who were examined by sputum microscopy increased by 39% per 100 000 prisoners, and TB case notification rates increased by 38%, in 2014 relative to 2013.
Keywords: tuberculosis, diagnosis, prisons, enhanced case finding, Axshya, India
Abstract
La tuberculose (TB) en prison est un problème majeur. Les prisons de l'état de Chhattisgarh, Inde, sont surpeuplées et il n'y a jamais eu d'actions formelles d'engagement dans la lutte contre la TB. En 2014, l'Union Internationale Contre la Tuberculose et les Maladies Respiratoires et le programme d'état pour la TB ont plaidé auprès des autorités carcérales de l'état afin de mettre en œuvre une meilleure stratégie de recherche des cas dans les prisons. Des réunions de sensibilisation (une/trimestre/prison) visant à améliorer les connaissances des détenus en matière de symptômes de la TB et de services disponibles ont été couplées à un meilleur accès au diagnostic. La proportion de patients présumés tuberculeux ayant eu une microscopie de crachats par 100 000 détenus a augmenté de 39% et le taux de déclaration des cas de TB a augmenté de 38% en 2014 par rapport à 2013.
Abstract
La tuberculosis (TB) en las prisiones constituye un grave problema. Los establecimientos penitenciarios de Chhattisgarh, en la India, sufren de hacinamiento y no cuentan con iniciativas formales que promuevan el control de la TB. En el 2014, la Unión Internacional Contra la Tuberculosis y las Enfermedades Respiratorias y el programa nacional contra la TB preconizaron con las autoridades penitenciarias la instauración de una estrategia de detección reforzada de casos en las prisiones. Se asociaron las reuniones de sensibilización (una reunión trimestral por centro) encaminadas a mejorar los conocimientos de los reclusos sobre los síntomas de la TB y los servicios de atención a su alcance con un mejor acceso al diagnóstico. En el 2014, el número de pacientes con presunción clínica de TB en quienes se practicó la baciloscopia del esputo por 100 000 reclusos aumentó un 39% y la tasa de notificación de casos de TB aumento un 38%, con respecto al 2013.
An estimated three million tuberculosis (TB) cases were missed worldwide in 2013, and this number increased to 4.3 million in 2015.1,2 To detect missed cases, and to strengthen the existing infrastructure of national TB programmes (NTPs), a number of recommendations are made in the End TB strategy, including an improved notification system, involvement of the private sector through public-private partnership models, and enhanced and active case finding using new rapid point-of-care diagnostic tests among vulnerable and marginalised populations at high risk for TB.1,3 Enhanced case finding is defined as providing information on the appropriate type of health-seeking behaviour, often combined with improving access to diagnostic services, for people experiencing TB symptoms.4
TB in prisons is a major public health problem in many settings,5 particularly in India, which has a high incidence of TB of 217 per 100 000 population.2 There are several reasons why TB propagates in prisons, including concomitant conditions—particularly human immunodeficiency virus (HIV) infection—injecting drug use, poor nutritional status, smoking, overcrowding and inadequate or inaccessible medical care.5 TB incidence in prisons is 23 times higher than in the general population.6 This situation is worsened by the emergence and spread of multidrug-resistant (MDR) and extensively drug-resistant (XDR) TB.2,7
Chhattisgarh, located in central India, is a vulnerable state, affected by the Naxalite conflict. As of August 2016, 28 of the 30 high-security prisons in the state (two prisons were non-functional) housed 19 473 inmates; the capacity is for 9267 inmates. In this paper, we describe the advocacy and sensitisation activities that we undertook in these prisons and the effect on TB case notification.
ASPECT OF INTEREST
Prison intervention is a flagship activity under India's Revised National Tuberculosis Control Programme (RNTCP). Prior to 2014, however, TB control activities in prisons in Chhattisgarh were neither systematically implemented nor reported. As a result, along with overcrowding in the different prisons in the state, the technical consultant of the International Union Against Tuberculosis and Lung Disease (The Union), in collaboration with Chhattisgarh State TB programme officials, informed state-level policy makers and administrators of the State Department of Prisons about the need for regular education of prison inmates on TB. Instructions were issued by state prison authorities to all the prisons, and by the State TB cell to staff at the district and sub-district levels, to coordinate regular sensitisation meetings (at least one session every 3 months per prison) and to provide reports in the sub-district and district level quarterly reports.
Sensitisation meetings were conducted in all 28 functional prisons in Chhattisgarh state in 2014, using various tools such as videos and flipcharts and contests such as question-and-answer games. Inmates who identified their own TB symptoms and sought care during the sensitisation meetings, or after the meetings during routine health check-ups, underwent sputum smear microscopy. In prisons without a designated microscopy centre (DMC) (n = 25), the district health system and prison authorities made arrangements for sputum smear testing either through accompanied patient referral or through sputum collection and transport to the nearest DMC. In districts where The Union's Project Axshya was involved (10/27 districts), community volunteers were involved in sputum collection and transport. Project Axshya is a flagship programme of The Union being implemented in 300 districts across 21 states of India to enhance the visibility and reach of the RNTCP programme.8
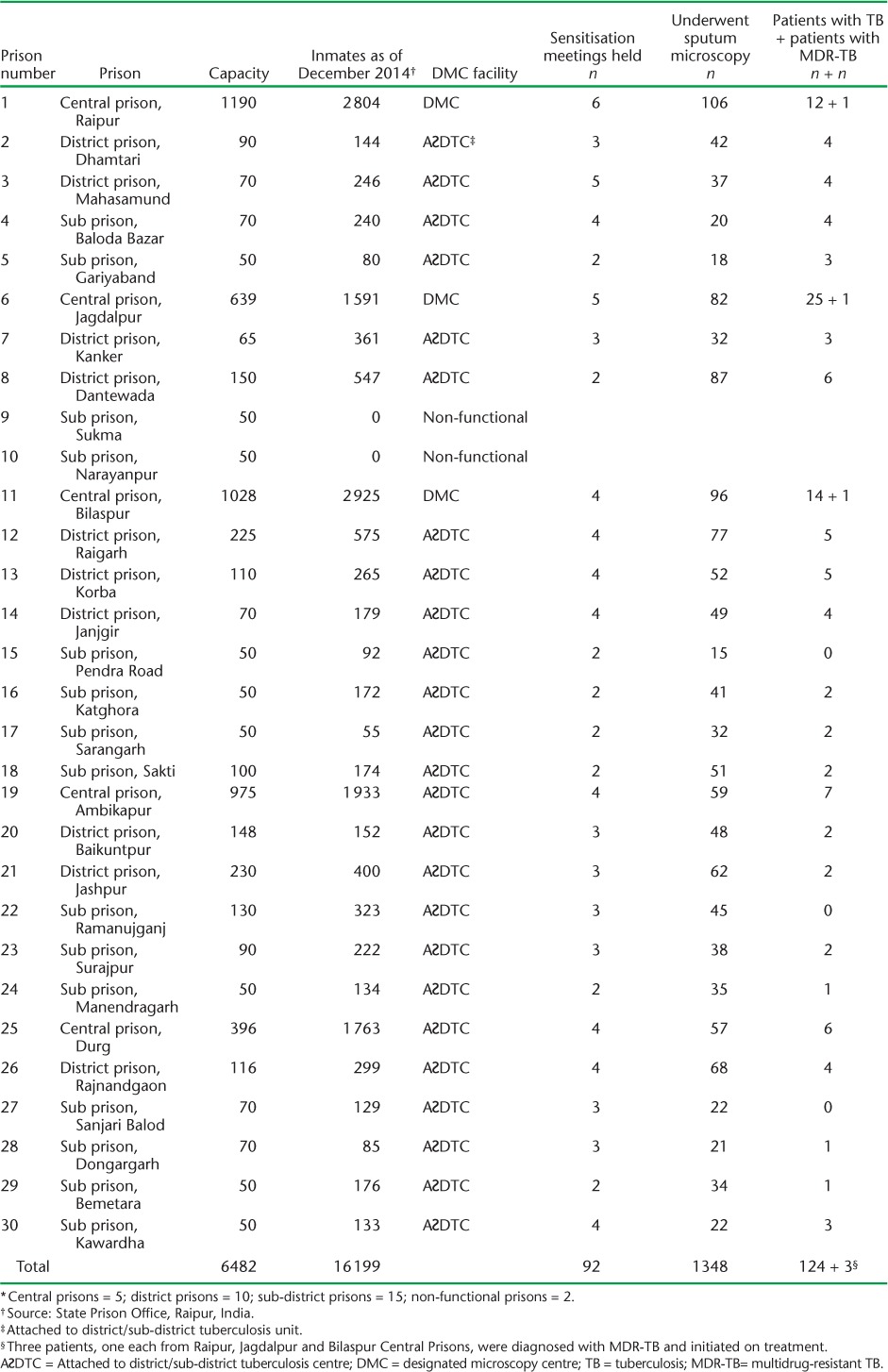
In 2014, 92 sensitisation meetings were conducted for 16 199 prisoners and 735 prison staff (Table 1). Sputum examination was performed for 1348 patients with presumptive TB, resulting in the diagnosis of 124 patients with TB, of whom 96 had smear-positive pulmonary TB and 28 had smear-negative pulmonary TB. Three patients were diagnosed with MDR-TB. All diagnosed patients were initiated on treatment per national guidelines. These prisons contributed 1% of the state's 154 868 patients with presumptive TB who were examined and 0.5% of the state's 28 832 notified TB cases in 2014.
TABLE 1.
Enhanced case finding conducted across the prisons * of Chhattisgarh State, India, 2014 (n = 30) †
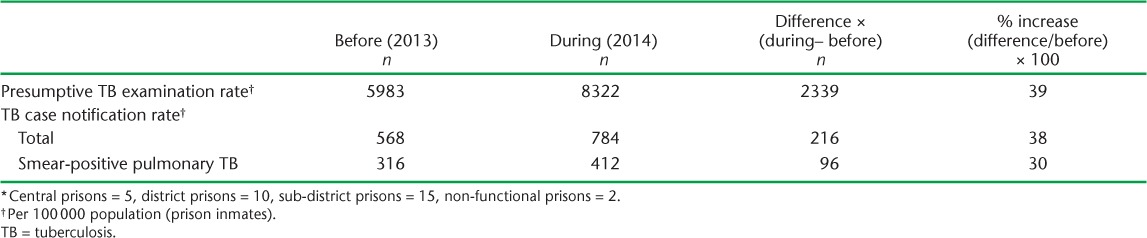
Compared to 2013, the number of patients with presumptive TB who were examined by sputum microscopy per 100 000 prisoners increased by 39% and the TB case notification rate increased by 38% in 2014 (Table 2). The sources of data were the RNTCP quarterly reports and the prison records.
TABLE 2.
Presumptive TB examination rate and TB case detection rate among prison inmates before and during enhanced case finding in prisons * (n = 30) in Chhattisgarh State, India
DISCUSSION
Prison inmates are at high risk for TB and require management. This paper shows that the implementation of an enhanced case-finding strategy with improved access to diagnostic services (via accompanied patient referral or sputum collection and transport) was associated with increased presumptive TB examination and TB case detection rates. We believe that the involvement of relevant stakeholders from the prisons and from TB control at the highest level was critical to success.
To the best of our knowledge, there is no published literature on prison interventions documenting improvement in the detection of TB in India. A situational analysis of TB control activities in a large prison in New Delhi, India, has been published.9 While a before-after study with a control arm would have been the ideal design to be able to attribute the increase in case detection to the enhanced case-finding strategy, this was not possible, given the implementation in all the prisons.
Enhanced case finding might also have led to early diagnosis, resulting in reduced transmission of TB within the prisons. Operational research focusing on these issues and integrating prison and national TB control activities will be helpful to enhance TB control in the prisons. Future research should also focus on assessing the perceptions of prison inmates and prison officials on the challenges in implementing these interventions. Given the high rates of TB, including MDR-TB, in prisons,7 we recommend systematic active screening of all prisoners10 every 3 months and linking presumed cases to diagnosis using rapid diagnostics such as Xpert MTB/RIF® (Cepheid, Sunnyvale, CA, USA).
In conclusion, sustained enhanced case finding with improved access to diagnostic services in prisons has value in improving TB case detection. This should be coupled with systematic screening using rapid diagnostics if we are to reduce TB in line with the World Health Organization End TB strategy.3
Acknowledgments
The authors acknowledge the support of all the district level NTP staff, the staff and volunteers of Project Axshya, implemented by the International Union Against Tuberculosis and Lung Disease (The Union) SouthEast Asia Office (New Delhi, India), the superintendents and assistant superintendents of the respective prisons involved in the implementation of the enhanced case-finding strategy, and The Global Fund to Fight AIDS, Tuberculosis and Malaria (Geneva, Switzerland), which supports Project Axshya, through which the technical consultants and interventions are supported. The authors thank the Department for International Development (London, UK), for funding the Global Operational Research Fellowship Programme at The Union (Paris, France), through which HDS works as an operational research fellow. The activities described in these papers were conducted under routine programme settings and did not require separate funding. The authors thank The Union South-East Asia Office for funding this open-access publication.
Footnotes
Conflicts of interest: none declared.
References
- 1. World Health Organization. . Reach the 3 million: Find. Treat. Cure TB. Geneva, Switzerland: WHO, 2014. [Google Scholar]
- 2. World Health Organization. . Global tuberculosis report 2016. WHO/HTM/TB/2016.13 Geneva, Switzerland: WHO, 2016. [Google Scholar]
- 3. World Health Organization. . End TB Strategy. WHO/HTM/TB/2015.19 Geneva, Switzerland: WHO, 2015. [Google Scholar]
- 4. World Health Organization. . Systematic screening for active tuberculosis: principles and recommendations. WHO/HTM/TB/2013.04 Geneva, Switzerland: WHO, 2013. [PubMed] [Google Scholar]
- 5. World Health Organization. . Tuberculosis in prisons. Geneva, Switzerland: WHO, 2016. http://www.who.int/tb/areas-of-work/population-groups/prisons-facts/en/# Accessed October 2016. [Google Scholar]
- 6. Baussano I, Williams B G, Nunn P, Beggiato M, Fedeli U, Scano F.. Tuberculosis incidence in prisons: a systematic review. PLOS Med 2010; 7: e1000381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. World Health Organization Regional Office for Europe. . Status paper on prisons and tuberculosis. (EUR/07/5063912) Copenhagen, Denmark: WHO Regional Office for Europe, 2007. [Google Scholar]
- 8. International Union Against Tuberculosis and Lung Disease. . Project Axshya. Paris, France: International Union Against Tuberculosis and Lung Disease, 2016. http://axshya-theunion.org/ Accessed November 2016. [Google Scholar]
- 9. Dhuria M, Sharma N, Chopra K K, Chandra S.. Universal access to DOTS in Delhi prisons: where do we stand? Indian J Tuberc 2016; 63: 39– 43. [DOI] [PubMed] [Google Scholar]
- 10. World Health Organization. . Systematic screening for active tuberculosis: an operational guide. WHO/HTM/TB/2015.16 Geneva, Switzerland: WHO, 2015. [Google Scholar]